

Abstract
Background
There is evidence that drinking during residential treatment is related to various factors, such as patients' general control beliefs and self‐efficacy, as well as to external control of alcohol use by program's staff and situations where there is temptation to drink. As alcohol use during treatment has been shown to be associated with the resumption of alcohol use after discharge from residential treatment, we aimed to investigate how these variables are related to alcohol use during abstinence‐oriented residential treatment programs for alcohol use disorders (AUD).
Methods
In total, 509 patients who entered 1 of 2 residential abstinence‐oriented treatment programs for AUD were included in the study. After detoxification, patients completed a standardized diagnostic procedure including interviews and questionnaires. Drinking was assessed by patients' self‐report of at least 1 standard drink or by positive breathalyzer testing. The 2 residential programs were categorized as high or low control according to the average number of tests per patient.
Results
Regression analysis revealed a significant interaction effect between internal and external control suggesting that patients with high internal locus of control and high frequency of control by staff demonstrated the least alcohol use during treatment (16.7%) while patients with low internal locus of control in programs with low external control were more likely to use alcohol during treatment (45.9%). No effects were found for self‐efficacy and temptation.
Conclusions
As alcohol use during treatment is most likely associated with poor treatment outcomes, external control may improve treatment outcomes and particularly support patients with low internal locus of control, who show the highest risk for alcohol use during treatment. High external control may complement high internal control to improve alcohol use prevention while in treatment.
Keywords: Alcohol Dependence, Alcohol Use, Locus of Control, Alcohol Testing
Alcohol dependence often develops into a chronic, relapsing condition that has serious physiological, psychological, and social consequences associated with immense direct and indirect costs (Rehm, 2010). Thus, the prediction of treatment success and the resumption of alcohol use among patients with addiction disorders are of major interest in addiction research. The most clear predictors of the resumption of alcohol use are gross measures of patient's demographic status, psychiatric status, program attendance, and treatment history (Abbott, 1984; Adamson et al., 2009; Brewer et al., 1998; Hall, 2001; Hubbard et al., 1997). However, alcohol use during abstinence‐oriented residential treatment programs has also been associated with poor alcohol use outcomes at follow‐up (Ludwig et al., 2013). Furthermore, there is evidence that the resumption of alcohol use is related to various factors, such as patients' general control beliefs and alcohol‐related self‐efficacy, as well as to the external control of alcohol use and situations where there is temptation to drink (e.g., (Adamson et al., 2009; Carton and Nowicki, 1994; Hall, 2001; Hubbard et al., 2003; Huckstadt, 1987; Koski‐Jännes, 1994; Ludwig et al., 2013; Rotter, 1990).
Locus of control has been demonstrated as an intrapersonal factor associated with alcohol use following an abstinent phase (Huckstadt, 1987). Locus of control as conceptualized by Rotter (1966) defines an individual's belief about the extent to which outcomes of events are under personal control (internal locus of control) or under the influence of chance, fate, or powerful others (external locus of control). Research dealing with the relationships between locus of control and alcohol use disorder (AUD) and its treatment points out the beneficial role of internal control attributions. Alcohol‐dependent individuals have been found to be more external in their drinking‐related locus of control than nondependent drinkers (Rohsenow and O'Leary, 1978). In addition, control beliefs have been shown to be an important factor in recovery from AUD, with more internal drinking‐related control beliefs being associated with more favorable trends in drinking outcomes (Koski‐Jännes, 1994). This is in line with a further study showing that high internal locus of control scores at pretreatment are associated with better treatment outcomes (Canton et al., 1988). In summary, most studies indicate that the locus of control of patients with AUD becomes more internal over treatment, and internal locus of control is associated with treatment success while external locus of control is more often associated with dropouts and the resumption of alcohol use.
However, in addition to intrapersonal factors, contextual factors also help to resist temptation and support abstinence. Autonomy support and control are the 2 most common intervention methods that are discussed in the field of teaching and coaching (Baumann and Kuhl, 2005). While autonomy‐supportive conditions are assumed to help individuals to satisfy their needs and to promote internal behavior regulation, controlling conditions offer less self‐determination and have been found to promote external behavior regulation. Some individuals profit from autonomy support, whereas others show better resistance to temptation to drink with external control. Studies, mainly conducted with students, indicate that state‐oriented subjects who show an inability to regulate emotions, thoughts, and behavior effectively need external sources of regulation to overcome their deficits in self‐motivation. However, on the contrary, action‐oriented subjects are more robust toward contextual conditions, probably because of their high ability to self‐regulate affect (Baumann and Kuhl, 2005; Jostmann and Koole, 2007; Koole and Jostmann, 2004).
