

Abstract
Background:
Whether the available Continuing Education (CE) programs meet pharmacists’ continuously increasing needs and preferences is open to question.
Objectives:
to investigate pharmacists’ perceptions and attitudes concerning available CE programs, evaluate the pharmacists’ choices with regard to selecting among different CE programs, and investigate the factors that are associated with preference to utilize online CE programs.
Method:
A 17-question survey was developed and mailed to a random sample of 600 Texan pharmacists. In addition to collecting basic demographic information, the survey investigated pharmacists’ choices with regard to delivery and content of CE programs, motivations to participation in CE programs, and pharmacists’ preferences for future CE programs.
Results:
A total of 161 pharmacists completed the survey and mailed back their responses. Excluding the 75 undeliverable surveys, the response rate was 31%. Approximately 83% of respondents found that currently available CE programs met their educational needs. The most important factors influencing pharmacists’ choices with regard to CE programs were the scope programs, the location where programs are held, and the cost associated with enrolling in such programs. Online CE was the most preferred mode of CE among participants. The factors that were associated with pharmacists’ preferences to complete 50% or more of required CE through online programs were previous use of online CE programs, preference to limit the duration of CE programs to 1 or 2 hour-long, and perceived ability to find adequate CE programs among currently available CE programs.
Conclusion:
The findings suggest modalities for CE programs providers on how to improve CE programs in the future in order to meet the preferences of local pharmacists.
Keywords: Education, Pharmacy, Continuing, Pharmacists, Attitude of Health Personnel, Surveys and Questionnaires, United States
INTRODUCTION
Pharmacists perceive continuing education (CE) programs as valuable and very effective in advancing their knowledge and educational needs.1 In addition to passing the course work and the practical training included in most pharmacy curricula in the United States (US), boards of pharmacy across the nation, including the Texas State Board of Pharmacy, require their licensed pharmacists to stay up-to-date regarding their practice-related knowledge. In Texas, this requirement is fulfilled by completing 30 hours of approved continuing education (CE) programs every reporting period consisting of 2 years.2 The Texas State Board of Pharmacy, however, does not mandate attending any live programs as part of the 30 contact hours needed for the biennial license renewal.3
From a professional point of view, pharmacists should be aware of any updates pertaining to the practice of pharmacy. The knowledge that students learn throughout college continuously changes. For example, new guidelines (e.g., screening for lung cancer)4 and treatment protocols (e.g., treatment of hypertension)5 were published over the past few years. This confirms the necessity of continuing education and learning among health care professionals in general, and among pharmacists in particular.6,7,8,9 Therefore, staying up-to-date with all matters that affect the practice of pharmacists is of paramount importance from professional and legal perspectives.
Emerging technologies and a worldwide shift from product-focus to patient-focus approaches, contributed to a significant change in the roles and responsibilities of pharmacists.6,10 Today, pharmacists have taken on roles far beyond that of traditional pill dispensing roles. Currently, the pharmacy field encompasses many disciplines and different new specialties including education, research, industry, informatics and many others.11 In order to meet these new challenges and arising responsibilities that have accompanied the evolution of the pharmacy profession, pharmacists need to stay competent throughout their career and make sure not only to maintain, but to always work on updating and improving their knowledge, skills and ability to assume job duties and variable responsibilities proficiently.12 This confirms the necessity of continuing education programs in supporting the role of pharmacists in different health care settings.8,9,10,13
As indicated by the Accreditation Council for Pharmacy Education (ACPE), pharmacy CE is a continuous process.14 ACPE regulations denote that continuing education should be maintained as long as pharmacists are licensed to practice. Currently there are more than 290,000 pharmacists in the US, with an expected 14% increase projected by 2020 according to the 2014 Occupational Employment and Wages Report issued by the US Bureau of Labor Statistics.15
Although CE programs are available nationwide, the demand for these programs is expected to grow over the next few years, reflected by increasing numbers of licensed pharmacists. Therefore, there is an increasing need for CE programs that meet rapidly changing practice of pharmacists. The potential role of academic institutions in providing CE programs was addressed in previous research in order to fill the gap between currently available CE programs and pharmacists’ professional needs.6
Considering the variability in educational needs and learning goals of pharmacists, it is essential for CE programs to evolve and refocus on meeting pharmacists’ new roles in different health care settings.6,7,16 The ACPE addressed Continuing Professional Development (CPD) in its strategic goals in order to improve the quality and outcomes of CE programs.17 As compared to CE, CPD is deemed a more interactive and tailored way of learning and training. The purpose of CPD is to provide education that is more relevant to individual pharmacists’ practice and profession.18
The literature is rich regarding the quantity and variety of different types of CE programs available for US pharmacists. Many studies have investigated the mode of CE programs delivery determining 1) how CE programs are implemented, and 2) the variety of subjects available in the literature.1,13,19,20,21,22,23,24,25,26,27 Furthermore, the ACPE mandates that providers of CE develop and conduct evaluations for the CE they provide.28 Such evaluations are to be completed by pharmacists based on their experience with each individual CE program. However, the literature is scant with regard to published evaluations of perceived adequacy of currently available CE programs.
