

Abstract
A developmental cascade model for adolescent substance use beginning in infancy was examined in a sample of children with alcoholic and non-alcoholic parents. The model examined the role of parents’ alcohol diagnoses, depression and antisocial behavior in a cascading process of risk via three major hypothesized pathways: first via parental warmth/sensitivity from toddler to kindergarten age predicting higher parental monitoring in middle childhood through early adolescence serving as a protective pathway for adolescent substance use; second, via child low self-regulation in the preschool years to a continuing externalizing behavior problem pathway leading to underage drinking and higher engagement with substance using peers; and third, via higher social competence from kindergarten age through middle childhood being protective against engagement with delinquent and substance using peers, and leading to lower adolescent substance use. The sample consisted of 227 intact families recruited from the community at 12 months of child age. Results were supportive for the first two pathways to substance use in late adolescence. Among proximal, early adolescent risks, engagement with delinquent peers and parent’s acceptance of underage drinking were significant predictors of late adolescent alcohol and marijuana use. The results highlight the important protective roles of maternal warmth/sensitivity in early childhood to kindergarten age, parental monitoring in middle childhood, and of child self-regulation in the preschool period as reducing risk for externalizing behavior problems, underage drinking, and engagement with delinquent peers in early adolescence. Specific implications for the creation of developmentally fine-tuned preventive intervention are discussed.
Keywords: Adolescent Substance Use, Children of Alcoholics, Self-Regulation, Parental Warmth, Peer Delinquency, Parental Monitoring
Introduction
Adolescence is characterized by significant physical, psychological, and social changes. One of the most notable behavioral changes during this period is an increase in risky behaviors (Crawford, Pentz, Chou, Li, & Dwyer, 2003). Substance use, like other risky behaviors, is initiated and escalates during adolescence (Colder, Campbell, Ruel, Richardson, & Flay, 2002). Indeed, the rates of alcohol, cigarette, and marijuana use are very low prior to about 11 years of age, and increase dramatically from 8th to 12th grades (Johnston, O’Malley, Miech, Bachman, & Schulenberg, 2015). Clearly, substance use involvement changes dramatically from early to later adolescence. Higher frequency of substance use by late adolescence may not only lead to abuse and dependence, but is also associated with greater problems at school, higher psychological distress, more physical health problems, engagement in risky sex, driving while impaired, as well as risk for crime and delinquency (Ritchwood, Ford, DeCoster, Sutton, & Lochman, 2015).
Children of parents with alcohol problems (COAs) are 4 to 10 times more likely to have clinically significant levels of alcohol problems themselves, to have earlier onset of drinking, and to progress from alcohol use to abuse more quickly (Chassin, Curran, Hussong, & Colder, 1997; Donovan, 2004). Thus, COAs are a large and critical component of the underage drinking population (Zucker, Donovan, Masten, Mattson, & Moss, 2009). As early as 1976, Zucker proposed that experiences of infants in alcoholic families could lead to developmental processes culminating in alcohol problems in later life. While there have been many developmental studies of COAs since then, none (except studies of fetal alcohol syndrome) have spanned infancy through late adolescence.
The importance of considering etiological models for substance use that span the developmental ages from infancy to adolescence is especially important given the emphasis on early childhood in recent theoretical models for the development of substance use (Dodge et al., 2009). This dynamic cascade model for development of substance use highlighted the importance of early childhood risk factors stemming from the parent (psychosocial risks) and the child (difficult child factors), as well as early parenting behavior, as primary prospective predictors of adolescent substance use onset. It also highlighted the role of cascading effects, where disruptions in salient issues at each stage of development prospectively predicted salient outcomes at the next stage. In the infant/toddler period, the salient developmental issue of great importance is the quality of the parent-child relationship. This may be most apparent during parent-child interactions that are influenced by proximal parental risk characteristics and child behavior. As children enter the preschool period, one of the most important developmental challenges is the development of self-regulation. Poor parenting and low child self-regulation in the preschool period then set the stage for behavior problems and low social competence as the children enter the school setting. Continuity in these risk factors through middle childhood increase risk for affiliation with delinquent and substance using peer groups in early adolescence, along with continued behavior problems. These aspects of child risks in the context of poor parental monitoring then set the stage for increased substance use risk in adolescence. In addition to these developmental pathways, the dynamic cascade model also supported direct paths from early childhood risks to adolescent parenting and peer problems (see Figure 1). The goal of this paper was to use this dynamic cascade model as a heuristic and test a conceptual model of developmental pathways to substance use from infancy to adolescence, among children of alcoholic fathers and a demographically similar control group.
Figure 1.
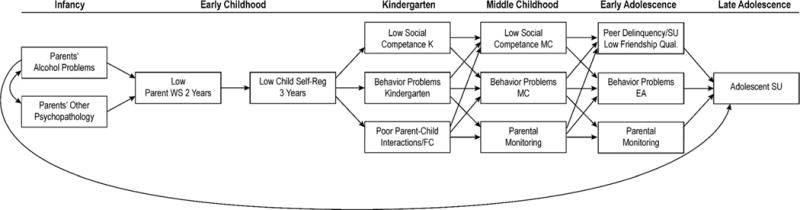
Conceptual model.
When applying this model to children of alcoholic fathers, it is important to note that parents’ alcohol problems often co-occur with other parental risk factors. Fathers’ alcohol problems may occur in the context of maternal heavy drinking or alcohol problems. Parental alcohol problems have also been repeatedly linked to paternal antisocial personality (Hussong, Flora, Curran, Chassin, & Zucker, 2008) and both maternal and paternal depression (Fitzgerald & Eiden, 2007, review). These parental risks are known to have adverse effects on parent-child interactions, thereby setting the stage for problematic child outcomes (Lyons-Ruth, Easterbrooks, & Cibelli, 1997).
One of the most salient aspects of parenting behavior during parent-child interactions in early childhood that is of critical importance throughout development is parental warmth/sensitivity (Raby, Roisman, Fraley, & Simpson, 2015). In recent years, much has been written about the enduring effects of maternal sensitivity in early childhood on child outcomes from early childhood through adolescence (Haltigan, Roisman, & Fraley, 2013) and adulthood (Raby et al, 2015). Indeed, the experience of high maternal sensitivity in early childhood has enduring effects on both adolescent psychopathology (Haltigan et al., 2013) and social/academic competence through adulthood (Raby et al., 2015). Less is known about the potential enduring effects of paternal sensitivity for adolescent outcomes, especially in samples consisting of fathers with clinically significant levels of alcohol problems. However, studies from more normative samples using short-term longitudinal designs indicate that closeness with fathers protects against affiliation with deviant peers in adolescence (Werner & Silbereisen, 2003), a proximal predictor of adolescent substance use. In addition to this larger literature, results from previous waves of this study indicated that parental warmth/sensitivity at 2 years mediates the association between parents’ alcoholism and children’s self-regulation (Eiden, Edwards, & Leonard, 2007). While parental warmth and sensitivity in the early years may be one of the most salient protective factors for child outcomes, in middle childhood and adolescence, parental monitoring becomes an increasingly important predictor of adolescent risk behaviors including substance use (Barnes, Reifman, Farrell, & Dintcheff, 2000). Indeed, parental monitoring or knowledge of child’s whereabouts and activities is one of the most robust protective factors for adolescent substance use across diverse samples of parents and adolescents (Clark, Donnellan, Robins, & Conger, 2015). Thus, one major pathway to substance use may be via low parental sensitivity from infancy to school age, poor parental monitoring from middle childhood to adolescence to higher substance use in adolescence.
In addition to parenting behavior, a second major pathway included in this conceptual model is via child self-regulation in early childhood to externalizing behavior problems (EBP) from school age to adolescence. Self-regulation involves the gradual shift from external to internal regulation that enables the child to conform to societal standards and to restrain antisocial and destructive impulses. Internalization of rules of conduct begins in the second year of life and is fairly well established by 3 years of age (Kochanska, 1993). Problems in self-regulation such as low effortful control and internalization of rules is prospectively associated with EBP among samples of alcoholic and non-alcoholic families at earlier ages (Eiden et al., 2007; Eisenberg et al., 2005; Loukas, Fitzgerald, Zucker, & Von Eye, 2001), and higher levels of EBP are associated with higher alcohol and other substance use (Jester et al., 2008). Indeed, both theory (Costello, Erkanli, Federman, & Angold, 1999; Ellickson & Hays, 1991; Jessor, 1991; Kellam & Anthony, 1998) and empirical evidence (Colder et al., 2013; Hussong, Huang, Curran, Chassin, & Zucker, 2010; Timmermans, van Lier, & Koot, 2008) provide strong support for prospective associations between EBP and adolescent substance use. Children with EBP from school age to adolescence are also more likely to affiliate with deviant peers (Dodge et al., 2009; Scalco et al., 2014). Thus, EBP have both direct and indirect associations with adolescent substance use. However, few studies have examined potential prospective predictive pathways from these aspects of self-regulation in early childhood to EBP from kindergarten age to early adolescence to substance use in later adolescence among COAs.
The third hypothesized pathway to substance use in this conceptual model is through peer relationships. According to socialization theory of substance use, peers play a critical, influential role in the initiation of substance use and changes from use to abuse (Kandel & Adler, 1982). By mid-adolescence, children begin to segregate into different peer groups (Sussman, Pokhrel, Ashmore, & Brown, 2007) on the basis of shared interests, beliefs, or preference for certain activities. These peer groups are relatively small and children behave differently in peer groups than they do at the dyadic level. Peer group substance use and delinquency is a strong and consistent proximal predictor of adolescent substance use in both cross-sectional and prospective studies (Scalco et al., 2014). Few studies have examined early childhood prospective predictors of engagement with delinquent peers in adolescence other than EBP. However, a few studies using prospective design with repeated measurement from adolescence to adulthood have highlighted the role of social competence as being protective against adolescent delinquency by reducing adolescent engagement with delinquent peers (e.g., Stepp, Pardini, Loeber, & Morris, 2011). Thus, we examined if social competence beginning at kindergarten age was associated with lower substance use in adolescence by lowering engagement with delinquent peers in adolescence.
