

ABSTRACT
Background
The impact of the 2003 residency duty hour reform on patient care remains a debated issue.
Objective
Determine the association between duty hour limits and mortality in patients with nervous system pathology.
Methods
Via a retrospective cohort study using the Nationwide Inpatient Sample from 2000–2010, the authors evaluated in-hospital mortality status in those with a primary discharge level diagnosis of disease or disorder of the nervous system. Odds ratios were calculated, and Bonferroni corrected P values and confidence intervals were determined to account for multiple comparisons relating in-hospital mortality with teaching status of the hospital by year.
Results
The pre-reform (2000–2002) and peri-reform (2003) periods revealed no significant difference between teaching and nonteaching hospital mortality (P > .99). The post-reform period (2004–2010) was dominated by years of significantly higher mortality rates in teaching hospitals compared to nonteaching hospitals: 2004 (P < .001); 2006 (P = .043); 2007 (P = .042); and 2010 (P = .003). However, data for 2005 (P ≥ .99), 2008 (P = .80), and 2009 (P = .09) did not show a significant difference in mortality.
Conclusions
Teaching and nonteaching hospital mortality was similar in patients with nervous system pathology prior to the duty hour reform. While nonteaching institutions demonstrated steadily declining mortality over the decade, teaching hospital mortality spiked in 2004 and declined at a more restricted rate. The timing of these changes could suggest a negative correlation of duty hour restrictions on outcomes of patients with nervous system pathology.
What was known and gap
The community continues to question the effect of the 2003 standards limiting resident duty hours, with studies to date producing conflicting findings.
What is new
An analysis of the relationship between duty hour limits and mortality in patients with disorders or diseases of the nervous system.
Limitations
Inability to rule out confounders or to select only teaching hospitals with neurology and neurological surgery programs.
Bottom line
The data showed higher mortality in teaching hospitals after implementation of the 2003 standards.
Introduction
The Accreditation Council for Graduate Medical Education (ACGME) implemented duty hour restrictions for resident physicians on July 1, 2003, and the policy changes put into place addressed several facets of resident work requirements (box).1–3 The primary aims of the new standards were to improve patient and resident safety. The decision was predicated on studies demonstrating that the reduction of fatigue and sleep deprivation among residents has beneficial effects, including increased quality of life, cognitive functioning, clinical performance, and the reduced risk of motor vehicle accidents.4–13 There is still debate as to whether the reform was entirely beneficial, as some studies found improvements in mortality rates following the duty hour policy changes and others demonstrated trends of stagnancy or increased mortality.
Box ACGME Resident Duty Hour Reform Policies of July 1, 2003
Resident Duty Hour Restrictions
80 hours per week limit (4-week average)
24-hour limit of continuous work
6-hour minimum allotted for transfer of care and educational activities
10 hours minimum off between periods of duty
1 in 7 days off of patient care
On call to be no more frequent than every third night
Abbreviation: ACGME, Accreditation Council for Graduate Medical Education.
Our study examined the association of duty hour restrictions on mortality in patients with primary discharge diagnoses of disorders or diseases of the nervous system. Furthermore, our study was designed to provide a novel approach to assess the effects of the changes in the ACGME standards. The existing literature examining the effect that the resident duty hour reform has had on patients dealing with neuropathology is rather limited. Furthermore, the studies that have attempted to assess this topic have predominantly focused on single site analyses of patients with specific diagnoses or procedures. Due to the current gaps in the literature, our study has examined the larger, more generalized cohort of patients by expanding the study sample to include all patients with neuropathology. The goal of this study was to determine if there was an association between the outcomes for this particular patient group and the ACGME standards modifications.
Methods
Data Source and Description
The Healthcare Cost and Utilization Project (HCUP) is a nationwide resource for patient data and is maintained by the Agency for Healthcare Research and Quality. They collect hospital discharge information from nonfederal, short-term, general, and specialty-specific hospitals.14 The Nationwide Inpatient Sample (NIS) approximates a 20% stratified sample of the hospitals represented in the HCUP database. These stratified data are weighted to generate nationally representative estimates. Individual records in the HCUP databases represent discrete hospital discharges and not necessarily discrete patients.
Since the data used have no patient identifiers, the University of Texas Health Science Center at San Antonio has exempted NIS data from Institutional Review Board review.
Case Definitions
Major diagnosis categories (MDCs) represent broad groups of diagnosis-related groups (DRGs) related to a particular organ or system, and not an etiology. DRGs group patients based on diagnosis, procedure, age, and other relevant criteria. Every hospital stay is assigned a single MDC and DRG.15 Our study examined the domain of patients with primary discharge diagnoses of Diseases and Disorders of the Nervous System (MDC01), which means that their neuropathology diagnosis was the primary reason for their admission deemed at the time of discharge. The HCUP-Net query system can be used to search the DRGs that compose MDC01 by year (http://hcupnet.ahrq.gov).