Additionally, published research with regard to pharmacists’ preferences for online CE programs is lacking. To our knowledge, no prior studies have addressed pharmacists’ feedback on the adequacy of currently available CE programs. Additionally, no prior studies have investigated the factors that are associated with pharmacists’ preferences for online CE programs. Available research only investigated pharmacists’ perceptions of different modalities concerning live CE programs29, or needs and interest with respect to continuing education and certificate programs.30
Meeting pharmacists’ needs and matching their preferences is an important prerequisite for effective CE programs. Pharmacists are more likely to better grasp information when presented topics meet their preferences.6,8,16,19 On average, pharmacists are willing to pay out-of-pocket in order to complete CE programs that meet their preferences, especially with respect to certificate programs.30 Therefore, the need to explore pharmacists’ perceptions and attitudes and identifying their educational preferences is of great value.1,10 Additionally, with technology advancement, continuing education has become very accessible where someone can attend live lectures from their home, or even listen and watch from their phones. Such research can guide the development and implementations of future CE programs that more effectively support the educational requirements. The primary aims of this study are to: 1) to investigate pharmacists’ perceptions and attitudes concerning available CE programs, 2) evaluate the pharmacists’ choices with regard to selecting among different CE programs, and 3) investigate the factors that are associated with preference to utilize online CE programs.
Due to the growing role of internet and online CE in the pharmacy field, this study hypothesized that online mode of CE programs will be the most preferred mode among the participants. Additionally, as younger people are usually more inclined to using the internet and online programs as compared with older people, it was hypothesized that year of graduation will be associated with participants’ preference to using online CE programs; that is the more recent graduation year, the higher likelihood to prefer using online CE programs for completing the CE requirements. Further, it was hypothesized that previous use of online CE programs will be correlated with future preference of using online mode of CE programs. Therefore, it was expected that those who utilized online CE programs in their most recent reporting period will be more likely to prefer utilizing online CE programs again in the future.
METHODS
This research was based on a cross-sectional study that employed survey methodology to collect information from a sample of Texan pharmacists. A questionnaire was developed and mailed it to a random sample of pharmacists. The participants in this study were licensed pharmacists who resided in Southern Texas at the time of data collection. The completion of 30 contact hours of CE programs, which is a requirement for maintaining the license to practice pharmacy in Texas, was an inclusion criterion in this study.
Prior to conducting this study, Texas A&M University Institutional Review Board (IRB) approval was obtained. The group of pharmacists that were sampled was randomly selected from a database of licensed pharmacists maintained by Texas A&M Coastal Bend Health Education Center (CBHEC). The survey was mailed to the randomly selected pharmacists (n=600), along with a cover letter indicating that collecting the data was anonymous and that completing the survey was optional. For the purpose of maximizing the response rate, respondents’ names were entered into a drawing to win three USD50 gift certificates using a coded number system to maintain anonymity. All the collected data was self-reported. Data analyses were conducted using IBM Statistics Software (SPSS), version 22.
