

Abstract
Context In a health service environment where timescales for patient participation in service design are short and resources scarce, a balance needs to be achieved between research rigour and the timeliness and utility of the findings of patient participation processes.
Objective To develop a pragmatic mind mapping approach to managing the qualitative data from patient participation processes.
Design While this article draws on experience of using mind maps in a variety of participation processes, a single example is used to illustrate the approach. In this example mind maps were created during the course of patient participation focus groups. Two group discussions were also transcribed verbatim to allow comparison of the rapid mind mapping approach with traditional thematic analysis of qualitative data.
Setting and participants The illustrative example formed part of a local alcohol service review which included consultation with local alcohol service users, their families and staff groups.
Findings The mind mapping approach provided a pleasing graphical format for representing the key themes raised during the focus groups. It helped stimulate and galvanize discussion and keep it on track, enhanced transparency and group ownership of the data analysis process, allowed a rapid dynamic between data collection and feedback, and was considerably faster than traditional methods for the analysis of focus groups, while resulting in similar broad themes.
Conclusion This study suggests that the use of a mind mapping approach to managing qualitative data can provide a pragmatic resolution of the tension between limited resources and quality in patient participation processes.
Keywords: focus groups, patient participation, qualitative research
Introduction
Working in the health services, where funding is often short‐term, policy changes come round with hurricane speed, and outcome measures are weighed heavily on the short‐term, there is always a tension between research rigour and the need for quick results.
With the current climate of promoting user involvement in the NHS in England, health trusts also have a duty to involve users in service design. 1 , 2 The Secretary of State for Health recently called for the NHS ‘to collect immediate feedback from patients on their experience of care’ (p3) and staff are advised to make systematic use of a mixture of feedback methods. 3 Meaningful consultation where users feel listened to and can engage in an ongoing dialogue with service providers has great benefits to both patients and service providers, leading to well used, needs‐led services and empowered, healthier patients; ‘High quality Patient & Public Involvement can truly change things for patients and carers, both in their experience of services and the quality of their care. It can also enhance the working lives of health professionals, helping them to increase service responsiveness, deliver improved health outcomes for all and improving job satisfaction’ (p16). 4
However, some of the participatory methods which are effective at reaching out to and engaging service users can lack scientific rigour, 5 while other methods which may be quick and easy to use, such as questionnaires, suffer poor response rates or may not give the kind of rich data commissioners need to understand patient perspectives fully. 6 So we have a further tension here between research rigour and meaningful user involvement.
It does appear that many health service managers and commissioners opt for a survey as their default method of choice when seeking the views of patients to inform service improvement or commissioning processes. The potential for using focus groups to acquire a deeper understanding of the views of service users is not always recognized, although their wider use within healthcare settings has been advocated. 7 Focus groups can be particularly useful when there is a need to bridge the gulf in understanding between service providers and users. 8
One barrier to their use may be that traditional qualitative methods require significant resources for transcribing and analysis, so that organizations’ capacity to conduct such exercises is restricted. Another barrier may be lack of qualitative research expertise within the organization. A critique of the use of focus groups in nursing research, for example, concluded that their use was often unsophisticated, especially in relation to data analysis. 9 We are faced, therefore, with the challenge of how to manage efficiently and with due rigour the rich qualitative data we get when we talk to patients and the community about local health services.
The use of mind mapping as a visual tool for engaging users during focus groups and for getting feedback from them afterwards, and as a tool for the analysis of qualitative data, could in some instances provide a pragmatic solution to the tensions outlined above.
