

Abstract
Randomized controlled clinical trial.
The main purpose of the present study was to comparatively analyze the effectiveness, advantages, and the complications of using semirigid synthetic softcast with respect to plaster of Paris (POP) during the treatment of clubfoot deformity.
The study group consisted of 196 babies (249 feet). A total of 133 feet treated by an orthopedic referral center using semirigid synthetic softcast were included in group A whereas the other 116 feet treated by another orthopedic clinic using POP cast were included in group B. The Pirani scores, number of cast applications, time period until Achilles tenotomy, any skin problems due to the cast itself, and/or cast removal were recorded. A final parent satisfaction score was also obtained.
The mean Pirani sores were significantly improved from the first administration to the time before Achilles tenotomy in both groups. There was no significant difference according to the number of casts applied until tenotomy. The slippage of the cast and skin lesions was significantly more common in group B. Higher parent satisfaction levels were detected in group A.
Semirigid softcast has been found as superior to POP in the aspects of parent satisfaction and cast-related complication rates.
INTRODUCTION
Talipes equinovarus is the most common congenital foot deformity diagnosed in newborns. Serial manipulative casting by the use of plaster of Paris (POP) has been accepted as the primary treatment modality to correct this multiplanar deformity. Application of serial manipulative POP casts was first introduced and popularized by Kite1 in the literature; however, the Ponseti technique has been the most popular and demonstrated as the most effective treatment approach.2,3 Using the Ponseti technique, the rates of satisfactory results have been reported as more than 90% by various authors in the literature.4,5
The Ponseti technique requires casting weekly, with each cast being applied just after the previous cast removal. Ponseti advised using POP casting because it could be easily molded. It is also cheap and can easily be obtained. However, one of the main problems with this type of cast is removal. POP can be more difficult for parents and clinical staff to remove than fiberglass casts. Some physicians dealing primarily with the treatment of clubfoot deformity, ask the parents of the patient to soak off the old cast the night before the application of the new cast upon arrival at the clinic. In this case, there is a time gap between the cast removal and the application of the new one. This period can compromise the duration of effective splintage. This may lengthen the time needed for correction and increase the number of casts needed.6 POP also has disadvantages such as soiling and heaviness.7 Moreover, the removal of the casts can be stressful for the child as well as the parents.8
Semirigid synthetic softcast is a lightweight material that allows rapid application and removal without any soaking or the use of an oscillating saw. It can easily be applied and dried within an acceptable period, allowing for molding. In addition, there is no time interval between cast removal and application.7 On the other hand, there are limited numbers of reports regarding the use of fiberglass cast materials in the treatment of clubfoot with the Ponseti technique.8–11
The main purpose of the present study was to comparatively analyze the effectiveness, advantages, and the complications of using semirigid synthetic softcast with respect to POP cast during the treatment of clubfoot deformity.
MATERIAL AND METHODS
After having approval from Selcuk University Faculty of Medicine Ethical Research Institutional Review Board, the present study retrospectively evaluated the clinical data of 196 patients who underwent serial manipulative casting treatment using Ponseti technique for clubfoot between September 2009 and October 2010. Idiopathic talipes equinovarus was the diagnosis for all cases. Clubfoot related to neuromuscular disorders such as myelomeningocele, cerebral palsy or arthrogriposis multiplex congenita, the patients who had a past medical history of any failed treatment for clubfoot, and the ones with any accompanying congenital deformity of the lower extremity were excluded from the study. The study group consisted of 196 babies and 249 feet. The patients were randomized into 2 groups. A total of 95 patients (133 feet) treated by an orthopedic referral center using semirigid synthetic softcast were included in group A, whereas the other 101 patients (116 feet) treated by another orthopedic referral center using POP cast were included in group B. Group A consisted of 59 boys (85 feet) and 36 girls (48 feet). Group B consisted of 61 boys (70 feet) and 40 girls (46 feet). The mean age at presentation was 3.44 ± 3 (range, 0–14) days in group A and 3.59 ± 3.2 (range, 0–16) days in Group B.
Serial manipulations and cast treatment was started as soon as possible after the first clinical visit (Fig. 1). The feet were scored according to the Pirani scoring system at the initial examination and during the last examination before Achilles tenotomy. Manipulations and serial weekly cast applications were begun immediately according to the Ponseti technique. The cavus, adductus, and varus components of the deformity were corrected by positioning the foot in supination and then abducting the foot while counter pressure was applied with the thumb over the head of talus. Above-the-knee casts made from the semirigid synthetic cast material (3 M Scotchcast Soft Cast; Health Care, St Paul, MN) for group A and from the POP for group B were applied. Each foot was approached separately for babies with bilateral clubfeet (Fig. 2).
FIGURE 1.