Some of the items in this study were adapted from two previous studies.13,31 The questionnaire consisted of three sections with a total of 17 items. All questions were closed-ended multiple choice questions. The first section investigated respondents’ demographic information. The second section investigated pharmacists’ perceptions on access to CE programs and frequency and characteristics of previous CE activities that pharmacists had completed. The third section examined pharmacists’ preferences regarding delivery mode and content of CE programs, motivations to completion of these CE programs, and plans for future CE activities. Further, the magnitude of interest in several subjects regarding CE programs was evaluated by using a 5-point Likert response format (No interest; Not very interested; Neutral; Some interest; Very interested).
A binary variable was created to measure participants’ preferences with regard to utilizing online CE programs for completion of most or all of their CE requirements. Values of this binary variable are 1) prefer to utilize online CE programs for 50% or more of required CE credit hours, or 2) prefer to utilize online CE programs for <50% of required CE credit hours. The 50% cut-off point was chosen in order to categorize participants into two groups based on whether they prefer to complete the majority of required CE through online mode. Then, bivariate analyses were conducted in order to investigate the association of this newly created variable with pharmacists’ year of graduation, primary practice setting, pharmacy degree, and other demographic and work-related factors. As all these variables are categorical, Pearson Chi-square analysis was utilized to check for association.
The factors that showed significance level of <0.1 in the bivariate analysis were entered into a binary logistic regression model in order to examine the predictors of participants’ preferences for online CE program. The reason for choosing a p-value of <0.1 was to include variables that are likely to show significance in the binary logistic regression model. The significance level for the binary logistic regression analysis was set to <0.05, and therefore, variables that showed significance association at a p-value of 0.05 or higher were dropped from the model.
RESULTS
The number of pharmacists who completed and mailed back the survey was 161. Seventy-five surveys came back as undeliverable. Therefore, the response rate was 31%. The sample’s demographic information and job characteristics are shown in Table 1. It was notable that the highest number of participants (44.7%) came from Corpus Christi, TX, which is an urban city located coastally in South Texas.
Table 1.
Participants Demographics
| Variable | Number (%) |
|---|---|
| Town | |
| Corpus Christi | 72 (44.7) |
| Elsewhere | 89 (55.3) |
| Primary Practicing Setting | |
| Community Independent | 40 (24.8) |
| Community Chain | 45 (28.0) |
| Hospital – Outpatient | 4 (2.5) |
| Hospital – Inpatient | 36 (22.4) |
| Long Term Care | 4 (2.5) |
| Pharmaceutical Industry | 1 (0.6) |
| College based | 3 (1.9) |
| Retired | 21 (13.0) |
| Other Settings (e.g., Administration) | 7 (4.3) |
| Number of years of practice | |
| 0-5 | 31 (19.3) |
| 10-Jun | 13 (8.1) |
| 20-Nov | 13 (8.1) |
| 21-30 | 28 (17.4) |
| 31-40 | 34 (21.1) |
| 41-50 | 21 (13.0) |
| Above 50 | 18 (11.2) |
| Missing Data | 3 (1.9) |
| Degree | |
| BSPharm | 106 (65.8) |
| PharmD | 55 (34.2) |
| College Graduated | |
| Texas A&M University | 13 (8.1) |
| Texas Tech University | 1 (0.6) |
| University of Texas at Austin | 71 (44.1) |
| Texas Southern University | 11 (6.8) |
| University of Houston | 32 (19.9) |
| Other Universities | 32 (19.9) |
| Missing Data | 1 (0.6) |
| Year Graduated from College | |
| Before 1970 | 30 (18.6) |
| 1970-1979 | 35 (21.7) |
| 1980-1989 | 30 (18.6) |
| 1990-1999 | 16 (9.9) |
| 2000-2009 | 27 (16.8) |
| 2010 or after | 22 (13.7) |
| Missing Data | 1 (0.6) |