Mind mapping
A mind map is a diagram used to represent concepts, ideas or tasks linked to and arranged radially around a central key word or idea. Primary branches represent the major ideas or themes around the central topic, and secondary branches tend to include more concrete illustrative examples. 10 In a closely related field, cognitive maps have been described by Eden, Jones and Sims as ‘a modeling technique which intends to portray ideas, beliefs, values and attitudes and their relationship one to another in a form which is amenable to study and analysis’ (p30). 11
While some authors make a point of clearly distinguishing mind maps from cognitive maps there is in fact a great deal of overlap in how they are used. 8 , 9 Both have been used widely in education and for note‐taking, problem‐solving and brainstorming. One of the advantages of mind mapping over standard note‐taking is that it appears to reflect our natural thinking patterns, which are said to be non‐linear. 10 Within health services mind maps have been found to be valuable in the fields of care planning, needs assessment, nursing research and practice development. 12 , 13 , 14 , 15 , 16 Where stakeholders hold divergent views on a topic under scrutiny, mind maps have been a useful tool for ensuring the broad range of views and perspectives are represented, with the aim of reaching a common understanding. 17
The use of mapping approaches in qualitative data analysis is perhaps not uncommon though seldom reported in detail. Certainly the approach shares similarities with the hierarchical frameworks of codes and categories created by qualitative data management software packages. The use of concept mapping as a tool for analyzing open‐ended survey responses has been pioneered by Trochim and Jackson 18 whose approach blends objective statistical analysis with the human judgment inherent in code‐based analysis. Others have recommended the use of maps as an expeditious method for handling the large volumes of audio‐recorded data from qualitative interviews. 19
Using mind maps for public participation: a case study
While this article draws on experience of using mind mapping in a variety of patient participation processes, a single example is given here to illustrate the approach taken. A local alcohol service review was planned to include consultation with service users, their carers, alcohol service providers, and others in the community who were current or past misusers of alcohol. Five focus groups were conducted as part of this consultation, alongside individual interviews where focus groups were not deemed practical or appropriate. A less structured group interview with chronic alcoholics was also conducted.
Focus group discussions were audio‐recorded with the written consent of participants. While the facilitator managed the focus group discussion using a semi‐structured topic schedule, shown in Fig. 1, a researcher created a mind map on flip‐chart paper during the course of the discussion.
Figure 1.
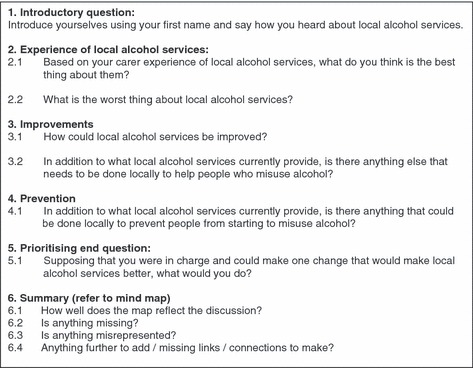
Focus group topic schedule.
A sample mind map is shown in Fig. 2. This is the map created during the focus group with carers and relatives of Community Alcohol Team (CAT) service users. The structure of the map mirrored the topic schedule used by the facilitator to some extent. For example, the introductory question was ‘how did you first come into contact with the CAT?’, and the range of responses given is shown in the branch headed ‘initial contact’. Subsequent discussion explored their positive and negative experiences of the service in turn. Towards the end of the discussion the facilitator asked for recommendations of how the service could be improved.
Figure 2.
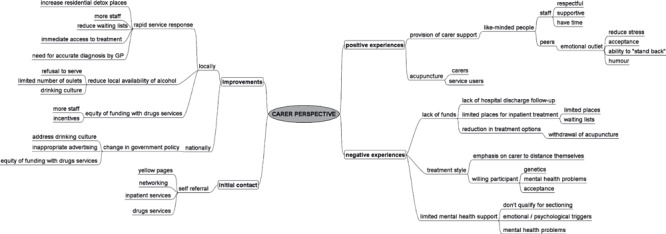
Sample mind map.
Participants were able to comment on the evolving mind map and were encouraged to correct any misinterpretations. They were given time at the end of the focus group to consider the mind map as a whole and could suggest amendments or additions.