In addition to these general aspects of parent, child, and family processes, social norms regarding drinking have been found to be an important proximal predictor of adolescent alcohol use (Jackson et al., 2014). While adolescent perceptions of peer norms are important predictors of drinking behavior, among children of alcoholics, perceived parent approval or acceptance of drinking may be an important specific predictor of adolescent norms and alcohol use (Brody, Flor, Hollett-Wright, McCoy, 1998; Brody, Flor, Hollett-Wright, McCoy Donovan, 1999).
It is unclear if the developmental pathways to adolescent substance use among COAs are different for adolescent alcohol use compared to other substances as few studies have examined this issue. One exception is a study by Hussong and colleagues (2012) indicating that parents’ lifetime alcohol use disorder was consistently and strongly associated with increased risk for adolescent alcohol, marijuana, as well as other illicit drug use. Thus, we did not have hypotheses about different pathways for different substances used by adolescents, but tested the conceptual model for adolescent alcohol and other drug use.
Finally, although there is some evidence that developmental pathways to problem behaviors may differ for boys and girls (Gorman-Smith & Loeber, 2005), given the limits of our sample size, we were unable to test for gender differences in our full etiological model. However, the literature with regard to gender differences in potential direct effects of fathers’ alcohol problems and adolescent substance use is mixed, with some studies indicating stronger effects for boys (McGue, 1997; McGue, Pickens, & Svikis, 1992; Ritter, Stewart, Bernet, Coe, & Brown, 2002), and others indicating no gender differences (Sher, Walitzer, Wood, & Brent, 1991; Shorey et al., 2013). Thus, we examined if the direct association between parents’ alcohol problems in infancy and adolescent substance use varied by child gender.
Method
Participants
The initial sample consisted of 227 families (116 girls, 111 boys) with 12-month-old infants at recruitment. Families were classified as being in one of two groups: the nonalcoholic or control group consisting of parents with no or few alcohol problems since the child’s birth (n = 102) and the father alcoholic group with families in which the father met criteria for alcohol abuse or dependence (n =125). Within the father alcoholic group, 95 mothers were light drinkers or abstainers, and 30 mothers were heavy drinkers or had current alcohol problems. Given the small sample size for the both alcoholic group, all analyses were conducted comparing alcoholic families with controls, with the majority of alcoholic families being in the alcohol group due to fathers’ current alcohol problems.
The majority of parents in the study were White (94% of mothers and 87% of fathers), approximately 5% of mothers and 7% of fathers were Black, and 2% of parents were other. Parental education ranged from less than a high school degree to postgraduate degree, with more than half of the mothers (59%) and fathers (54%) having completed some post–high school education or having a college degree. Annual family income ranged from $4,000 to $95,000 at recruitment, with the mean income $41,824 (SD = $19,423). All of the mothers were residing with the father of the child in the study at recruitment, and most of the parents were married to each other (88%). Mother’s age at recruitment ranged from 19 to 41 years (M = 30.7, SD = 4.5) and the fathers’ from 21 to 58 years (M = 33.0, SD = 5.9).
Procedure
The names and addresses of these families were obtained from the New York State birth records for Erie County (see Eiden et al., 1999, 2007, for procedural details). Because we had a large pool of families potentially eligible for the nonalcoholic group, alcoholic and nonalcoholic families were matched on race/ethnicity, maternal education, child gender, parity, and marital status. Family assessments were conducted at nine different child ages, in early childhood (12, 18, 24, 36, and 48 months, at kindergarten age (5–6 years of age), in middle childhood (when they were in 4th and 6th grades, about 9–10 and 11–12 years of age), in early adolescence (when they were in 8th grade, 13–14 years of age) and in later adolescence (when they were in 11th/12th grades, 15–19 years of age). Mother-child visits were conducted first followed by father-child visits one to two weeks later. The study was approved by the University at Buffalo Social Science Institutional Review Board. Informed written consents were obtained from both parents, and child assents were obtained from kindergarten-age on, child consents were obtained in later adolescence. Data from infancy (12 months) to later adolescence were used in analyses.
Measures
Parent measures
Parents’ alcohol use
An adapted, self-report measure of The University of Michigan Composite International Diagnostic Interview (Anthony, Warner, & Kessler, 1994; Kessler et al., 1994) was used to assess parental alcohol abuse and dependence. Several questions were reworded to inquire as to “how many times” a problem had been experienced, as opposed to whether it happened “very often”. In addition to the screening criteria, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 2000) criteria for alcohol abuse and dependence diagnoses for current alcohol problems (in the past year) were used to assign final diagnostic group status at the time of recruitment (12 months of child age; see Eiden et al., 2007 for details).
Parents’ antisocial behavior
Parents’ antisocial behavior was assessed using a modified, 28-item version on the Antisocial Behavior Checklist (Ham, Zucker, & Fitzgerald, 1993; Zucker and Noll, 1980) when the infant was 12 months old. The measure was only used at one time point because it is a measure of lifetime antisocial behavior. The internal consistency for the current sample for both mother and father were quite high (Cronbach’s α = .90 for fathers and .82 for mothers). The antisocial behavior scores for both parents were skewed and were transformed using square root transformations.
Parents’ depression
The Center for Epidemiological Studies Depression scale (CES-D; Radloff, 1977) was used to measure mothers’ depressive symptoms at 12 months. The CES-D is a scale designed to measure depressive symptoms in community populations. It is a widely used, self-report measure with high internal consistency (Radloff, 1977), and strong test–retest reliability (Boyd, Weissman, Thompson, & Myers, 1982; Ensel, 1982). Internal consistencies in the present study were Cronbach’s α = .91 for mothers and .88 for fathers.
Parental Warmth/Sensitivity
During the 24-month assessment, parents were asked to interact with their child as they normally would at home for 10 minutes in a room full of toys. Mother-child and father-child interactions were conducted separately. These free-play interactions were coded using a collection of global five-point rating scales using the Parent-Child Early Relational Assessment (Clark, 1999). Composite measures of maternal and paternal warmth/sensitivity were derived from these scales, yielding two composite scales, one for mothers and one for fathers. The warmth/sensitivity composite included items such as expressed positive affect, positive involvement, responsiveness, reading child cues, flexibility, low intrusiveness, consistency/predictability, and low negative affect, with higher scores indicating more positive behavior. The internal consistencies (Cronbach’s alpha) for these scales were .93 and .95 for mothers and fathers respectively. At kindergarten age, parents were asked to decorate a picture frame with their children for 20 minutes. These interactions were coded using the Iowa Family Interaction Rating Scales (Melby, et al., 1998). The warmth/sensitivity composite at kindergarten age included items such as positive reinforcement, sensitive child centered behaviors, humor, positive mood, warmth-support, prosocial behaviors, and physical affection. The internal consistencies for these composite scales were Cronbach’s α = .94 for both mothers and fathers. Two sets of coders scored all of the parent-child interactions. All coders were unaware of group membership, and the coding of mothers and fathers was alternated so that the coder who coded one parent did not code the other parent. Coders were trained on both scales by the first author until they achieved at least 80% reliability. A minimum of at least 15% of observations were selected at random for inter-rather reliability checks. For the 24 month assessments, inter-rater reliability was calculated for 17% of the sample (n =38) and intra-class correlation coefficients ranged from .81 to .92 for mothers and fathers. Inter-rater reliability was calculated for 12% of the sample at kindergarten age, and was .90 for mothers and .95 for fathers.
Parental Monitoring
Parental monitoring was measured with a 9-item child report scale that assessed the degree to which mothers were aware of the child’s whereabouts, acquaintances, and behaviors (Grundy, Gondoli, & Blodgett Salafia, 2007; Sturge-Apple, Gondoli, Bonds, & Salem, 2003) at the middle childhood and early adolescent assessments. Sample items included “how often does your mom/dad know where you go when you are not at home?” and “how often does your mom/dad know who your friends are?” Internal consistencies ranged from Cronbach’s α = .79 at 6th grade to .84 at 8th grade. Maternal and paternal monitoring scores were significantly correlated at both middle childhood (r =.42, p < .001) and early adolescence (r = .61, p < .001), and were composited by taking the average of maternal and paternal reports within each age. High scores on these two final measures reflected high parental monitoring.
Parent Acceptance of Drinking
In early adolescence, children’s perceptions of their parents’ alcohol norms were assessed using modified version of a 14-item measure (Brody, Flor, Hollett-Wright, & McCoy, 1998). The original measure asked about adolescents’ own alcohol norms. In the modified version, children were asked to report on parental acceptance of drinking for a child in 8th grade using a 5-point scale ranging from 1 (totally unacceptable) to 5 (totally acceptable). The internal consistency of this scale was Cronbach’s α = .82.
Child measures
Self-regulation
The self-regulation measure at 3 years included an effortful control battery, an observational measure of internalization of maternal rules, and an observational measure of internalization of fathers’ rules (see Eiden et al., 2007; Kochanska et al., 1996, for details). The effortful control battery consisted of a battery of three tasks developed by Kochanska et al. (1996): a snack delay, whisper, and lab gift. The scores on all three tasks were standardized and a final effortful control score was computed by taking the average of all the scores. The internal consistency of this scale at 3 years was Cronbach’s α = .79. Observations of child internalization of the parental directive to not touch the objects on a prohibited shelf was assessed during a 12 minute observational paradigm (Kochanska & Aksan, 1995). The child’s behavior was coded for every 15-second interval averaged across the entire 12 minutes so that high scores reflected high behavioral internalization. Internalization was coded by two independent coders blind to group status and other information about the families. Inter-rater reliability based on 20 cases (640 15-second coded segments) was κ = .98. The percent agreement for the categories ranged from 90% for gentle touch to 100% for deviation. These three indicators were significantly correlated with each other. Thus, a composite variable was computed by standardizing the measures and taking the average of the two internalization variables and summing with the effortful control composite. The internal consistency of this scale was Cronbach’s alpha = .77.