When asked about the type of CE programs that the participants completed during their most recent CE reporting period, they indicated different modalities. At least 59.6% of the participants indicated that they did not complete CE hours through attending live programs at local, state, or national association meetings; attending employer sponsored presentations or industry sponsored meetings or dinners; reading written or correspondence programs; reading journals, listening to audio storage devices or watching videotapes, or through other non-listed modalities (Table 2). However, almost half of the participants (45.3%) indicated that they completed at least 50% of the required CE credit hours through online CE programs. As a result, Online CE Programs was the most commonly used type of CE programs among the sample for their most recent CE reporting period. The types of CE programs that were found to be most preferred to complete (for at least 50% of pharmacists’ required CE credit hours) are listed in ascending order is as follow: Tapes, other recording devices or Videotapes (none of the participants); employer sponsored presentations, industry-sponsored meetings or dinners, and journals-based CE programs (1.2% of the participants for each); written or correspondence CE programs (3.1% of the participants); live CE programs at local, State, or national association meetings (16.8% of the participants); and online CE programs (35.0% of the participants). In sum, online CE was the most preferred modality through which participants would like to complete the required CE credit hours. This corresponds to what was found regarding the most commonly used modality (Table 2) where 45.3% of the sample indicated that they had completed at least 50% of their CE hours in their most recent reporting period through online CE programs.
Table 2.
The percentage of the total CE credits were completed and preferred by the type of CE activity for participants
| Total CE hrs Completed | Total CE hrs Preferred | |||||
|---|---|---|---|---|---|---|
| Type of CE program participants had | 0 | 1-50% | 51-100% | 0 | 1-50% | 51-100% |
| Live Programs at Local/State/National Association Meetings | 96(59.60%) | 46(28.50%) | 19(11.80%) | 46(39.80%) | 70(43.40%) | 27(16.80%) |
| Employer Sponsored Speakers | 128(79.50%) | 31(19.30%) | 2(1.20%) | 100(62.10%) | 59(36.70%) | 2(1.20%) |
| Industry Sponsored Meetings/Dinners | 116(72.00%) | 43(26.70%) | 2(1.20%) | 83(51.6) | 76(47.20%) | 2(1.20%) |
| Written/Correspondence Programs | 116(72.00%) | 35(21.70%) | 10(6.20%) | 119(73.90%) | 37(23) | 5(3.10%) |
| Journals | 114(70.80%) | 37(23%) | 10(6.20%) | 113(70.20%) | 46(28.60%) | 2(1.20%) |
| Online Programs | 41(25.50%) | 47(29.10%) | 73(45.40%) | 39(24.20%) | 65(40.30%) | 56(34.80%) |
| Tapes, DVD’s or Videotapes | 152(94.40%) | 8(4.90%) | 1(0.60%) | 149(92.50%) | 12(7.40%) | 0(0.00% |
| Other | 154(95.70%) | 4(2.40%) | 3(1.80%) | 159(98.80%) | 1(0.60%) | 1(0.60%) |
The annual cost of earning the CE hours for participants was variable among the sample. Approximately 64.0% of the participants indicated that the CE programs were arranged by their employers (i.e., their out of pocket cost is zero) whereas other participants mentioned that it cost them more than USD600 a year. Further, 64.0% of the participants indicated that their employers did not reimburse them for any cost they incur for completing CE programs.
With regard to modalities through which pharmacists prefer to complete their CE programs, online CE was the most preferred modality (Table 3). Furthermore, most participants (82.6%) thought that currently available CE programs were adequate and that they met pharmacists’ practice needs (Table 3). Notably, when prompted about the most preferred duration of CE program, almost half of our sample (48.4%) chose between 1 and 2-hour long CE programs, which make this duration of CE programs the most preferred among the participants (Table 3). Finally, although 82.6% of the participants thought that currently available CE programs were adequate to meet their CE needs, 45% of the participants indicated that they were willing to subscribe to the Texas A&M CE service on an annual basis (Table 3). Only 11% were not willing to subscribe to this service.