Researchers wrote detailed field notes immediately after the focus group. Within 3 days of the focus group the mind map was typed up using mind mapping software (e.g. Freemind™, Sourceforge, Germany; http://www.sourceforge.net). The researchers listened back to the recording of the discussion, reflected on their field notes and made additions and amendments based on listening back, reflection and the field notes. Sufficient time was blocked out to enable this to be done in a single sitting.
Amendments that were made to the mind map were distinguished from the original map by using a different font colour. A copy of this amended mind map was then sent to all participants for member checking to establish credibility. 20
The only exception we made to using this mind mapping approach was with the group interview with chronic alcoholics. This example provides a useful illustration of one of the drawbacks of the approach. The setting for the discussion was their home (an unofficial wet house) and they would not have been receptive to a structured session. Because the discussion with this particular group was relatively unstructured, meandering and contained several contradictions and internal inconsistencies it did not lend itself to capture using a mind map. Instead, detailed notes were taken both during the discussion and while listening back to the audio‐recording. The key themes from this group were then drawn out, agreed by the researchers, and included in the meta‐map described below. Any verbatim quotes taken from the recordings to illustrate key themes from the discussions were recorded separately. These were used in the final report so that participants’ own voices would have a chance to come through.
A meta‐map was created once data collection was completed for all focus groups and interviews, incorporating all the major themes that emerged and showing how often a given theme came up. This process was made easier by the fact that the topic schedule for each focus group was structurally similar, resulting in mind maps that contained broadly similar primary branches. This meta‐map became somewhat unwieldy because of the volume of data, but was useful in representing the totality of themes, including contradictions, in one place and in a graphical format that enabled a holistic perspective. The resulting map shared similarities with the sort of coding framework generated by qualitative data management software, except that with this approach the raw data stayed at the audio‐recording stage without being transcribed.
The meta‐map was used as a basis for writing up the findings from the consultation in a standard report format, making use of the illustrative quotes recorded separately. The mind maps themselves were included as an appendix to the report, ensuring first that participant anonymity had been protected.
Comparison with thematic analysis
To compare the data generated from using this mind mapping technique with traditional qualitative analysis, two of the focus groups were transcribed and analysed by a researcher who had neither been present during the focus group nor seen the mind maps. The themes generated by the mind mapping approach were broadly the same as those that emerged by traditional thematic analysis. The mind mapping approach to analysis was also considerably quicker (taking two as opposed to three hours) although the principal time saving is to be gained in not having the focus group transcribed. While most of the codes created by both analytic approaches were either identical or similar, they were not always to be found under the same theme. So, for example the mind map in Fig. 2 shows the code ‘increase residential detox places’ under ‘improvements: locally’, whereas the alternative analysis placed ‘need for more residential places’ under the theme of ‘access to services’. The thematic analysis did, perhaps not surprisingly, create a greater number of codes than the mind mapping. For example a code that was missed by the mind map was, ‘hospital seen as a sanctuary for the carer but they and the relative are often judged’. To give some context to this case study, a summary of the main findings from this phase of the consultation is presented in Fig. 3.
Figure 3.
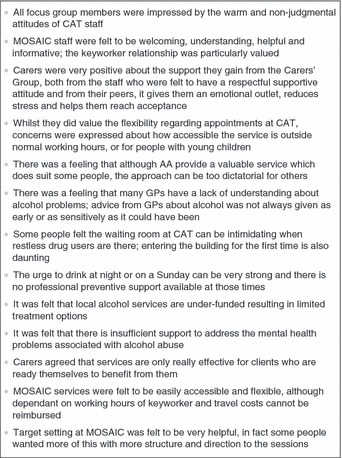
Main findings.
Discussion
In the spirit of the Leeds Declaration public health research should aim to treat patients and the public as partners rather than subjects, and opportunities for meaningful user involvement in the research process should be maximized. 21 The use of mind mapping in the context described here does appear to provide an efficient way to achieve the dual aims of user involvement in service development and in research processes.
