

Abstract
Background
Subjective expectations regarding future health are rarely studied, yet may have implications for medical decision making, health behaviour and health economic analysis.
Objective
To study people's subjective expectations regarding length and future quality of life in Hungary and compare these with previous findings from the Netherlands.
Methods
A cross‐sectional survey was performed, using a questionnaire that was put on a highly frequented web journal during 1 day. Main socio‐demographic variables and health status of the voluntary participants were registered using the EQ‐5D questionnaire. People were asked about the age they expected to live and the health status they expected to have at ages 60, 70, 80 and 90, using the EQ‐5D descriptive system. Responses were matched and compared to age‐ and gender‐specific life expectancy data from the Hungarian National Statistics and to age‐ and gender‐specific EQ‐5D scores from a prior nationally representative survey in Hungary.
Results
In total, 9407 people were included in the analysis with mean age of 36.1 (SD 10.6) years, mainly qualified (degree 74.0%), employed (86.0%) men (67.1%). People overestimated their life expectancy (women, 1.6; men, 8.2 years) and expected a sharp deterioration in health at the age 70. Age, current health status, perception of a healthy lifestyle and kins' age at death were important explanatory factors for subjective expectations. Subjective life expectancy correlates strongly with expected future health status.
Conclusions
The striking similarities between two surveys from distinct nations suggest that people's (mis)expectations regarding length and future quality of life are probably rather generalizable between jurisdictions within Europe.
Keywords: ageing, expectations, health status, Hungary, longevity
Life is largely a matter of expectation. (Horace)
Background
Expectations regarding future events may importantly influence current actions of individuals. The area of health is no exception. If someone dies in his or her thirties, we feel that it happened unfairly early, as we normally expect to live beyond that age. We consider it normal to see a young man speeding up to catch the bus, but we admire when a 90‐year‐old person does the same, as we expect the ability to run to decline beyond a certain age. While such expectations are, in general terms, in line with objective data (http://www.eurofound.europa.eu/), they may nonetheless not be completely accurate.1 This is important because health‐care interventions aim to improve health in terms of length and/or quality of life. A patients' evaluation can play a decisive role in medical decision making, uptake of interventions and sustained compliance.2 If patients' subjective expectations strongly differ from objective expectations, their decisions may result in suboptimal behaviour.
Brouwer and Van Exel3 investigated people's subjective expectations regarding length and future quality of life in the Netherlands. They found that respondents significantly overestimated their life expectancy but appeared to underestimate future health‐related quality of life from age 70 onwards. Regression analyses revealed that age, current health status and perception of current lifestyle were especially important explanatory variables of peoples's own expectations regarding length and quality of life.3
However, these Dutch findings are not necessarily generalizable for other countries. Life expectancy at birth differs strongly among populations across Europe, and gender‐/age‐matched health status varies substantially as well. For instance, life expectancy at birth in Hungary is about 6.4 years shorter than in the Netherlands (http://www.oecd.org), and for instance, health status of women in the age group 70–79 years is on average 54.5 (SD = 22.1) in Hungary and 79.7 (SD = 15.8) in the Netherlands, measured on a 0–100 visual analogue scale (VAS) (with 100 representing best imaginable and 0 worst imaginable health).4
Given such epidemiological differences between countries, one would expect differences in expectations regarding length and quality of life between jurisdictions. Furthermore, it would be interesting to study the generizability of response patterns and the explanatory factors of expectations. Therefore, we investigate whether the patterns (and the predictors) of over‐ and underestimations of length and future quality of life in Hungary resemble those in the Netherlands. We, therefore, employ similar methods as used in the Dutch study to be able to directly compare the results.
Objectives
The purpose of this study was to assess people's subjective expectations regarding length and future health‐related quality of life in Hungary and to compare these with more objective figures. We moreover aimed to analyse the determinants of people's subjective expectations and, finally, to compare the results with findings from the Netherlands.
Methods and participants
Set of questions applied
We used the questionnaire developed and applied by Brouwer and Van Exel3 to avoid differences owing to methodological differences. The survey included questions on basic demographic data: gender, age, marital status, highest education level, occupation and net monthly income. Smoking status, having healthy lifestyle compared to others and kins' age at death were also surveyed. Ethnic background was not asked in the Hungarian version, because this is not allowed in Hungary. (Note also that the proportion of foreign citizens is insignificant in Hungary; i.e. 0.9% in 2008.)
Health status of the participants was expressed as a utility score, using the official Hungarian version of the EuroQol questionnaire. The EuroQol consists of two pages comprising the descriptive system (EQ‐5D) and the VAS (EQ‐VAS).1 The descriptive part covers five general aspects of health: mobility, self‐care, usual activity, pain/discomfort and anxiety/depression. The respondent was asked to indicate his/her health state by ticking in the box indicating the most appropriate statement (no problem, some problems, major problems) in each of the five dimensions, making a total of 243 possible health states. Utility scores for all health states were based on UK tariffs, because no Hungarian EQ‐5D tariffs exist. The same UK utility scores were used to compute reference values for health in a representative sample (n = 5503) of the general population in Hungary.5 The second part of the EuroQol questionnaire is a vertical VAS ranging from 0 to 100, where 100 represents the best and 0 the worst imaginable health state. Respondents rated their current health state by marking the appropriate point on the EQ‐VAS.
In the second section of the survey, respondents were queried about the age they themselves expected to reach. Regarding future health, people were asked to indicate the health‐related quality of life they expected to have at ages 60, 70, 80 and 90, respectively. For this purpose, the statements were formulated based on the EQ‐5D descriptive system. Respondents were asked to tick the level of problem (no, some, major) for each dimension of the EQ‐5D (mobility, self‐care, usual activity, pain/discomfort, anxiety/depression) they expect to have at ages 60, 70, 80 and 90, respectively (Appendix). Respondents who had already reached the given age were asked to proceed to the next question in order to only observe expectations. The questionnaire was translated into Hungarian in collaboration with the Dutch researchers. The EQ‐5D‐related points were formulated based on the wording of the validated Hungarian EQ‐5D version.