Relying on external sources of regulation can compensate for self‐regulatory deficits (Baumann and Kuhl, 2005). As patients with AUD often show self‐regulatory deficits, treatment centers frequently apply alcohol testing to further support abstinence and obtain feedback on success rates. The interaction of alcohol testing with patients' locus of control has not yet been explored. Thus, it is the aim of this retrospective analysis to investigate how patients' general control beliefs are related to alcohol testing and alcohol use during residential treatment programs. Moreover, we estimate the influence of state and situational variables on alcohol use by including self‐efficacy and situations where there is temptation to drink.
Materials and Methods
This observational study was conducted in the 2 largest inpatient alcohol treatment center programs in Switzerland (Klinik Südhang, Forel Klinik), offering abstinence‐oriented treatment for AUD. Treatment centers have agreed to provide treatment programs based on the same treatment principles and to share a common research unit. The comparability of the cognitive‐behavioral oriented treatment programs is ensured by offering the same length of stay and similar amounts of group and single psychotherapy sessions including relapse prevention, and sports therapy, art therapy, work integration, and social service. A description of the study's methodology and results concerning the content and dimensionality of therapists' and patients' views of control measures have been published elsewhere (Klingemann et al., 2013).
The 2 specialized clinics for the treatment of AUD differed in their external control of alcohol use by program's staff as follows: (i) the low external control clinic (LCC) used a system of random detection of alcohol consumption using breath and urine testing; (ii) the high external control clinic (HCC) systematically assessed expelled air after each stay outside the clinic area and conducted unannounced inspections using alcohol breathalyzer tests and urine testing for drug use. Patients of both clinics were asked to report any alcohol consumption.
Patients
During the study period of 2.5 years (November 2009 to May 2011), 509 patients with AUD entered into 1 of 2 residential treatment programs for AUD with an intended 3‐month length of stay. Provision of informed consent was the only inclusion criteria applied in the study.
Approximately two‐thirds of the patients were male and lived alone (Table 1). Almost 60% were unemployed when admitted to treatment, almost 80% had more than a high school education, and more than 80% had previous detoxifications.
Table 1.
Demographic and Clinical Characteristics and Predictor Variables at Admission Presented Separately for Clinics with High and Low Frequency of Control
| Low external control clinic (LCC) (n = 323) | High external control clinic (HCC) (n = 186) | t (df)/χ2 (df) | p | |
|---|---|---|---|---|
| Female/male | 108/215 | 62/124 | 0.001 (1) | 0.981 |
| Age [M (SD)] | 45.35 (10.12) | 47.48 (11.38) | −2.18 (507) | 0.029 |
| Employed (no/yes) | 154/159 | 102/81 | 1.976 (1) | 0.160 |
| Firm relationship, married (no/yes) | 234/81 | 131/48 | 0.072 (1) | 0.789 |
| Education | ||||
| Less than high school | 30 | 33 | 9.34 (2) | 0.009 |
| High school | 209 | 117 | ||
| College | 27 | 27 | ||
| Severity of drinking problems AUDIT [M (SD)] | 27.52 (6.83) | 26.43 (6.80) | 1.73 (504) | 0.084 |
| Years of problematic drinking [M (SD)] | 10.89 (±8.2) | 10.37 (±8.2) | 0.655 (461) | 0.513 |
| Previous detoxifications | ||||
| None | 43 | 30 | 1.53 (3) | 0.676 |
| One | 109 | 57 | ||
| Two or three | 87 | 56 | ||
| More than three | 71 | 38 | ||
| Physical damage (yes/no) | 116/207 | 74/112 | 0.756 (1) | 0.384 |
| Mental disorder or impairment other than AUD (yes/no) | 152/171 | 97/89 | 1.225 (1) | 0.268 |
| Mean number of controls per patient | 10.96 (±18.74) | 50.18 (±27.86) | −17.10 (282.92) | 0.000 |
| Alcohol use during treatment (no/yes) | 191/132 | 130/56 | 5.86 (1) | 0.015 |
| Internal locus of control (IES) [M (SD)] | 3.90 (±0.75) | 3.87 (±0.68) | 0.426 (436) | 0.671 |
| External locus of control (IES) [M (SD)] | 2.53 (±0.69) | 2.65 (±0.76) | −1.81 (431) | 0.073 |
| Confidence to abstain from alcohol (AASE‐G) [M (SD)] | 73.39 (±17.39) | 76.85 (±17.21) | −1.98 (427) | 0.047 |
| Temptation to drink (AASE‐G) [M (SD)] | 70.84 (±17.31) | 73.92 (±16.93) | −1.79 (431) | 0.073 |
AASE‐G, German version of the Alcohol Abstinence Self‐efficacy Scale; AUDIT, Alcohol Use Disorders Identification Test; IES, internal and external locus of control scale.