The photograph of a 2 days old baby with bilateral clubfeet at the initial examination.
FIGURE 2.

The photograph of a baby applied bilateral above knee casts made of semirigid synthetic softcast according to the Ponseti method.
All the medical records for the patients were reviewed, especially the clinical evaluation at the initial and final examinations, including Pirani scores.12 The number of cast applications and the period until Achilles tenotomy was also documented. Any skin problems due to the cast itself (such as pressure wounds) and cast removal (such as skin scratches) were recorded. The period for each foot casting was also noted. All the casts were removed in the clinic just before the next manipulation, so that the reduction loss was minimized. When the foot achieved 70° of abduction relative to thigh, percutaneous Achilles tenotomy was indicated if there was <15° of dorsiflexion at the same time. A total of 113 of the 133 feet (84.9%) in group A and 95 of the 116 feet (81.9%) in group B underwent percutaneous Achilles tenotomy, followed by 3 weeks of casting. All the tenotomies were performed under local or general anesthesia in the operating room. Dennis–Browne splints, as described in the Ponseti method, were applied after the removal of the final cast.10 A final parent satisfaction score was also obtained.9 According to this 5-point evaluation system (excellent = 5, very good = 4, good = 3, fair = 2, and poor = 1), cast convenience, cast weight, infant tolerance, durability, material satisfaction, and likelihood of recommending the material scores were noted at the end of the final cast removal.
Number Cruncher Statistical System 2007 statistical software (UT) was used for the statistical analyses. The descriptive statistics describing the demographic information were expressed as medians, ranges, and interquartile ranges or in medians and standard deviations. A Wilcoxon test was used to compare the initial and the final Pirani scores before Achilles tenotomy. Also, a Mann–Whitney U test was used to compare the variables at the initial and final clinical examinations. Qualitative data were compared using Fisher exact test and Chi-square tests. A P value of 0.05 or less with confidence interval 95% was considered significant.
RESULTS
The mean Pirani sores were significantly improved from the first administration of the patients up to the time before Achilles tenotomy in both groups (Table 1). However, no significant difference was detected between the groups according to the change in the mean Pirani score (P = 0.198). The number of casts applied until the patients reached at the Achilles tenotomy stage was 3.6 ± 1 (range, 2–5) in group A and 3.8 ± 0.8 (range, 2–5) in group B. There was no significant difference between the groups according to the number of casts applied until Achilles tenotomy (P = 0.081). In group A, the mean Pirani score at presentation was 5.75 ± 0.51 for the feet required a tenotomy and 4.13 ± 0.96 for those that did not. In group B, the mean Pirani score at presentation was 5.56 ± 0.49 for the feet required a tenotomy and 4.04 ± 0.90 for those that did not (Table 2). The Pirani scores before Achilles tenotomy or at the end of serial manipulative casting for the ones who did not require an Achilles tenotomy were significantly lower than the initial scores in all patients (P = 0.0001).
TABLE 1.
Comparison of Pirani Scores at the Initial Administration and Before the Achilles Tenotomy
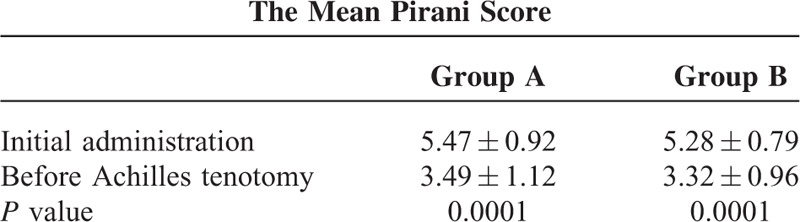
TABLE 2.
Comparison of Pirani Scores Between the Patients Required Achilles Tenotomy or Did Not

Minor complications were noted in 12 patients from group A. Nine patients had minor skin irritations (5 skin scratches in the groin, 3 superficial skin abrasions on the dorsal skin of the foot, and 2 superficial heel ulcerations) that did not require any treatment or pausing of the cast applications. There were also 3 cast slippages. In group B, a total number of 23 complications were noted. Seven patients had minor skin irritations (3 skin scratches in the groin and 4 superficial skin abrasions on the dorsal skin of the foot). The slippage of the cast was detected in 9 feet. Skin scratches due to oscillating saw during the cast removal were documented in 7 feet. Three of those feet required pausing of the cast applications for a 1-week period and thus, increased the total period of serial manipulative casting treatment. The slippage of the cast and skin lesions during the removal of the cast was significantly more common in group B (P = 0.017).