Web‐based survey
We created a web‐based design of the questionnaire. This was also a main source in the Dutch study, again to increase comparability and to reach large numbers of respondents. The survey was performed in collaboration with a highly frequented Hungarian web journal called ‘Index’ (journal site: http://index.hu/) on the 26th of November 2008. The questionnaire was put on the main page of the journal in the morning for 4 h. Subsequently, it could be reached through a link available from the front page until midnight. The survey was structured in such a way that people were first asked about their expectations regarding future health‐related quality of life. Next, we asked about their subjective life expectancy, after which questions followed regarding their next of kin's age of death. The web surface allowed people to go back, review and change previous responses.
Comparison with actual expectancies
Subjective life expectancy was compared to objective life expectancy on an individual basis, using age‐ and gender‐specific actual life expectancy data. These data were obtained from the Hungarian National Statistics (http://www.ksh.hu). This ensured that subjective expectations of, for instance, a 55‐year‐old woman, were compared to her objective expectations. Expected health status at the included ages was compared on an individual level, also using gender‐ and age‐matched EQ‐5D scores of a representative survey in Hungary.5
Statistical analysis
IBM SPSS, Release 20.0 (IBM, Armonk, NY, USA) was used for the analysis. Besides descriptive statistics, we used linear regression analysis to investigate factors associated with subjective expectations regarding length of life and the difference between subjective and objective expectations regarding length of life. Logistic regression was applied to analyse the explanatory factors of life expectation overestimation. A cox regression (survival model) was carried out to investigate the covariates that influence the time respondents expect to live until death occurs. Finally, linear regression analysis was performed to investigate factors associated with subjective expectations of their future quality of life (EQ‐5D scores at ages 60–90).
Results
General characteristics
A total of 15 300 respondents were rooted into the questionnaire during the 16 h (from 8.00 am until midnight) the questionnaire was online. Uncompleted cases were filtered out, and only respondents aged 18–100 years, answering the gender question and expecting to live to at least current age, were considered for the analysis. A sample of 9407 people was included with mean age of 36.08 (SD = 10.619) years. Demographic data and main characteristics are presented in Table 1. Demographic characteristics of the study sample showed that it is not representative of the general population. Men (67.1%) were overrepresentated, as well as married people (64.3%), because these comprise 46.8% and 49.2% of the general Hungarian population, respectively, in 2008. The proportion of singles was representative (29.9 vs. 29.0%), but divorced respondents were underrepresented (5.4 vs. 9.4%). The low rate of widowers (0.8 vs. 12.2% in the general population) is probably related to the relatively young age of the study group. Degree (BSc, MSc) as highest educational level occurred much more frequently in the study than in the general adult population (42.7 vs. 13.0%) along with a lower rate of high school level (respondents: 30.9%, general population: 48.0%). Most respondents were employed (85.8%), only a few were retired (2.4%), while unemployed people did not participate in the study. Most of the respondents (58.1%) had more than 560 euros as their net monthly income, which is higher than the average net monthly income of employees in Hungary (i.e. 468 Euros). (Conversion 1 Euro = 261 HUF).
Table 1.
Sample characteristics (N = 9407) and general population (GP) reference values for gender, age, marital status and highest educational level
| Variable | Category | N | % | GP% |
|---|---|---|---|---|
| Gender | Female | 3099 | 32.9 | 53.2 |
| Male | 6308 | 67.1 | 46.8 | |
| Age (years) | 18–24 | 1085 | 11.5 | 15.2a |
| 25–34 | 3912 | 41.6 | 18.6 | |
| 35–44 | 2519 | 26.8 | 16.3 | |
| 45–54 | 1200 | 12.8 | 17.5 | |
| 55–64 | 599 | 6.4 | 14.1 | |
| 65–74 | 81 | 0.9 | 10.5 | |
| 75–84 | 9 | 0.1 | 6.5 | |
| ≥85 | 2 | 0.0 | 1.3 | |
| Marital status | Married/living together | 6044 | 64.3 | 49.2 |
| Single | 2785 | 29.6 | 29.0 | |
| Divorced | 505 | 5.4 | 9.4 | |
| Widow | 73 | 0.8 | 12.2 | |
| Highest education level | Primary | 50 | 0.5 | 27.8a |
| Secondary | 2438 | 25.9 | 43.0 | |
| High school | 2904 | 30.9 | 8.3 | |
| University | 4015 | 42.7 | 4.7 | |
| Employment status | Full‐time job | 7665 | 81.5 | – |
| Part‐time job | 403 | 4.3 | – | |
| Pensioner | 223 | 2.4 | – | |
| Disability pensioner | 66 | 0.7 | – | |
| Student | 711 | 7.6 | – | |
| Housewife | 339 | 3.6 | – | |
| Net income (€/month) | 0–249 | 814 | 8.7 | – |
| 250–400 | 1315 | 14.0 | – | |
| 401–560 | 1819 | 19.3 | – | |
| 561–900 | 2584 | 27.5 | – | |
| 901–2260 | 2235 | 23.8 | – | |
| ≥2261 | 638 | 6.8 | – | |
| Health status (EQ‐VAS score) | 0–24 | 327 | 3.5 | – |
| 25–49 | 322 | 3.4 | – | |
| 50–74 | 2213 | 23.5 | – | |
| 75–100 | 6545 | 69.6 | – | |
| Smoking status (>5 cigarettes/day) | Yes | 1695 | 18.0 | – |
| No | 7697 | 82.0 | – | |
| Healthy lifestyle | Healthier than most others | 3802 | 40.4 | – |
| Comparable to others | 4476 | 47.6 | – | |
| Less healthy than most others | 1127 | 12.0 | – | |
| Kins' age at death (years) | <55 | 36 | 0.4 | – |
| 55–65 | 357 | 3.8 | – | |
| 65–75 | 2331 | 24.8 | – | |
| 75–85 | 4843 | 51.5 | – | |
| 85–95 | 1179 | 18.9 | – | |
| >95 | 61 | 0.6 | – |
Age group, 15–24 years.