After providing a complete description of the study to the subjects, written informed consent was obtained. All patients voluntarily participated in the anonymous survey for the medical statistics of Switzerland and filled out questionnaires for diagnostic and quality assurance purposes.
Procedure
At admission to an abstinence‐oriented residential treatment program for AUD, detoxified patients underwent a standardized diagnostic process including interviews and questionnaires assessing sociodemographic characteristics (age, sex, employment, and prior detoxifications), psychological parameters (e.g., severity of dependence, comorbidities), and acute or chronic medical conditions, which were used for therapy and clinic internal evaluations, as well as for the medical statistics of Switzerland.
Assessments
The patients' characteristics and severity of AUD were assessed with the act‐info (addiction, care and therapy information: a nationwide documentation system for clients of Swiss drug and addiction help centers) interview that includes questions on sociodemographic characteristics, such as age, gender, and employment; indices and severity of substance use and its consequences; the number of previous detoxifications; and psychological and social functioning. This interview is a nationwide instrument used during attendance and discharge of any inpatient treatment program for addictive disorders. The Alcohol Use Disorders Identification Test (AUDIT) as part of the act‐info assessment was used to assess the severity of drinking problems (Saunders et al., 1993).
Internal and external locus of control was assessed at treatment admission using a short questionnaire with 3 items for each subscale (Jakoby and Jacob, 2009). Patients rated their perceived internal and external locus of control on a 5‐point Likert‐type scale.
Self‐efficacy was assessed at treatment intake with the German version of the Alcohol Abstinence Self‐efficacy Scale (AASE‐G; Bott et al., [Link]; AASE; DiClemente et al., 1994). Patients were asked to rate their confidence to abstain from alcohol across 20 different high‐risk situations on a 5‐point Likert‐type scale. A parallel set of items assessed subjects' temptation to drink in each situation.
The number of internal alcohol controls implemented by the clinic, as well as the number of alcohol use incidents during the inpatient treatment program, was assessed for each patient. Alcohol use during treatment was assessed based on self‐reports and breathalyzer testing. Alcohol use was operationalized as the consummation of at least 1 standard drink (i.e., 10 to 12 g ethanol). Patients who used other substances besides alcohol, such as cannabis or benzodiazepine, but who did not use alcohol were not included in the analyses.
Statistics
The 2 clinics with different control frequencies were compared using independent t‐tests or chi‐squared tests regarding patients' characteristics, frequency of controls per patient, and alcohol consumption during treatment.
To assess the influence and interaction of internal and external control on alcohol use during treatment, patients were divided into 2 groups based on the internal and external locus of control scale (IES) (Jakoby and Jacob, 2009), depending on whether they scored above or below the mean. The external control variable was based on the different control frequencies of the 2 clinics.
To determine which variables might predict alcohol use during treatment, we first performed bivariate correlations. To assess the most important predictors of alcohol use during inpatient treatment, a hierarchical logistic regression for the primary outcome (alcohol use during treatment) was conducted. The significantly correlated demographic baseline measurements such as age at treatment admission, number of detoxifications, and the severity of AUD (AUDIT) were entered as control variables in step 1. The confidence to abstain from alcohol (AASE‐G) and temptation to drink subscale scores at treatment admission were entered as state parameters in step 2, and finally, the interaction of internal and external control was entered in step 3. The statistical significance level was set at p < 0.05 for 2‐sided tests.
Results
Description of the Subjects and Clinics
There were no significant differences between the 2 clinics in the demographic and clinical characteristics of the patients at baseline, except in the level of education and the confidence to abstain from alcohol at treatment admission (Table 1).