The mean parent satisfaction scores were 4 over 5 for cast convenience, 4.5 for cast weight, 3.9 for infant tolerance, 4.5 for cast durability, 4.4 for material satisfaction, and 4.4 for the likelihood of recommending the cast material in group A. In group B, the mean parent satisfaction scores were 3.6 for cast convenience, 2.9 for cast weight, 3.8 for infant tolerance, 4.2 for cast durability, 3.1 for material satisfaction, and 3.3 for the likelihood of recommending the cast material.
DISCUSSION
The history of the clubfoot treatment was assessed in detail by the Iowa Clinic in 2000.2 Surgical treatment techniques had major problems, such as stiffness, small feet, and poor functional results.1,4,13 The Ponseti technique has been used with satisfactory results for more than 20 years. The major advantage of this method is achieving good deformity correction without any major operations. With this technique, many authors reported good-to-excellent results.14–16 One of the main issue regarding the Ponseti technique is the need for close follow-ups. If family compliance is not good, the results become worse.14,16–18
The Ponseti technique has been described in detail by Ponseti et al.3,16,18–21 The Ponseti technique requires traditional POP for casting material because it can easily be molded. The standard removal techniques for POP casts include holding the extremity in water for approximately 30 minutes and then unwrapping or using a cast saw or a cast knife, which can be very irritating for the baby and the parents. Semirigid synthetic softcast may also be the choice of material used during serial manipulative cast applications. The main advantages of fiberglass materials are radiolucency, lighter weight, improved strength, faster curing time, lower risk of thermal burn, cleaner application and removal, and improved durability. A semirigid fiberglass material has been marketed as having additional advantages over classic rigid fiberglass materials, such as molding ability, flexibility, comfort, and ease of removal and unwrapping.8 Semirigid fiberglass cast materials can be removed easily with unwinding alone in a few minutes.10 On the other hand, the major disadvantage of fiberglass material is its high cost.
Some studies have been designed to compare semirigid synthetic and traditional POP cast materials in the treatment of clubfoot. One of them described better functional results with POP, although the cast convenience and parent satisfaction parameters were better with fiberglass material.11 Dimeglio scoring system was used for this study and the number of the patients was 34. Our study revealed different results compared to Pittner et al although we used approximately the same parameters such as complete time, different results could be secondary to the scoring system which was used and low number of the patients. Brewster et al10 reported the results of clubfoot treatment with softcast. They used below knee soft casts and concluded that using below knee soft cast was comparable to those using above knee POP cast. Pirani scoring system was used during this study. The similar results compared to our study can be secondary to the same scoring system and similar number of patients. This matched the conclusion drawn by another report showing that fiberglass was statically superior in its durability, performance, and ease of removal; 94% of parents strongly preferred semirigid fiberglass over POP for their children's serial casting. Other advantages of fiberglass materials include its light weight, lack of soiling, and water resistance.8
We noted Pirani severity scores for each patient during the treatment and follow-up visits. All the manipulations and the cast positions were also applied according to Ponseti technique.2 Our results confirm the efficacy of the Ponseti technique of manipulation and serial casting. Overall, we obtained acceptable correction with serial casting alone in 15% of feet and with percutaneous Achilles tenotomy in 85% of feet. Parental compliance during the treatment is one of the main factors in the nonsurgical treatment.5,18,22 Any improvement in treatment technique that can increase compliance may provide better outcomes. Our results demonstrated that using semirigid synthetic softcast for clubfoot treatment provides higher parent satisfaction with lower rates of cast-related complications. Furthermore, the fiberglass cast is durable, and its removal is easier than the POP cast.8
The main limitation of the current study was the retrospective evaluation of prospectively followed patient groups. Another limitation was the application of only the Pirani scoring system. The different results of similar studies using the scoring system of Dimeglio could not be checked for the efficacy of softcast material. On the other hand, the current study was a comparative analysis between the 2 groups of patients with similar clinical features and treated by 2 orthopedic referral clinics using 2 different types of casting material for the Ponseti technique. Our cohort was a large series included patients with primary idiopathic clubfoot deformity diagnosed and treated immediately after birth. Although we did not apply a priori calculation for the sample size, post-hoc analysis was performed and the statistical power of our study in the aspect of achieving a comparison between the 2 groups according to the 2 types of cast material was 0.97 with an alpha value of 0.05. The effect of semirigid synthetic softcast on long-term results and recurrence rate was not evaluated in this study, and thus we recommend that further studies are required. This study may be a reference for future investigations.
In conclusion, the results that we acquired during the present study were similar to those of previous reports on the effectiveness of the Ponseti method of manipulation and casting. The semirigid fiberglass did demonstrate a trend toward greater parent satisfaction with the material. Semirigid softcast material can easily be used with the Ponseti technique for clubfoot treatment because it provides higher parent satisfaction levels and is easier for the physicians to apply and remove.
Footnotes
The authors have no conflicts of interest to disclose.