The rate of people with educational level lower than primary school is 16.2%.
Health status of the respondents
The average health status in our sample was 0.85 (SD = 0.18) when using the EQ‐5D tariffs and 76.6 (SD = 19.2) when using the VAS. Altogether, a total of 2862 (30.4%) participants indicated on the VAS to have a health score below 75, while the majority (n = 6380, 67.8%) of respondents scored their health in the range of 75–99 on the VAS. A total of 165 respondents (1.8%) indicated to be in perfect health, that is, had the maximum score of 100 on the VAS. Comparing the EQ‐5D scores of the sample with gender‐ and age‐matched population‐based data in Hungary, we found no significant difference.5
Expectations on length of life
The results related to expectations regarding length of life are presented in Table 2. Subjective expectations regarding length of life ranged between 24 and 100 years. We observed 68 distinct expected ages of death. The median expected age of death was 80 years for both genders; 16.5% of the respondents expected to live until age 80. Ages 85, 75, 70 and 90 were also frequently indicated (12.0, 11.0, 9.5 and 8.0%, respectively) in this open‐ended question. Analysis by age groups revealed that the median subjective expectation regarding length of life was 80 years in all age groups between 18 and 64 years. However, it was higher among the older respondents (with median values of 85.0 and 97.5 years in age groups 65–84 and ≥85 years, respectively).
Table 2.
Comparison of subjective and actual (age‐ and gender‐specific) life expectancy of respondents, according to sample characteristics
| Variable | Category | Life expectancy (years), mean (SD) | ||
|---|---|---|---|---|
| Self‐estimate | Actual | Difference | ||
| Total sample | 79.58 (10.83) | 73.54 (3.84) | 6.04 | |
| Gender | Female | 80.27 (10.06) | 78.63 (0.89) | 1.64 (10.06) |
| Male | 79.25 (11.17) | 71.05 (1.64) | 8.20 (11.16) | |
| Age (years) | 18–24 | 78.39 (12.12) | 72.65 (3.79) | 5.74 (12.45) |
| 25–34 | 79.21 (11.33) | 72.77 (3.67) | 6.45 (11.77) | |
| 35–44 | 79.96 (10.4) | 73.16 (3.51) | 6.81 (10.71) | |
| 45–54 | 80.01 (9.90) | 75.18 (3.40) | 4.85 (10.51) | |
| 55–64 | 80.87 (8.26) | 77.38 (2.74) | 3.48 (8.63) | |
| 65–74 | 84.80 (7.13) | 80.17 (1.94) | 4.63 (7.17) | |
| 75–84 | 86.33 (5.41) | 84.28 (1.28) | 2.05 (5.04) | |
| ≥85 | 97.50 (3.54) | 93.39 (4.36) | 4.11 (0.82) | |
| Marital Status | Married/living together | 80.06 (10.20) | 73.72 (3.76) | 6.34 (10.64) |
| Single | 78.44 (12.09) | 72.59 (3.64) | 5.86 (12.48) | |
| Divorced | 80.29 (10.36) | 75.84 (3.88) | 4.45 (10.70) | |
| Widow | 79.26 (10.87) | 79.27 (3.49) | −0.01 (10.5) | |
| Highest education level | Primary | 72.61 (16.87) | 74.77 (5.23) | −2.16 (16.47) |
| Secondary | 77.39 (11.48) | 73.37 (3.88) | 4.01 (11.96) | |
| High school | 79.52 (10.66) | 73.54 (3.81) | 5.98 (10.98) | |
| University | 81.05 (10.17) | 73.62 (3.82) | 7.43 (10.66) | |
| Employment status | Full‐time job | 79.55 (10.65) | 73.29 (3.69) | 6.26 (11.06) |
| Part‐time job | 81.56 (10.52) | 74.75 (4.02) | 6.81 (10.81) | |
| Pensioner | 82.20 (8.88) | 78.92 (3.13) | 3.28 (8.80) | |
| Disability pensioner | 71.71 (9.16) | 76.32 (3.6) | −4.61 (8.93) | |
| Student | 78.95 (12.46) | 72.37 (3.68) | 6.55 (12.88) | |
| Housewife | 79.12 (11.91) | 75.96 (3.59) | 3.16 (12.21) | |
| Net income (€/month) | 0–249 | 77.07 (13.37) | 73.57 (4.05) | 3.50 (13.75) |
| 250–400 | 78.43 (11.08) | 74.68 (4.11) | 3.75 (11.66) | |
| 401–560 | 79.14 (10.88) | 74.37 (4.04) | 4.77 (11.29) | |
| 561–900 | 79.90 (10.14) | 73.55 (3.80) | 6.35 (10.37) | |
| 901–2260 | 80.39 (10.39) | 72.59 (3.36) | 7.80 (10.55) | |
| 2261 ‐ | 82.35 (9.76) | 72.15 (2.78) | 10.20 (10.10) | |
| Health status (EQ‐VAS score) | 0–74 | 75.10 (11.65) | 74.05 (3.95) | 0.81 (11.97) |
| 75–99 | 78.97 (10.08) | 73.57 (3.82) | 5.40 (10.42) | |
| 100 | 83.00 (9.27) | 73.23 (3.76) | 9.78 (9.81) | |
| Smoking status (>5 cigarettes/day) | Yes | 75.53 (11.8) | 73.19 (3.77) | 2.34 (12.1) |
| No | 80.48 (10.4) | 73.61 (3.85) | 6.86 (10.87) | |
| Healthy lifestyle | Healthier than most others | 82.72 (9.71) | 73.63 (3.83) | 9.09 (10.30) |
| Comparable to others | 78.64 (10.29) | 73.69 (3.91) | 4.95 (10.82) | |
| Less healthy than most others | 72.78 (12.56) | 72.64 (3.49) | 0.14 (12.69) | |
| Kins' age at death (years) | <55 | 62.17 (19.47) | 73.96 (4.06) | −11.79 |
| 55–65 | 70.75 (12.71) | 73.71 (3.90) | −2.96 | |
| 65–75 | 75.1 (10.31) | 73.32 (3.74) | 1.78 | |
| 75–85 | 80.4 (9.81) | 73.49 (3.82) | 6.91 | |
| 85–95 | 85.08 (9.60) | 73.90 (3.96) | 11.18 | |
| More than 95 | 87.54 (12.01) | 74.17 (4.81) | 13.37 | |