Table 3.
Characteristics of Preferred CE Programs.
| Variable | Number (%) |
|---|---|
| Preferred length of CE | |
| 1 hour long | 32 (19.9%) |
| 1 to 2-hour long | 78 (48.4%) |
| Half a day (4-hour long) | 21 (13.0%) |
| All day (7 hours) | 14 (8.7%) |
| A weekend option (14 hours) | 12 (7.5%) |
| Missing Data | 4 (2.5%) |
| Finding adequate educational programming to meet your practice needs today | |
| Yes | 133 (82.6%) |
| No | 18 (11.2%) |
| Missing Data | 10 (6.2%) |
| Willingness to subscribe to the Texas A&M service on an annual basis | |
| Yes | 73 (45.3%) |
| No | 18 (11.2%) |
| Maybe | 66 (41%) |
| Missing Data | 4 (2.5%) |
Criteria for which the participants made their decisions with regard to selection of CE programs are shown in Table 4. Most participants indicated that scope of programs (area or practice) was the most important criterion when deciding on CE programs, followed by location of meetings and associated cost. Participants’ preferences with regard to the scope of CE programs are shown in Figure 1. All of the potential topics of CE were ranked according to participants’ preferences (i.e., Participants’ thoughts regarding subjects that are very interesting for CE programs). The top CE choice was “Best Practices in Medication Error Reduction” with 51.6% of the participant indicating that they are very interested in it. “Nuclear Pharmacy” was the topic that the participants were least interested in learning about (Figure 1). Only 5.6% indicated that they were very interested in completing CE programs in this topic.
Table 4.
Ranking of Importance.
| Factor | Unimportant | Of a little importance | Moderately importance | Important importance | Very importance | Missing importance |
|---|---|---|---|---|---|---|
| Cost of Programming | 18(11.20%) | 12(7.50%) | 26(16.10%) | 37(23.00%) | 62(38.50%) | 6(3.70%) |
| Scope of Programming (Area or Practice) | 14(8.70%) | 19(11.80%) | 29(18.00%) | 23(14.30%) | 70(43.50%) | 6(3.70%) |
| Location of Meetings | 15(9.30%) | 18(11.20%) | 17(10.60%) | 40(24.80%) | 65(40.40%) | 6(3.70%) |
| Type of Program Offerings (mode of delivery) | 8(5.00%) | 29(18.00%) | 29(18.00%) | 50(31.10%) | 40(24.80%) | 5(3.10%) |
| Social Interaction with Live Programming | 63(39.10%) | 23(14.30%) | 23(14.30%) | 24(14.90%) | 22(13.70%) | 6(3.70%) |
Figure 1.
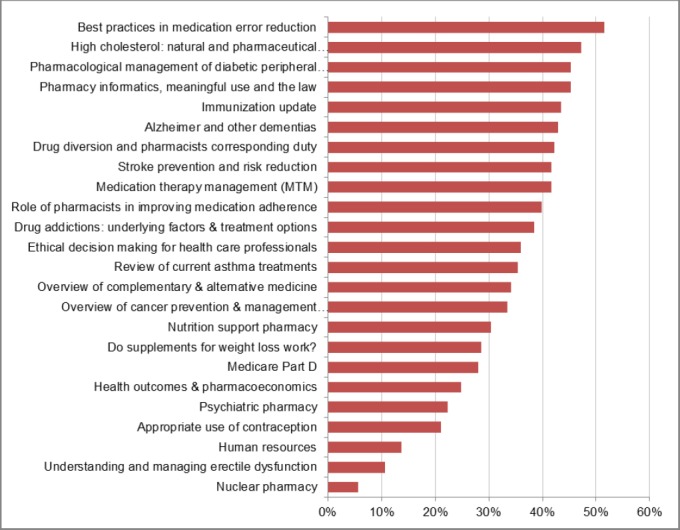
Pharmacists’ preferences regarding the CE programs. Percentage of pharmacists who were “very interested” in each of these surveyed topics.