The LCC showed significantly fewer controls per patient and more alcohol use during treatment (Table 1). Of the 188 patients who used alcohol during treatment, 81 consumed only once, 46 patients twice, 31 patients 3 times, 14 patients 4 times, 7 patients 5 times, 5 patients 6 times, 2 patients 7 times, and 2 patients 8 times. The primary diagnosis of all patients was AUD. Only a few patients reported comorbid substance use (n = 14; 7.1%), but the 2 clinics did not differ regarding patients' comorbid substance use (χ2 = 2.78; df = 3; p ≥ 0.05). Furthermore, the 2 clinics did not differ regarding additional comorbid mental disorders such as anxiety, depression, psychotic disorders, and suicidality (χ2 = 1.24; df = 1; p > 0.05) as well as comorbid medical health problems such as Hep‐B, Hep‐C, liver disorder, esophageal varices, pancreatitis, or polyneuropathy (χ2 = 0.55; df = 1; p > 0.05).
Internal and External Control
Of the 280 patients in the group with low internal locus of control, 117 used alcohol during treatment, while only 42 of the 158 patients in the group with high internal locus of control used alcohol (χ2 = 10.1; df = 1; p ≤ 0.001). The results for the external control (alcohol testing) group were similar: more patients from the LCC consumed alcohol at least once during treatment compared to the HCC (Table 1).
Predicting Alcohol Use During Treatment
Bivariate correlations were used to assess the relationship between variables at admission to a residential treatment program (baseline) and alcohol use during treatment. The correlations demonstrated that alcohol use was positively correlated with the severity of AUD (AUDIT: r = 0.12, df = 506, p ≤ 0.01) and the number of detoxifications (r = 0.12, df = 491, p < 0.01), while it was negatively correlated with the age at treatment admission (r = −0.26, df = 509, p < 0.001), (IES; (r = −0.14, df = 438, p < 0.01), confidence to abstain from alcohol (AASE‐G; r = −0.25, df = 43, p < 0.001), temptation to drink (AASE‐G; r = −0.25, df = 433, p < 0.001), and external control frequency (r = −0.17, df = 509, p < 0.05). Furthermore, there was a trend of the level of education on alcohol use (χ2 = 4.74; df = 2; p ≤ 0.09). However, the frequency of alcohol consumption 6 months prior to treatment was not associated with alcohol use during treatment (r = −0.16, df = 476, p < 0.729) nor did patients with alcohol use during treatment differ regarding alcohol use before treatment admission (χ2 = 3.81; df = 5; p > 0.5).
The hierarchical logistic regression indicated that age at treatment admission (B = −0.05; p < 0.001), number of detoxifications (B = 0.28; p < 0.05), and internal control (B = −0.55; p < 0.05) were shown to be significant predictors for alcohol use during treatment. Moreover, there was a trend for external control to be a predictor (B = −0.42; p < 0.1). The severity of AUD (B = 0.01; p > 0.7), level of education (B = −0.03; p > 0.6), and the subscales measuring confidence to abstain from alcohol (AASE‐G; B = −0.01; p < 0.1) and temptation to drink (AASE‐G; B = −0.01; p > 0.2) were not significant predictors.
To investigate the interaction of internal (high vs. low IES) and external (high‐ vs. low‐control frequency) control on alcohol consumption during treatment, we conducted the same hierarchical logistic regression with the interaction of internal and external control in step 3. The interaction of internal and external control (p = 0.015), age at treatment admission (p = 0.001), and number of detoxifications (p = 0.040) were the only significant predictors for alcohol consumption during treatment (Table 2). Again, the severity of AUD (p > 0.7), level of education (p > 0.8), and the subscales measuring confidence to abstain from alcohol (AASE‐G; p > 0.3) and temptation to drink (AASE‐G; p > 0.2) were not significant predictors. The influence of the association between internal and external control on alcohol use during treatment is displayed in Fig. 1, indicating that patients with low internal and low external control show the highest rate of alcohol use during treatment, while patients with high internal and high external control demonstrate the lowest rate.
Table 2.