The comparison of participants' subjective expectations regarding length of life with gender‐ and age‐matched actual statistical life expectancy of the Hungarian population is also presented in Table 2. On average, we found an overestimation of length of life; 71.3% of the respondents overestimated his/her life expectancy. The difference was especially large for men. Widows, people with low educational level (primary school), disability pensioners and respondents whose next of kins died early (at age <55 or between 55–65 years) on average expected to live shorter than their age‐ and gender‐matched statistical life expectancy. The most (unrealistically) optimistic expectations were held by respondents with the following characteristics: male, 35–44 years old, married, having a degree, working part‐time, having a high income (>2261 Euro/month), having the maximum score (100) on the VAS, being non‐smoker, considering to have a healthier lifestyle than most others and having next of kins who died when they were over 95 years old. (Table 2)
Future health‐related quality of life
The questions concerning subjective expectations regarding future quality of life pertained to the ages 60, 70, 80 and 90. This age range was relevant for the majority of the sample (in terms of being ages reached in the future) as 9141 (97.8%) of the participants were aged below 60, while 9375 (99.7%) were aged below 70. Only 3 and 1 respondents were aged over 80 and 90 years, respectively. Participants expected a rapid decline in health with age. The health status people expected to have at age 60 was similar to the average observed health of the present 60‐year‐olds in the population. However, a sharper decline in health was expected from age 70, which causes a clear gap between subjective expectations and observed health status in the elderly Hungarian population, which broadened further for ages 80 and 90 (Fig. 1). People appear to unduly expect low health levels at older ages, therefore.
Figure 1.
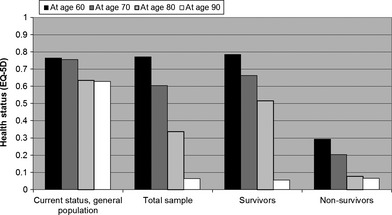
Expectations regarding health‐related quality of life for certain ages: separating ‘expected survivors’ and ‘expected non‐survivors’.
Not all respondents expected to live until the ages presented in the future quality of life questions (i.e. 60 up to 90). One may consider expectations regarding future health at ages one does not expect to live to be less meaningful. Hence, in Fig. 1, we show the difference in expectations between respondents expecting to be alive at a given age (‘expected survivors’) and those not expecting to live at a given age (‘expected non‐survivors’). This figure highlights, unsurprisingly, the former clearly have (significantly) better expectations than the latter for all future ages, except age 90 where the difference is negligible.
Determinants of expectations
Table 3 contains information on the factors associated with subjective expectations. Owing to the large sample size, nearly all variables had a statistically significant relation to subjective expectations regarding age of death, with the exception of certain employment status (P < 0.05). In addition, current age of the respondents did not significantly influence the overestimation of remaining life duration (logistic regression). Expected survival duration, moreover, was not affected by gender and marital status of the respondents (Cox regression).
Table 3.
Regression analysisa
| Variable | Life expectancyb | Health‐related quality of life expectancyc | |||||
|---|---|---|---|---|---|---|---|
| Subjective expectation | Difference subjective‐objective | Overestimating life expectancyd | Survival model (Cox regression)e | At age 60 | At age 70 | At age 80 | |
| Gender | −0.038* | 0.272* | 2.347* | – | – | – | – |
| Age | 0.078* | −0.031** | – | 0.996* | 0.090* | 0.080* | 0.054* |
| Marital status | 0.027* | 0.032** | 1.230* | – | – | – | – |
| Educational level | 0.048* | 0.043* | 1.154* | 0.945* | 0.044* | 0.052* | 0.042* |
| Employment status | |||||||
| Full‐time job | −0.058* | – | – | 1.157* | −0.038* | −0.043* | −0.038* |
| Part‐time job | – | 0.032* | 1.533** | – | – | – | – |
| Pensioner | – | – | – | – | 0.020*** | – | – |
| Disability pensioner | −0.030* | −0.020*** | 0.310* | 1.755* | −0.037* | −0.038* | – |
| Student | – | 0.026*** | 1.737* | – | – | – | – |
| Net income | 0.038* | 0.040* | 1.001* | 1.000** | 0.031** | 0.028** | 0.034* |
| Health status (EQ‐VAS score) | 0.246* | 0.233* | 1.029* | 0.988* | 0.499* | 0.404* | 0.319* |
| Smoking status | −0.069* | −0.066* | 0.641* | 1.163* | – | – | – |
| Healthy lifestyle | 0.162* | 0.157* | 1.791* | 0.789* | 0.131* | 0.152* | 0.170* |
| Kins' age at death | 0.302* | 0.288* | 1.092* | 0.965* | 0.108* | 0.149* | 0.152* |
| R 2 | 0.27 | 0.32 | 0.30 | 0.34 | 0.34 | 0.21 | |
Standardized coefficients are presented. Statistical significance of coefficients: *P < 0.001; **P < 0.01; ***P < 0.05.
