

Supplemental Digital Content is available in the text
Abstract
We aimed to obtain overall and regional estimates of hypertension prevalence, and to examine the pattern of this disease condition across different socio-demographic characteristics in low-and middle-income countries.
We searched electronic databases from inception to August 2015. We included population-based studies that reported hypertension prevalence using the current definition of blood pressure ≥140/90 mm Hg or self-reported use of antihypertensive medication. We used random-effects meta-analyses to pool prevalence estimates of hypertension, overall, by World Bank region and country income group. Meta-regression analyses were performed to explore sources of heterogeneity across the included studies.
A total of 242 studies, comprising data on 1,494,609 adults from 45 countries, met our inclusion criteria. The overall prevalence of hypertension was 32.3% (95% confidence interval [CI] 29.4–35.3), with the Latin America and Caribbean region reporting the highest estimates (39.1%, 95% CI 33.1–45.2). Pooled prevalence estimate was also highest across upper middle income countries (37.8%, 95% CI 35.0–40.6) and lowest across low-income countries (23.1%, 95% CI 20.1–26.2). Prevalence estimates were significantly higher in the elderly (≥65 years) compared with younger adults (<65 years) overall and across the geographical regions; however, there was no significant sex-difference in hypertension prevalence (31.9% vs 30.8%, P = 0.6). Persons without formal education (49.0% vs 24.9%, P < 0.00001), overweight/obese (46.4% vs 26.3%, P < 0.00001), and urban settlers (32.7% vs 25.2%, P = 0.0005) were also more likely to be hypertensive, compared with those who were educated, normal weight, and rural settlers respectively.
This study provides contemporary and up-to-date estimates that reflect the significant burden of hypertension in low- and middle-income countries, as well as evidence that hypertension remains a major public health issue across the various socio-demographic subgroups. On average, about 1 in 3 adults in the developing world is hypertensive. The findings of this study will be useful for the design of hypertension screening and treatment programmes in low- and middle-income countries.
INTRODUCTION
Hypertension drives the global burden of cardiovascular disease, being widely acknowledged as the most common cardiovascular disorder and number 1 risk factor for mortality.1–3 The occurrence of hypertension is increasing globally, with projections estimating a 30% increase in prevalence by the year 2025.4 However, owing to several factors such as the ongoing nutritional transition, increasing trends in sedentary lifestyle, and other modifiable risk factors, and inadequate health care systems, populations in low- and middle-income countries (LMICs) may bear a higher burden of the disease, compared with the global average. Projections estimate that three-quarters of the world's hypertensive population will reside in LMICs within the next decade.4 However, there is a dearth of evidence providing up-to-date estimates of the occurrence of hypertension and its determinants across the developing regions of the world. The existing systematic reviews have, hitherto, been country-specific,5 or focused on African populations.6,7 Therefore, we aimed to fill this gap in the evidence by providing overall and regional estimates of hypertension prevalence across LMICs and to examine the pattern of this disease across different socio-demographic characteristics.
METHODS
Protocol and Registration
The systematic review rational and methods were specified in advance and documented in a protocol, which was published in the PROSPERO register (CRD42013006162).8
Eligibility Criteria
We included population-based studies that reported crude prevalence estimates of hypertension in LMICs (see Table 1 for full inclusion and exclusion criteria).
TABLE 1.
Eligibility criteria

Information Sources and Search Strategy
We searched the following electronic databases from inception to August 2015: EMBASE, Ovid MEDLINE, and the WHO Global Cardiovascular Infobase for relevant articles. The search was conducted using the following medical subject heading (MeSH) terms and keywords: “hypertension” OR “blood pressure” OR “hypertens∗” AND “population-based” OR “etiology” OR “etiology” OR “prevalence” OR “epidemiolog∗” AND “low- and middle-income countries” OR “developing countries” (see Appendix 1 for the MEDLINE search strategy). We also scanned through cross-references of identified primary studies and review articles for eligible studies.
Study Selection
Three reviewers (AMS, CN, and OU) independently evaluated the eligibility of the studies obtained from the literature searches. All articles yielded by the database search were initially screened by their titles and abstracts to obtain studies that met our inclusion criteria. In cases of discrepancies, agreement was reached by consensus and by discussion with a fourth reviewer (SS).
Data Collection Process and Data Items
Three reviewers (AMS, CN, and OU) independently evaluated the methodological quality of each included study and extracted data using a piloted form; discrepancies were resolved by discussion with a fourth reviewer (SS). Data extracted included year of publication, country of origin, study design, sample size, sampling strategy, study period, setting (rural/urban), gender distribution, age group, mean age, body mass index (BMI) category, hypertension prevalence, diagnostic criteria for hypertension, confounders, smoking status, alcohol use, education and employment status. Countries were grouped by region and income according to World Bank9 development indicators. Age group, gender, BMI category, smoker status, alcohol use, and study setting were coded as dichotomous variables. We defined overweight/obesity as BMI ≥ 25 kg/m2. Total prevalence estimates of hypertension were calculated from studies providing only subgroup estimates. The total mean age in each study was also obtained from reports of this variable measure within subgroups.
Risk of Bias in Included Studies
Methodological quality entailed assessing the risk of bias for each study using a domain-based tool adapted from the Newcastle-Ottawa Scale (see Appendix 2, http://links.lww.com/MD/A543).10 The risk of bias in each study was classified as low, moderate, high or unclear across the following domains: selection of participants (selection bias), sample size justification (selection bias), outcome measurement (detection bias), and confounding adjustment.
Ethical Approval
Being a systematic review of published literature, no ethical approval was required for conducting this study. However, we ensured that all studies included in our review provided evidence of ethical approval and informed consent from all patients or respondents where required.
Statistical Analysis
We stabilized the raw proportions of participants with hypertension from each study using the Freeman–Tukey variant of the arcsine square root transformed proportion11 suitable for pooling proportions (see Appendix 3, http://links.lww.com/MD/A543). In performing the meta-analyses, we used the DerSimonian–Laird random-effects model12 due to anticipated variations in study population, methodologies, and stage of epidemic transition. We assessed heterogeneity among studies by inspecting the forest plots and using the chi squared test for heterogeneity with a 10% level of statistical significance, and using the I2 statistic, where we interpreted a value of 50% as representing moderate heterogeneity.13,14 We assessed the potential for publication bias by evaluating funnel plot asymmetry using Egger's test for regression asymmetry.15 Where there was evidence of publication bias, we used the “trim and fill” analysis of Duval and Tweedie16 to examine the potential impact of missed or unpublished studies on the pooled estimates of hypertension prevalence.
The potential modifying effects of various study-level variables on the overall prevalence of hypertension were explored using subgroup and univariable random-effects meta-regression analyses: year of publication, age group, gender, education status, employment status, smoker status, alcohol use, overweight/obesity, country income groups,9 and study settings (urban, rural or mixed).
Hypertension prevalence estimates were reported with 95% confidence intervals (CIs). All P values were exact (except where P < 0.0001)14 and 2-tailed; P < 0.05 was considered statistically significant. Analyses were conducted using Stata version 12 for Windows (Stata Corp, College Station, TX) using the “metaprop” rountine.17 This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (http://www.prisma-statement.org).18 The PRISMA checklist is provided in Appendix 4, http://links.lww.com/MD/A543.
RESULTS
Study Flow and Characteristics
Figure 1 shows the study selection flow. The literature search yielded 3315 articles. After an initial screening process, 404 articles were selected for critical reading. One hundred and sixty two (162) studies were excluded for not meeting the selection criteria, leaving 242 studies (from 239 publications),19–254 which we considered eligible for inclusion in this systematic review. Table 2 and eTables 1–6, http://links.lww.com/MD/A543 summarize the characteristics of the included studies by region.
FIGURE 1.

PRISMA flow diagram showing study selection.
TABLE 2.
Characteristics of Included Studies by Regions

Studies comprised data on 1,494,609 participants (52% females) from 45 countries (Table S7, http://links.lww.com/MD/A543). Most of the studies were conducted in India (n = 50 studies; 20.7%), Brazil (n = 26; 10.7%), Nigeria (n = 25; 10.3%), and China (n = 22; 9.1%). Although a third of the included studies (n = 74; 30.6%) originated from sub-Saharan African countries, all 6 regions, including East Asia and Pacific, Europe and Central Asia, Latin America and Caribbean, Middle East and North Africa, South Asia, and sub-Saharan Africa were represented in our review. Figure 2 showcases country-wide differences among the 45 countries included in this study.
FIGURE 2.

Prevalence estimates of hypertension by region, income group, and study setting.
All articles were population-based observational studies. Hypertension was diagnosed as blood pressure (BP) ≥140/90 mm Hg in all but 3 studies where assessment was based on self-reported physician diagnoses alone.58,62,70 The mean age overall was 45.9 ± 12.1 years with participants from Europe and Central Asia being the youngest (35.7 ± 11.4 years) and those from East Asia and Pacific being the oldest (51.7 ± 9.1 years). Participants in the Middle East and North Africa had the highest estimates of combined overweight/obesity (56.8% [95% CI 40.6–73.2]), whereas the lowest rates were found in the South Asia region (29.0% [95% CI 18.4–41.0]).
Risk of Bias of Included Studies
Summary of risk of bias assessment for each study is shown in Appendix 5, http://links.lww.com/MD/A543. Overall, 111 studies (46%) were assessed as having low risk of selection bias within the sampling domain, having selected participants randomly. Based on sample size justification, the risk of selection bias was also assessed as low in 73 studies (30%). Detection bias was low in 193 studies (80%) reporting the use of a validated tool for measuring blood pressure. However, assessment of hypertension was not blind in any of the included studies, consequently resulting in high risk of detection bias within this domain in all 242 studies.
Pooled Prevalence by Geographical Regions
The country-specific prevalence of hypertension is shown in Figure 2. All 242 studies reported the crude prevalence of hypertension and were included in meta-analysis. The reported hypertension ranged from 2.5% (95% CI 1.9–3.2)107 to 90% (95% CI 89.9–90.2)29 (both studies in India). The pooled hypertension prevalence for all studies yielded an estimate of 32.3% (95% CI 29.4–35.3). The I2 statistic was 99.9%, indicating substantial heterogeneity across the included studies. The contour-enhanced funnel plot for assessing publication bias is shown in eFigure 1, http://links.lww.com/MD/A543. The funnel plot appears symmetric and shows no evidence of publication bias.
The prevalence estimates of hypertension across regions, country income groups, and settings are shown in Figure 3. Subgroup analysis by region showed the highest prevalence estimate of hypertension in the Latin America and Caribbean region (39.1% [95% CI 33.1–45.2]) (eFigure 2, http://links.lww.com/MD/A543)29,35,46–73 whereas the Middle East and North Africa region had the lowest prevalence (26.9% [95% CI 19.3–35.3]) (eFigure 3, http://links.lww.com/MD/A543).74–81
FIGURE 3.

Country-specific hypertension prevalence.