REFERENCES
- 1.Kite JH. Nonoperative treatment of congenital clubfoot. Clin Orthop Relat Res 1972; 84:29–38. [DOI] [PubMed] [Google Scholar]
- 2.Dobbs MB, Morcuende JA, Gurnett CA, et al. Treatment of idiopathic clubfoot: an historical review. Iowa Orthop J 2000; 20:59–64. [PMC free article] [PubMed] [Google Scholar]
- 3.Ponseti IV, Campos J. Observations on pathogenesis and treatment of congenital club foot. Clin Orthop 1972; 84:50–60. [DOI] [PubMed] [Google Scholar]
- 4.Laaveg SJ, Ponseti IV. Long-term results of treatment of congenital club foot. J Bone Joint Surg Am 1980; 62:23–31. [PubMed] [Google Scholar]
- 5.Lehman WB, Mohaideen A, Madan S, et al. A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot. J Pediatr Orthop B 2003; 12:133–140. [DOI] [PubMed] [Google Scholar]
- 6.Terazas-Lafargue G, Morcuende JA. Effect of cast removal timing in the correction of idiopathic clubfoot by Ponseti method. Iowa Orthop J 2007; 27:24–27. [PMC free article] [PubMed] [Google Scholar]
- 7.Patel NK, Jeer PJ, Cornell MS. Using cling film to protect lower limb plaster casts in babies with clubfoot. Br J Nurs 2007; 16:1140–1142. [DOI] [PubMed] [Google Scholar]
- 8.Coss HS, Hennrikus WL. Parent satisfaction comparing two bandage materials used during serial casting in infants. Foot Ankle Int 1996; 17:483–486. [DOI] [PubMed] [Google Scholar]
- 9.Ng BK, Lam TP, Cheng JC. Treatment of severe clubfoot with manipulation using synthetic cast material and a foam-casting platform: a preliminary report. J Pediatr Orthop B 2010; 19:164–170. [DOI] [PubMed] [Google Scholar]
- 10.Brewster MB, Gupta M, Pattison GT, et al. Ponseti casting: a new soft option. J Bone Joint Surg Br 2008; 90:1512–1515. [DOI] [PubMed] [Google Scholar]
- 11.Pittner DE, Klingele KE, Beebe AC. Treatment of clubfoot with the Ponseti method: a comparison of casting materials. J Pediatr Orthop 2008; 28:250–253. [DOI] [PubMed] [Google Scholar]
- 12.Dyer PJ, Davis N. The role of the Pirani scoring system in the management of club foot by the Ponseti method. J Bone Joint Surg (Br) 2006; 88:1082–1084. [DOI] [PubMed] [Google Scholar]
- 13.Aronson J, Puskarich CL. Deformity and disability from treated clubfoot. J Pediatr Orthop 1990; 10:109–119. [PubMed] [Google Scholar]
- 14.Abdelgawad AA, Lehman WB, van Bosse HJ, et al. Treatment of idiopathic clubfoot using the Ponseti method: minimum 2-year follow-up. J Pediatr Orthop B 2007; 16:98–105. [DOI] [PubMed] [Google Scholar]
- 15.Colburn M, Williams M. Evaluation of the treatment of idiopathic clubfoot by using the Ponseti method. J Foot Ankle Surg 2003; 42:259–267. [DOI] [PubMed] [Google Scholar]
- 16.Morcuende JA, Dolan LA, Dietz FR, et al. Radical reduction in the rate of extensive corrective surgery for club foot using the Ponseti method. Pediatrics 2004; 113:376–380. [DOI] [PubMed] [Google Scholar]
- 17.Changluani M, Gang NK, Rajagopal TS, et al. Treatment of idiopathic clubfoot using the Ponseti method. Initial experience. J Bone Joint Surg Br 2006; 881385–881387. [DOI] [PubMed] [Google Scholar]
- 18.Dobbs MB, Rudzki JR, Purcell DB, et al. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfeet. J Bone Joint Surg Am 2004; 86-A:22–27. [DOI] [PubMed] [Google Scholar]
- 19.Ponseti IV. Treatment of congenital club foot. J Bone Joint Surg Am 1992; 74:448–454. [PubMed] [Google Scholar]
- 20.Ponseti IV. Common errors in the treatment of congenital clubfoot. Int Orthop 1997; 21:137–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kowalcczyk B, Lejman T. The principles of the Ponseti method in the treatment of congenital clubfoot. Ortop Traumatol Rehabil 2007; 9:436–440. [PubMed] [Google Scholar]
- 22.Ponseti IV, Smoley EN. Congenital clubfoot: the results of treatment. J Bone Joint Surg Am 1963; 45:261–275. [Google Scholar]