Coding used for the analysis: gender: female = 0, male = 1; marital status: not married = 0, married = 1; highest educatonal level: primary school = 1, secondary school = 2, college = 3, university = 4; net monthly income: mean values of net income ranges presented in Table 1 were used for the analysis; smoking status: no = 0, yes = 1; healthy lifestyle: less healthy than most others = 1, comparable to most others = 2, healthier than most others = 3; kins' age at death: mean values of ranges presented in Table 1 were used for the analysis.
Dependent variable: subjective life expectancy and difference between subjective and actual expectancy. Predictors: age, kins' age at death, monthly net income, health status (EQ‐5D score), gender, marital status, highest educational level, full‐time employed, part‐time employed, pensioner, disability pensioner, student, smoking status, healthy lifestyle. Method: stepwise, entry/removal criteria: 0.05/0.10.
Dependent variable: subjective expectation of future HRQoL. Predictors: age, kins' age at death, monthly net income, health status (EQ‐5D score), gender, marital status, highest educational level, employed in full‐time job, employed in part‐time job, pensioner, disability pensioner, student, smoking status, healthy lifestyle. Method: stepwise, entry/removal criteria: 0.05/0.10.
The binary dependent variable ‘Overestimation’ takes the value 1 if one overestimates his/her age and zero value otherwise. Based on corresponding logistic regression results, the odds ratio (OR) inflator factor estimates the impact of the predictor considered on the Prob (Over)/Prob (Under) risk ratio. Hence, an OR >1 indicates an overestimation effect in a percentage sense while OR with <1 indicates the opposite direction. Note, that predictor with an OR close to 1 is irrelevant. For instance, the multiplicative impact of the ‘Educational level’ is 1.154, that is, a 15.4% increase in the Odds.
The interpretation of the Cox survival hazards is similar to the ‘Overestimation’. The only difference is the meaning of the so‐called ‘hazard’ term. The hazard is the risk of that one survives a particular age and then terminates instantly. For instance, the multiplicative impact on the risk of the ‘Educational level’ is 0.945, measuring a 5.5% decline in the hazard.
A number of results deserve attention. The variables kins' age at death, current health status, perceived healthy lifestyle relative to others and current age were most strongly associated with subjective expectations regarding length of life (all in the expected direction; see Table 3). In explaining the difference between objective and subjective expectations, a similar pattern was observed. There, the variables kins' age of death, current health and net income were most strongly associated with overestimation of average objective expectations, as well as gender, with men strongly overestimating objectively expected length of life. Here, lifestyle was less prominent. The Cox regression (investigating survival) indicated that expected survival was mainly associated with current age, kins' age of death, net income and current health.
Multivariate regression analysis was not suitable to explain expected health at age 90, because the R 2 of the full model turned out to be just 0.002. Expected health at ages 60, 70 and 80 was mainly associated with current health, lifestyle, kins' age of death and current age, all in the expected direction.
We also analysed the relationship between the subjective expectations regarding length of life and those regarding future quality of life. For this exploratory analysis, we performed an ordinary least squares regression, in which the dependent variable was the subjective expectation regarding remaining length of life (measured in days) and independent variables were the expected health levels at ages 60, 70, 80 and 90 (which could have negative values). Estimation results are shown in Table 4 and show that, with the exception of expected health at age 90, the associations between the expectations regarding length and quality of life were all statistically significant and positive. If these associations would be interpreted in a more causal way than considered defendable here, the results imply that when expected health at age 60 increases by one unit on its scale, the expected number of days lived increases by 32.5 days. Given the fact that we cannot claim anything about causality (which may well run in the other direction), we emphasize the fact that these results should be interpreted as associations.
Table 4.
Regression analysis of expected length of life and expected health‐related quality of life at ages 60, 70, 80 and 90a
| Variable | Unstandardized coefficients | Standardized coefficients | |||
|---|---|---|---|---|---|
| B | Standard error | β | t | Significance | |
| Expected health status at age… | |||||
| 60 years | 32.46 | 2.018 | 0.23 | 16.081 | 0.000 |
| 70 years | 14.82 | 1.818 | 0.14 | 8.154 | 0.000 |
| 80 years | 17.76 | 1.100 | 0.22 | 16.138 | 0.000 |
| 90 years | −0.86 | 0.637 | −0.01 | −1.345 | 0.179 |
| Constant | 25054.1 | 110.5 | 226.8 | 0.000 | |
Dependent variable: self‐expectation on length of life measured in days.
Comparison with results from the Netherlands
Given the very similar study designs, it is interesting to compare our results to those in the Dutch study (Brouwer and Van Exel3). In both studies, the average age of participants was relatively low (Hungary: 36.1 years, the Netherlands: 33.6 years), and partly as a result, an overrepresentation of healthy, highly educated people was observed.3 Overestimation of life expectancy was strikingly similar in both countries (women: 1.6 vs. 1.7 years; men: 8.2 vs. 7.0 years, respectively). Both studies observe the expected sharp decline in health after the age of 70 (Fig. 2). These expectations regarding future health were clearly below observed health in the elderly populations in both countries.3, 5 Current age and health, lifestyle and kins' age of death were importantly associated with subjective expectations regarding length of life in both studies.