The East Asia and Pacific region (35.7% [95% CI 32.2–39.4]) (eFigure 4, http://links.lww.com/MD/A543)19–37 and Europe and Central Asian region (32.0% [95% CI 28.0–37.0]) were second and third respectively to the Americas (eFigure 4, http://links.lww.com/MD/A543 and eFigure 5, http://links.lww.com/MD/A543). Prevalence estimates for the Sub-Saharan Africa38–45 and South Asia29,35,82–108 regions are shown respectively in eFigure 6, http://links.lww.com/MD/A543 and eFigure 7, http://links.lww.com/MD/A543.
Pooled Prevalence by Country Income Groups
Upper middle income countries had a higher prevalence of hypertension (37.8% [95% CI 35.0–40.6]), compared with lower middle income (31.1% [95% CI 26.1–36.4]) and low-income countries (23.1% [95% CI 20.1–26.2]) (eFigures 8–10, http://links.lww.com/MD/A543). Hypertension prevalence was also higher among populations in urban settings (32.7% [95% CI 30.4–35.0]), compared with populations in rural settings (25.2% [95% CI 20.9–29.8]) (eFigures 11 and 12, http://links.lww.com/MD/A543).29–31,40,42,76,78,80,99,111,113,121,128,131,135,136,140,146
Pooled Prevalence by Participants’ Socio-Demographic Characteristics
We summarized the patterns of hypertension across different socio-demographic characteristics for each region in Table 3. In all regions except the Middle East and North Africa region, where no data on hypertension prevalence was reported for the elderly (≥ 65 years), the proportion of hypertension was substantially higher among adults ≥ 65 years, compared to adults < 65 years (mean prevalence 65.6% [95% CI 53.6–75.0] vs 28.7% [95% CI 21.8–37.6], P < 0.00001).22,23,30,31,40,42,46,55,56,59,61,62,65,66,69,70,84,90,91,95,97,99,101,113,117,121,122,128,131,134–136,146,147 Nonetheless, hypertension prevalence in the Middle East and North Africa region was reportedly high among adults < 65 years (32.4% [95% CI 18.7–47.9]).78,79
TABLE 3.
Prevalence Estimates of Hypertension by Region Across Socio-demographic Characteristics also Showing Risk of Bias in Included Studies

Although prevalence of hypertension in men overall (33%) was slightly higher compared with women (31.2%), this difference was not statistically significant (P = 0.76). Additionally, no significant sex-deference in hypertension prevalence was observed by region.
We found higher proportions of hypertension among nonsmokers compared to smokers in Europe and Central Asia, Latin America and Caribbean, and Middle East and North Africa regions. Whereas the proportions of hypertension was higher amongst smokers compared to nonsmokers in East Asia and Pacific, South Asia, and Sub-Saharan Africa regions. Alcohol use data was not reported in any study originating from countries in the Middle East and North Africa or the East Asia and Pacific regions. With the exception of the sub-Saharan Africa region, hypertension rates were comparable between nondrinkers and current drinkers; nondrinkers had a substantially higher proportion of hypertension compared to current drinkers in sub-Saharan Africa (32.0% [95% CI 20.9–44.2] vs 21.7% [95% CI 14.6–29.6], P < 0.00001).113,121,131,135,136,140 Importantly, hypertension rates were consistently higher among overweight/obese participants, compared to normal weight persons across all regions (mean prevalence 46.4% [95% CI 33.1–60.7] vs 26.3% [95% CI 15.8–37.8], P < 0.00001).30,33,41,44,47,55,56,61,62,65,66,69,78,85,90,97,99,106,113,117,128,131,134–136,140
With respect to study setting, prevalence estimates of hypertension were higher in urban communities, compared to participants in rural settings in the Latin America and Caribbean region (51.2% [95% CI 30.1–72.0] vs 42.8% [95% CI 26.1–60.4], P = 0.00017),29 East Asia and Pacific (51.2% [32.8–69.5] vs 47.5% [25.5–70.1], P < 0.00001), South Asia (35.9% [95% CI 19.1–54.7] vs 28.0% [95% CI 18.8–38.2], P < 0.00001),29,99 and Sub-Saharan Africa (34.9% [95% CI 23.0–47.8] vs 29.9% [95% CI 22.6–37.9], P = 0.017).111,113,121,128,131,135,136,140,146
Hypertension rates were also generally higher among the noneducated, compared to participants with a primary education (mean prevalence 50.2% [95% CI 30.4 – 69.3] vs 36.3% [95% CI 23.7–50.4], P < 0.00001) and participants with a secondary or tertiary education (mean prevalence 25.0% [95% CI 18.8 – 31.9], P < 0.00001).22,30,31,33,40,41,44,47,55,56,61,65,66,69,70,76,79,81,97,99,106,113,117,121,128,131,134,136,140,146,147
Factors Associated With the Overall Hypertension Prevalence
The results of the meta-regression analyses showed that age (coefficient + 0.04 [95% CI 0.03–0.05], P < 0.0001) (Fig. 4), overweight/obesity (coefficient + 0.02 [95% CI 0.01–0.03] P = 0.001) (Fig. 5), and educational status (coefficient + 0.01 [95% CI 0.001–0.02] P = 0.049) (Fig. 6) accounted for significant heterogeneity in hypertension prevalence between studies. Given that <50% of the included studies had a low risk of sampling bias, we performed meta-regression analysis to determine if the observed heterogeneity in hypertension prevalence was partly influenced by variations in population sampling between studies; our analysis showed no statistically significant effect (coefficient + 0.11 [95% CI −0.04–0.26], P = 0.14).
FIGURE 4.

Meta-regression of hypertension against age.
FIGURE 5.
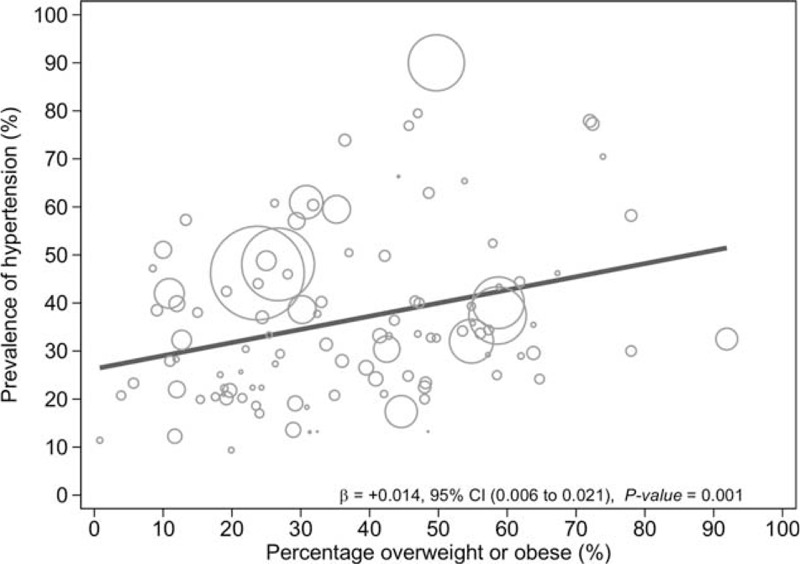
Meta-regression of hypertension prevalence against overweight/obesity.
FIGURE 6.
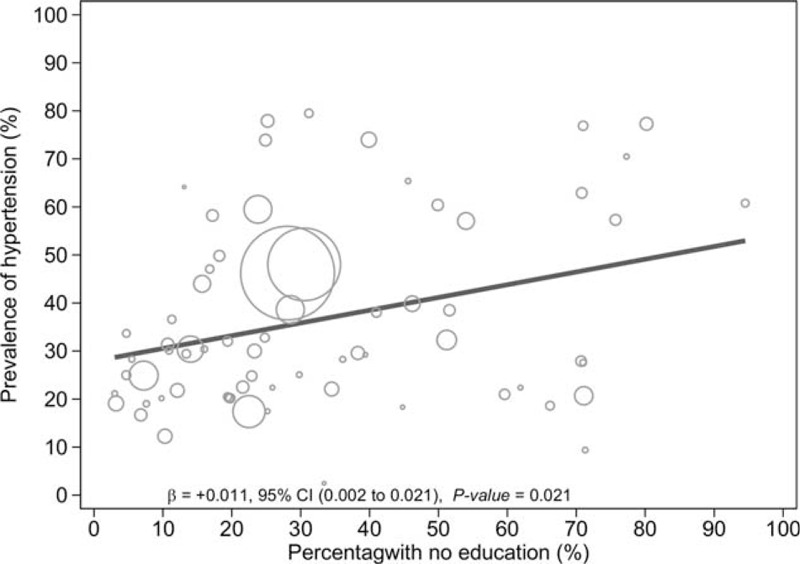
Meta-regression of hypertension against education.
DISCUSSION
Main Findings
To our knowledge, this is the first systematic review on hypertension prevalence and its socio-demographic patterning in the developing world. Our review suggests that hypertension remains an important public health problem in LMICs, with 1 in 3 persons affected by the disease. Our findings also suggest that older age and increased body weight may be consistent predictors of hypertension across LMICs, given that prevalence estimates of hypertension were substantially higher in the elderly, compared with younger adults, and in overweight/obese persons, compared with normal weight persons. Lower educational status was also found to be associated with a high prevalence of hypertension; however, this association was not consistent across counties and geographical regions.
Our results correspond to Kearney and colleagues4 who found hypertension prevalence to be highest among Latin America and Caribbean populations, compared to other regions, based on data collected prior to 2001. This broadly suggests that hypertension prevalence estimates in the Latin America and Caribbean region may have driven the burden of the disease in the developing world for more than a decade. Hypertension rates were more likely to be higher in upper middle income countries than in lower middle income countries, and the latter more likely to be higher compared to low-income countries. We hypothesize that a temporal relationship exists between increasing levels of affluence and urbanization and raised blood pressure. This plausibly accounts for the graded rise in hypertension rates, which is characteristic of the epidemiological transition within urban societies in resource-limited settings.241,242 The higher prevalence of hypertension in urban settings compared to rural settings, as shown in our study and in previous reviews,6,243 are also in accordance with this hypothesis.
Our findings also suggest that hypertension may be associated with socio-economic inequalities in LMICs: prevalence estimates for hypertension were inversely proportional to educational attainment, resulting in a downward socioeconomic gradient for hypertension. Evidence of health inequalities associated with hypertension in LMICs are not uncommon.244,245 Although men and women hypertension prevalence estimates were comparable overall, the slightly higher prevalence in men than women observed in our results are consistent with previous systematic reviews.6,243 This slight difference may be explained by evidence confirming male predilection for cardiovascular problems in the middle-age group, which attenuates in older adults as exemplified by an increased risk of cardiovascular diseases among post-menopausal women.244,245 Nonetheless, we observed a significant direct association between mean age and hypertension prevalence, which may be attributed to age-related structural changes in blood vessels which potentially cause narrowing of the vascular lumen, and consequently increasing blood pressure, as have been reported in previous studies.246–248 This hypothesis may also explain the unusually high prevalence estimates of hypertension (>70%) observed in a few of the included studies,30,32,232 given that the sampled population in these studies comprised mostly of the elderly.