Social competence
Parental ratings of social competence at Kindergarten were computed by asking the mother and father two items each: “How well does your child get along with classmates”; “How easy is it for your child to make new friends”; these four responses were then averaged. These items were rated on a scale of 1 to 5, with higher scores indicating higher social competence. The scale had moderate internal consistency, Cronbach’s alpha = .67, for the combined scale. Social competence in middle childhood was assessed using the Revised Class Play (RCP; Masten, Morison, & Pellegrini, 1985), a measure of peer reputation. The RCP includes 15 positive and 15 negative behavioral roles. The classmates of the children in the study were asked to pretend they were directors of a play and nominate individual peers for the 30 different behavioral roles or character descriptions. Children were asked to choose one boy and one girl for each role and to choose classmates who “acted that way in real life.” The number of nominations received by the participant in this study was tallied. These nominations were summed into four scores reflecting four dimensions of aggressive-disruptive, sensitive-isolated, leadership-sociability, and prosocial. The standardized leadership-sociability score was used in middle childhood.
Externalizing problem behaviors
Child externalizing problem behaviors (EBP) were assessed using the Externalizing subscale of the Child Behavior Checklist (CBCL; Achenbach, 1991). Maternal reports of EBP were used in the model at Kindergarten age and youth self-reports (YSR) were used in middle childhood and early adolescence. The internal consistency for maternal report at Kindergarten age was Cronbach’s α = .86, YSR middle childhood was α = .89 and early adolescence was α = .92.
Peer delinquency and substance use
Peer delinquency was assessed through child report at 8th grade using a modified, 11 item version of the Peer Delinquency Scale (Loeber, Stouthamer-Loeber, Van Kammen, & Farrington, 1991). The measure was modified to reflect the child’s peer group. Children were asked to identify their peer group and then complete the delinquency scale with regard to these peers. Children were asked to report the number of friends who had engaged in delinquent behavior such as skipping school without an excuse, going joyriding, and hitting someone with the idea of hurting that person in the last 6 months. These items were rated on a five-point scale ranging from 0 = None to 4= All. The internal consistency for the current sample was α = .82.
Peer substance use was assessed through child report at 8th grade using a 10 item scale that measured how many of the adolescents’ peers used alcohol, cigarettes, marijuana, and other drugs on an occasional or regular basis based on previous studies (Chassin, Curran, Hussong, & Colder, 1996), with response options ranging from 0 = None to 4= All. The internal consistency for the current sample was α = .84. Given that the peer delinquency and peer substance use measures were highly correlated, r = .70, these measures were then averaged to create a composite peer delinquency and substance use measure.
Adolescent substance use
Lifetime alcohol use was assessed in early adolescence with a one item question, “Have you ever had more than a few sips of beer, wine or liquor?” Alcohol use was assessed during the late adolescent wave with two items that assessed on how many days in the last month that the adolescent had a drink, and how many drinks per drinking day did the adolescent have. Cigarette use was assessed during the late adolescent wave with two items that assessed on how many days in the last month that the adolescent had smoked, and how many cigarettes per smoking day did the adolescent have. These questions were based on the Youth Risk Behavior Surveillance Survey (YRBS, Grunbaum, Lowry, & Kann, 2001). Marijuana use was assessed at 12th grade with a one item question “In the last 30 days, how many times have you tried marijuana?”, with response options ranging from 1 = Never to 7 = 40 or more times (Substance Abuse and Mental Health Services Administration, 2007). Other drug use was assessed with a composite of 20 questions assessing individual drug use such as “In the last 30 days, how many times have you tried LSD?”, with response options ranging from 1 = Never to 7 = 40 or more times (Substance Abuse and Mental Health Services Administration, 2007). All of the substance use variables were highly skewed and were transformed using square root transformations.
Results
Missing Data
As would be expected of any longitudinal study involving multiple family members, there were incomplete data for some participants at one or more of the five assessments included in this study. Of the 227 families included in analyses, all provided data at 12 and 18 months; 222 (97.8%) mothers and 218 (96.0%) fathers provided data at 24 months; 205 (90.3%) mothers and 193 (85.0%) fathers provided data at 36 months; 185 (81.5%) mothers and 174 fathers (76.7%) provided data at kindergarten, 168 (74.0%) mothers, 157 (69.2%) fathers, and 168 (74.0%) children provided data at 4th grade, 165 (72.7%) mothers, 151 (66.5%) fathers, and 164 (72.2%) children provided data at 6th grade, 154 (67.8%) mothers, 129 (56.8%) fathers, and 162 (71.4%) children provided data at 8th grade, and 186 (81.9%) children provided data at 12th grade.
Among the 227 families, 11% (n = 25) had missing adolescent substance use data because we were unable to locate them. Among the 202 families who were contacted for the later adolescent wave, 2.4% (n = 5) of the parents refused participation, and 5% (n = 11) had passive refusals (did not complete assessments in spite of repeated reminders and scheduling). There were no significant group differences between families with missing versus complete data on any of the alcohol variables, depression, or parenting. Among mothers, 56% of those with missing data at 24 months, 59% of those with missing data at kindergarten age, 52% of those with missing data in middle childhood, and 52% of those with missing data in early adolescence were in the alcoholic group. Fathers’ data were used in infancy, toddler, and kindergarten age. Among fathers, 77% of those with missing data at toddler age, and 62% of those with missing data at kindergarten age were in the alcoholic group. There was no significant association between mothers’ missing data and alcohol group status (p > .10). The association between missingness and father alcoholic status was marginally significant at 2 years, χ2 (1) = 2.66, p = .10, φ = .11, and non-significant at kindergarten age (φ = .08).
With regard to child outcome data, 68% of those with missing data at 3 years, 63% of those with missing data at kindergarten age, 55% of those with missing data in middle childhood, 52% of those with missing data in early adolescence, and 51% of those with missing data in later adolescence, were in the alcohol group. None of these associations between missing on child outcome vs. not and alcohol group status were statistically significant (p > .10). There was no association between missingness and any of the child outcome variables measured at the multiple time points (p > .10). However, families with missing data had fathers who reported higher antisocial behavior compared with those with complete data (Means = 37.78 and 43.64, SDs = 7.54 and 12.27, respectively). Although it is clear that the data were not missing completely at random, data did meet criteria for being missing at random (MAR; Little and Rubin, 1989).
Data Analytic Plan
The demographics and means for the variables in the study by alcohol group status, and correlations among variables were examined first. Next, structural equation modeling (SEM) was used to test the conceptual model depicted in Figure 1 in two steps, first with both the direct associations between alcohol group status and later adolescent substance use and the indirect or mediated pathways, and second, with only the indirect paths from parents’ alcohol group status in infancy to adolescent substance use. These two nested models were compared. All SEM analyses were conducted using Mplus (Version 7.11; Muthen & Muthen, 1998–2013). To take advantage of all data provided by participants, we used full-information maximum likelihood (FIML) to estimate parameters in our models (Arbuckle, 1996). The goodness of fit of the models was examined by using the comparative fit index (CFI) and the root mean-square error of approximation (RMSEA). Indirect effects were examined using the model indirect command in Mplus with bias-corrected bootstrapped standard errors (MacKinnon, 2004). Five thousand bootstrap samples and the 95% bias-corrected confidence intervals (CIs) were used to test significance of indirect effects. Given the limits of sample size, we were unable to test if the full etiological model was different for boys and girls. We examined gender differences in a simplified multiple-group SEM model that included only the two causal paths from parents’ alcohol group status to later adolescent alcohol and marijuana use and the covariance between the residuals of the two variables. These models were tested by comparing fully unconstrained with fully constrained models. The Δχ2 was used as an omnibus test of differences across groups.
Descriptive and correlational analyses
The demographics of the sample by alcohol group status are presented in Table 1. Mothers in the alcoholic group were younger and there were fewer fathers with a college degree in the alcoholic group. There were no significant group differences on fathers’ age, parents’ ethnicity, mothers’ education, gender of the child, or number of children in the family. Group differences in the variables included in model testing are presented in Table 2. There are several notable aspects of these group differences. First, lifetime antisocial behaviors and depressive symptoms in infancy were elevated in parents in the alcoholic compared to nonalcoholic group. Both mothers and fathers in alcoholic families reported more lifetime antisocial behavior and higher depressive symptoms at the first assessment compared to nonalcoholic families. Second, mothers and fathers in alcoholic families displayed lower warmth/sensitivity during play interactions with their toddlers compared to non-alcoholic parents. Third, in kindergarten and throughout middle childhood, parenting behaviors and childhood functioning did not differ by alcohol group status, with the exception of poor social competence among children of alcoholics. Finally, despite the relative lack of differences in middle childhood, differences between groups began to emerge in early adolescence and were significant by late adolescence. Parents in the alcoholic group were perceived by their children as being more accepting of underage drinking and these adolescents were more likely to have peers who engaged in delinquent and substance using behaviors. Adolescents with alcoholic parents reported more alcohol, marijuana, cigarette, and other drug use in later adolescence compared to those in the control group. However, the base rates for cigarette use and other drug use were much lower than for marijuana and alcohol use. Of the total sample, 14.2% smoked cigarettes over the last 30 days, and 7.0% reported other drug use, versus 78.1% who drank any alcohol, and 42.1% who smoked any marijuana. Given these low base rates, cigarette and other drug use were not included in the final models described below1.
Table 1.
Demographics by 12 Month Alcohol Group
| Variable | Control Group (n = 102) |
Alcoholic Group (n = 125) |
Sig Test | P value |
|---|---|---|---|---|
| Mother’s age | 31.40 (4.37) | 30.28 (4.26) | F(1) = 3.81 | .052 |
| Father’s age | 33.17 (6.05) | 32.89 (5.73) | F(1) = 0.13 | ns |
| Mother’s ethnicity | χ2(1) = 0.23 | |||
| White | 95.1% | 95.1% | ||
| Other | 4.9% | 4.9% | ||
| Father’s ethnicity | χ2(1) = 1.21 | ns | ||
| White | 93% | 89% | ||
| Other | 7% | 11% | ||
| Mother’s education | χ2(5) = 1.93 | ns | ||
| Less than high school | 1.0% | 2.9% | ||
| High school degree | 39.2% | 40.2% | ||
| Some college | 30.4% | 27.5% | ||
| 4 year college degree | 29.4% | 29.4% | ||
| Father’s education | χ2(5) = 11.91 | .048 | ||
| Less than high school | 4.0% | 5.1% | ||
| High school degree | 35.4% | 49.5% | ||
| Some college | 19.2% | 17.2% | ||
| 4 year college degree | 41.4% | 28.3% | ||
| Gender of childa | 49.0% | 49% | χ2(1) = .00 | ns |
| Number of children | 2.15 (.92) | 2.08 (.86) | F(1) = .33 | ns |
Percent female
Table 2.