Figure 2.
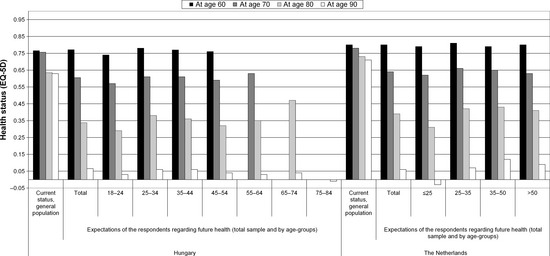
Comparison of the expected health status with the actual health values of the general population at ages 60, 70, 80 and 90 in Hungary and in the Netherlands.3, 5
The difference between subjective expectations regarding longevity and (average) objective figures on life expectancy was associated with similar variables as well in the two studies: current health, lifestyle, kins' age of death and gender. Current age, current health and lifestyle were strongly associated with expectations regarding health‐related quality of life at older ages in both samples as well. However, in the current study, kins' age of death was associated with these expectations as well, while this association was not significant in the Dutch study. Sample size may play a role here. Finally, positive associations were detected in both studies between expectations regarding length and future quality of life.
Discussion
In this study, we surveyed the expectations regarding length and future health‐related quality of life in a non‐representative sample from the Hungarian general public, using an internet‐based questionnaire. In our sample, young and middle‐aged, qualified, employed men were overrepresented, which needs emphasis. In general, respondents (especially men) appear to overestimate the length of life relative to the average objective figures. However, they sharply underestimate their health at the age of 70, when compared to national statistics. These results show striking resemblance with the Dutch findings (Brouwer and Van Exel3). Moreover, these findings can have important implications for health policy, for instance, aimed at influencing unhealthy habits, as well as medical decision making.
The apparent overestimation of length of life (relative to objective estimates) deserves careful interpretation. Men clearly overestimate length of life to a larger extent than women do (8.2 vs. 1.6 years). For women, the estimation of life expectancy (in relation to current national figures) may be considered fairly accurate for two reasons. First, our respondents were relatively young, and therefore, this question involved estimating the timing of an event typically 30–50 years later in time. A difference of 1.6 years with objective figure may be considered fairly accurate, in that sense, in particular, also considering that education and employment status in the sample were somewhat higher than in the general population. Second, the statistical data on actual life expectancy contain uncertainty regarding forecasts as well. The average difference of 1.6 years in women's expectations is, therefore, negligible. This does not hold, however, for the 8.2 years difference in men's subjective and objective expectations.
Another important thing to note is that adjusting expectations regarding length of life upwards may be fully rational given the increasing life expectancy in many countries, including Hungary. Life expectancy at birth in Hungary has been increasing continually for women in the past 60 years (from 63.4 to 77.8 years between 1949 and 2008, an increase of 14.4 years). Men's life expectancy at birth increased less in the same period (from 59.3 to 69.8 years, an increase of 10.5 years). In the past two decades (1990–2008), a similar increase was observed for men and women, that is, 4.1 years for women and 4.7 years for men. This indicates that an overestimation relative to current figures is rational if growth in life expectancy is expected to continue. These figures cannot explain the observed difference in overestimation between the two genders, however. Note also that the expected growth in life expectancy in turn may be related to difficult assumptions regarding future health care, environment, safety and so on. Investigating the origins of expectations in that sense is an important topic for future research.
A final remark is that we used national (age‐ and gender‐specific) averages to compare individual expectations to. It is clear that people may rightfully expect to live longer (or shorter) than this average, for instance, when they are relatively wealthy or living healthily. Some of the main variables associated with a higher subjective expectation regarding length of life indeed point in that direction. For instance, when one observes next of kins becoming relatively old, this may rightfully increase own expectations (e.g. due to genetic factors). Current age also is a logical influence in that context, as well as lifestyle variables. With a relatively wealthy and healthy sample, relatively positive expectations may be fully justified, as the objective figures here were not corrected for such factors. Given the recruitment strategy employed here, resulting in a non‐representative sample, such considerations are particularly relevant in interpreting our findings.
An important finding was the sharp decline people expect in health at the age of 70. While the expected health level at age 60 was similar to the observed health in people of that age, expected health at ages 70, 80 and 90 were far below observed health in those age groups. This large difference may occur because of a lack of awareness regarding actual health of elderly or selective observation of elderly in poor health. Another explanation may be that young and old people differ in their interpretation of the descriptions of the EQ‐5D, for example, due to adaptation. For instance, if a young man sees a 70‐year‐old person walking slowly to a grocery store, he may interpret this as having ‘some problems in walking about’ (hence the slow speed). On the other hand, the 70‐year‐old may have adapted to this speed and compared himself to other elderly and thus may have interpreted his state as ‘no problem in walking about’. Such discrepancies in health perception between observers and affected people have been frequently noted in the literature on quality of life.6 While such differences in interpretation may always be present between people of different age groups, these may be especially important in the context of the current study. This holds because we asked relatively young people to predict future health on the EQ‐5D. These young people may therefore have a different interpretation of the EQ‐5D descriptions in predicting future health than the elderly who provided the ‘objective figures’. Such a discrepancy would lead to a sharper decline in predicted health than observed health, which is exactly what we observe. It seems highly unlikely, however, that this would explain the full gap between observed and expected future health.