Our review confirms that smoking is an independent risk factor for hypertension in Asian communities,249,250 given that smokers were more likely than nonsmokers to be hypertensive in the Asia regions alone.
Nevertheless, the higher proportions of hypertension among nonsmokers compared to smokers in the non-Asia regions may be attributed to smokers erroneously self-reporting their smoker status as nonsmokers in some of the included studies. Whereas this argument may account for the higher prevalence of hypertension among nondrinkers, compared to drinkers, in the sub-Saharan Africa region, it is also important to emphasize that nonsmokers and nondrinkers alike may engage in other harmful behaviors known to increase the risk of hypertension. Obviously, we cannot rule out the potential of reverse causation in cross-sectional studies, as it is possible that both nonsmokers and nondrinkers may have quit these harmful behaviors due to underlying medical conditions.251 However, it is important to state that we were not able to separate never smokers and never drinkers from exsmokers and exdrinkers in most of the included studies.
The association between combined overweight/obesity and hypertension shown in our results exemplify the role of excess body weight in hypertension prevalence, which has been long recognized and consistent across numerous observational and trial data.252–256
Study Limitations and Strengths
We acknowledge that the overall quality of the included studies was moderate at best, especially given that more than a third of the studies (39%) were assessed as having high risk of sampling bias. However, as shown using meta-regression analysis, we emphasize that the high rates of sampling bias had no undue impact on the overall hypertension prevalence.
High amounts of heterogeneity across the included studies were another limitation of our study. Prevalence estimates from different regions were pooled in this meta-analysis, and as expected, high heterogeneity between studies was found in the meta-analyses. A substantial amount of the heterogeneity across studies was explained by such factors as differences in population characteristics and study methodologies. Nonetheless, as affirmed by previous evidence, meta-analyses are the preferred options to narrative syntheses for interpreting the results in a review, even in spite of the presence of a considerable amount of heterogeneity.257 Heterogeneity appeared to be the norm rather than exception in published meta-analyses of observational studies, in which case, it should be expected and quantified appropriately.258 Although we found some evidence of publication bias, it has been documented that tests of publication bias may lead to false-positive results in the presence of significant heterogeneity.257,259 Nonetheless, the “trim and fill” analysis revealed that the presence of publication bias had no significant impact on the overall prevalence of hypertension. Although we might have missed some potentially relevant studies; however, this systematic review arguably constitutes the largest study on hypertension prevalence in the resource-limited settings, comprising >1 million participants. In addition, we speculate that nonsmokers and nondrinkers may potentially be at risk of hypertension due to other health-damaging behaviors; our study therefore highlights the importance of expatiating on other lifestyle variables as potential correlates of hypertension and other cardiovascular conditions. For example, we were not able to examine the potential impact of differential dietary patterns and dietary salt intake on the observed variations in hypertension prevalence across countries. It is likely that differences in average dietary salt intake at the population level may contribute to some of the observed variations in hypertension prevalence across countries and world regions.259–261
In spite of the aforementioned limitations, the review's strengths are important. We conducted comprehensive searches of databases to ensure that all relevant publications were identified. We also reduced potential bias in the conduct of this review by having the authors independently scan through the search output and extract the data. In addition, there was reasonable coverage of evidence for most geographic regions, such as South Asia and sub-Saharan Africa; these regions were well represented by a sufficient number of studies with large sample size, which allows for generalizability of the results across these geographic regions.
Implications of the Results
The elderly, overweight/obese, noneducated and urban settlers present opportunities for targeted health promotion and preventive interventions in LMICs. Given the high burden of infectious diseases in these countries, it might be economically justified to implement intervention programs for hypertension in higher-risk populations alone. However, the occurrence of hypertension in the general population remains unacceptably high, which poses an ethical dilemma to relying on high-risk strategies only in these settings; countries in the Middle East and North Africa region may even not have sufficient evidence to implement public health interventions in certain high-risk populations such as the elderly.
Health inequalities associated with hypertension have been recognized as an important public health issue in low- and middle-income countries.244,245,262 Addressing the wider social determinants of the disease is therefore crucial to its control in these countries. Failure to address these issues portends additional threats to the sustainability of public health infrastructure, especially alongside the prevailing effects of infectious disease epidemics.
Population-wide strategies such as reduction in dietary salt intake from processed foods are warranted in these low-resource settings, because they have been proven to be cost-effective means to shift blood pressure distribution at the population level, thus reducing the burden of cardiovascular disease associated with the epidemic of hypertension.263–268 Specifically, population-wide salt reduction through legislation, voluntary agreements with food industries and mass media campaigns are evidence-based cost-effective strategies for reducing hypertension prevalence in low- and middle-income countries, potentially preventing millions of years lost to the disease as a result of ill-health, disability or premature death.269 The absence of studies targeting the elderly in the Middle East and North Africa region also emphasizes the need for further research into resident high-risk subgroups. Hypertension among the elderly is likely to be a significant public health problem in the region considering that prevalence estimates in the young and middle-age are also high.
In conclusion, this study provides contemporary and up-to-date estimates that reflect the significant burden of hypertension and evidence that hypertension remains a major public health issue in LMICs. On average, about one-third of the adult population in these countries are hypertensive. However, this evidence originates from studies limited by high risk of selection bias and substantial between-study variations in the results. Nonetheless, we provide the most comprehensive evidence and first pooled analyses on hypertension prevalence in the developing world. There is a need for studies to accurately predict future trends of hypertension prevalence estimates in low- and middle-income countries. Additionally, future studies should explore alternative techniques to address heterogeneity, such as disease mapping or hierarchical modeling. The findings of this study would be useful for the design of hypertension screening and treatment programs in LMICs.
Supplementary Material
Footnotes
Abbreviations: BMI = body mass index, CI = confidence interval, LMICs = low- and middle-income countries, MeSH = Medical Subject Heading, mm Hg = millimetres of mercury, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-analyses, WHO = World Health Organization.
Authors’ Contributions: all authors contributed to the study concept and design. AMS, CN, and OU analyzed and interpreted the data. AMS and CN prepared the first draft of the article. All authors revised it critically and approved final submission.
Funding Statement: CUN acknowledges support from the University of Warwick Chancellor's Scholarship (ID 1160088). OAU acknowledges support from the Marie Curie International Postdoc Fellowship Grant (2012-0064). The funding sources had no role in the design, conduct, and reporting of the study.
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Mathers C, Stevens G, Mascarenhas M. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva: World Health Organization; 2009. [Google Scholar]
- 2.World Heart Federation. 2015. Cardiovascular disease risk factors. [online] Available at: http://www.world-heart-federation.org/cardiovascular-health/cardiovascular-disease-risk-factors/(Accessed 18/05/2015). [Google Scholar]
- 3.World Health Organization. 2015. Top ten causes of death. [online] Available at: http://www.who.int/mediacentre/factsheets/fs310/en/(Accessed 17/05/2015). [Google Scholar]
- 4.Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension: analysis of worldwide data. Lancet 2005; 365:217–223. [DOI] [PubMed] [Google Scholar]
- 5.Picon RV, Fuchs FD, Moreira LB, et al. Prevalence of hypertension among elderly persons in urban Brazil: a systematic review with meta-analysis. Am J Hypertens 2013; 26:541–548. [DOI] [PubMed] [Google Scholar]
- 6.Addo J, Smeeth L, Leon DA. Hypertension in sub-Saharan Africa: a systematic review. Hypertension 2007; 50:1012–1018. [DOI] [PubMed] [Google Scholar]
- 7.Adeloye D, Basquill C. Estimating the prevalence and awareness rates of hypertension in Africa: a systematic analysis. PLoS ONE 2014; 9:1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sarki AM, Uthman OA, Kandala N-B, Stranges S, Nduka C. Prevalence of hypertension in low-and middle-income countries: a systematic review. PROSPERO 2013: CRD42013006162. [online] Available at: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42013006162(Accessed 12/05/2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.World Bank Countries and Economies. Geneva: The World Bank Group; 2014. [Google Scholar]
- 10.Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute; 2014. [Google Scholar]
- 11.Miller JJ. The Inverse of the Freeman-Tukey double arcsine transformation. Am Stat 1978; 32:138. [Google Scholar]
- 12.Dersimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7:177–188. [DOI] [PubMed] [Google Scholar]
- 13.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21:1539–1558. [DOI] [PubMed] [Google Scholar]
- 14.Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003; 327:557–560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Egger M, Davey SG, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997; 315:629–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Duval S, Tweedie R. A non-parametric “Trim and Fill” method of accounting for publication bias in meta-analysis. J Am Stat Ass 2000; 95:89–98. [Google Scholar]