Means and standard deviations for study variables by parents’ alcohol group status.
| Variable | Control Group n = 102 |
Alcoholic Group n = 125 |
F value | p value |
|---|---|---|---|---|
| Infancy (12 months) | ||||
| Paternal antisocial behavior | 36.16 (6.33) | 42.68 (9.56) | 35.00 | .00 |
| Maternal antisocial behavior | 34.27 (4.42) | 37.32 (5.85) | 18.90 | .00 |
| Paternal depression | 6.35 (6.25) | 8.61 (7.43) | 5.94 | .02 |
| Maternal depression | 7.09 (6.16) | 9.71 (8.01) | 7.37 | .01 |
| Toddle Age (2 years) | ||||
| Maternal warmth/sensitivity | 4.70 (.44) | 4.38 (.53) | 22.81 | .00 |
| Paternal warmth/sensitivity | 4.64 (.54) | 4.19 (.66) | 30.59 | .00 |
| Preschool Age (3 years) | ||||
| Child self-regulation | 10.01 (.68) | 9.97 (.77) | .17 | ns |
| Kindergarten Age | ||||
| Social competence | 4.45 (.54) | 4.28 (.54) | 3.96 | .05 |
| Externalizing behavior problems | 7.76 (5.09) | 8.92 (5.38) | 2.22 | ns |
| Maternal warmth/sensitivity | 6.01 (.89) | 6.03 (1.11) | .01 | ns |
| Paternal warmth/sensitivity | 5.18 (1.30) | 5.14 (1.33) | .03 | ns |
| Middle Childhood | ||||
| Social competence | .15 (.86) | −.09 (.90) | 1.83 | ns |
| Externalizing behavior problems | 5.35 (4.38) | 6.58 (5.13) | 2.64 | .10 |
| Parental monitoring | 3.28 (.52) | 3.17 (.49) | 1.96 | ns |
| Early Adolescence | ||||
| Parent norms | 4.46 (4.71) | 7.10 (5.65) | 9.83 | .00 |
| Parental monitoring | 3.19 (.53) | 3.04 (.67) | 2.27 | ns |
| Adolescent alcohol use | .14 (.35) | .16 (.37) | .25 | ns |
| Peer delinquency/substance use | −.19 (.85) | .13 (.91) | 5.25 | .02 |
| Externalizing behavior problems | 6.98 (5.27) | 8.68 (6.07) | 3.43 | .07 |
| Later Adolescence | ||||
| Alcohol use | 6.20 (6.88) | 9.07 (8.77) | 5.77 | .02 |
| Marijuana use | 1.58 (1.24) | 2.27 (2.03) | 7.34 | .01 |
| Cigarette use | .38 (1.53) | 1.58 (4.30) | 5.71 | .02 |
| Other illicit drug use | .39 (1.51) | 1.49 (3.24) | 7.89 | .01 |
Correlations of the other study variables with adolescent substance use are shown in Table 3. Fathers with high lifetime antisocial behavior had partners with high antisocial behavior, reported more symptoms of depression, and had partners with more depression. Parents with higher lifetime antisocial behavior displayed lower warmth/sensitivity during play interaction with their toddlers. Fathers’ lifetime antisocial behavior was associated with higher EBP at all ages, lower maternal monitoring in middle childhood, and higher parental acceptance of drinking in early adolescence, and higher frequency of marijuana use in later adolescence. Mothers’ lifetime antisocial behavior was associated with higher EBP at Kindergarten age, higher parental acceptance of drinking, and higher marijuana use in later adolescence. Parental depression was associated with lower social competence and EBP at kindergarten age.
Table 3.
Correlations Among Study Variables
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. F ASB | – | |||||||||||||||||||
| 2. M ASB | .44** | – | ||||||||||||||||||
| 3. F CESD | .31** | .21** | – | |||||||||||||||||
| 4. M CESD | .21** | .30** | .12 | – | ||||||||||||||||
| 5. M WS T | −.11 | −.16* | .04 | −.08 | – | |||||||||||||||
| 6. F WS T | −.20** | −.25** | −.08 | −.17* | .47** | – | ||||||||||||||
| 7. SR P | −.02 | −.03 | −.03 | −.03 | .31** | .12 | – | |||||||||||||
| 8. SC K | −.17* | −.26** | −23** | −.17* | .28** | .16 | .19* | – | ||||||||||||
| 9. EBP K | .25** | .25** | .26** | .21** | −.08 | −.14 | −.24** | −.33** | – | |||||||||||
| 10. M WS K | −.05 | −.01 | −.09 | −.13 | .29** | .21** | .21** | .15 | −.09 | – | ||||||||||
| 11. F WS K | −.07 | .00 | .02 | −.15 | .24** | .31** | .17* | .07 | −.05 | .36** | – | |||||||||
| 12. SC MC | −.01 | −.10 | −.22* | −.13 | .17 | .16 | .22* | .37** | −.09 | .21* | .09 | – | ||||||||
| 13. EBP MC | .16* | .12 | .04 | .06 | −.08 | −.10 | −.26** | −.04 | .21* | −.16 | .00 | −.13 | – | |||||||
| 14. MM MC | −.21** | −.10 | .03 | −.04 | .14 | .13 | .25** | .11 | −.15 | .22** | .13 | .12 | −.33** | – | ||||||
| 15. PAD EA | .22** | .23** | .01 | −.04 | −.15 | −.11 | −.10 | −.07 | .04 | −.16 | .01 | −.09 | .32** | −.32** | – | |||||
| 16. MM EA | −.13 | −.11 | .03 | −.09 | .11 | .09 | .18* | .01 | −.05 | .22* | .15 | .15 | −.31** | .58*** | −.31** | – | ||||
| 17. AU EA | .13 | .00 | .02 | −.04 | −.07 | −.07 | −.13 | .09 | .07 | .00 | .05 | .02 | .28** | −.22** | .36** | −.24** | – | |||
| 18. PDS EA | .11 | .13 | .07 | −.02 | −.14 | −.03 | −.20 | −.04 | .14 | −.08 | −.03 | −.05 | .43** | −.37** | .42** | −.42** | .40*** | – | ||
| 19. EBP EA | .22** | .09 | −.08 | .06 | −.09 | −.01 | −.08 | −.09 | .20* | −.08 | −.01 | −.06 | .54** | −.31** | .39** | −.44** | .30** | .54** | – | |
| 20. AU LA | .08 | .05 | .06 | .03 | −.12 | −.13 | .04 | .00 | .08 | .06 | .08 | −.01 | .15 | −.13 | .35** | −.13 | .17* | .38** | .18* | |
| 21. MU LA | .22** | .21** | −.03 | −.02 | −.05 | −.23** | −.02 | −.04 | .16 | .03 | .02 | .07 | .13 | −.07 | .36** | −.19* | .10 | .32** | .24** | .39** |
p < .05;
p < .01;
Note: I: Infancy; T: Toddler age; K: Kindergarten age; MC: Middle childhood; EA: Early Adolescence; LA: Later Adolescence; ASB = Antisocial behavior; CESD = CESD depressive symptoms; WS = Warmth and sensitivity; SR = Self‐regulation; SC = Social competence; EBP: Externalizing Problems; MM = Maternal monitoring; PAD = Parental acceptance of drinking; AU = Alcohol use; PDS = Peer delinquency and substance use; MU = Marijuana use.
There was modest stability in parental warmth/sensitivity from toddler to kindergarten age, and higher maternal warmth/sensitivity at kindergarten age was associated with higher maternal monitoring in middle childhood and early adolescence. Children of mothers who were warm/sensitive at toddler age displayed higher self-regulation in the laboratory context at preschool age, and were reported by parents to have higher social competence at kindergarten age. Higher paternal warmth/sensitivity at toddler age was associated with lower frequency of marijuana use in later adolescence.
Children with high self-regulation by preschool age had low EBP and high social competence at kindergarten age and in middle childhood, and high maternal monitoring in early adolescence. Children with high EBP at kindergarten age continued to have higher EBP in middle childhood and early adolescence and reported their mothers as having less knowledge of their whereabouts (low monitoring) in middle childhood. Children who reported their mothers as having low monitoring and had higher EBP in middle childhood also perceived their parents as being more accepting of drinking, reported greater engagement with delinquent and substance using peers, greater EBP and alcohol use in early adolescence.
Parental acceptance of drinking, engagement with delinquent peers, and EBP in early adolescence, were associated with higher substance use in later adolescence. In addition to these proximal associations, parents’ lifetime antisocial behavior reported in infancy, lower paternal warmth/sensitivity at toddler age, and higher EBP at kindergarten age were also associated with higher frequency of adolescent marijuana use.
Testing the Conceptual Model
We first examined the model that included hypothesized indirect paths as well as the two direct paths from alcohol group status in infancy to later adolescent alcohol and marijuana use. This direct plus indirect effects model included alcohol group status, and parents’ antisocial and depressive symptoms as exogenous variables from infancy. The causal paths from these exogenous variables to parents’ warmth/sensitivity at toddler age, paths from parents’ warmth/sensitivity to child self-regulation at preschool age, from child self-regulation to EBP, social competence, and maternal warmth/sensitivity at kindergarten age, and paths from these variables to EBP, social competence, and parental monitoring at middle childhood. The model included causal paths from these middle childhood variables to peer delinquency and substance use, EBP, parental monitoring, parents’ alcohol norms or acceptance of drinking, and children’s alcohol use in early adolescence. Finally, these early adolescent variables were included as proximal predictors of later adolescent substance use. In addition to these causal paths, the model also included within time covariances between all variables.
Results indicated that this conceptual model had a marginally adequate fit to the data, χ2 (138) = 175.66, p = .02; RMSEA = .04, 90% CI [.02, .06]; CFI = .94; TLI = .90. Neither of the two direct paths from alcohol group status to later adolescent alcohol and marijuana use were significant. We next estimated the indirect effects only model, without these two direct paths. The exclusion of these two paths did not significantly change the model chi-square, Δχ2(2) = 3.96, ns, and this model remained an adequately fitting model only, χ2 (140) = 179.62, p = .01; RMSEA = .04, 90% CI [.02, .05]; CFI = .93; TLI = .89.