The comparison between our results and those from the Dutch study is interesting, but should be made with some caution. While in both studies, the majority of the participants was relatively young and healthy, the current study had a relatively large proportion of men (67 vs. 45% in the Dutch study). Interestingly, a similar proportion of the participants in both studies perceived to have a healthier lifestyle than most others (Netherlands: 43%, Hungary: 40.4%). Many respondents in both studies reported that the age of death of their close relatives was between 75 and 85 years (49.0 and 51.5%). The rate of smokers was clearly higher in the Netherlands (34.0 vs. 18.0%).
On average, respondents in the Dutch study expected to live longer than those in the Hungarian study (mean, 83.2 vs. 79.6 years), which is to be expected given differences in objective life expectancy between the two countries. Nevertheless, the patterns in the expectations and associated variables in the two countries are remarkably similar. In both studies, respondents, especially men, appear to overestimate length of life, yet underestimate their future quality of life. Moreover, current age, current health and lifestyle were the main factors associated with own expectations regarding length and quality of life, and age of death of relatives and smoking were strongly associated with subjective life expectancy.
We are not the first to investigate subjective expectations regarding length and future quality of life. Most studies to date, however, were only concerned with length of life. Most of these existing studies were conducted in the United States. Mirowsky (7), for instance, reported that men expected to live longer than actuarial estimates (on average 3 years). Afro‐Americans moreover expected to live about 6 years longer than actuarial estimates. Family relationships, informal health and social support also contributed to long‐life expectations. The role of lifestyle was confirmed as well, that is, people who smoke, drink heavily and have poor nutritional habits expect shorter lives and those who walk and exercise regularly expect longer lives.7, 8, 9 Perozek10 argued that individuals are uniquely qualified to predict their own mortality based on their own genetic background, as well as environmental and behavioural risk factors that are often known only to the individual. Smith et al.11 indeed show that people can predict their own demise and that subjective expectations are ‘a fairly accurate index of personal survival probability, both in its responsiveness to events that experts would suggest increase the odds of death and as a prediction of future mortality’. Smith12 reported that experiencing a catastrophe, such as a hurricane, can also significantly reduce people's longevity estimations. Perozek10 points out that individuals' expectations about survival probabilities may provide additional information to demographers and policymakers in their challenge to predict mortality. Lang et al.13 explored desires regarding length of life and end of life in German adults, showing desired lifetime to be consistently around 85 years with few age differences. Popham et al.14 investigated expectations in British adults. Just under a quarter of respondents did not think it likely they would live to 75 years or older. People in sustained lower socio‐economic positions were more likely to be pessimistic about their life expectancy. Furthermore, smoking was associated with poorer self‐rated health and low self‐rated life expectancy, with 49% of the heaviest smokers being pessimistic about their longevity.14 Our results compare well to those reported in the literature, therefore.
It needs emphasis that evidence on expectations regarding future quality of life is scarce. More investigation of these expectations appears warranted, especially because the patterns of these expectations clearly differ from those regarding length of life. Unduly low expectations regarding future health may have important implications, for instance, for the subjective assessment of benefits of health programmes such as those improving health behaviour. If people need to reduce current pleasures (eating, drinking, smoking) to gain additional years of life at the end of their lives, these benefits may be perceived as too small a reward to justify the costs if the gained years are expected to be lived in poor health. This implies that wrong expectations may lead to wrong behavioural decisions.
People's concerns about future health and longevity have several other implications as well. For instance, a new method has been developed in the past years to assess 10‐year osteoporotic fracture risk, the so‐called FRAX® algorithm.15 Perception and evaluation of a 10‐year hip fracture risk are likely to differ between patients who expect to live no longer than five more years and those who expect to live for at least another 20 years. As a consequence, acceptance of and compliance with a long‐term antiporotic drug regimen may also be affected by these expectations. Discussions on and information about future health and length of life could help patients to make better informed decisions and to more accurately plan for the future.
The fact that people may hold explicit expectations regarding length and quality of life may also affect preference elicitation techniques. In health economics, for instance, the time trade‐off (TTO) method is often used to assess the utility of health states. A typical TTO exercise asks respondents to choose between living longer in poorer health and living shorter in better health. If respondents have different subjective expectations regarding their lifespan and quality of life than the ones presented in the exercise and do not fully abstract from those, TTO scores may be influenced by these subjective expectations. van Nooten and Brouwer and van Nooten et al. indeed report such influences. These findings support the relevance of our results not only in medical communication, decision making and compliance but also in health economic methodology.16, 17
A number of limitations of our study need noting. Our sample was not fully representative as healthy, young and employed men more often participated in this web‐based survey. To achieve comparability with the previous Dutch study, we applied a very similar questionnaire. We decided not to expand on this questionnaire (e.g. also using more detailed quality of life instruments or questions regarding lifestyle, marital status, etc.) in order to keep the questionnaire short (given the administration strategy). Future research could attempt to ask more detailed background questions. For instance, easy access to health‐care facilities or having relatives suffering from chronic or degenerative illnesses may influence subjective expectations regarding length and future quality of life. Another interesting research question for future research relates to knowledge about (average) objective life expectancy in one's home country or how certain behaviours and characteristics objectively influence length and quality of life.
It needs noting that the way in which the web‐survey was structured and administered may have influenced our results. For instance, the fact that we started with expectations regarding future health up to the age of 90 may have influenced the answers regarding expected age of death. We could not test this further. In addition, it may be possible that people answered the questionnaire more than once, since the website did not preclude this. We do stress that there was no incentive for people to do so and, given the large number of observations, the influence of occasional repetition on our results would be negligible.