Analyses indicated that 72 participants (45% of the sample) preferred to utilize online CE programs over other CE programs to complete at least 50% of the required CE credit hours, whereas 88 participants (55% of the sample) preferred to utilize online CE programs to complete less than 50% of the required CE credit hours. Bivariate analysis showed that several factors were associated with preference to complete 50% or higher of the required CE credit hours (Table 5). Factors that showed significance (Mode of most recent CE programs, perceived ability to find adequate CE programs, and preferred duration of CE programs) were entered in the binary logistic regression in order to measure the association of each of these factors with the preference for online CE program. The regression model (Table 5) demonstrated that three variables were significant predictors of preference to complete 50% or higher of the required CE through utilizing online mode. Pharmacists preferring online mode were more likely to have used online mode in the past and to think that available CE programs are adequate, but were less likely to prefer CE programs that are longer than two hours.
Table 5.
Categorical variables distribution and chi-square analysis with the dependent variable and significant variables in the final binary logistic regression equation model
| Variable | Prefer online CE for <50% of credit hours N (%) | Prefer online CE for 50% or more of credit hours N (%) | Test Statistics | OR (95%CI) |
|---|---|---|---|---|
| Most recent utilization of online CE programs | ||||
| > 49% of credit hours | 22 (25%) | 65 (75%) | N=160; p=0.000 chi-sq=68.02; df=1 | 28.089(10.2-77.6) |
| < 50% of credit hours | 66 (90%) | 7 (10%) | ||
| Perceived Ability to find adequate CE programs | ||||
| Yes | 65 (49%) | 67 (51%) | N=150; p=0.000 chi-sq=13.06; df=1 | 16.8(1.7-161.6) |
| No | 17 (94%) | 1 (6%) | ||
| Number of years in practice | ||||
| 0-5 | 18 (60%) | 12 (40%) | N=157 chi-sq=3.34; df=6 p=0.765 | |
| 10-Jun | 5 (38%) | 8 (62%) | ||
| 20-Nov | 7 (54%) | 6 (46%) | ||
| 21-30 | 14 (50%) | 14 (50%) | ||
| 31-40 | 17 (50%) | 17 (50%) | ||
| 41-50 | 12 (57%) | 9 (43%) | ||
| >50 | 12 (67%) | 6 (33%) | ||
| Year graduated | ||||
| Before 1970 | 20 (67%) | 10 (33%) | N=159; p=0.312 chi-sq=5.95; df=5 | |
| 1970-1979 | 21 (60%) | 14 (40%) | ||
| 1980-1989 | 13 (43%) | 17 (57%) | ||
| 1990-1999 | 7 (44%) | 9 (56%) | ||
| 2000-2009 | 12 (46%) | 14 (54%) | ||
| 2010 and after | 14 (64%) | 8 (36%) | ||
| Degree | ||||
| BS Pharm | 57 (54%) | 49 (46%) | N=160; p=0.662 chi-sq=0.19; df=1 | |
| PharmD | 31 (57%) | 23 (43%) | ||
| Practice Setting | ||||
| Community pharmacy (chain or independent | 43 (51%) | 41 (49%) | N=160; p=0.309 chi-sq=1.04; df=1 | |
| Other Practice Settings | 45 (59%) | 31 (41%) | ||
| Preferred duration of CE programs | ||||
| One or 2 hours | 49 (45%) | 61 (55%) | N=156; p=0.000 chi-sq=14.87; df=1 | |
| Longer than 2 hours | 36 (78%) | 10 (22%) | ||
OR, Odds Ratio (Exponential Coefficient); CI, Confidence Interval; chi-sq, chi quare; df, degrees of freedom
DISCUSSION
This study investigated pharmacists’ perceptions regarding their CE needs, as well as factors that impact their selections of CE programs. Additionally, the factors that were associated with preference to utilize online CE programs for 50% or more of the required CE credit hours were investigated. The sample included pharmacists who worked in different settings such as health care, academia, and industry. Further, the sample included participants who have had practiced pharmacy for as few as less than 5 years or as many as more than 50 years. Even though the participants were graduates of different universities inside and outside Texas, all of them were residents of Texas, and licensed to practice pharmacy in Texas.