Advantages of mind mapping
Perhaps the most significant advantage which mind mapping holds over traditional qualitative data handling is speed. A 90‐min focus group takes 6 to 8 hours to transcribe and will produce 30 or more pages of data to be painstakingly analysed line by line. Krueger, a leading expert in focus groups, makes the following estimate:
If you are planning on using transcripts, you might assume that it will take 6–10 hours to prepare each transcript. Then assuming that you have 3 or 4 focus groups and are using field notes, transcripts, and selective listening to the audio recording you might plan for 60 to 100 hours to arrive at a draft narrative report with quotes. Don’t be surprised if it takes another 20 or so hours for edits and revisions before the report is finalized. If you have never done analysis before, plan to add about 30% more time. 22
Based on these projections, assuming a busy health professional who is relatively new to qualitative research could only dedicate 1 day a week to her focus group study, the analysis and writing up of 3–4 focus groups would take her approximately 4 months. In contrast, the approach outlined above involves no transcription, and the first stage of analysis, generation of coded categories, occurs during the focus group itself. As the mind map develops the researcher is in essence generating coded categories ‘live’– a process which in traditional qualitative thematic analysis would take place by sifting through pages of transcripts after the event.
It is normal practice to have two co‐facilitators for a focus group, one who moderates the discussion and one who does the note‐taking and looks after the practical smooth running of the group. 22 Therefore running a focus group in the way described here involves no additional researcher resource.
A knock‐on benefit of the time saved is that within limited resources a larger number of focus groups can be conducted. If these were repeated interviews with the same groups this could allow greater depth of inquiry and the opportunity for enhanced validity through critical reflection upon the mind map from the previous discussion, perhaps probing further for exceptions or deviant cases, or picking up on and exploring contradictions. Alternatively, if additional discussions were conducted with new groups of participants this could allow a greater number of community voices to feed into the design of services.
It is also worth noting that even verbatim transcriptions have their limitations, since converting a discussion into text will always involve the loss of non‐verbal nuances, and will be subject to human errors such as misinterpretation of content. 23 While visual cues will still be missed, working directly with the data in audio format can enhance validity by avoiding these shortcomings. A team of Canadian researchers have recently explored the use of court reporters to provide a live transcript during focus group discussion, an approach which does appear to overcome many of the difficulties currently experienced, and seems worthy of further investigation. 24
The analytical method described has the added potential benefit of increasing the likelihood of participant ownership, particularly when used in a focus group setting where the mind map evolves during the course of the discussion and can be commented upon by participants, 25 and where the mapper can directly check back with participants that their discussion is being correctly represented. However, if we are to acknowledge the existence of multiple social realities, then it becomes difficult to know how best to alter the mind map in response to an individual member’s post hoc comments. Perhaps a more credible mind map would be reached if the group could consider the mind map collectively at a later date so that a group consensus upon any changes could be reached.
There is also potential for patients to be involved, with the right support and training, in the generation of the mind map during the focus group. Many people will already be familiar with the use of mind maps in, for example, education or problem solving; it would not be a difficult skill to master, and could make the process more empowering for patients.
The process of mind mapping is said to allow free thinking and to clear the mind of previous assumptions about the subject. 10 A tool that encourages this kind of thinking can be valuable both during the focus group discussion, and afterwards if it can help the researcher to bracket previous assumptions. 26
During the course of a semi‐structured focus group discussion the emerging mind map can help to galvanize discussion, highlight links between themes that might not otherwise have been evident, and can be referred to by the facilitator to bring wayward discussion back on track. However, as Krueger 27 cautions in his discussion of the use of flip charts during focus groups, there can be drawbacks to their use:
At their worst, flip charts can slow down the conversation, and, in the process, participants forget their ideas because they are waiting for the writer to capture the thought. Because the participant’s comment must be written quickly, it must be truncated and critical elements may be lost. At their best, flip charts help participants stay on topic and remember what others have said. (p80)
Key to the success of using mind maps during focus groups is therefore the skill of the facilitator. The skills and attributes required for good facilitation of focus groups are described in depth elsewhere 27 but suffice it to say that the facilitator should encourage the flow of discussion to continue while the mind map is being written and, where comments are vague, probing should be employed to elicit a deeper understanding of the concept or idea being expressed. Listening back to the audio‐recording allows for missing elements to be added to the map afterwards. In our experience, listening back to the recording invariably reveals some categories that were omitted from the original map. To ensure the mind map is a good reflection of the themes raised may require repeated listening to the audio recording.