Another limitation of our study is that only age‐ and gender‐specific statistical life expectancy data are available in Hungary. Thus, we could not match the projections to statistical data adjusted to the socio‐economic status or unhealthy behaviours as well. Now, we observe that smokers in our sample overestimated their life expectancy less than non‐smokers (2.3 vs. 6.9 years; see Table 2), as compared to an objective life expectancy value that is not controlled for smoking status (only age and gender). If, however, in reality, the life expectancy of smokers is lower than that of non‐smokers and we would have such data to use for comparison, we could expect the overestimation to increase for smokers (as their actual life expectancy would be lower than the current comparator value) and to decrease for non‐smokers. Moreover, we used an adapted EQ‐5D instrument in obtaining expectations regarding future health, exactly like the one we used previously.3 It needs noting that the EQ‐5D was adjusted somewhat to obtain expectations regarding health states at older ages and not intended nor validated for obtaining expectations. The fact that the results of expected health at age 60 resembles actual quality of life at age 60 reasonably well may signal that people handle the questions posed as intended; this should be further investigated. Future research in these areas is encouraged, therefore.
Conclusions
To conclude, especially men appear to overestimate their life expectancy. Men and women expect a rapid deterioration of health‐related quality of life at the age of 70, strongly underestimating actual future health. Our findings confirm the previous results from the Netherlands. In addition, owing to the larger sample size, it refines those outcomes offering more detailed data for a broader age group. The striking similarities between the two studies from two distinct countries, which differ in terms of life expectancy and cultural aspects, suggest that the result patterns reported here may be relevant in more European countries. These findings may have important implications, for instance, for health policy and medical decision making.
Acknowledgements
No conflicts of interest have been declared. Authors are grateful to the web journal ‘Index’ for the opportunity and for their help in designing the electronic version of the questionnaire.
Questionnaire used in the surveya: expected health problems at ages 60, 70, 80 and 90 were asked applying the statements of the EQ‐5D
| I think at age 60 I will have…(Please mark your response) | ||||
| a. | No | Some | Major | Problems with walking about |
| b. | No | Some | Major | Problems with washing or dressing |
| c. | No | Some | Major | Problems with performing usual activities |
| d. | No | Some | Severe | Pain or discomfort |
| e. | No | Some | Severe | Anxiety or depression |
Ages 70, 80 and 90 were asked in a same construct.
References
- 1. Rabin R, de Charro F. EQ‐5D: a measure of health status from the EuroQol Group. Annals of medicine, 2001; 33: 337–343. [DOI] [PubMed] [Google Scholar]
- 2. Rothman ML, Beltran P, Cappelleri JC, Lipscomb J, Teschendorf B. Patient‐reported outcomes: conceptual issues. Value in Health, 2007; 10: S66–S75. [DOI] [PubMed] [Google Scholar]
- 3. Brouwer WB, van Exel NJ. Expectations regarding length and health related quality of life: some empirical findings. Social science & medicine, 2005; 61: 1083–1894. [DOI] [PubMed] [Google Scholar]
- 4. Szende A, Williams A. Measuring Self‐Reported Population Health: An International Perspective Based on EQ‐5D. Budapest: SpringMed Publishing Ltd, 2004. [Google Scholar]
- 5. Szende A, Nemeth R. [Health‐related quality of life of the Hungarian population]. Orvosi hetilap, 2003; 144: 1667–1674. [PubMed] [Google Scholar]
- 6. Brazier J, Akehurst R, Brennan A et al Should patients have a greater role in valuing health states?. Applied Health Economics and Health Policy, 2005; 4: 201–208. [DOI] [PubMed] [Google Scholar]
- 7. Mirowsky J. Subjective life expectancy in the US: correspondence to actuarial estimates by age, sex and race. Social science & medicine, 1999; 49: 967–979. [DOI] [PubMed] [Google Scholar]
- 8. Ross CE, Mirowsky J. Family relationships, social support and subjective life expectancy. Journal of health and social behavior, 2002; 43: 469–489. [PubMed] [Google Scholar]
- 9. Sarkisian CA, Hays RD, Mangione CM. Do older adults expect to age successfully? The association between expectations regarding aging and beliefs regarding healthcare seeking among older adults. Journal of the American Geriatrics Society, 2002; 50: 1837–1843. [DOI] [PubMed] [Google Scholar]
- 10. Perozek M. Using subjective expectations to forecast longevity: do survey respondents know something we don't know? Demography, 2008; 45: 95–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Smith VK, Taylor DH, Frank A. Longevity expectations and death: can people predict their own demise? American Economic Review, 2001; 91: 1126. [Google Scholar]
- 12. Smith VK. Risk perceptions, optimism, and natural hazards. Risk analysis, 2008; 28: 1763–1767. [DOI] [PubMed] [Google Scholar]
- 13. Lang FR, Baltes PB, Wagner GG. Desired lifetime and end‐of‐life desires across adulthood from 20 to 90: a dual‐source information model. The Journals of Gerontology, 2007; 62: P268–P276. [DOI] [PubMed] [Google Scholar]
- 14. Popham F, Mitchell R. Self‐rated life expectancy and lifetime socio‐economic position: cross‐sectional analysis of the British household panel survey. International journal of epidemiology, 2007; 36: 58–65. [DOI] [PubMed] [Google Scholar]
- 15. Kanis JA, McCloskey EV, Johansson H, Oden A, Strom O, Borgstrom F. Development and use of FRAX in osteoporosis. Osteoporosis International: A Journal Established as Result of Cooperation Between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, 2010; 21: S407–S413. [DOI] [PubMed] [Google Scholar]
- 16. van Nooten F, Brouwer W. The influence of subjective expectations about length and quality of life on time trade‐off answers. Health economics, 2004; 13: 819–823. [DOI] [PubMed] [Google Scholar]
- 17. van Nooten FE, Koolman X, Brouwer WB. The influence of subjective life expectancy on health state valuations using a 10 year TTO. Health economics, 2009; 18: 549–558. [DOI] [PubMed] [Google Scholar]