The modification indices (MI) indicated that the addition of a path from child self-regulation in early childhood to EBP in middle childhood would substantially improve the fit of the model (Δχ2(1) = 11.09, p < .01). This path was theoretically well justified, and was added to the model. After adding this path, MIs further suggested that the addition of a theoretically justified path from father’s depressive symptoms in infancy to children’s EBP in kindergarten (Δχ2(1) = 8.79, p < .01). After adding this path, the MIs supported the addition of a final, theoretically justified path from father’s depressive symptoms in infancy to children’s social competence at Kindergarten age (Δχ2(1) = 7.72, p < .01). The final indirect effects model with the additional three paths fit the data well, χ2 (137) =152.02, p = .18; RMSEA = .02, 90% CI [.00, .04]; CFI = .97; TLI = .96.
The final model is depicted in Figure 2. For ease of presentation, only the significant pathways are depicted in this Figure. The structural paths indicated a pathway to adolescent substance use from child self-regulation at preschool age to EBP from kindergarten through middle childhood and peer delinquency in early adolescence. Lower child self-regulation at preschool age accounted for unique variance in EBP at kindergarten and middle childhood age in addition to continuity of EBP from kindergarten to middle childhood. EBP in middle childhood accounted for unique variance in engagement with delinquent and substance using peers and with higher alcohol use in early adolescence. Peer delinquency was a unique predictor of alcohol and marijuana use in late adolescence.
Figure 2.
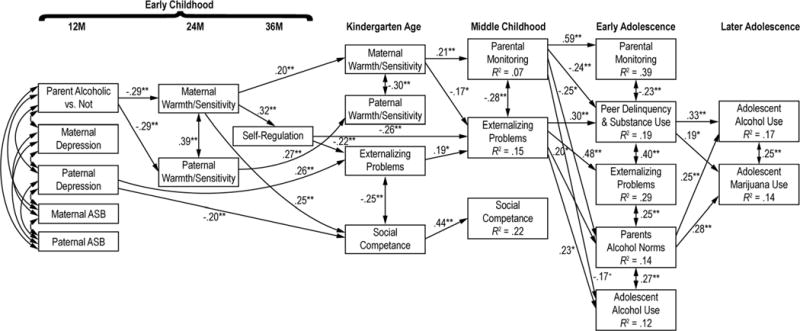
The final model. The numbers represent standardized path coefficients. Nonsignificant paths are not depicted for ease of presentation. Also not included are the error terms and the significant within time covariance between the following variables. The standardized values of these significant covariances were: between peer delinquency/substance use and parents’ alcohol norms, r = .31, p < .001; between peer delinquency/substance use and early adolescent alcohol use, r = .30, p < .001; and EBP and parental monitoring in early adolescence, r = −.30, p < .001.
This pathway from self-regulation to EBP began with parents in the alcohol group displaying lower warmth/sensitivity during play interactions with their toddlers. Lower maternal warmth/sensitivity at toddler age accounted for unique variance in lower child self-regulation at preschool age, lower social competence at kindergarten age, and was somewhat stable from toddler to kindergarten age. Moreover, maternal warmth/sensitivity at kindergarten age accounted for unique variance in maternal monitoring, which remained stable from middle childhood to early adolescence, and was longitudinally and cross-sectionally associated with lower EBP and engagement with delinquent peers. In summary, self-regulation, EBP, and engagement with delinquent/substance using peers represented a chain of cascading mechanisms that were predicted by a cascading chain of maternal parenting behaviors, warmth/sensitivity and monitoring. Parental alcohol problems and associated psychopathology appeared to impact this early in development through their influence on maternal warmth/sensitivity.
In addition to the paths described above, there were several other notable paths. First, while much of the influence of parental psychopathology on child outcomes occurred via maternal warmth/sensitivity, fathers’ depression accounted for significant unique variance in both EBP and social competence in kindergarten. Second, parental monitoring was directly predictive of early adolescent alcohol use, and was prospectively associated with parents’ alcohol norms, and parents’ acceptance of underage drinking was uniquely predictive of late adolescent substance use.
There were significant indirect effects from parents’ alcohol problems in infancy to later adolescent alcohol, B = .08, [95% CIs = .02, .25], as well as marijuana use, B = .01, [95% CIs = .01, .04]. Among the specific pathways, only the pathway from parents’ alcohol group status in infancy → lower maternal warmth/sensitivity at 2 years → lower child self-regulation at 3 years → higher externalizing problems in middle childhood → higher delinquency/substance use in early adolescence → higher alcohol use in later adolescence was statistically significant, B = .04, [95% CIs = .01, .15].
Gender differences
In order to examine if the direct association between parents’ alcohol group status in infancy and adolescent alcohol use varied for girls and boys, we conducted multiple group SEM including only the two causal paths from parents’ alcohol group status in infancy to later adolescent alcohol and marijuana use, and the covariance between the residuals of these two measures. A fully unconstrained model was compared to a model constraining the two paths. The fully unconstrained model was not a significantly better-fitting model than the fully constrained model, Δ χ2 (2) = 2.36, p =.31, suggesting that there were no significant gender differences between the association of alcohol group status and adolescent substance use.
Discussion
The main goal of this study was to examine three hypothesized pathways to adolescent substance use beginning in infancy based on a developmental cascade model of adolescent substance use: a parenting pathway, a child self-regulation to externalizing pathway, and a social competence pathway, among children at high risk due to fathers’ alcohol problems. A secondary goal was to examine if there remained potential direct associations between parent’s alcohol problems in infancy and adolescent substance use, after accounting for these theoretically significant developmental pathways. The final goal was to examine if these direct associations were different for boys and girls.
One of the most critical pathways beginning in infancy was the role of parental warmth/sensitivity in setting the stage for cascade of child risks. Our results were supportive of the importance of maternal warmth/sensitivity in the toddler years as an important protective factor for promoting child self-regulation in the preschool years and social competence in kindergarten. There was also modest stability in maternal warmth/sensitivity from toddler to kindergarten age. Maternal warmth/sensitivity in kindergarten continued to be protective against increases in EBP from kindergarten age to middle childhood. These results are generally supportive of recent findings about the enduring effects of maternal sensitivity in early childhood for children’s social-emotional competence through adolescence (Haltigan, Roisman, Fraley, 2013) by a process of cascading risk. Although paternal warmth/sensitivity in early childhood was associated with lower marijuana and other drug use in late adolescence at the bivariate level, there was no unique association between fathers’ warmth/sensitivity and proximal or distal risks after including maternal warmth/sensitivity in the model. Results from earlier waves of this study indicated that the mediating role of maternal and paternal sensitivity varied by the aspect of child self-regulation and by child gender. When examining mediators of changes in specific aspects of self-regulation from 2 to 3 years, results indicated that fathers’ warmth/sensitivity mediated the association between fathers’ alcohol problems and effortful control for boys (Eiden, Edwards, & Leonard, 2004), and for child internalization of paternal rules for both boys and girls (Eiden, Edwards, & Leonard, 2006). The results with regard to gender differences in the influence of fathers on child outcomes are similar to those reported in other studies (e.g., Webster, Low, Siller, & Hackett, 2013). However, in these previous analyses, maternal and paternal warmth/sensitivity were analyzed separately. The current results indicated that when both maternal and paternal warmth/sensitivity were included in the same model, only maternal warmth/sensitivity accounted for unique variance in a composite measure of child self-regulation at 3 years that included both effortful control and internalization of rules. Given sample size, it was not possible to examine if the role of maternal and paternal warmth/sensitivity in predicting developmental pathways to substance use differed for boys and girls. This is an important area for future research.
Higher maternal, but not paternal warmth/sensitivity in the early years was associated with higher parental monitoring in middle childhood. Parental monitoring or knowledge of child activities was a particularly significant prospective predictor of proximal early adolescent risks included in the model, including engagement with delinquent peers and early adolescent alcohol use. The importance of parental monitoring for adolescent risk behavior has been well established in the literature (Clark, Donnellan, Robins, & Conger, 2015). In addition, previous studies of children of alcoholics have reported the significant protective role of parental monitoring by lowering engagement with delinquent peers (Chassin, Pillow, Curran, Molina, & Barrera, 1993). The current results extend these previous findings downward to middle childhood. High parental monitoring in middle childhood was a unique protective factor for early adolescent behaviors including lowering engagement with delinquent peers and alcohol use in early adolescence. In contrast, early adolescent parental monitoring was not a unique predictor of adolescent substance use, although it was associated with lower marijuana use at the bivariate level. The majority of studies on parental monitoring are either based on cross-sectional data, or on short-term longitudinal studies with a wide age range of children within each wave (e.g., Tilton-Weaver, Burk, Kerr, & Stattin, 2013). One advantage of targeting assessments within a narrow developmental window is that it is informative for targeting timing of interventions. The current results indicate that parental monitoring in middle childhood (6th grade) may be critical for reducing risk for early adolescent problem behaviors.
A second pathway from parents’ alcohol problems to adolescent substance use was via child risks. The results were supportive of a pathway from child’s self-regulation in early childhood to stability in EBP to middle childhood, which then set the stage for engagement with delinquent and substance using peers, underage drinking, and late adolescent substance use. Indeed, EBP in middle childhood accounted for unique variance in early adolescent alcohol use. The externalizing pathway to underage drinking and adolescent substance use has been well established in the literature (Colder et al., 2013; Hussong et al., 2010; Timmermans et al., 2008). However, instead of direct associations between EBP and late adolescent substance use, the current model is supportive of a mediated pathway via engagement with delinquent and substance using peers (Dodge, 2009; Scalco et al., 2014). It is also supportive of the literature on adolescent rule breaking, indicating that children who were aggressive or defiant in the early school years were more likely to have deviant friends, which was predictive of early adolescent rule breaking (Ettekal & Ladd, 2015). This literature suggests that this occurs through peer rejection of aggressive children, who are then at greater risk for affiliating with deviant peers (Ettekal & Ladd, 2015). Our results are consistent with previous studies suggesting that both selection and socialization processes play an important role in the development of adolescent risk behaviors. Children who have higher levels of EBP in middle childhood were more likely to spend time in delinquent and substance using peer groups. Socialization processes then explained the association between engagement with delinquent peers and late adolescent substance use, and this association was no longer explained by children’s own externalizing behaviors. As suggested in earlier research (Ettekal & Ladd, 2015; Patterson, Dishion, Yoerger, 2000; Scarr, 1992), delinquent peer groups may provide the social context for children with EBP by providing access to and the normative context for greater substance use by late adolescence.