One of the reasons why mind mapping appears to be particularly suited to consultation on service redesign is that the inquiry is likely to be fairly focused. Health service managers commissioning patient consultation often need quite specific feedback about what works, where improvements can be made and what barriers there may be to accessing services. This type of feedback can be clearly represented in a mind map. Whereas, in circumstances where a relatively unstructured and exploratory inquiry is called for, mind mapping is less likely to be the method of choice, and a more formal, detailed approach to analysis may be more appropriate.
Comments from both focus group participants and commissioners about the mind maps indicate that they are a pleasing graphical summary, allowing a holistic overview of the themes. Indeed, we have found that a large (A2 size) meta‐map can be a useful focal point for discussions with commissioners and service providers about how to take forward patients’ and carers’ recommendations from a consultation. For ease of interpretation the meta‐map, or indeed any of the maps, may be colour coded so that, for example, the hot topics are in red. Icons can also be used to highlight positive experiences, problem areas, or ideas for improvement. In the consultation described above the meta‐map was in fact used only by the researchers and was too large and convoluted to be easily interpreted by others. However, where the volume of data is smaller, say from a handful of patient interviews, a meta‐map can be a very useful summary.
It is also worth noting that the rapid dynamic which this approach allows between data collection and feedback means that it is particularly well suited for use in Action Research, where cycles of knowledge gathering and feedback into action are a central feature. This approach means that the key themes from a focus group can be fed back to decision‐makers within a matter of weeks.
Limitations of mind mapping
No attempt is made here to argue that this rapid approach to qualitative data handling can rival traditional qualitative data analysis for depth or level of interpretation. Although the raw data are retained as digital audio files, listening back to the discussion does not compare with the level of data immersion achieved through thematic analysis of transcripts or by Grounded Theory approaches. The sheer speed with which the initial mind map is created during the focus group does not allow for considered reflection at that time, although this can be done afterwards. The traditional thematic analysis conducted did reveal more codes than shown in the mind maps and the structure of the thematic framework was less aligned to the topic schedule.
A significant challenge to the validity of this mind mapping approach is researcher bias. Human judgment plays a major part in the construction of the mind map, both in terms of the choice of words used to summarize participants’ comments and ideas, and the choice of where to position those words on the map. Researchers working with concept mapping have sought to avoid such bias by getting participants to independently sort the emergent concepts into categories themselves, using at least 10 sorters to create a map whose structure is statistically determined. 18 There may be scope within the approach described here for involving focus group members more in the sorting of themes and categories themselves and in identifying the connections between them, thereby creating their own mind map during a follow‐up session expressly designed to achieve this. Other measures can also be taken to improve validity, such as seeking to refute initial assumptions, probing for exceptions and by picking up on and exploring contradictions.
Further, there is a difference between what is most important to focus group participants and what is talked about most during the discussion. 28 The mind map will reflect what issues are raised and its shape will, at least in its first draft, be determined by the order in which topics are discussed rather than the importance attributed to these by the participants. However, sensitive facilitation can elicit an understanding of what participants feel are the most important issues and these can be highlighted accordingly on the map towards the end of the discussion.
In our experience with this technique we have found that it is well suited for the recording of key issues for participants concerning the topic under discussion. However, it is less amenable to getting beyond answering the ‘what?’ questions to exploring the ‘why?’ questions. So, for example the mind map in Fig. 2 shows that carers value the acupuncture service, but we do not find out why. However, this is something that could be further explored during subsequent focus groups.