- 17.Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health 2014; 72:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009; 339:b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shmulewitz D, Auerbach SB, Lehner T, et al. Epidemiology and factor analysis of obesity, type II diabetes, hypertension, and dyslipidemia (syndrome X) on the Island of Kosrae, Federated States of Micronesia. Hum Hered 2001; 51:8–19. [DOI] [PubMed] [Google Scholar]
- 20.Wu L, He Y, Jiang B, et al. Trends in prevalence, awareness, treatment and control of hypertension during 2010 in an urban elderly population of China. PLoS ONE 2015; 10:e0132814.doi:101371/journal pone 0132814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gu D, Reynolds K, Wu X, et al. Prevalence, awareness, treatment, and control of hypertension in China. Hypertension 2002; 40:920–927. [DOI] [PubMed] [Google Scholar]
- 22.Lim TO, Morad Z. Prevalence, awareness, treatment and control of hypertension in the Malaysian adult population: results from the national health and morbidity survey 1996. Singapore Med J 2004; 45:20–27. [PubMed] [Google Scholar]
- 23.Minh HV, Byass P, Chuc NT, et al. Gender differences in prevalence and socioeconomic determinants of hypertension: findings from the WHO STEPs survey in a rural community of Vietnam. J Hum Hypertens 2006; 20:109–115. [DOI] [PubMed] [Google Scholar]
- 24.Rampal L, Rampal S, Azhar MZ, et al. Prevalence, awareness, treatment and control of hypertension in Malaysia: a national study of 16,440 subjects. Public Health 2008; 122:11–18. [DOI] [PubMed] [Google Scholar]
- 25.Sun Z, Zheng L, Xu C, et al. Prevalence of prehypertension, hypertension and, associated risk factors in Mongolian and Han Chinese populations in Northeast China. Int J Cardiol 2008; 128:250–254. [DOI] [PubMed] [Google Scholar]
- 26.Zhang X, Zhu M, Dib HH, et al. Knowledge, awareness, behaviour (KAB) and control of hypertension among urban elderly in Western China. Int J Cardiol 2009; 137:250–254. [DOI] [PubMed] [Google Scholar]
- 27.Lee S-A, Cai H, Yang G, et al. Dietary patterns and blood pressure among middle-aged and elderly Chinese men in Shanghai. Br J Nutri 2010; 104:265–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Swaddiwudhipong W, Mahasakpan P, Limpatanachote P, et al. Correlations of urinary cadmium with hypertension and diabetes in persons living in cadmium-contaminated villages in north-western Thailand: a population study. Environ Res 2010; 110:612–616. [DOI] [PubMed] [Google Scholar]
- 29.Thuy AB, Blizzard L, Schmidt MD, et al. The association between smoking and hypertension in a population-based sample of Vietnamese men. J Hypertens 2010; 28:245–250. [DOI] [PubMed] [Google Scholar]
- 30.Prince MJ, Ebrahim S, Acosta D, et al. Hypertension prevalence, awareness, treatment and control among older people in Latin America, India and China: a 10/66 cross-sectional population-based survey. J Hypertens 2012; 30:177–187. [DOI] [PubMed] [Google Scholar]
- 31.Ha DA, Goldberg RJ, Allison JJ, et al. Prevalence, awareness, treatment, and control of high blood pressure: a population-based survey in Thai Nguyen, Vietnam. PLoS ONE 2013; 8:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kiau HB, Kaur J, Nainu BM, et al. Prevalence, awareness, treatment and control of hypertension among the elderly: the 2006 National health and morbidity survey III in Malaysia. Med J Malaysia 2013; 68:332–337. [PubMed] [Google Scholar]
- 33.Amiri M, Majid HA, Hairi FM, et al. Prevalence and determinants of cardiovascular disease risk factors among the residents of urban community housing projects in Malaysia. BMC Public Health 2014; 14 Suppl 3:1–9.S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Fan L, Feng SX, Han B, et al. Prevalence awareness, treatment and control of hypertension in Henan Province, China. Aust J Rural Health 2014; 22:264–269. [DOI] [PubMed] [Google Scholar]
- 35.Feng XL, Pang M, Beard J. Health system strengthening and hypertension awareness, treatment and control: data from the China Health and Retirement Longitudinal Study. Bull World Health Organ 2014; 92:29–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lloyd-Sherlock P, Beard J, Minicuci N, et al. Hypertension among older adults in low-and middle-income countries: prevalence, awareness and control. Int J Epidemiol 2014; 43:116–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Nguyen TP, Schuiling-Veninga CC, Nguyen TB, et al. Models to predict the burden of cardiovascular disease risk in a rural mountainous region of Vietnam. ViHRI 2014; 3C:87–93. [DOI] [PubMed] [Google Scholar]
- 38.Wang X, Yang F, Bots ML, et al. Prevalence and clustering of cardiovascular risk factors in adults in Northeast China. Heart Asia 2014; 6:122–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Zhao Q, Gu D, Lu F, et al. Blood pressure reactivity to the cold pressure test predicts hypertension among Chinese adults: the GenSalt study. Am J Hypertens 2015; doi:101093/ajh/hpv035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Hou Z, Meng Q, Zhang Y. Hypertension prevalence, awareness, treatment, and control following China's healthcare reform. Am J Hypertens 2015; doi:101093/ajh/hpv125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Chen L, Zong Y, Wei T, et al. Prevalence, awareness, medication, control, and risk factors associated with hypertension in Yi ethnic group aged 50 years and over in rural China: the Yunnan minority eye study. BMC Public Health 2015; 15:383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Li G, Hu H, Dong Z, et al. Urban and suburban differences in hypertension trends and self-care: three population-based cross-sectional studies from 2005–201. PLoS ONE 2015; 10:e0117999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Wang S, Liu Y, Li F, et al. A novel quantitative body shape score for detecting association between obesity and hypertension in China. BMC Public Health 2015; 15:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Guo J1, Zhu YC, Chen YP, et al. The dynamics of hypertension prevalence, awareness, treatment, control and associated factors in Chinese adults: results from CHNS 1991–2011. J Hypertens 2015; 33:1688–1696. [DOI] [PubMed] [Google Scholar]
- 45.Li D, Lv J, Liu F, et al. Hypertension burden and control in mainland China: analysis of nationwide data 2003-2012. Int J Cardiol 2015; 184:637–644. [DOI] [PubMed] [Google Scholar]
- 46.Gu H, Li W, Yang J, et al. Hypertension prevalence, awareness, treatment and control among Han and four ethnic minorities (Uygur, Hui, Mongolian and Dai) in China. J Hum Hypertens 29:555–560. [DOI] [PubMed] [Google Scholar]
- 47.Lu K, Ding R, Tang Q, et al. Association between self-reported global sleep status and prevalence of hypertension in Chinese adults: data from the Kailuan community. Int J Environ Res Public Health 2015; 12:488–503.doi:103390/ijerph120100488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ke L, Ho J, Feng J, et al. Prevalence, awareness, treatment and control of hypertension in Macau: results from a cross-sectional epidemiological study in Macau, China. Am J Hypertens 2015; 28:159–165. [DOI] [PubMed] [Google Scholar]
- 49.Wei Q, Sun J, Huang J, et al. Prevalence of hypertension and associated risk factors in Dehui City of Jilin Province in China. J Hum Hypertens 2015; 29:64–68. [DOI] [PubMed] [Google Scholar]
- 50.Do HT, Geleijinse JM, Le MB, et al. National prevalence and associated risk factors of hypertension and prehypertension among Vietnamese adults. Am J Hypertens 2015; 28:89–97. [DOI] [PubMed] [Google Scholar]
- 51.Shapo L, Pomerleau J, McKee M. Epidemiology of hypertension and associated cardiovascular risk factors in a country in transition: a population based survey in Tirana City, Albania. J Epidemiol Community Health 2003; 57:734–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Onal AE, Erbil S, Ozel S, et al. The prevalence of and risk factors for hypertension in adults living in Istanbul. Blood Press 2004; 13:31–36. [DOI] [PubMed] [Google Scholar]
- 53.Mishra V, Arnold F, Semenov G, et al. Epidemiology of obesity and hypertension and related risk factors in Uzbekistan. Eur J Clin Nutr 2006; 60:1355–1366. [DOI] [PubMed] [Google Scholar]
- 54.Erem C, Hacihasanoglu A, Kocak M, et al. Prevalence of prehypertension and hypertension and associated risk factors among Turkish adults: Trabzon hypertension study. J Public Health 2008; 31:47–58. [DOI] [PubMed] [Google Scholar]
- 55.Dorobantu M, Darabont RO, Badila E, et al. Prevalence, awareness, treatment, and control of hypertension in Romania: results of the SEPHAR study. Int J Hypertens 2010; Article ID 970694:1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Altun B, Suleymanlar G, Utas C, et al. Prevalence, awareness, treatment and control of hypertension in adults with chronic kidney disease in Turkey: results from the CREDIT study. Kidney Blood Press Res 2012; 36:36–46. [DOI] [PubMed] [Google Scholar]
- 57.Dogan N, Toprak D, Demir S. Hypertension prevalence and risk factors among adult population in Afyonkarahisar region: a cross-sectional research. Anadolu Kardiyol Derg 2012; 12:47–52. [DOI] [PubMed] [Google Scholar]
- 58.Harhay MO, Harhay JS, Nair MM. Education, household wealth and blood pressure in Albania Armenia, Azerbaijan and Ukraine: findings from the demographic health surveys. Eur J Int Med 2013; 24:117–126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Supiyev A, Kossumov A, Utepova L, et al. Prevalence, awareness, treatment and control of arterial hypertension in Astana, Kazakhstan: a cross-sectional study. Public Health 2015. 1–6.xxx. [DOI] [PubMed] [Google Scholar]
- 60.Ordunez-Garcia PO, Espinosa-Brito AD, Cooper RS, et al. Hypertension in Cuba: evidence of a narrow black-white difference. J Hum Hypertens 1998; 12:111–116. [DOI] [PubMed] [Google Scholar]
- 61.Barreto SM, Passos VM, Firmo JO, et al. Hypertension and clustering of cardiovascular risk factors in a community in southeast Brazil—The Bambuí Health and Ageing Study. Arq Bras Cardiol 2001; 77:576–581. [DOI] [PubMed] [Google Scholar]
- 62.Freitas OC, Carvalho FR, Neves JM, et al. Prevalence of hypertension in the urban population of Catanduva, in the State of Sao Paulo, Brazil. Arq Bras Cardiol 2001; 77:16–21. [DOI] [PubMed] [Google Scholar]
- 63.Lorenzo C, Serrano-Rios M, Martinez-Larrad MT, et al. Prevalence of hypertension in Hispanic and non-Hispanic white populations. Hypertension 2002; 39:203–208. [DOI] [PubMed] [Google Scholar]
- 64.Matos AC, Ladeia AM. Assessment of cardiovascular risk factors in a rural community in the Brazilian State of Bahia. Arq Bras Cardiol 2003; 81:297–302.3. [DOI] [PubMed] [Google Scholar]
- 65.Gus I, Harzheim E, Zaslavsky C, et al. Prevalence, awareness, and control of systemic arterial hypertension in the State of Rio Grande do Sul. Arquivos Brasileiros de Cardiologia 2004; 83:429–433. [DOI] [PubMed] [Google Scholar]