Online CE mode was by far the most commonly used mode of CE among the participants in their most recent reporting period. This may be explained by the flexibility that is associated with completing online CE programs as compared with other modes of CE programs. With technology, online CE programs can be completed from any place, which means that they are not associated with travel requirements. Additionally, unless such online CE programs are live, they can be completed anytime, which adds a great flexibility and a convenience advantage as compared with other CE programs. These advantages help pharmacists avoid much of the time and location inconvenience that is associated with learning and education.32 It was notable that 13.7% of the participants reported that they paid more than USD400 annually in order to complete their CE requirements. Half of these pharmacists reported incurring more than USD600 a year. This might be especially important for 36% of the participants whose employers do not provide reimbursement for cost incurred by completing the CE requirements.
This barrier has been documented in the literature with regard to participation in learning among pharmacists.32 This finding corresponds with the findings presented in Table 4 as 61.5% of the participants indicated that cost of CE programs is an important or a very important criterion when making decisions regarding selection of CE programs.
Online CE programs were the most preferred modality for CE. Again, the convenience of this modality makes it associated with time and location constraints to a lesser extent. Additionally, the availability of many different online CE programs topics, which may be offered free of charge, gives pharmacists a high range of flexibility in selecting online CE programs. Further, as most online CE programs can be linked to the National Association of Boards of Pharmacy (NABP), pharmacists will not need to print out, mail, or request any certificates for completion of CE programs; reports are submitted electronically and certificates are automatically uploaded to pharmacists’ accounts at the NABP website upon the completion of the CE program. In sum, most online CE programs offer convenience that many other modalities do not provide.
Despite the time constraint associated with completing CE, which reported in previous research32, the length of CE programs that was most preferred among the participants was 1 to 2 hour-long (preferred by 48.4%), followed by only 1 hour long CE programs (preferred by 19.9%). This indicates that shorter duration CE programs are not necessarily associated with more convenience. In sum, CE programs that are not shorter than 1-hour and not longer than 2-hour are the most preferred among the sampled pharmacists.
As shown in Figure 1, 51.6% of the participants indicated that they were very interested in having CE programs in the field of “Best Practices in Medication Error Reduction”. Considering that this topic is not a license renewal requirement by Texas State Board of Pharmacy, having such a high percentage of pharmacists showing interest in this topic is worth more research in the future. There may be many explanations to why a high percentage of participants showed interest in this topic. A Concern among the participants with regard to potential errors in their practice might be one of these factors.
The topic that the sample was least interested in was “Nuclear Pharmacy”. This is understandable as only few numbers of pharmacists currently practice in this area of pharmacy. Contrary to our hypothesis, year of graduation was not significantly associated with preference to completing 50% or more of required CE credit hours through online CE programs. This may refute the common belief that younger pharmacists are more likely to prefer online CE programs. Additionally, this may provide another perspective as previous studies indicated the popularity of internet education among young learners.33 However, consistent with our hypothesis, past utilization of online CE programs was a predictor of participants’ preferences to complete 50% or more of required CE credit hours through online CE programs. Additionally, those who perceived that they were able to find adequate CE programs were more likely to prefer completing 50% or more of required CE credit hours through online CE programs. This demonstrates the association between thinking that available CE programs are adequate and preferring online CE programs. As this is a cross-sectional study, this relationship may be understood by the influence of the dependent variable on the independent variable. To clarify, those who utilize online CE programs may have found such mode highly satisfying with regard to the variety of programs and the multiple selection of topics that are covered with online CE programs, hence available CE programs are adequate. Future research may examine this relationship in more depth.