Hospitals included in this database were divided into 2 cohorts based on teaching status. The determination of teaching status was defined by the American Hospital Association Annual Survey, and teaching hospitals were defined as those that had American Medical Association–approved residency programs, were members of the Council of Teaching Hospitals and Health Systems, or had full-time equivalent intern- and resident-to-bed ratios of 0.25 or higher.15 HCUP limited patients examined to those 18 years of age or older, excluding pediatrics patients. The primary outcome was in-hospital mortality, which included all mortality that occurred in the hospitals, intermediate care facilities, skilled nursing facilities, and freestanding hospices.15
Study Sample
A retrospective cohort study was performed using the NIS from 2000 to 2010. The study period was selected to examine mortality trends in pre-reform (2000–2002), peri-reform (2003), and post-reform (2004–2010) periods in relation to the duty hour policy implementation. Adult patients with a primary discharge diagnosis of disease or disorder of the nervous system (n = 4 802 979) were included in the analysis. Data from hospitals with unknown teaching status were excluded.
Statistical Analysis
A univariate logistic regression model for complex survey designs (proc surveylogistic, SAS version 9.4, SAS Institute Inc, Cary, NC) was used to estimate the association between mortality and hospital teaching status by year. Patients with MDC01 were identified by querying the NIS database from 2000 to 2010. Pre-reform (2000–2002), peri-reform (2003), and post-reform (2004–2010) period trends were displayed graphically. Odds ratios relating in-hospital mortality with the teaching status of the hospital, 95% confidence intervals, and corresponding P values for no association were determined by year. Confidence intervals and P values were corrected for multiple comparisons with the Bonferroni method.
Results
Patient Cohort
Of the total of almost 87 million discharges, the final analysis included nearly 5 million with a primary disease or disorder of the nervous system. Over the 11-year period of these databases, a total of 10 367 unique hospitals were sampled, of which 1804 (17.4%) were teaching hospitals and 901 (8.7%) were teaching hospitals visited by the patients experiencing neurological conditions. Among those discharges occurring with neurological conditions, 50.5% (11 869 542 of 23 526 071) occurred at teaching hospitals, and this percentage ranged from 46.3% (984 073 of 2 127 522) in 2005 to 55.9% (1 281 307 of 2 293 759) in 2010. Discharges from hospitals with unknown teaching status were excluded.
Mortality Analysis
The respective mortality rates for teaching and non-teaching hospitals by year, along with P values, odds ratios, and 95% confidence intervals are displayed in the table. The pre-reform period (2000–2002) and peri-reform period (2003) revealed no difference between teaching and nonteaching hospital mortality in MDC01 admissions. The post-reform period saw teaching hospital mortality increase rapidly, rebound, and then decline at a slower rate compared to the steady decline observed in nonteaching hospitals (figure). Years 2005, 2008, and 2009 did not meet our study's standards for significance. The remaining post-reform years demonstrated significantly greater mortality rates in teaching hospitals compared to nonteaching hospitals.
Table.
Mortality Comparisons of MDC01 Between Teaching and Nonteaching Hospitals by Year

Figure.
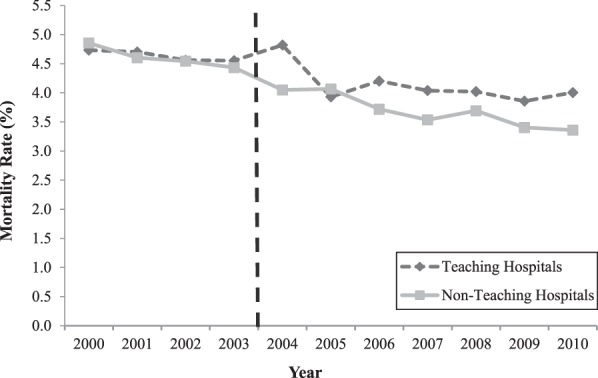
Nervous System Disease/Disorder Mortality by Hospital Teaching Status
Abbreviations: MDC, major diagnosis category; HCUP, Healthcare Cost and Utilization Project; NIS, Nationwide Inpatient Sample. Note: Mortality rates by hospital teaching status for patients with MDC01 were queried from HCUP-Net NIS data from 2000–2010. Values were plotted for each year of the study period. Teaching hospitals = light gray dashed line; nonteaching hospitals = dark gray solid line; duty hour restriction implementation = vertical dashed line.