Results of the Hierarchical Logistic Regression Analysis with Relapse During Treatment as the Dependent Variable
| Predictors | B | SE (B) | Wald | OR | CI (95%) |
|---|---|---|---|---|---|
| Step 1 | |||||
| Age | −0.038 | 0.012 | 10.46** | 0.96 | 0.94 to 0.99 |
| AUDIT | 0.011 | 0.019 | 0.34 | 1.01 | 0.98 to 1.05 |
| No. of detoxifications | 0.240 | 0.117 | 4.22* | 1.27 | 1.01 to 1.59 |
| Level of education | −0.209 | 0.211 | 0.982 | 0.811 | 0.55 to 1.23 |
| Step 2 | |||||
| Temptation to drink (AASE‐G) | −0.012 | 0.011 | 1.16 | 0.99 | 0.97 to 1.01 |
| Confidence to abstain from alcohol (AASE‐G) | −0.015 | 0.011 | 1.94 | 0.99 | 0.97 to 1.00 |
| Step 3 | |||||
| Internal × external controla | −0.157 | 0.065 | 5.90* | 0.86 | 0.75 to 0.97 |
*p < 0.05, **p < 0.01.
Interaction of internal (high vs. low IES) and external (high‐ vs. low‐control frequency clinic) control.
B, regression coefficient; SE, standard error; CI, confidence interval; OR, odds ratio; AASE‐G, German version of the Alcohol Abstinence Self‐efficacy Scale; AUDIT, Alcohol Use Disorders Identification Test; IES, internal and external locus of control scale.
Figure 1.
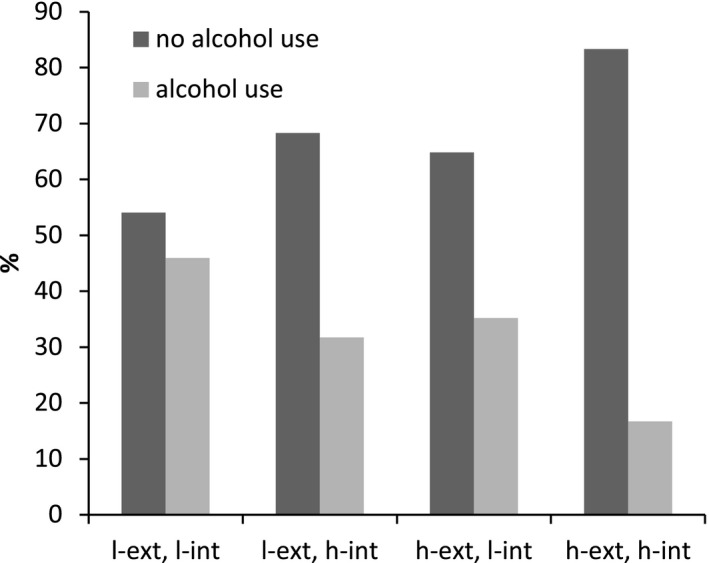
Percentage of alcohol use during residential treatment programs for alcohol use disorders displayed separately for internal (high vs. low) and external (high vs. low) control groups. l‐ext, l‐int: low external control, low internal control (45.9% alcohol use); l‐ext, h‐int: low external control, high internal control (31.7% alcohol use); h‐ext, l‐int: high external control, low internal control (35.2% alcohol use); h‐ext, h‐int: high external control, high internal control (16.7% alcohol use).
Discussion
We examined the contribution of patients' internal locus of control and the external control frequency of 2 clinics on alcohol use during residential abstinence‐oriented treatment programs for alcohol use disorder AUD. Patients with low internal locus of control at treatment admission showed a significantly higher risk of alcohol use during treatment compared to patients with high scores on the internal locus of control scale. Similar results were found for external control by residential programs; patients in the residential program with an unsystematic low frequency of controls showed significantly more alcohol use compared to the patients in the residential program with a systematic high frequency of controls.
In regard to the prediction of alcohol use and the investigation of the contribution of internal and external control variables, we controlled statistically for important predictors of outcome, such as age at treatment admission, number of detoxifications, severity of AUD, confidence in abstaining from alcohol, and temptation to drink. The results demonstrated that only about 17% of the patients with high internal locus of control and high frequency of controls by staff exhibited alcohol use during treatment. However, about 46% of the patients with low internal locus of control and low external frequency of controls used alcohol during treatment. While the predictive value of age, number of detoxifications, and self‐efficacy have also been found in previous studies (Adamson et al., 2009; Ciraulo et al., 2003; Ludwig et al., 2013), the type of interaction demonstrated in this study between locus of control and alcohol testing has not been found before. Patients with high internal locus of control benefit the most from alcohol testing, suggesting that internal control beliefs are consolidated in the co‐occurrence of external control. Even when patients' internal control is low, the frequency of abstinence is doubled when external control is high.