Contrary to expectations and previous research, higher social competence was not protective against adolescent substance use by reducing adolescent engagement with delinquent peers (e.g., Stepp et al., 2011). The literature on the protective effects of social competence is small, with a few suggesting direct, protective effects on antisocial behavior and substance use (Caplan et al., 1992; Sorlie, Hagen, & Ogden, 2008), and others indicating that this association is mediated by lowering engagement with delinquent peers (Stepp et al., 2011). However, a closer examination of this literature indicates that differences in measurement of social competence and differences in the nature of samples may account for mixed findings. For instance, the study by Stepp et al. (2011) was based on the Pittsburgh Youth Study who were boys selected for being at high risk for antisocial behavior. Moreover, the measurement of social competence included items that reflected attentional and self-regulatory processes (e.g., fails to carry out assigned tasks, difficulty following directions, demands must be met immediately) rather than social competence per se. This is more similar to our measures of self-regulation and externalizing problems than to social competence. Our measure of social competence in middle childhood was based on peer nominations. Others have reported significant direct associations between social competence and substance use, with high social competence exerting a protective effect (Fishbein et al., 2006). However, the aspect of social competence measured in this study was a combination of high emotional control and interpersonal communication. It is also possible that the association between social competence and adolescent substance use may vary by gender or be moderated by other factors such as school connectedness, adolescent participation in extracurricular activities, substance use cognitions, and drug refusal skills (Lifrak, McKay, Rostain, Alterman, & O’Brien, 1997; Piko, 2006). Future studies of children of alcoholics may well examine these issues.
In addition to these pathways, adolescent perceptions of parent norms or acceptance of drinking in early adolescence was associated with greater frequency of alcohol and marijuana use in late adolescence. The associations with marijuana use may reflect the normative nature of alcohol use by late adolescence. It is possible that children who perceived their parents to be accepting of alcohol use in early adolescence may also perceive their parents to be accepting of drug use by late adolescence. One limitation of these data is the lack of measures regarding parental norms for other drug use including marijuana. However, the current results suggest that child perceptions of parents’ norms regarding alcohol use in early adolescence may be a marker for general acceptance of substance use.
In addition to these pathways, there were direct associations between fathers’ depressive symptoms in infancy and child outcomes at kindergarten age. The results with regard to externalizing problems are consistent with previous studies indicating higher levels of EBP among children of depressed parents, associations between depression and EBP among children of alcoholics (Loukas et al., 2001), and studies indicating direct associations between fathers’ but not mothers’ depression and children’s EBP (e.g., Low & Stocker, 2005). It is possible that fathers’ depression is a marker for increased stress or negativity in the family environment, and this association is not mediated by fathers’ parenting behavior during father-child interactions but more general indices of family functioning or marital quality.
It is important to recognize that this is depression in the context of an alcohol disorder and it may represent the affective impact of drinking and alcohol problems. In addition, few fathers had scores in the range of clinical depression. Nonetheless, fathers’ depression, even in this range, may have predicted lower social competence due to a number of different factors. According to social learning theory, depression could be associated with poor social competence because depressed parents are poor role models for healthy social relationships and may have more restricted affect. Depressed fathers may also be less supportive of children’s interactions outside the home. Fathers’ depression may be particularly predictive because fathers may serve as playmates more often than mothers, and fathers may play an important role in helping children create and maintain relationships outside the family. The ability of depressed fathers to provide such guidance may be impaired.
Finally, analyses of gender differences indicated that these direct associations were not different for boys and girls. Previous studies have noted that boys in alcoholic families had higher vulnerability to risk (Carbonneau et al., 1998; Loukas, Zucker, Fitzgerald, & Krull, 2003; Tarter, Krisci, Clark, 1997; Zucker, Kincaid, Fitzgerald, & Bingham, 1995). One major limitation of this study was we were unable to examine if gender moderated the developmental pathways to adolescent substance use given limits of sample size. However, in previous papers from this sample, we reported that unlike boys in the other groups, boys with alcoholic parents did not display the normative decline in aggressive behavior from 3 to 4 years of age (Edwards, Eiden, Colder, & Leonard, 2006). Thus, given the important role of EBP as a pathway to substance use risk, it is possible that boys were at higher risk for this pathway compared to girls. Future studies with larger samples aggregated from multiple studies or having larger samples may be better able to address the possibility that developmental pathways to adolescent substance use were different for boys and girls. We were also not able to examine if families with two alcoholic parents were at greater risk, given the small number of families in this group. Future studies with larger samples of families in which both parents have alcohol problems may better examine this issue. Our sample size was also too limited to examine if the developmental pathways to substance use were different for alcoholic vs. control families. Future studies with larger samples may examine if parents’ alcohol problems may moderate the mediational pathways to substance use.
In addition to limits of sample size given the complexity of the model, there were other limitations. One major limitation is that the results may not generalize to families of single mothers who separated from or never lived with a partner with alcohol problems. Our eligibility requirements at recruitment included the requirement that both biological parents of the participant child had been living together since the child’s birth. This was an essential design feature that allowed us to examine the family processes as an important contributor of risk. However, this also limited generalizability and reduced diversity of the sample. The current results are also not generalizable to families in which the mother has alcohol problems but the father does not. However, it is important to note that in the majority of families with alcohol problems, mothers’ alcohol problems often exist in the context of fathers’ alcohol problems.
Conclusions and Implications for Interventions
In spite of these limitations, the study fills an important gap in the literature on etiological pathways to substance use among children of alcoholic fathers and matched controls. The results from this prospective, multi-method study highlight the important protective roles of maternal warmth/sensitivity in early childhood to kindergarten age, parental monitoring in middle childhood, and of child self-regulation in the preschool period as reducing risk for EBP, underage drinking, and engagement with delinquent peers in early adolescence. These results have implications for prevention of adolescent substance use with regard to both timing and content. Timing preventive interventions in early childhood may be most beneficial in preventing the cascade of risks via EBP and engagement with delinquent peers from school age to early adolescence. However, preventive interventions in middle childhood, before transition to high school, may also be beneficial with regard to preventing underage drinking and engagement with delinquent peers. With regard to content, interventions in early childhood focused on teaching parents, especially mothers, to be warm and sensitive during interactions with their toddlers and to monitor their children’s activities and peer groups during the transition from middle childhood to early adolescence may have the most benefit. Interventions designed to promote children’s self-regulation in the preschool years may also be beneficial in preventing continuing EBP and early engagement with substance use. In the context of fathers’ alcoholism, interventions with the non-alcoholic parent or the mother may have long lasting implications for preventing underage drinking and more frequent substance use in late adolescence.
Footnotes
We did examine if cigarette and other drug use were associated with any of the variables in the model at the bivariate level. Cigarette use in late adolescence was significantly correlated with paternal antisocial behavior reported in infancy, r = .28, p < .001, and alcohol use, r = .21, p < .01, marijuana use, r = .43, p < .001, and other drug use in late adolescence, r = .17, p < .05. Other drug use in late adolescence was associated with lower paternal warmth/sensitivity at toddler age, r = −.16, p < .05, parental monitoring in middle childhood, r = −.20, p < .05, parental acceptance of drinking r = .24, p < .01, parental monitoring, r = −.24, p < .01, peer delinquency/substance use, r = .26, p < .01, and externalizing in early adolescence, r = .20, p < .05, and alcohol use, r = .22, p < .01, and marijuana use in late adolescence, r = .50, p < .001.