It is also harder for the mapper to capture contradictory or unclearly expressed comments, so there is a risk that this type of data may get overlooked in favour of clearly expressed coherent points. Here it is down to the skill of the facilitator to probe for deeper understanding, and to set the scene so that participants are encouraged to express differing perspectives. It is important for the mind mapper to strive not to oversimplify or imply consensus where none exists. Differing views may, for example, be colour coded to distinguish them. Where a participant’s view changes during the course of the focus group it is valuable to also record this.
To enhance the validity of the analytical process it is suggested that, where a series of focus groups are to be undertaken, and if resources allow, the first two could be transcribed and thematically analysed. This would allow for the researcher(s) to get more fully immersed in some of the early data. Subsequent mind mapped categories could then be compared with the categories generated by traditional analysis.
A summary of the advantages and limitations of this mind mapping approach is given in Fig. 4.
Figure 4.
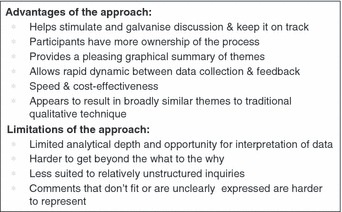
Advantages and limitations.
Other uses for mind maps in qualitative research
The use of mind maps in qualitative research is not limited to focus groups. Within our organization we have also experimented with their use for the capture of key themes following individual interviews. Clearly, some of the advantages outlined in Fig. 4 are precluded if the mind map is created after the discussion (participant ownership, keeping the discussion on track). However, there is more time for considered reflection and the structure of the map is more likely to reflect what is most important to the interviewee as opposed to the structure of the topic guide.
Another way we have used the approach has been for summarizing the themes emerging from a series of narratives collected as part of an Appreciative Inquiry. Very briefly, Appreciative Inquiry is a solution focused process that engages individuals within an organization or community in its renewal through collecting stories of what works and building on that. 29 In this instance the narratives were not audio‐recorded and only brief notes were written, after all the purpose of the Appreciative Inquiry was less qualitative research and more community mobilization. However, it seemed a shame not to bring together these fifty or so stories into some sort of coherent summary. A meta‐map proved the ideal tool.
Future directions
It is hoped that this article will stimulate further debate about the use of mind maps in qualitative research. In particular, their validity needs more academic scrutiny and assessment. The potential for greater patient involvement in the creation and validation of the mind maps is another area that warrants more exploration.
Competing interests
None declared.
Funding
This study was unfunded.
Acknowledgements
We would like to acknowledge the contribution of Julie Hardman (Doctoral Researcher, Manchester Metropolitan University) to the development of this approach to using mind maps. We would also like to thank all the focus group participants for their valuable contribution and feedback.