- 66.Ordunez P, Munoz LB, Espinosa-Brito A, et al. Ethnicity, education, and blood pressure in Cuba. Am J Epidemiol 2005; 162:49–56. [DOI] [PubMed] [Google Scholar]
- 67.Almeida-Pititto B, Gimeno SG, Freire RD, et al. Leptin is not associated independently with hypertension in Japanese-Brazilian women. Braz J Med Biol Res 2006; 39:99–105. [DOI] [PubMed] [Google Scholar]
- 68.Jean-Baptiste ED, Larco P, Charles-Larco N, et al. Glucose intolerance and other cardiovascular risk factors in Haiti. Prevalence of diabetes and hypertension in Haiti (PREDIAH). Diabetes Metab 2006; 32:443–451. [DOI] [PubMed] [Google Scholar]
- 69.Lessa I, Magalhaes L, Araujo MJ, et al. Arterial hypertension in the adult population of Salvador (BA)—Brazil. Arq Bras Cardiol 2006; 87:683–692. [DOI] [PubMed] [Google Scholar]
- 70.Jardim PC, Gondim Mdo R, Monego ET, et al. High blood pressure and some risk factors in a Brazilian capital. Arq Bras Cardiol 2007; 88:398–403. [DOI] [PubMed] [Google Scholar]
- 71.Medina-Lezama J, Zea-Diaz H, Morey-Vargas OL, et al. Prevalence and patterns of hypertension in Peruvian Andean Hispanics: the PREVENCION study. J Am Soc Hypertens 2007; 1:216–225. [DOI] [PubMed] [Google Scholar]
- 72.Capilheira MF, Santos IS, Azevedo MR, et al. Risk factors for chronic non-communicable diseases and the CARMEN Initiative: a population-based study in the South of Brazil. Cad Saúde Pública 2008; 24:2767–2774. [DOI] [PubMed] [Google Scholar]
- 73.Ordunez P, Barcelo A, Bernal JL, et al. Risk factors associated with uncontrolled hypertension: findings from the baseline CARMEN survey in Cienfuegos, Cuba. J Hypertens 2008; 26:663–671. [DOI] [PubMed] [Google Scholar]
- 74.Sparrenberger F, Fuchs SC, Moreira LB, et al. Stressful life events and current psychological distress are associated with self-reported hypertension but not with true hypertension: results from a cross-sectional population-based study. BMC Public Health 2008; 8:1–9.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Longo GZ, Neves J, Luciano VM, et al. Prevalence of high blood pressure levels and associated factors among adults in Southern Brazil. Arq Bras Cardiol 2009; 93:360–366. [DOI] [PubMed] [Google Scholar]
- 76.Reichert FF, Azevedo MR, Breier A, et al. Physical activity and prevalence of hypertension in a population-based sample of Brazilian adults and elderly. Prev Med 2009; 49:200–204. [DOI] [PubMed] [Google Scholar]
- 77.Rodrigues SL, Baldo MP, Mill JG. Association of waist-stature ratio with hypertension and metabolic syndrome: population-based study. Arq Bras Cardiol 2009; 95:186–191. [DOI] [PubMed] [Google Scholar]
- 78.Rosario TM, Scala LC, Franca GV, et al. Prevalence, control and treatment of arterial hypertension in Nobres-MT. Arq Bras Cardiol 2009; 93:622–628. [DOI] [PubMed] [Google Scholar]
- 79.Diaz ME, Jimenez S, Garcia RG, et al. Overweight, obesity, central adiposity and associated chronic diseases in Cuban adults. MEDICC Review 2009; 11:23–28. [DOI] [PubMed] [Google Scholar]
- 80.Cipullo JP, Martin JF, Ciorlia LA, et al. Hypertension prevalence and risk factors in a Brazilian urban population. Arq Bras Cardiol 2010; 94:488–494. [DOI] [PubMed] [Google Scholar]
- 81.Nascente FM, Jardim PC, Peixoto Mdo R, et al. Arterial hypertension and its correlation with some risk factors in a small Brazilian town. Arq Bras Cardiol 2010; 95:502–509. [DOI] [PubMed] [Google Scholar]
- 82.Hofelmann DA, Antunes JL, Silva DA, et al. Is income area level associated with blood pressure in adults regardless of individual-level characteristics? A multilevel approach. Health Place 2012; 18:971–977. [DOI] [PubMed] [Google Scholar]
- 83.Kerkhoff AC, Moreira LB, Fuchs FD, et al. Association between hypertension and musculoskeletal complaints: a population-based study. J Hypertens 2012; 30:2112–2117. [DOI] [PubMed] [Google Scholar]
- 84.Lyra R, Silva RS, Montenegro RM, et al. High prevalence of arterial hypertension in a Brazilian Northeast population of low education and income level, and its association with obesity and metabolic syndrome. Rev Assoc Med Bras 2010; 58:209–214. [PubMed] [Google Scholar]
- 85.Mendes TA, Goldbaum M, Segri NJ, et al. Factors associated with the prevalence of hypertension and control practices among elderly residents of Sao Paulo city, Brazil. Cad Saude Publica 2013; 29:2275–2286. [DOI] [PubMed] [Google Scholar]
- 86.Selem SS, Castro MA, Cesar CL, et al. Validity of self-reported hypertension is inversely associated with the level of education in Brazilian individuals. Arq Bras Cardiol 2013; 100:52–59. [DOI] [PubMed] [Google Scholar]
- 87.Silva DA, Petroski EL, Peres MA. Accuracy and measures of association of anthropometric indexes of obesity to identify the presence of hypertension in adults: a population-based study in Southern Brazil. Eur J Nutr 2013; 52:237–246. [DOI] [PubMed] [Google Scholar]
- 88.Posso AJ, Borrel JA, Fontes F, et al. High blood pressure in Panama: prevalence, sociodemographic and biologic profile, treatment, and control (STROBE). Medicine 2014; 93:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Bernabe-Ortiz A, Carrillo-Larco RM, Gilman RH, et al. CRONICAS Cohort Study Group. J Epidemiol Community Health 2015; 0:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Bresan D, Bastos JL, Leite MS. Epidemiology of high blood pressure among the Kaingang people on the Xapecó Indigenous Land in Santa Catarina State, Brazil, 2013. Cad Saúde Pública 2015; 31:331–344. [DOI] [PubMed] [Google Scholar]
- 91.de Souza TCF, Perisse ARS, Moura M. Noise exposure and hypertension: investigation of a silent relationship. BMC Public Health 2015; 15:328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Unger A, Felzemburgh RD, Synder RE, et al. Hypertension in a Brazilian urban slum population. J Urban Health 2015; 92:446–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Vieira MC, Sperandei S, Reis A. Physical activity overcomes the effects of cumulative work time on hypertension prevalence among Brazilian taxi drivers. J Sports Med Phys Fitness 2015; [Epub ahead of print]. [PubMed] [Google Scholar]
- 94.Almeida RC, Dias DJ, Deguchi KT, et al. Prevalence and treatment of hypertension in urban and riverside areas in Porto Velho, the Brazilian Amazon. Postgrad Med 2015; 127:66–72. [DOI] [PubMed] [Google Scholar]
- 95.Ibrahim MM, Rizk H, Appel LJ, et al. Hypertension prevalence, awareness, treatment, and control in Egypt. Hypertension 1995; 26:886–890. [DOI] [PubMed] [Google Scholar]
- 96.Bahrami H, Sadatsafavi M, Pourshams A, et al. Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC Public Health 2006; 6:1–9.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Azimi-Nezhad M, Ghayour-Mobarhan M, Esmaeili HA, et al. Newly detected hypertension in an Iranian population: an epidemiological study. Asian Biomed 2009; 3:653–662. [Google Scholar]
- 98.Ramezani MA, Dastanpour M, Eshaghi SR, et al. Determinants of awareness, treatment and control of hypertension in Isfahan, Central Iran. Arch Med Sci 2009; 4:523–530. [Google Scholar]
- 99.Ebrahimi M, Mansournia MA, Haghdoost AA, et al. Social disparities in prevalence, treatment and control of hypertension in Iran: second national surveillance of risk factors of noncommunicable diseases, 2006. J Hypertens 2010; 28:1620–1629. [DOI] [PubMed] [Google Scholar]
- 100.Berraho M, El Achhab Y, Benslimane A, et al. Hypertension and type 2 diabetes: a cross-sectional study in Morocco (EPIDIAM Study). Pan Afr Med J 2012; 11:1–9.52. [PMC free article] [PubMed] [Google Scholar]
- 101.Modesti PA, Bamoshmoosh M, Rapi S, et al. Relationship between hypertension, diabetes and proteinuria in rural and urban households in Yemen. J Hum Hypertens 2013; 27:572–579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Veghari G, Sedaghat M, Maghsodlo S, et al. Impact of literacy on the prevalence, awareness, treatment and control of hypertension in adults in Golestan Province (northern Iran). Caspian J Intern Med 2013; 4:580–584. [PMC free article] [PubMed] [Google Scholar]
- 103.Khalifeh M, Salameh P, Hajje AA, et al. Hypertension in the Lebanese adults: impact on health related quality of life. J Epidemiol Global Health 2015; http://dxdoiorg/101016/jjegh201502003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Matar D, Frangieh AH, Abouassi S, et al. Prevalence, awareness, treatment, and control of hypertension in Lebanon. J Clin Hypertens 2015; 17:381–388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Sepanlou SG, Newson RB, Poustchi H, et al. Cardiovascular disease mortality and years of life lost attributable to non-optimal systolic blood pressure and hypertension in northeastern Iran. Arch Iran Med 2015; 18:144–152. [PMC free article] [PubMed] [Google Scholar]
- 106.Yazdanpanah L, Shahbazian H, Shahbazian H, et al. Prevalence, awareness and risk factors of hypertension in southwest of Iran. J Renal Inj Prev 2015; 4:51–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Gupta R, Sharma AK. Prevalence of hypertension and subtypes in an Indian rural population: clinical and electrocardiographic correlates. J Hum Hypertens 1994; 8:823–829. [PubMed] [Google Scholar]
- 108.Gupta R, Guptha S, Gupta VP, et al. Prevalence and determinants of hypertension in the urban population of Jaipur in western India. J Hypertens 1995; 13:1193–1200. [DOI] [PubMed] [Google Scholar]
- 109.Goel NK, Kaur P, Dr PC. Sen Memorial Award —1994. Role of various risk factors in the epidemiology of hypertension in a rural community of Varanasi district. Indian J Public Health 1996; 40:71–76. [PubMed] [Google Scholar]
- 110.Singh RB, Beegom R, Mehta AS, et al. Prevalence and risk factors of hypertension and age-specific blood pressures in five cities: a study of Indian women. Int J Cardiol 1998; 63:165–173. [DOI] [PubMed] [Google Scholar]
- 111.Malhotra P, Kumari S, Kumar R, et al. Prevalence and determinants of hypertension in an un-industrialised rural population of North India. J Hum Hypertens 1999; 13:467–472. [DOI] [PubMed] [Google Scholar]
- 112.Gurav RB, Kartikeyan S, Jadhav BS. Biochemical profile of hypertensive individuals in an urban community. Indian J Med Sci 2001; 55:663–668. [PubMed] [Google Scholar]
- 113.Swami HM, Bhatia V, Gupta M, et al. Population based study of hypertension among elderly in northern India. Public Health 2002; 116:45–49. [DOI] [PubMed] [Google Scholar]
- 114.Hazarika NC, Biswas D, Narain K, et al. Hypertension and its risk factors in tea garden workers of Assam. Natl Med J India 2002; 15:63–68. [PubMed] [Google Scholar]
- 115.Reddy NK, Kumar DN, Rayudu NV, et al. Prevalence of risk factors for coronary atherosclerosis in a cross-sectional population of Andhra Pradesh. Indian Heart J 2002; 54:697–701. [PubMed] [Google Scholar]
- 116.Gupta R, Gupta VP, Sarna M, et al. Prevalence of coronary heart disease and risk factors in an urban Indian population: Jaipur Heart Watch-2. Indian Heart J 2002; 54:59–66. [PubMed] [Google Scholar]