References
- Achenbach TM. Manual for the Child Behavior Checklist/4-18 and 1991 profile. Burlington, VT: University of Vermont Department of Psychiatry; 1991. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, text revision. 4th. Washington, DC: Author; 2000. [Google Scholar]
- Andreasen NC, Rice J, Endicott J, Reich T, Coryell W. The family history approach to diagnosis: How useful is it? Archives of General Psychiatry. 1986;43:421–429. doi: 10.1001/archpsyc.1986.01800050019002. [DOI] [PubMed] [Google Scholar]
- Anthony JC, Warner LA, Kessler RC. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental and Clinical Psychopharmacology. 1994;2:244–268. [Google Scholar]
- Arbuckle JL. Full information estimation in the presence of incomplete data. In: Marcoulides GA, Schumacker RE, editors. Advanced Structural Equation Modeling: Issues and Techniques. Mahwah, NJ: Lawrence Erlbaum Associates; 1996. pp. 243–277. [Google Scholar]
- Barnes GM, Reifman AS, Farrell MP, Dintcheff BA. The effects of parenting on the development of adolescent alcohol misuse: A six-wave latent growth model. Journal of Marriage & the Family. 2000;62:175–186. [Google Scholar]
- Boyd JH, Weissman MM, Thompson WD, Myers JK. Screening for depression in a community sample: Understanding the discrepancies between depression syndrome and diagnostic scales. Archives of General Psychiatry. 1982;39(10):1195–1200. doi: 10.1001/archpsyc.1982.04290100059010. [DOI] [PubMed] [Google Scholar]
- Brody GH, Flor DL, Hollett-Wright N, McCoy JK. Children’s development of alcohol use norms: Contributions of parent and sibling norms, children’s temperaments, and parent-child discussions. Journal of Family Psychology. 1998;12(2):209–219. [Google Scholar]
- Brody GH, Flor DL, Hollett-Wright N, McCoy JK, Donovan JE. Parent-child relationships, child temperament profiles and children’s alcohol use norms. Journal of Studies on Alcohol. 1999;13:45–51. doi: 10.15288/jsas.1999.s13.45. [DOI] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage; 1994. pp. 136–162. [Google Scholar]
- Caplan M, Weissberg RP, Grober JS, Sivo PJ, Grady K, Jacoby C. Social competence promotion with inner-city and suburban young adolescents: Effects on social adjustment and alcohol use. Journal of Consulting and Clinical Psychology. 1992;60:56–63. doi: 10.1037/0022-006X.60.1.56. [DOI] [PubMed] [Google Scholar]
- Carbonneau R, Tremblay R, Vitaro F, Dobkin PL, Saucier JF, Pihl RO. Paternal alcoholism, paternal absence and the development of problem behaviors in boys from age six to twelve years. Journal of Studies on Alcohol. 1998;59:387–398. doi: 10.15288/jsa.1998.59.387. [DOI] [PubMed] [Google Scholar]
- Chassin L, Curran PJ, Hussong AM, Colder CR. The relation of parent alcoholism to adolescent substance use: A longitudinal follow-up study. Journal of Abnormal Psychology. 1996;105(1):70–80. doi: 10.1037//0021-843x.105.1.70. [DOI] [PubMed] [Google Scholar]
- Chassin L, Curran PJ, Hussong AM, Colder CR. The relation of parent alcoholism to adolescent substance use: A longitudinal follow-up study. In: Marlatt GA, VandenBos GR, Marlatt GA, VandenBos GR, editors. Addictive behaviors: Readings on etiology, prevention, and treatment. Washington, DC, US: American Psychological Association; 1997. pp. 509–533. [Google Scholar]
- Chassin L, Pillow DR, Curran PJ, Molina BSG, Barrera M., Jr Relation to parental alcoholism to early adolescent substance use: A test of three mediating mechanisms. Journal of Abnormal Psychology. 1993;102(1):3–19. doi: 10.1037//0021-843x.102.1.3. [DOI] [PubMed] [Google Scholar]
- Clark DA, Donnellan MB, Robins RW, Conger RD. Early adolescent temperament, parental monitoring, and substance use in Mexican-origin adolescents. Journal of Adolescence. 2015;41:121–130. doi: 10.1016/j.adolescence.2015.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark R. The Parent-Child Early Relational Assessment: A factorial validity study. Educational and Psychological Measurement. 1999;59:821–846. [Google Scholar]
- Colder CR, Campbell RT, Ruel E, Richardson JL, Flay BR. A finite mixture model of growth trajectories of adolescent alcohol use: Predictors and consequences. Journal of Consulting and Clinical Psychology. 2002;70:976–985. doi: 10.1037//0022-006x.70.4.976. [DOI] [PubMed] [Google Scholar]
- Colder CR, Scalco M, Trucco EM, Read JP, Lengua LJ, Wieczorek WF, Hawk LW., Jr Prospective associations of internalizing and externalizing problems and their co-occurrence with early adolescent substance use. Journal of Abnormal Child Psychology. 2013;41:667–677. doi: 10.1007/s10802-012-9701-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello EJ, Erkanli A, Federman E, Angold A. Development of psychiatric comorbidity with substance abuse in adolescents: Effects of timing and sex. Journal of Clinical Child Psychology. 1999;28:298–311. doi: 10.1207/S15374424jccp280302. [DOI] [PubMed] [Google Scholar]
- Crawford AM, Pentz MA, Chou CP, Li C, Dwyer JH. Parallel developmental trajectories of sensation seeking and regular substance use in adolescents. Psychology of Addictive Behaviors. 2003;17:179–192. doi: 10.1037/0893-164X.17.3.179. [DOI] [PubMed] [Google Scholar]
- Dodge KA. Mechanisms of gene-environment interaction effects in the development of conduct disorder. Perspectives on Psychological Science. 2009;4:408–414. doi: 10.1111/j.1745-6924.2009.01147.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodge KA, Malone PS, Lansford JE, Miller S, Pettit GS, Bates JE. A dynamic cascade model of the development of substance-abuse onset. Monographs of the Society for Research in Child Development. 2009;73:1–31. doi: 10.1111/j.1540-5834.2009.00528.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donovan JE. Adolescent alcohol initiation: A review of psychosocial risk factors. Journal of Adolescent Health. 2004;35:529–529. doi: 10.1016/j.jadohealth.2004.02.003. [DOI] [PubMed] [Google Scholar]
- Edwards EP, Eiden RD, Colder C, Leonard KE. The development of aggression in 18 to 48 month old children of alcoholic parents. Journal of Abnormal Child Psychology. 2006;34:409–423. doi: 10.1007/s10802-006-9021-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Edwards EP, Leonard KE. Predictors of effortful control among children of alcoholic and nonalcoholic fathers. Journal of Studies on Alcohol. 2004;65:309–319. doi: 10.15288/jsa.2004.65.309. [DOI] [PubMed] [Google Scholar]
- Eiden RD, Edwards EP, Leonard KE. Children’s internalization of rules of conduct: Role of parenting in alcoholic families. Psychology of Addictive Behaviors. 2006;20:305–315. doi: 10.1037/0893-164X.20.3.305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eiden RD, Edwards EP, Leonard KE. A conceptual model for the development of externalizing behavior problems among kindergarten children of alcoholic families: Role of parenting and children’s self-regulation. Developmental Psychology. 2007;43:1187–1201. doi: 10.1037/0012-1649.43.5.1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Zhou Q, Spinrad TL, Valiente C, Fabes RA, Liew J. Relations among positive parenting, children’s effortful control, and externalizing problems: A three-wave longitudinal study. Child Development. 2005;76:1055–1071. doi: 10.1111/j.1467-8624.2005.00897.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellickson PL, Hays RD. Antecedents of drinking among young adolescents with different alcohol use histories. Journal of Studies on Alcohol. 1991;52:398–408. doi: 10.15288/jsa.1991.52.398. [DOI] [PubMed] [Google Scholar]
- Ensel WM. The role of age in the relationship of gender and marital status to depression. Journal of Nervous and Mental Disease. 1982;170:536–543. doi: 10.1097/00005053-198209000-00004. [DOI] [PubMed] [Google Scholar]
- Ettekal I, Ladd GW. Developmental pathways from childhood aggression– disruptiveness, chronic peer rejection, and deviant friendships to early-adolescent rule breaking. Child Development. 2015;86(2):614–631. doi: 10.1111/cdev.12321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fishbein DH, Herman-Stahl M, Eldreth D, Paschall MJ, Hyde C, Hubal R, Ialongo N. Mediators of the stress–substance-use relationship in urban male adolescents. Prevention Science. 2006;7:113–126. doi: 10.1007/s11121-006-0027-4. [DOI] [PubMed] [Google Scholar]
- Fitzgerald HE, Eiden RD. Paternal alcoholism, family functioning, and infant mental health. Zero to Three. 2007:11–18. [Google Scholar]
- Gorman-Smith D, Loeber R. Are developmental pathways in disruptive behaviors the same for girls and boys? Journal of Child and Family Studies. 2005;14:15–27. [Google Scholar]
- Grunbaum JA, Lowry R, Kann L. Prevalence of health-related behaviors among alternative high school students as compared with students attending regular high schools. Journal of Adolescent Health. 2001;29:337–343. doi: 10.1016/s1054-139x(01)00304-4. [DOI] [PubMed] [Google Scholar]
- Grundy AM, Gondoli DM, Blodgett Salafia EH. Marital conflict and preadolescent behavioral competence: maternal knowledge as a longitudinal mediator. Journal of Family Psychology. 2007;21:675–682. doi: 10.1037/0893-3200.21.4.675. [DOI] [PubMed] [Google Scholar]
- Haltigan JD, Roisman GI, Fraley RC. The predictive significance of early caregiving experiences for symptoms of psychopathology through midadolescence: Enduring or transient effects? Development and Psychopathology. 2013;25:209–221. doi: 10.1017/S0954579412000260. [DOI] [PubMed] [Google Scholar]
- Ham HP, Zucker RA, Fitzgerald HE. Assessing antisociality with the Antisocial Behavior Checklist: Reliability and validity studies. Presented at the annual meeting of the American Psychological Society; Chicago. 1993. Jun, [Google Scholar]
- Hu LT, Bentler PM. Evaluating model fit. In: Hoyle RH, editor. Structural equation modeling: Concepts, issues, and applications. Thousand Oaks, CA: Sage; 1995. pp. 76–99. [Google Scholar]
- Hussong A, Huang W, Curran P, Chassin L, Zucker R. Parent alcoholism impacts the severity and timing of children’s externalizing symptoms. Journal of Abnormal Child Psychology. 2010;38:367–380. doi: 10.1007/s10802-009-9374-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong A, Huang W, Serrano D, Curran P, Chassin L. Testing whether and when parent alcoholism uniquely affects various forms of adolescent substance use. Journal of Abnormal Child Psychology. 2012;40:1265–1276. doi: 10.1007/s10802-012-9662-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM, Cai L, Curran PJ, Flora DB, Chassin LA, Zucker RA. Disaggregating the distal, proximal, and time-varying effects of parent alcoholism on children’s internalizing symptoms. Journal of Abnormal Child Psychology. 2008;36:335–346. doi: 10.1007/s10802-007-9181-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM, Flora DB, Curran PJ, Chassin LA, Zucker RA. Defining risk heterogeneity for internalizing symptoms among children of alcoholic parents. Development and Psychopathology. 2008;20:165–193. doi: 10.1017/S0954579408000084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson KM, Roberts ME, Colby SM, Barnett NP, Abar CC, Merrill JE. Willingness to drink as a function of peer offers and peer norms in early adolescence. J Stud Alcohol Drugs. 2014;75:404–414. doi: 10.15288/jsad.2014.75.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jessor R. Risk behavior in adolescence: A psychosocial framework for understanding and action. Journal of Adolescent Health. 1991;12:597–605. doi: 10.1016/1054-139x(91)90007-k. [DOI] [PubMed] [Google Scholar]