Note that self‐efficacy and temptation to drink did not contribute to alcohol use during residential treatment, suggesting that more malleable variables are not associated with alcohol use while patients are attending an intensive, residential treatment program for AUD. Thus, locus of control, in conjunction with external control, seems to exert a stronger influence on remaining abstinent.
Some methodological limitations should be taken into consideration. A generalized measure was used to assess locus of control (Jakoby and Jacob, 2009) instead of the Drinking‐related Internal–External Locus of Control Scale (DRIE; Kivlahan et al., 1983). Nevertheless, we resisted applying a drinking‐specific instrument as we aimed to assess the construct from a comprehensive perspective instead of focusing on drinking control. Furthermore, there are variables such as craving (Martinotti et al., 2013), anhedonic aspects (Hatzigiakoumis et al., 2011), and temperamental characteristics (Khazaal et al., 2013) that may have an influence on starting alcohol use. In addition, we do not have data about the total standard drinks per day or week prior to treatment admission or during treatment. As we did not examine or control these variables, we cannot exclude their influence on treatment outcome or alcohol use during treatment. A further limitation arises from the study design that considered alcohol testing as a naturalistic rather than an experimental condition. Confounding variables might cause center‐specific differences that may alternatively account for the results, although the 2 programs were quite similar in terms of patient, treatment, and setting characteristics. Controlled studies with drinking‐specific measures are necessary to further examine the relationship between locus of control and the effects of alcohol testing. Follow‐up data on alcohol use after discharge from treatment may improve the clinical relevance of the findings. Furthermore, the costs of alcohol testing have to be taken into account and related to the benefits of control.
The present findings are of clinical relevance for several reasons. External controls can help to significantly reduce alcohol use during treatment and even patients with high internal locus of control benefit considerably from external controls. As alcohol use during treatment is associated with the resumption of alcohol use after residential treatment (Ludwig et al., 2013), external controls can enhance treatment outcomes, especially for those patients with low internal locus of control, who demonstrated the highest risk for alcohol use during treatment.
Acknowledgments
This research was supported by a grant from the Swiss Foundation for Alcohol Research (No. 202) and is part of the research project, How wet are inpatient alcohol clinics.
References
- Abbott MW (1984) Locus of control and treatment outcome in alcoholics. J Stud Alcohol Drugs 45:46. [DOI] [PubMed] [Google Scholar]
- Adamson SJ, Sellman JD, Frampton CMA (2009) Patient predictors of alcohol treatment outcome: a systematic review. J Subst Abuse Treat 36:75–86. [DOI] [PubMed] [Google Scholar]
- Baumann N, Kuhl J (2005) How to resist temptation: the effects of external control versus autonomy support on self‐regulatory dynamics. J Pers 73:443–470. [DOI] [PubMed] [Google Scholar]
- Bott KE, Rumpf HJ, Bischof G, Meyer C, Hannöver W, Hapke U, John U(2003) Alkoholabstinenz‐Selbstwirksamkeitsfragebogen; deutsche Version (AASE‐G): Deutsche Version der Alcohol Abstinence Self‐Efficacy (AASE) Scale [Alcohol Abstinence Self‐Efficacy‐Scale, German Version], in Elektronisches Handbuch zu Erhebungsinstrumenten im Suchtbereich (EHES) [Electronic Handbook on Assessment Instruments in the Addiction Field], Vol. 3.00 (Glöckner‐Rist A, Rist F, Küfner H. eds). Zentrum für Umfragen, Methoden und Analysen. Mannheim. [Google Scholar]
- Brewer JB, Zhao Z, Desmond JE, Glover GH, Gabrieli JDE (1998) Making memories: brain activity that predicts how well visual experience will be remembered. Science 281:1185–1187. [DOI] [PubMed] [Google Scholar]
- Canton G, Giannini L, Magni G, Bertinaria A, Cibin M, Gallimberti L (1988) Locus of control, life events and treatment outcome in alcohol dependent patients. Acta Psychiatr Scand 78:18–23. [DOI] [PubMed] [Google Scholar]
- Carton JS, Nowicki S (1994) Antecedents of individual differences in locus of control of reinforcement: a critical review. Genet Soc Gen Psychol Monogr 120: 31–81. [Google Scholar]
- Ciraulo DA, Piechniczek‐Buczek J, Iscan EN (2003) Outcome predictors in substance use disorders. Psychiatr Clin North Am 26:381–409. [DOI] [PubMed] [Google Scholar]
- DiClemente CC, Carbonari JP, Montgomery RP, Hughes SO (1994) The Alcohol Abstinence Self‐Efficacy scale. J Stud Alcohol 55:141–148. [DOI] [PubMed] [Google Scholar]
- Hall EA (2001) Feelings about drug use: drug‐related locus of control. Criminal Justice Research Group, Integrated Substance Abuse Programs, Semel Institute of Neuroscience and Human Behavior, University of California, Los Angeles.