- 117.Bharucha NE, Kuruvilla T. Hypertension in the Parsi community of Bombay: a study on prevalence, awareness and compliance to treatment. BMC Public Health 2003; 3:1–6.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Deepa R, Shanthirani CS, Pradeepa R, et al. Is the ‘Rule of Halves’ in hypertension still valid? Evidence from the Chennai Urban Population Study. JAPI 2003; 51:153–157. [PubMed] [Google Scholar]
- 119.Hazarika NC, Biswas D, Mahanta J. Hypertension in the elderly population of Assam. J Assoc Phys India 2003; 51:567–573. [PubMed] [Google Scholar]
- 120.Shanthirani CS, Pradeepa R, Deepa R, et al. Prevalence and risk factors of hypertension in a selected south Indian population—The Chennai Urban Population Study. JAPI 2003; 51:20–27. [PubMed] [Google Scholar]
- 121.Gupta PC, Gupta R, Pednekar MS. Hypertension prevalence and blood pressure trends in 88 653 subjects in Mumbai. India J Hum Hypertens 2004; 18:907–910. [DOI] [PubMed] [Google Scholar]
- 122.Hazarika NC, Narain K, Biswas D, et al. Hypertension in the native rural population of Assam. Natl Med J India 2004; 17:300–304. [PubMed] [Google Scholar]
- 123.Ahmad K, Jafar TH. Prevalence and determinants of blood pressure screening in Pakistan. J Hypertens 2005; 23:1979–1984. [DOI] [PubMed] [Google Scholar]
- 124.Das SK, Sanyal K, Basu A. Study of urban community survey in India: growing trend of high prevalence of hypertension in a developing country. Int J Med Sci 2005; 2:70–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Siddiqui H, Anjum Q, Omair A, et al. Risk factors assessment for hypertension in a squatter settlement of Karachi. JPMA 2005; 55:390–392. [PubMed] [Google Scholar]
- 126.Prabhakaran D, Shah P, Chaturvedi V, et al. Cardiovascular risk factor prevalence among men in a large industry of northern India. Natl Med J India 2005; 18:59–65. [PubMed] [Google Scholar]
- 127.Thankappan KR, Shah B, Mathur P, et al. Risk factor profile for chronic noncommunicable diseases: results of a community-based study in Kerala, India. Indian J Med Res 2010; 131:53–63. [PubMed] [Google Scholar]
- 128.Mohan V, Deepa M, Farooq S, et al. Prevalence, awareness and control of hypertension in Chennai—The Chennai Urban Rural Epidemiology Study (CURES-52). JAPI 2007; 55:326–332. [PubMed] [Google Scholar]
- 129.Vaidya A, Pokharel PK, Nagesh S, et al. War veterans of Nepal and their blood pressure status: a population-based comparative study. J Hum Hypertens 2007; 21:900–903. [DOI] [PubMed] [Google Scholar]
- 130.Wijewardene K, Mohideen MR, Mendis S, et al. Prevalence of hypertension, diabetes and obesity: baseline findings of a population based survey in four provinces in Sri Lanka. Ceylon Med J 2005; 50:62–70. [DOI] [PubMed] [Google Scholar]
- 131.Reddy KS, Prabhakaran D, Jeemon P, et al. Educational status and cardiovascular risk profile in Indians. Proc Natl Acad Sci 2007; 104:16263–16268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Gupta R, Kaul V, Bhagat N, et al. Trends in prevalence of coronary risk factors in an urban Indian population: Jaipur Heart Watch-4. Indian Heart J 2007; 59:346–353. [PubMed] [Google Scholar]
- 133.Chaturvedi S, Pant M, Yadav G. Hypertension in Delhi: prevalence, awareness, treatment and control. Trop Doct 2007; 37:142–145. [DOI] [PubMed] [Google Scholar]
- 134.Agrawal VK, Bhalwar R, Basannar DR. Prevalence and determinants of hypertension in a rural community. MJAFI 2008; 64:21–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Yadav G, Chaturvedi S, Grover VL. Prevalence, awareness, treatment and control of hypertension among the elderly in a resettlement colony of Delhi. Indian Heart J 2008; 60:313–317. [PubMed] [Google Scholar]
- 136.Kusuma YS, Gupta SK, Pandav CS. Knowledge and perceptions about hypertension among neo- and settled-migrants in Delhi, India. CVD Prev Control 2009; 4:119–129. [Google Scholar]
- 137.Pednekar MS, Gupta R, Gupta PC. Association of blood pressure and cardiovascular mortality in India: Mumbai cohort study. Am J Hypertens 2009; 22:1076–1084. [DOI] [PubMed] [Google Scholar]
- 138.Pednekar MS, Hakama M, Hebert JR, et al. Association of body mass index with all-cause and cause-specific mortality: findings from a prospective cohort study in Mumbai (Bombay), India. Int J Epidemiol 2008; 37:524–535. [DOI] [PubMed] [Google Scholar]
- 139.Midha T, Idris M, Saran R, et al. Isolated systolic hypertension and its determinants: a cross-sectional study in the adult population of Lucknow district in north India. Indian J Community Med 2010; 35:89–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Bhardwaj R, Kandoria A, Marwah R, et al. Prevalence, awareness and control of hypertension in rural communities of Himachal Pradesh. JAPI 2010; 58:423–425. [PubMed] [Google Scholar]
- 141.Jonas JB, Nangia V, Matin A, et al. Prevalence, awareness, control, and associations of arterial hypertension in a rural Central India population: The Chennai India Eye and Medical Study. Am J Hypertens 2010; 23:347–350. [DOI] [PubMed] [Google Scholar]
- 142.Kinra S, Bowen LJ, Lyngdoh T, et al. Sociodemographic patterning of noncommunicable disease risk factors in rural India: a cross sectional study. BMJ 2010; 341:c4974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Kar SS, Thakur JS, Virdi NK, et al. Risk factors for cardiovascular diseases: is the social gradient reversing in northern India? Natl Med J India 2010; 23:206–209. [PubMed] [Google Scholar]
- 144.Chataut J, Adhikari RK, Sinha NP. The prevalence of and risk factors for hypertension in adults living in central development region of Nepal. Kathmandu Univ Med J 2011; 33:13–18. [DOI] [PubMed] [Google Scholar]
- 145.Norboo T, Stobdan T, Tsering N, et al. Prevalence of hypertension at high altitude: cross-sectional survey in Ladakh, Northern India 2007–2011. BMJ Open 2015; 5:e007026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Manimunda SP, Sugunan AP, Benegal V, et al. Association of hypertension with risk factors & hypertension related behaviour among the aboriginal Nicobarese tribe living in Car Nicobar Island, India. Indian J Med Res 2011; 133:287–293. [PMC free article] [PubMed] [Google Scholar]
- 147.Thrift AG, Evans RG, Kalyanram K, et al. Gender-specific effects of caste and salt on hypertension in poverty: a population-based study. J Hypertens 2011; 29:443–450. [DOI] [PubMed] [Google Scholar]
- 148.Bansal SK, Saxena V, Kandpal SD, et al. The prevalence of hypertension and hypertension risk factors in a rural Indian community: a prospective door-to-door study. J Cardiovasc Dis Res 2012; 3:117–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Bharati DR, Nandi P, Yamuna TV, et al. Prevalence and covariates of undiagnosed hypertension in the adult population of Puducherry, South India. Nepal J Epidemiol 2012; 2:191–199. [Google Scholar]
- 150.Dutta A, Ray MR. Prevalence of hypertension and pre-hypertension in rural women: a report from the villages of West Bengal, a state in the eastern part of India. Aust J Rural Health 2012; 20:219–225. [DOI] [PubMed] [Google Scholar]
- 151.Esam MS, Husain AS. Prevalence of prehypertension and hypertension in rural Bareilly. Nat J Med Res 2012; 2:291–294. [Google Scholar]
- 152.Prasad DS, Kabir Z, Dash AK, et al. Prevalence and predictors of adult hypertension in an urban eastern Indian population. Heart Asia 2012. 49–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Vaidya A, Pathak RP, Pandey MR. Prevalence of hypertension in Nepalese community triples in 25 years: a repeat cross-sectional study in rural Kathmandu. Indian Heart J 2012; 6402:128–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Vaidya A. Is ethnicity an important determinant of high blood pressure in Nepalese population? A community-based cross-sectional study in Dawakot, Nepal. Kathmandu Univ Med J 2012; 10:20–23.1. [DOI] [PubMed] [Google Scholar]
- 155.Meshram II, Arlappa N, Balkrishna N, et al. Prevalence of hypertension, its correlates and awareness among adult tribal population of Kerala state, India. J Postgrad Med 2012; 58:255–261. [DOI] [PubMed] [Google Scholar]
- 156.Samuel P, Antonisamy B, Raghupathy P, et al. Socioeconomic status and cardiovascular risk factors in rural and urban areas of Vellore, Tamil Nadu, South India. Int J Epidemiol 2012; 41:1315–1327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Kaur M. Blood pressure trends and hypertension among rural and urban Jat women of Haryana, India. Coll Antropol 2012; 36:139–144. [PubMed] [Google Scholar]
- 158.Jeemon P, Prabhakaran D, Goenka S, et al. Sentinel Surveillance in Industrial Populations Study Group. Impact of comprehensive cardiovascular risk reduction programme on risk factor clustering associated with elevated blood pressure in an Indian industrial population. Indian J Med Res 2012; 135:485–493. [PMC free article] [PubMed] [Google Scholar]
- 159.Gupta R, Sharma KK, Gupta A, et al. Persistent high prevalence of cardiovascular risk factors in the urban middle class in India: Jaipur Heart Watch-5. J Assoc Phys India 2012; 60:11–16. [PubMed] [Google Scholar]
- 160.Gupta R, Pandey RM, Misra A, et al. High prevalence and low awareness, treatment and control of hypertension in Asian Indian women. J Hum Hypertens 2012; 26:585–593. [DOI] [PubMed] [Google Scholar]
- 161.Chinnakali P, Mohan B, Upadhyay RP, et al. Hypertension in the elderly: prevalence and health seeking behaviour. N Am J Med Sci 2012; 4:558–562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Kokiwar PR, Gupta SS, Durge PM, et al. Prevalence of hypertension in a rural community of central India. J Assoc Phys India 2012; 60:26–29. [PubMed] [Google Scholar]
- 163.Borah PK, Shankarishan P, Hazarika NC, et al. Hypertension subtypes and angiotensin converting enzyme (ACE) gene polymorphism in Indian population. J Assoc Phys India 2012; 60:11. [PubMed] [Google Scholar]
- 164.Bhagyalaxmi A, Atul T, Shikha J. Prevalence of risk factors of non-communicable diseases in a district of Gujarat, India. J Health Popul Nutr 2013; 31:78–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Gupta R, Deedwania PC, Achari V, et al. Normotension, prehypertension, and hypertension in urban middle-class subjects in India: Prevalence, awareness, treatment, and control. Am J Hypertens 2013; 26:83–94. [DOI] [PubMed] [Google Scholar]
- 166.Khan RJ, Stewart CP, Christian P, et al. A cross-sectional study of the prevalence and risk factors for hypertension in rural Nepali women. BMC Public Health 2013; 13:1–10.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 167.Adhikari K, Gupta N, Koshy AK. Gender differences on risk factors of non-communicable diseases—A community based cross-sectional study in Central Nepal. JNHRC 2014; 12:88–93. [PubMed] [Google Scholar]
- 168.Zaman MM, Bhuiyan MR, Karim MN, et al. Clustering of non-communicable diseases risk factors in Bangladeshi adults: an analysis of STEPS survey 2013. Public Health 2015; 15:659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Gupta R, Sharma KK, Gupta BK, et al. Geographic epidemiology of cardiometabolic risk factors in middle class urban residents in India: cross-sectional study. J Global Health 2015; 5:010411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.Menon J, Vijaykumar N, Joseph JK, et al. Below the poverty line and non-communicable diseases in Kerala: The Epidemiology of Non-communicable Diseases in Rural Areas (ENDIRA) study. Int J Cardiol 2015; 187:519–524. [DOI] [PubMed] [Google Scholar]