- Jester JM, Nigg JT, Buu A, Puttler LI, Glass JM, Heitzeg MM, Zucker RA. Trajectories of childhood aggression and inattention/hyperactivity: Differential effects on substance abuse in adolescence. Journal of the American Academy of Child and Adolescent Psychiatry. 2008;47:1158–1165. doi: 10.1097/CHI.0b013e3181825a4e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Miech RA, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use: 1975–2014: Overview, key findings on adolescent drug use. Ann Arbor: Institute for Social Research, University of Michigan; 2015. [Google Scholar]
- Kandel DB, Adler I. Socialization into marijuana use among French adolescents: A cross-cultural comparison with the United States. Journal of Health and Social Behavior. 1982;23:295–309. [PubMed] [Google Scholar]
- Kellam SG, Anthony JC. Targeting early antecedents to prevent tobacco smoking: Findings from an epidemiologically based randomized field trial. American Journal of Public Health. 1998;88:1490–1495. doi: 10.2105/ajph.88.10.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the National Comorbidity Survey. Archives of General Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Kochanska G. Toward a synthesis of parental socialization and child temperament in early development of conscience. Child Development. 1993;64:325–347. [Google Scholar]
- Kochanska G, Aksan N. Mother-child mutually positive affect, the quality of child compliance to requests and prohibitions, and maternal control as correlates of early internalization. Child Development. 1995;66:236–254. [Google Scholar]
- Kochanska G, Murray K, Jacques TY, Koenig AL, Vandegeest KA. Inhibitory control in young children and its role in emerging internalization. Child Development. 1996;67:490–507. [PubMed] [Google Scholar]
- Lifrak PD, McKay JR, Rostain A, Alterman AI, O’Brien CP. Relationship of perceived competencies, perceived social support, and gender to substance use in young adolescents. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36(7):933–940. doi: 10.1097/00004583-199707000-00015. [DOI] [PubMed] [Google Scholar]
- Little RJA, Rubin DB. The analysis of social science data with missing values. Sociological Methods and Research. 1989;18:292–326. [Google Scholar]
- Loeber R, Stouthamer-Loeber M, Van Kammen W, Farrington D. Initiation, escalation and desistance in juvenile offending and their correlates. Journal of Criminal Law & Criminology. 1991;83:36–82. [Google Scholar]
- Loukas A, Fitzgerald HE, Zucker RA, Von Eye A. Parental alcoholism and co-occurring antisocial behavior: Prospective relationships to externalizing behavior problems in their young sons. Journal of Abnormal Child Psychology. 2001;29:91–106. doi: 10.1023/a:1005281011838. [DOI] [PubMed] [Google Scholar]
- Loukas A, Zucker RA, Fitzgerald HE, Krull JL. Developmental trajectories of disruptive behavior problems among sons of alcoholics: Effects of parent psychopathology, family conflict, and child undercontrol. Journal of Abnormal Psychology. 2003;112:119–131. [PubMed] [Google Scholar]
- Low SM, Stocker C. Family functioning and children’s adjustment: Associations among parents’ depressed mood, marital hostility, parent-child hostility, and children’s adjustment. Journal of Family Psychology. 2005;19:394–403. doi: 10.1037/0893-3200.19.3.394. [DOI] [PubMed] [Google Scholar]
- Lyons-Ruth K, Easterbrooks MA, Cibelli CD. Infant attachment strategies, infant mental lag, and maternal depressive symptoms: Predictors of internalizing and externalizing problems at age 7. Developmental Psychology. 1997;33:681–692. doi: 10.1037//0012-1649.33.4.681. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP. Introduction to statistical mediation analysis. Mahwah, NJ: Erlbaum; 2004. [Google Scholar]
- Masten AS, Morison P, Pellegrini DS. A revised class play method of peer assessment. Developmental Psychology. 1985;21:523–533. [Google Scholar]
- McGue M. A behavioral-genetic perspective on children of alcoholics. Alcohol Health and Research World. 1997;21:210–217. [PMC free article] [PubMed] [Google Scholar]
- McGue M, Pickens RW, Svikis DS. Sex and age effects on the inheritance of alcohol problems: a twin study. Journal of Abnormal Psychology. 1992;101:3–17. doi: 10.1037//0021-843x.101.1.3. [DOI] [PubMed] [Google Scholar]
- Melby JN, Conger RD, Book R, Rueter M, Lucy L, Repinski D, Scaramella L. The Iowa Family Interaction Rating scales. 5th. Iowa State University, Institute for Social and Behavioral Research; 1998. Unpublished document. [Google Scholar]
- Muthén LK, Muthén BO. Mplus User’s Guide. Seventh. Los Angeles, CA: Muthén & Muthén; 1998–2013. [Google Scholar]
- Patterson G, Dishion T, Yoerger K. Adolescent growth in new forms of problem behavior: Macro- and micro-peer dynamics. Prevention Science. 2000;1:3–13. doi: 10.1023/a:1010019915400. [DOI] [PubMed] [Google Scholar]
- Piko BF. Adolescent smoking and drinking: the role of communal mastery and other social influences. Addictive Behaviors. 2006;31(1):102–114. doi: 10.1016/j.addbeh.2005.04.013. [DOI] [PubMed] [Google Scholar]
- Raby KL, Roisman GI, Fraley RC, Simpson JA. The enduring predictive significance of early maternal sensitivity: social and academic competence through age 32 years. Child Development. 2015;86:695–708. doi: 10.1111/cdev.12325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Ritchwood TD, Ford H, DeCoster J, Sutton M, Lochman JE. Risky sexual behavior and substance use among adolescents: A meta-analysis. Children and Youth Services Review. 2015;52:74–88. doi: 10.1016/j.childyouth.2015.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ritter J, Stewart M, Bernet C, Coe M, Brown SA. Effects of childhood exposure to familial alcoholism and family violence on adolescent substance use, conduct problems, and self-esteem. Journal of Traumatic Stress. 2002;15:113–122. doi: 10.1023/A:1014803907234. [DOI] [PubMed] [Google Scholar]
- Scalco MD, Colder CR, Hawk LW, Read JP, Wieczorek WF, Lengua LJ. Internalizing and externalizing problem behavior and early adolescent substance use: a test of a latent variable interaction and conditional indirect effects. Psychology of Addictive Behaviors. 2014;28:828–840. doi: 10.1037/a0035805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scarr S. Developmental theories for the 1990s: Development and individual differences. Child Development. 1992;63:1–19. [PubMed] [Google Scholar]
- Sher KJ, Walitzer KS, Wood PK, Brent EE. Characteristics of children of alcoholics: putative risk factors, substance use and abuse, and psychopathology. Journal of Abnormal Psychology. 1991;100:427–448. doi: 10.1037//0021-843x.100.4.427. [DOI] [PubMed] [Google Scholar]
- Shorey RC, Fite PJ, Elkins SR, Frissell KC, Tortolero SR, Stuart GL, Temple JR. The association between problematic parental substance use and adolescent substance use in an ethnically diverse sample of 9th and 10th graders. Journal of Primary Prevention. 2013;34:381–393. doi: 10.1007/s10935-013-0326-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sørlie MA, Hagen KA, Ogden T. Social competence and antisocial behavior: Continuity and distinctiveness across early adolescence. Journal of Research on Adolescence. 2008;18:121–144. [Google Scholar]
- Stepp SD, Pardini DA, Loeber R, Morris NA. The relation between adolescent social competence and young adult delinquency and educational attainment among at-risk youth: The mediating role of peer delinquency. The Canadian Journal of Psychiatry. 2011;56:457–465. doi: 10.1177/070674371105600803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sturge-Apple ML, Gondoli DM, Bonds DD, Salem LN. Mothers’ responsive parenting practices and psychological experience of parenting as mediators of the relation between marital conflict and mother-preadolescent relational negativity. Parenting. 2003;3(4):327–355. [Google Scholar]
- Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: National Findings. Washington, DC: Department of Health and Human Services; 2007. [Google Scholar]
- Sussman S, Pokhrel P, Ashmore RD, Brown BB. Adolescent peer group identification and characteristics: A review of the literature. Addictive Behaviors. 2007;32:1602–1627. doi: 10.1016/j.addbeh.2006.11.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tarter RE, Kirisci L, Clark DB. Alcohol use disorder among adolescents: Impact of paternal alcoholism on drinking behavior, drinking motivation, and consequences. Alcoholism: Clinical & Experimental Research. 1997;21:171–178. doi: 10.1111/j.1530-0277.1997.tb03745.x. [DOI] [PubMed] [Google Scholar]
- Tilton-Weaver LC, Burk WJ, Kerr M, Stattin H. Can parental monitoring and peer management reduce the selection or influence of delinquent peers? Testing the question using a dynamic social network approach. Developmental Psychology. 2013;49:2057–2070. doi: 10.1037/a0031854. [DOI] [PubMed] [Google Scholar]
- Timmermans M, van Lier PA, Koot HM. Which forms of child/adolescent externalizing behaviors account for late adolescent risky sexual behavior and substance use? Journal of Child Psychology and Psychiatry and Allied Disciplines. 2008;49:386–394. doi: 10.1111/j.1469-7610.2007.01842.x. [DOI] [PubMed] [Google Scholar]
- Webster L, Low J, Siller C, Hackett RK. Understanding the contribution of a father’s warmth on his child’s social skills. Fathering. 2013;11:90–113. [Google Scholar]
- Werner NE, Silbereisen RK. Family relationship quality and contact with deviant peers as predictors of adolescent problem behaviors: The moderating role of gender. Journal of Adolescent Research. 2003;18:454–480. [Google Scholar]
- Zucker RA. Parental influences upon drinking patterns of their children. In: Greenblatt M, Schuckit MA, editors. Alcoholism problems in women and children. New York: Grune & Stratton; 1976. [Google Scholar]
- Zucker RA, Donovan JE, Masten AS, Mattson ME, Moss HB. Developmental processes and mechanisms: ages 0–10. Alcohol Res Health. 2009;32:16–29. [PMC free article] [PubMed] [Google Scholar]
- Zucker RA, Kincaid SB, Fitzgerald HE, Bingham CR. Alcohol schema acquisition in preschoolers: Differences between children of alcoholics and children of nonalcoholics. Alcoholism: Clinical & Experimental Research. 1995;19:1011–1017. doi: 10.1111/j.1530-0277.1995.tb00982.x. [DOI] [PubMed] [Google Scholar]
- Zucker RA, Noll RB. The antisocial behavior checklist. Michigan State University, Department of Psychology; East Lansing: 1980. Unpublished work from the UMMSU Longitudinal Study. [Google Scholar]