References
- 1. Department of Health . Creating a Patient‐Led NHS. London: DH, 2005. [Google Scholar]
- 2. Department of Health . Our Health, Our Care, Our Say: A New Direction for Community Services. White Paper. London: DH, 2006. [Google Scholar]
- 3. Department of Health . Understanding What Matters. London: DH, 2009. [Google Scholar]
- 4. Andersson E, Tritter J, Wilson R. eds. Overview: Does Patient and Public Involvement Matter? Healthy Democracy: The Future of Involvement in Health and Social Care. Warwick: National Centre for Involvement, 2006: 7–16. [Google Scholar]
- 5. Cornwall A, Jewkes R. What is participatory research? Social Science & Medicine, 1995; 41: 1667–1676. [DOI] [PubMed] [Google Scholar]
- 6. Martin J, Matheson J. Responses to declining response rates on government surveys. Social Survey Methodology Bulletin, 1999; 45: 33–37. [Google Scholar]
- 7. Kitzinger J. Qualitative research: introducing focus groups. British Medical Journal, 1995; 311: 299–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Fitzpatrick R, Boulton M. Qualitative methods for assessing health care. Quality in Health Care, 1994; 3: 107–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Webb C, Kevern J. Focus groups as a research method: a critique of some aspects of their use in nursing research. Journal of Advanced Nursing, 2001; 33: 798–805. [DOI] [PubMed] [Google Scholar]
- 10. Buzan T. The Mind Map Book. London: BBC Books, 1993. [Google Scholar]
- 11. Eden C, Jones S, Sims D. Messing About in Problems. Oxford: Pergamon, 1983. [Google Scholar]
- 12. Kern CS, Bush KL, McCleish JM. Mind‐mapped care plans: integrating an innovative educational tool as an alternative to traditional care plans. Journal of Nursing Education, 2006; 45: 112–119. [DOI] [PubMed] [Google Scholar]
- 13. Mueller A, Johnston M, Bligh D. Viewpoint: joining mind mapping and care planning to enhance student critical thinking and achieve holistic nursing care. Nursing Diagnosis, 2002; 13: 24–27. [DOI] [PubMed] [Google Scholar]
- 14. Steyn P, Lindmark G, Noach D. Schering prize for the best poster. Mind mapping can be an affordable method as a tool to do a needs assessment in a developing country with scarce resources. British Journal of Family Planning, 2000; 26: 234–235. [Google Scholar]
- 15. Wilson VJ, McCormack G, Ives G. Understanding the workplace culture of a special care nursery. Journal of Advanced Nursing, 2005; 50: 27–38. [DOI] [PubMed] [Google Scholar]
- 16. Garbett R, McCormack B. The qualities and skills of practice developers. Nursing Standard, 2002; 16: 33–36. [DOI] [PubMed] [Google Scholar]
- 17. Meier P. Mind‐mapping: a tool for eliciting and representing knowledge held by diverse informants. Social Research Update, 2007; 52: 1–4. [Google Scholar]
- 18. Jackson K, Trochim W. Concept mapping as an alternative approach for the analysis of open‐ended survey responses. Organizational Research Methods, 2002; 5: 307. [Google Scholar]
- 19. Northcott N. Cognitive mapping: an approach to qualitative data analysis. Nurs Times Research, 1996; 1: 456–463. [Google Scholar]
- 20. Lincoln YS. Emerging criteria for qualitative and interpretive research. Qualitative Inquiry, 1995; 3: 275–289. [Google Scholar]
- 21. Hunter D, Lang A. The Leeds Declaration. Leeds: Nuffield Institute for Health, 1993. [Google Scholar]
- 22. Krueger RA. Analyzing focus group interviews. Journal of Wound, Ostomy & Continence Nursing, 2006; 33: 478–481. [DOI] [PubMed] [Google Scholar]
- 23. Halcomb E, Davidson P. Is verbatim transcription of interview data always necessary? Applied Nursing Research, 2006; 19: 38–42. [DOI] [PubMed] [Google Scholar]
- 24. Scott SD, Sharpe H, O’Leary K et al. Court reporters: a viable solution for the challenges of focus group data collection? Qualitative Health Research, 2009; 19: 140–146. [DOI] [PubMed] [Google Scholar]
- 25. Eden C. Analyzing cognitive maps to help structure issues or problems. European Journal of Operational Research, 2004; 159: 673–686. [Google Scholar]
- 26. Tattersall C, Watts A, Vernon S. Mind mapping as a tool in qualitative research. Nursing Times, 2007; 103: 32–33. [Google Scholar]
- 27. Krueger RA. Moderating Focus Groups. London: Sage, 1997. [Google Scholar]
- 28. Morgan DL. Focus Groups as Qualitative Research, 2nd edn London: Sage, 1997. [Google Scholar]
- 29. Cooperrider DL, Whitney D. Collaborating for Change: Appreciative Inquiry. San Francisco: Berrett‐Koehler, 1999. [Google Scholar]