- 171.Ranasinghe P, Cooray DN, Jayawardena R, et al. The influence of family history of hypertension on disease prevalence and associated metabolic risk factors among Sri Lankan adults. BMC Public Health 2015; 15:576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Rahman MM, Gilmour S, Akter S, et al. Prevalence and control of hypertension in Bangladesh: a multilevel analysis of a nationwide population-based survey. J Hypertens 2015; 33:465–472. [DOI] [PubMed] [Google Scholar]
- 173.Bhansali A, Dhandania VK, Deepa M, et al. Prevalence of and risk factors for hypertension in urban and rural India: the ICMR-INDIAB study. J Hum Hypertens 2015; 29:204–209. [DOI] [PubMed] [Google Scholar]
- 174.Edwards R, Unwin N, Mugusi F, et al. Hypertension prevalence and care in an urban and rural area of Tanzania. J Hypertens 2000; 18:145–152. [DOI] [PubMed] [Google Scholar]
- 175.Amoah AG. Hypertension in Ghana: a cross-sectional community prevalence study in greater Accra. Ethn Dis 2003; 13:310–315. [PubMed] [Google Scholar]
- 176.Cappuccio FP, Micah FB, Emmett L, et al. Prevalence, detection, management, and control of hypertension in Ashanti, West Africa. Hypertension 2004; 43:1017–1022. [DOI] [PubMed] [Google Scholar]
- 177.Erhun WO, Olayiwola G, Agbani EO, et al. Prevalence of hypertension in a university community in South West Nigeria. Afr J Biomed Res 2005; 8:15–19. [Google Scholar]
- 178.Agyemang C, Bruijnzeels MA, Owusu-Dabo E. Factors associated with hypertension awareness, treatment, and control in Ghana, West Africa. J Hum Hypertens 2006; 20:67–71. [DOI] [PubMed] [Google Scholar]
- 179.Kamadjeu RM, Edwards R, Atanga JS, et al. Prevalence, awareness and management of hypertension in Cameroon: findings of the 2003 Cameroon burden of diabetes baseline survey. J Hum Hypertens 2006; 20:91–92. [DOI] [PubMed] [Google Scholar]
- 180.Duda RB, Kim MP, Darko R, et al. Results of the Women's Health Study of Accra: assessment of blood pressure in urban women. Int J Cardiol 2007; 117:115–122. [DOI] [PubMed] [Google Scholar]
- 181.Kengme AP, Awah PK, Fezeu L, et al. The burden of high blood pressure and related risk factors in urban Sub-Saharan Africa: evidences from Douala in Cameroon. Afri Health Sci 2007; 7:38–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.Niakara A, Fournet F, Gary J, et al. Hypertension, urbanization, social and spatial disparities: a cross-sectional population-based survey in a West African urban environment (Ouagadougou, Burkina Faso). Trans Roy Soc Trop Med Hyg 2007; 101:1136–1142. [DOI] [PubMed] [Google Scholar]
- 183.Omuemu VO, Okojie OH, Omuemu CE. Awareness of high blood pressure status, treatment and control in a rural community in Edo state. Nig J Clin Prac 2007; 10:208–212. [PubMed] [Google Scholar]
- 184.Thorogood M, Connor M, Tollman S, et al. A cross-sectional study of vascular risk factors in a rural South African population: data from the Southern African Stroke Prevention Initiative (SASPI). BMC Public Health 2007; 7:1–10.326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Damasceno A, Azevedo A, Silva-Matos C, et al. Hypertension prevalence, awareness, treatment, and control in Mozambique: Urban/rural gap during epidemiological transition. Hypertension 2009; 54:77–83. [DOI] [PubMed] [Google Scholar]
- 186.Grimsrud A, Stein DJ, Seedat S, et al. The association between hypertension and depression and anxiety disorders: results from a Nationally-representative sample of South African adults. PLoS ONE 2009; 4:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 187.Tesfaye F, Byass P, Wall S. Population based prevalence of high blood pressure among adults in Addis Ababa: uncovering a silent epidemic. BMC Cardiovasc Disord 2009; 9:1–10.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 188.Wamala JF, Karyabakabo Z, Ndungutse D, et al. Prevalence of factors associated with hypertension in Rukungiri District, Uganda—A community-based study. Afri Health Sci 2009; 9:153–160. [PMC free article] [PubMed] [Google Scholar]
- 189.Ekwunife OI, Udeogaranya PO, Nwatu IL. Prevalence, awareness, treatment and control of hypertension in a Nigerian population. Health 2010; 2:731–735. [Google Scholar]
- 190.Oladapo OO, Salako L, Sodiq O, et al. A prevalence of cardiometabolic risk factors among a rural Yoruba south-western Nigerian population: a population-based survey. CVJ Africa 2010; 21:26–31. [PMC free article] [PubMed] [Google Scholar]
- 191.Sani MU, Wahab KW, Yusuf BO, et al. Modifiable cardiovascular risk factors among apparently healthy adult Nigerian population- a cross sectional study. BMC Res Notes 2010; 3:1–7.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 192.Ulasi II, Ijoma CK, Onodugo OD. A community-based study of hypertension and cardio-metabolic syndrome in semi-urban and rural communities in Nigeria. BMC Health Serv Res 2010; 10:1–6.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 193.Maher D, Waswa L, Baisley K, et al. Epidemiology of hypertension in low-income countries: a cross-sectional population-based survey in rural Uganda. J Hypertens 2011; 29:1061–1068. [DOI] [PubMed] [Google Scholar]
- 194.Ulasi II, Ijoma CK, Onwubere BJ, et al. High prevalence and low awareness of hypertension in a market population in Enugu, Nigeria. Intl J Hypertens 2011; doi: 104061/2011/869675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 195.Wokoma FS, Alasia DD. Blood pressure pattern in Barako—a rural community in Rivers state, Nigeria. Nig Health J 2011; 11:8–13. [Google Scholar]
- 196.Awoke A, Awoke T, Alemu S, et al. Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovasc Disord 2012; 12:1–6.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 197.Dzudie A, Kengne AP, Muna WF, et al. Prevalence, awareness, treatment and control of hypertension in a self-selected Sub-Saharan African urban population: a cross-sectional study. BMJ Open 2012; 2:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 198.Hendriks ME, Wit FW, Roos MT, et al. Hypertension in Sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PLoS ONE 2012; 7:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 199.Macia E, Duboz P, Gueye L. Prevalence, awareness, treatment and control of hypertension among adults 50 years and older in Dakar, Senegal. CVJ Africa 2012; 23:265–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 200.Mayega RW, Makumbi F, Rutebemberwa E, et al. Modifiable socio-behavioural factors associated with overweight and hypertension among persons aged 35 to 60 years in Eastern Uganda. PLoS ONE 2012; 7:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 201.Msyamboza KP, Kathyola D, Dzowela T, et al. The burden of hypertension and its risk factors in Malawi: nationwide population-based STEPS survey. Int Health 2012; 4:246–252. [DOI] [PubMed] [Google Scholar]
- 202.Adebayo RA, Balogun MO, Adedoyin RA, et al. Prevalence of hypertension in three rural communities of Ife North Local Government Area of Osun state, South West Nigeria. Int J Gen Med 2013; 6:863–868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 203.Asekun-Olarinmoye EO, Akinwusi PO, Adebimpe WO, et al. Prevalence of hypertension in the rural adult population of Osun state, southwestern Nigeria. Int J Gen Med 2013; 6:317–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 204.Ekanem US, Opara DC, Akaowo CD. High blood pressure in a semi-urban community in south–south Nigeria: a community-based study. Afr Health Sci 2013; 13:56–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 205.Kandala N-B, Tigbe W, Manda SO, et al. Geographic variation of hypertension in Sub-Saharan Africa: a case study of South Africa. Am J Hypertens 2013; 26:382–391. [DOI] [PubMed] [Google Scholar]
- 206.Musinguzi G, Nuwaha F. Prevalence, awareness and control of hypertension in Uganda. PLoS ONE 2013; 8:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 207.Ogah OS, Madukwe OO, Chukwuonye II, et al. Prevalence and determinants of hypertension in Abia state Nigeria: results from the Abia state non-communicable diseases and cardiovascular risk factors survey. Etnicity Dis 2013; 23:161. [PubMed] [Google Scholar]
- 208.Ogunmola OJ, Olaifa AO, Oladapo OO, et al. Prevalence of cardiovascular risk factors among adults without obvious cardiovascular disease in a rural community in Ekiti State, Southwest Nigeria. BMC Cardiovasc Disord 2013; 13:1–8.89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 209.Okpechi IG, Chukwuonye II, Tiffin N, et al. Blood pressure gradients and cardiovascular risk factors in urban and rural populations in Abia state south eastern Nigeria using the WHO STEPwise Approach. PLoS ONE 2013; 8:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 210.Peer N, Steyn K, Lombard C, et al. A high burden of hypertension in the urban black population of Cape Town: the Cardiovascular Risk in Black South Africans (CRISBA) Study. PLoS ONE 2013; 8:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 211.Peltzer K, Phaswana-Mafuya N. Hypertension and associated factors in older adults in South Africa. CVJ Africa 2013; 24:66–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 212.Pessinaba S, Mbaye A, Yabeta GA, et al. Prevalence and determinants of hypertension and associated cardiovascular risk factors: data from a population-based, cross-sectional survey in Saint Louis, Senegal. CVJ Africa 2013; 24:180–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 213.Awosan KJ, Ibrahim MTO, Essien E, et al. Dietary pattern, lifestyle, nutrition status and prevalence of hypertension among traders in Sokoto Central market, Sokoto, Nigeria. Int J Nutr Metab 2014; 6:9–17. [Google Scholar]
- 214.Awuah RB, Anarfi JK, Agyemang C, et al. Prevalence, awareness, treatment and control of hypertension in urban poor communities in Accra, Ghana. J Hypertens 2014; 32:1–8. [DOI] [PubMed] [Google Scholar]
- 215.Doulougou B, Kouanda S, Bado A, et al. Hypertension in the adult population of Kaya health and demographic surveillance system in Burkina Faso: prevalence and associated factors. Int J Trop Dis Health 2014; 4:94–110. [Google Scholar]
- 216.Doulougou B, Kouanda S, Rossier C, et al. Differences in hypertension between informal and formal areas of Ouagadougou, a sub-Saharan African city. BMC Public Health 2014; 14:1–9.893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 217.Duboz P, Boetsch G, Gueye L, et al. Hypertension prevalence, awareness, treatment and control in Dakar (Senegal). J Hum Hypertens 2014; 28:489–493. [DOI] [PubMed] [Google Scholar]