Discussion
This study demonstrates a potential association between the 2003 duty hour changes and increased mortality in teaching hospitals versus nonteaching hospitals in primary discharge diagnoses involving nervous system pathology. In contrast, from 2000 to 2003, differences in mortality rates for these diagnoses were not observed. Over this decade, mortality declined for both types of hospitals.
The current literature details possible explanations for how the duty hour reform may have negatively affected patient care. Hutter and colleagues16 noted concerns regarding the professional development of future surgeons, as well as challenges transitioning from a patient-oriented mentality to one of a shift-worker. However, these concerns of diminished resident professionalism due to development of a “shift work” mentality remain debated in the literature as possibly being overstated.17 Other concerns include diminished continuity of care, more frequent resident handoffs, and a general reduction in a training physician's clinical experience.18–22 These potential challenges brought on by the duty hour restrictions may provide some explanation for the mortality trends observed in our study.
Although limited in quantity, there are several studies that have examined the duty hour reform's effects on specific nervous system pathology patient populations. Many of these studies have demonstrated worse patient outcomes following the duty hour reform, including neurological surgery trauma, craniotomy for meningiomas, spinal surgeries, brain tumors, and cerebrovascular neurological procedures.23–26 These authors stipulated that the training and performance of neurological surgery residents is particularly vulnerable to the limitations that the duty hour reform placed on them. Furthermore, Grady and colleagues18 suggested that the reform may have exchanged the risks of resident fatigue for those of an inexperienced neurological surgery workforce. In contrast, 1 study found no difference in acute ischemic stroke mortality after the implementation of the duty hour reform.27 While these studies individually examine very specific patient populations, cumulatively they may suggest that some patients are more susceptible than others to the obstacles the reform has placed on physicians.
This study has several limitations. The design allows merely the identification of an association between duty hour limits and mortality in patients with neuropathology diagnoses, and cannot attribute causality. Potential confounders include the tendency of teaching hospitals to have higher case complexity, to have patients with more comorbidities, and to have different demographic compositions. Additionally, not all teaching hospitals have accredited neurological surgery and/or neurology residency programs, and the NIS data limited our ability to identify these institutions.
Furthermore, variables such as severity of injury, chronicity, acuity, and comorbidities are not captured in this national database, thus confounding our ability to normalize for these variables. We attempted to add a novel perspective by using the broad patient cohort of MDC01; however, the generalization that subsequently occurs with this approach must be noted as a limitation due to the many unknowns regarding specific DRGs that may be driving the observed mortality fluctuations. Mortality may not necessarily be the best indicator for quality of care for every DRG, as benign diseases may never result in death regardless of the patient care. Future studies should attempt to account for these unknowns.
Conclusion
Prior to the implementation of the ACGME duty hour reform, the mortality rates of patients with nervous system pathology were comparable regardless of hospital teaching status in a national database that did not control for other differences between these hospitals. Following the reform, mortality rates for this patient population diverged between teaching and nonteaching institutions, with higher mortality rates observed in teaching hospitals for 4 of the next 7 years.
References
- 1. Nasca TJ, Day SH, Amis ES, Jr, , et al. The new recommendations on duty hours from the ACGME task force. N Engl J Med. 2010; 363 2: e3. [DOI] [PubMed] [Google Scholar]
- 2. ACGME. Report of the ACGME Work Group on Resident Duty Hours. Chicago, IL: ACGME; 2002. http://www.acgme.org/acWebsite/dutyHours/dh_wkgroupreport611.pdf. Accessed April 21, 2016. [Google Scholar]
- 3. ACGME. Statement of justification/impact for the final approval of common standards related to resident duty hours. 2003. http://www.acgme.org/DutyHours/lmpactStatement.pdf. Accessed April 21, 2016. [Google Scholar]
- 4. Arnedt J, Owens J, Crouch M, et al. Neurobehavioral performance of residents after heavy night call vs after alcohol ingestion. JAMA. 2005; 294 9: 1025– 1033. [DOI] [PubMed] [Google Scholar]