- Hatzigiakoumis DS, Martinotti G, Di Giannantonio M, Janiri L (2011) Anhedonia and substance dependence: clinical correlates and treatment options. Front Psychiatry 2: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hubbard RL, Craddock SG, Anderson J (2003) Overview of 5‐year followup outcomes in the drug abuse treatment outcome studies (DATOS). J Subst Abuse Treat 25:125–134. [DOI] [PubMed] [Google Scholar]
- Hubbard RL, Craddock SG, Flynn PM, Anderson J, Etheridge RM (1997) Overview of 1‐year follow‐up outcomes in the Drug Abuse Treatment Outcome Study (DATOS). Psychol Addict Behav 11:261. [Google Scholar]
- Huckstadt A (1987) Locus of control among alcoholics, recovering alcoholics, and non‐alcoholics. Res Nurs Health 10:23–28. [DOI] [PubMed] [Google Scholar]
- Jakoby N, Jacob R (2009) Messung von internen und externen Kontrollüberzeugungen in allgemeinen Bevölkerungsumfragen. Zuma Nachrichten 45:61–71. [Google Scholar]
- Jostmann NB, Koole SL (2007) On the regulation of cognitive control: action orientation moderates the impact of high demands in Stroop interference tasks. J Exp Psychol Gen 136:593. [DOI] [PubMed] [Google Scholar]
- Khazaal Y, Gex‐Fabry M, Nallet A, Weber B, Favre S, Voide R, Zullino D, Aubry J‐M (2013) Affective temperaments in alcohol and opiate addictions. Psychiatr Q 84:429–438. [DOI] [PubMed] [Google Scholar]
- Kivlahan DR, Donovan DM, Walker RD (1983) Predictors of relapse: interaction of drinking‐related locus of control and reasons for drinking. Addict Behav 8:273–276. [DOI] [PubMed] [Google Scholar]
- Klingemann H, Schläfli K, Eggli P, Stutz S (2013) Drinking episodes during abstinence‐oriented inpatient treatment: dual perspectives of patients and therapists—a qualitative analysis. Alcohol Alcohol 48:322–328. [DOI] [PubMed] [Google Scholar]
- Koole SL, Jostmann NB (2004) Getting a grip on your feelings: effects of action orientation and external demands on intuitive affect regulation. J Pers Soc Psychol 87:974. [DOI] [PubMed] [Google Scholar]
- Koski‐Jännes A (1994) Drinking‐related locus of control as a predictor of drinking after treatment. Addict Behav 19:491–495. [DOI] [PubMed] [Google Scholar]
- Ludwig F, Tadayon‐Manssuri E, Strik W, Moggi F (2013) Self‐efficacy as a predictor of outcome after residential treatment programs for alcohol dependence: simply ask the patient one question!. Alcohol Clin Exp Res 37:663–667. [DOI] [PubMed] [Google Scholar]
- Martinotti G, Di Nicola M, Tedeschi D, Callea A, Di Giannantonio M, Janiri L, Craving Study Group (2013) Craving Typology Questionnaire (CTQ): a scale for alcohol craving in normal controls and alcoholics. Compr Psychiatry 54:925–932. [DOI] [PubMed] [Google Scholar]
- Rehm J (2010) The risks associated with alcohol use and alcoholism. Alcohol Res Health 34:135–143. [PMC free article] [PubMed] [Google Scholar]
- Rohsenow DJ, O'Leary MR (1978) Locus of control research on alcoholic populations: a review. I. Development, scales, and treatment. Int J Addict 13:55–78. [DOI] [PubMed] [Google Scholar]
- Rotter JB (1966) Generalized expectancies for internal versus external control of reinforcement. Psychological monographs: General and Applied 80:1. [PubMed] [Google Scholar]
- Rotter JB (1990) Internal versus external control of reinforcement: a case history of a variable. Am Psychol 45:489. [Google Scholar]
- Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M (1993) Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption–II. Addiction 88:791–804. [DOI] [PubMed] [Google Scholar]