- 218.Helelo TP, Gelaw YA, Adane AA. Prevalence and associated factors of hypertension among adults in Durame town, Southern Ethiopia. PLoS ONE 2014; 9:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 219.Moges B, Amare B, Fantahun B, et al. High prevalence of overweight, obesity, and hypertension with increased risk to cardiovascular disorders among adults in northwest Ethiopia: a cross sectional study. BMC Cardiovasc Disord 2014; 14:1–10.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 220.Minicuci N, Biritwum RB, Mensah G, et al. Sociodemographic and socioeconomic patterns of chronic non-communicable disease among the older adult population in Ghana. Glob Health Action 2014; 7:21292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Oladimeji AM, Fawole O, Nguku P, et al. Prevalence and factors associated with hypertension and obesity among civil servants in Kaduna, Kaduna State, June 2012. Pan Afr Med J 2014; 18 Supp 1:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 222.Oluyombo R, Olamoyegun MA, Olaifa O, et al. Cardiovascular risk factors in semi-urban communities in southwest Nigeria: patterns and prevalence. J Epidemiol Global Health 2014; 5:167–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 223.Abebe SM, Berhane Y, Worku A, et al. Prevalence and associated factors of hypertension: a cross-sectional community based study in Northwest Ethiopia. PLoS ONE 2015; 10:e0125210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 224.Akpan EE, Ekrikpo UE, Udo AI, et al. Prevalence of hypertension in Akwa Ibom State, South–South Nigeria: rural versus urban communities study. Int J Hypertens 2015; article ID 975819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 225.Angaw K, Dadi AF, Alene KA. Prevalence of hypertension among federal ministry civil servants in Addis Ababa, Ethiopia: call for a workplace-screening program. BMC Cardiovasc Dis 2015; 15:76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 226.Anteneh ZA, Yalew WA, Abitew DB. Prevalence and correlation of hypertension among adult population in Bahir Dar city, northwest Ethiopia: a community based cross-sectional study. Int J Gen Med 2015; 8:175–185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 227.Asiki G, Murphy GA, Baisley K, et al. Prevalence of dyslipidaemia and associated risk factors in a rural population in South-Western Uganda: a community based survey. PLoS ONE 2015; 10:e0126166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 228.Isara AR, Okundia PO. The burden of hypertension and diabetes mellitus in rural communities in southern Nigeria. Pan Afr Med J 2015; 20:103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 229.Musinguzi G, Geertruyden J-P, Bastiaens H, et al. Uncontrolled hypertension in Uganda: a comparative cross-sectional study. J Clin Hypertens 2015; 17:63–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 230.Oguoma VM, Nwose EU, Skinner TC, et al. Prevalence of cardiovascular disease risk factors among a Nigerian adult population: relationship with income level and accessibility to CVD risks screening. BMC Public Health 2015; 15:397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 231.Wandera SO, Kwagala B, Ntozi J. Prevalence and risk factors for self-reported non-communicable diseases among older Ugandans: a cross-sectional study. Glob Health Action 2015; 8:27923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 232.Sowemimo I, Ajayi I, Akpa O, et al. Prevalence of hypertension and associated factors among residents of Ibadan-north local government area of Oyo state, Nigeria. J Hypertens 2015; 33 Supp 1:e31. [Google Scholar]
- 233.Kingue S, Ngoe CN, Menanga AP, et al. Prevalence and risk factors of hypertension in urban areas of Cameroon: a nationwide population-based cross-sectional study. J Clin Hypertens (Greenwich) 2015; 3: doi: 101111/jch12604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 234.Bushara SO, Noor SK, Elmadhoun WM, et al. Undiagnosed hypertension in a rural community in Sudan and association with some features of the metabolic syndrome: how serious is the situation? Ren Fail 2015; 4:1–5. [DOI] [PubMed] [Google Scholar]
- 235.Seck SM, Diop-Dia A, Dia DG, et al. Prevalence of hypertension and assessment of its impact on self-rated health in rural populations: a cross-sectional study in northern Senegal. Med Sante Trop 2015; 3: [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 236.Ezeala-Adikaibe BA, Orjioke C, Ekenze OS, et al. Population-based prevalence of high blood pressure among adults in an urban slum in Enugu, South East Nigeria. J Hum Hypertens 2015; 28: Doi: 101038/jhh201549. [DOI] [PubMed] [Google Scholar]
- 237.Ibekwe R. Modifiable risk factors of hypertension and socio-demographic profile in Oghara, Delta State; prevalence and correlates. Ann Med Health Sci Res 2015; 5:71–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 238.Ugwuja E, Ezenkwa U, Nwibo A, et al. Prevalence and determinants of hypertension in an agrarian rural community in southeast Nigeria. Ann Med Health Sci Res 2015; 5:45–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 239.Botha S, Fourie CM, Schutte R, et al. Soluble urokinase plasminogen activator receptor and hypertension among black South Africans after 5 years. Hypertens Res 2015; 38:439–444. [DOI] [PubMed] [Google Scholar]
- 240.Sander LD, Newell K, Ssebbowa P, et al. Hypertension, cardiovascular risk factors and antihypertensive medication utilisation among HIV-infected individuals in Rakai, Uganda. Trop Med Int Health 2015; 20:391–396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 241.Amuna P, Zotor FB. Epidemiological and nutrition transition in developing countries: impact on human health and development. Proc Nutr Soc 2008; 67:82–90. [DOI] [PubMed] [Google Scholar]
- 242.Kroll M, Bharucha E, Kraas F. Does rapid urbanization aggravate health disparities? Reflections on the epidemiological transition in Pune, India. Glob Health Action 2014; 7:23447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 243.Pereira M, Lunet N, Azevedo A, et al. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. J Hypertens 2009; 27:963–975. [DOI] [PubMed] [Google Scholar]
- 244.Jousilahti P, Vartiainen E, Tuomilehto J, et al. Sex, age, cardiovascular risk factors, and coronary heart disease. A prospective follow-up study of 14786 middle-age men and women in Finland. Circulation 1999; 99:1165–1172. [DOI] [PubMed] [Google Scholar]
- 245.Rosano GM, Vitale C, Marazzi G, et al. Menopause and cardiovascular disease: the evidence. Climacteric 2007; 1:19–24. [DOI] [PubMed] [Google Scholar]
- 246.Pinto E. Blood pressure and ageing. Postgrad Med J 2007; 83:109–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 247.Franklin SS, Gustin W, Wong ND, et al. Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997; 96:308–315. [DOI] [PubMed] [Google Scholar]
- 248.Landahl S, Bengtsson C, Sigurdsson JA, et al. Age-related changes in blood pressure. Hypertension 1986; 8:1044–1049. [DOI] [PubMed] [Google Scholar]
- 249.Singh RB, Suh IL, Singh VP. Hypertension and stroke in Asia: prevalence, control and strategies in developing countries for prevention. J Hum Hypertens 2000; 14:749–763. [DOI] [PubMed] [Google Scholar]
- 250.Thawornchaisit P, de Looze F, Reid CM, et al. Health risk factors and the incidence of hypertension: 4-year prospective findings from a national cohort of 60 569 Thai Open University students. BMJ Open 2013; 3:e002826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 251.Hammer GP, du Prel J, Blettner M. Avoiding bias in observational studies. Dtsch Arztebl Int 2009; 106:664–668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 252.Dyer AR, Elliot P, Shipley M. Body mass index versus height and weight in relation to blood pressure. Am J Epidemiol 1990; 131:589–596. [DOI] [PubMed] [Google Scholar]
- 253.Folsom AR, Kushi LH, Anderson KE, et al. Associations of general and abdominal obesity with multiple health outcomes in older women: the Iowa Women's Health Study. Arch Intern Med 2000; 160:2117–2128. [DOI] [PubMed] [Google Scholar]
- 254.Hu G, Barengo NC, Tuomilehto J, et al. Relationship of physical activity and body mass index to the risk of hypertension: a prospective study in Finland. Hypertension 2004; 43:25–30. [DOI] [PubMed] [Google Scholar]
- 255.Radi S, Lang T, Lauwers-Cances V, et al. One-year hypertension incidence and its predictors in a working population: the IHPAF study. J Hum Hypertens 2004; 18:487–494. [DOI] [PubMed] [Google Scholar]
- 256.Ioannidis JP, Patsopoulos NA, Rothstein HR. Reasons or excuses for avoiding meta-analysis in forest plots. BMJ 2008; 336:1413–1415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 257.Higgins JP. Commentary: heterogeneity in meta-analysis should be expected and appropriately quantified. Int J Epidemiol 2008; 37:1158–1160. [DOI] [PubMed] [Google Scholar]
- 258.Terrin N, Schmid CH, Lau J, et al. Adjusting for publication bias in the presence of heterogeneity. Stat Med 2003; 22:2113–2126. [DOI] [PubMed] [Google Scholar]
- 259.Huang Z, Willett WC, Manson JE, et al. Body weight, weight change, and risk for hypertension in women. Ann Intern Med 1998; 128:81–88. [DOI] [PubMed] [Google Scholar]
- 260.Kaufman JS, Owoaje EE, James SA, et al. Determinants of hypertension in West Africa: contribution of anthropometric and dietary factors to urban–rural and socioeconomic gradients. Am J Epidemiol 1996; 143:1203–1218. [DOI] [PubMed] [Google Scholar]
- 261.Rose G, Stamler J, Stamler R, et al. Intersalt: an international study of electrolyte excretion and blood pressure. Results for 24 hour urinary sodium and potassium excretion. BMJ 1998; 297:319–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 262.Stamler J. The INTERSALT Study: background, methods, findings, and implications. Am J Clin Nutr 1997; 65:626S–642S. [DOI] [PubMed] [Google Scholar]
- 263.Zhao L, Stamler J, Yan LL, et al. Blood pressure differences between northern and southern Chinese: role of dietary factors: the International Study on Macronutrients and Blood Pressure. Hypertension 2004; 43:1332–1337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 264.Fateh M, Emamian MH, Asgari F, et al. Socioeconomic inequality in hypertension in Iran. J Hypertens 2014; 32:1782–1788. [DOI] [PubMed] [Google Scholar]
- 265.He FJ, Li J, Macgregor GA. Effect of longer term modest salt reduction on blood pressure: cochrane systematic review and meta-analysis of randomised trials. BMJ 2013; 346:3. [DOI] [PubMed] [Google Scholar]
- 266.World Health Organization. 2015. Creating an enabling environment for population-based salt reduction strategies. [online] Available at: http://www.who.int/dietphysicalactivity/reducingsalt/en/ (Accessed 17/05/2015). [Google Scholar]
- 267.World Health Organization. 2012. Guideline: Potassium intake for adults and children; [online] Available at: http://apps.who.int/iris/bitstream/10665/77986/1/9789241504829_eng.pdf?ua=1 (Accessed 15/05/2015). [PubMed] [Google Scholar]
- 268.Stranges S, Cappuccio FP. Prevention and management of hypertension without drugs. Curr Hypertens Rev 2007; 3:182–195. [Google Scholar]
- 269.Murray CJL, Lauer JA, Hutubessy RCW, et al. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular-disease risk. Lancet 2003; 361:717–725. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.