- 5. Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005; 352 2: 125– 134. [DOI] [PubMed] [Google Scholar]
- 6. Berkoff K, Rusin W. Pediatric house staff's psychological response to call duty. J Dev Behav Pediatr. 1991; 12 1: 6– 10. [PubMed] [Google Scholar]
- 7. Grantcharov TP, Bardram L, Peter FJ, et al. Laparoscopic performance after one night on call in a surgical department: prospective study. BMJ. 2001; 323 7323: 1222– 1223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Kapur N, House A. Job satisfaction and psychological morbidity in medical house officers. J R Coll Physicians Lond. 1997; 31 2: 162– 167. [PMC free article] [PubMed] [Google Scholar]
- 9. Leonard C, Fanning N, Attwood J, et al. The effect of fatigue, sleep deprivation and onerous working hours on the physical and mental wellbeing of pre-registration house officers. Ir J Med Sci. 1998; 167 1: 22– 25. [DOI] [PubMed] [Google Scholar]
- 10. Lingenfelser T, Kaschel R, Weber A, et al. Young hospital doctors after night duty: their task-specific cognitive status and emotional condition. Med Educ. 1994; 28 6: 566– 572. [DOI] [PubMed] [Google Scholar]
- 11. Marcus CL, Loughlin GM. Effect of sleep deprivation on driving safety in housestaff. Sleep. 1996; 19 10: 763– 766. [DOI] [PubMed] [Google Scholar]
- 12. Philibert I. Sleep loss and performance in residents and nonphysicians: a meta-analytic examination. Sleep. 2005; 28 11: 1392– 1402. [DOI] [PubMed] [Google Scholar]
- 13. Taffinder NJ, McManus IC, Gul Y, et al. Effect of sleep deprivation on surgeons' dexterity on laparoscopy simulator. Lancet. 1998; 352 9135: 1191. [DOI] [PubMed] [Google Scholar]
- 14. Health Cost and Utilization Project. Online HCUP overview course. http://www.hcup-us.ahrq.gov/overviewcourse.jsp. Accessed April 21, 2016. [Google Scholar]
- 15. Agency for Healthcare Research and Quality. HCUPnet definitions. http://hcupnet.ahrq.gov/HCUPnet.jsp?GoTo=HCUPnetDefinitions. Accessed April 21, 2016. [DOI] [PubMed] [Google Scholar]
- 16. Hutter MM, Kellogg KC, Ferguson CM, et al. The impact of the 80-hour resident workweek on surgical residents and attending surgeons. Ann Surg. 2006; 243 6: 864– 875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Szymczak JE, Brooks JV, Volpp KG, et al. To leave or to lie? Are concerns about a shift-work mentality and eroding professionalism as a result of duty hour rules justified? Milbank Q. 2010; 88 3: 350– 381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Grady MS, Batjer HH, Dacey RG. Resident duty hour regulation and patient safety: establishing a balance between concerns about resident fatigue and adequate training in neurosurgery. J Neurosurg. 2009; 110 5: 828– 836. [DOI] [PubMed] [Google Scholar]
- 19. Irani JL, Mello MM, Ashley SW, et al. Surgical residents' perceptions of the effects of the ACGME duty hour requirements 1 year after implementation. Surgery. 2005; 138 2: 246– 253. [DOI] [PubMed] [Google Scholar]
- 20. Jagannathan J, Vates GE, Pouratian N, et al. Impact of the Accreditation Council for Graduate Medical Education work-hour regulations on neurosurgical resident education and productivity. J Neurosurg. 2009; 110 5: 820– 827. [DOI] [PubMed] [Google Scholar]
- 21. Mukherjee S. A precarious exchange. N Engl J Med. 2004; 351 18: 1822– 1824. [DOI] [PubMed] [Google Scholar]
- 22. Ofri D. Residency regulations—resisting our reflexes. N Engl J Med. 2004; 351 18: 1824– 1826. [DOI] [PubMed] [Google Scholar]
- 23. Babu R, Thomas S, Hazzard MA, et al. Worse outcomes for patients undergoing brain tumor and cerebrovascular procedures following the ACGME resident duty-hour restrictions. J Neurosurg. 2014; 121 2: 262– 276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Babu R, Thomas S, Hazzard MA, et al. Morbidity, mortality, and health care costs for patients undergoing spine surgery following the ACGME resident duty-hour reform. J Neurosurg Spine. 2014; 21 4: 502– 515. [DOI] [PubMed] [Google Scholar]
- 25. Dumont TM, Tranmer BI, Horgan MA, et al. Trends in neurosurgical complication rates at teaching vs nonteaching hospitals following duty-hour restrictions. Neurosurgery. 2012; 71 5: 1041– 1046. [DOI] [PubMed] [Google Scholar]
- 26. Hoh BL, Neal DW, Kleinhenz DT, et al. Higher complications and no improvement in mortality in the acgme resident duty-hour restriction era: an analysis of more than 107,000 neurosurgical trauma patients in the nationwide inpatient sample database. Neurosurgery. 2012; 70 6: 1369– 1382. [DOI] [PubMed] [Google Scholar]
- 27. Alshekhlee A, Walbert T, DeGeorgia M, et al. The impact of Accreditation Council for Graduate Medical Education duty hours, the July phenomenon, and hospital teaching status on stroke outcomes. J Stroke Cerebrovasc Dis. 2009; 18 3: 232– 238. [DOI] [PubMed] [Google Scholar]