Finally, it was notable that those who preferred long CE programs (longer than 2 hours) were less likely to prefer completing 50% or more of required CE credit hours through online CE programs. This denotes the importance of having short CE programs for pharmacists preferring the online mode of CE programs. This finding may present a challenge for the uptake of certificate programs. Usually, certificate programs are longer than the average CE program as they provide intensive knowledge on specific areas.34 The association of preferred duration of CE programs and preference to online CE programs may warrant further exploration in future research.
This study included participants from Texas, mainly from the southern area. Results may not be generalizable to other pharmacists across the US, which may limit the external validity of this investigation. Additionally, some demographic information (e.g., race/ethnicity, income, and gender) was not collected. As the survey was self-administered, a relatively low response rate (31%) was observed. Therefore, results should be interpreted in light of potential nonresponse bias. In an attempt to reduce this bias, certain procedures were undertaken including personalized mail packets, providing financial incentives, inclusion of a stamped and self-addressed envelope in the survey packet for returning the completed survey, and mailing a second set of the survey packet to eligible participants who did not respond after mailing the first packet. In typical market research, the response rate achieved by this study would be considered rather low. In the pharmacy sector, however, such a response rate is generally considered acceptable. Previous research demonstrated that pharmacists tend not to respond to surveys due to being inundated with them and suffering from survey fatigue35, or simply due to not having time to do so.36
Nonresponse bias was assessed by a methodological procedure that was recommended by Oppenheim37 and Churchill38, which is based on the premise that late respondents are similar to non-respondents. Those who responded to the initial mailing and subsequent reminders were tracked. After analysis, there was no statistically significant difference between the percentages of those who had Pharm.D. degree in early versus late respondents. Therefore, it was concluded that non-respondents were not significantly different from respondents. It is anticipated that the results of this study provide useful insight into pharmacists’ attitudes, behaviors, and preferences related to continuing pharmacy education.
CONCLUSIONS
This paper presented an assessment of pharmacists’ attitudes, behaviors, and preferences related to pharmacy CE programs. Online CE was the most preferred mode of CE among the participants. It was associated with certain variables including pharmacists’ perceived ability to find adequate CE programs. These findings demonstrate the importance of online mode of CE as it is one of the most convenient modes of providing CE programs to pharmacists. The results of this study might be used to design more engaging programs and provide CE to pharmacists in way that is more convenient and interesting for them. Providers of CE programs may need to focus more on the prevalence and interest of utilizing online mode for providing CE programs for pharmacists. Future research may focus on the factors that predict participating in certain CE programs, or certain modalities through which CE programs are offered. Additionally, future research may investigate the association of demographic factors (race, gender, income) with pharmacists’ preferences with regard to completing CE programs in order to design CE programs that are more tailored to specific groups among pharmacists.
Footnotes
CONFLICT OF INTEREST
None declared.
Funding: This research was supported by Texas A&M Coastal Bend Health Education Center (CBHEC).
Contributor Information
Fadi M. Alkhateeb, Director of Assessment & Accreditation & Associate Professor of Pharmacy Administration, Department of Pharmacy Practice, Irma Lerma Rangel College of Pharmacy, Texas A&M Health Science Center. Kingsville, TX (United States). alkhateeb@pharmacy.tamhsc.edu
Omar F. Attarabeen, Assistant Professor of Pharmacy Practice. Marshall University College of Pharmacy. Huntington, WV (United States). attarabeen@marshall.edu
Sarah Alameddine, Assistant Professor of Pharmacy Practice. Nova Southeastern University. Fort Lauderdale, FL (United States). salameddine@nova.edu.
References
- 1.Maio V, Belazi D, Goldfarb NI, Phillips AL, Crawford AG. Use and effectiveness of pharmacy continuing-education materials. Am J Health Syst Pharm. 2003;60(16):1644–1649. doi: 10.1093/ajhp/60.16.1644. [DOI] [PubMed] [Google Scholar]
- 2.Texas State Board of Pharmacy. [accessed on July 4 2015];Continuing Education. https://www.pharmacy.texas.gov/infocist/continue.asp .
- 3.Texas Administrative Code. Examining Board. [accessed on October 28 2015];Texas State Board of Pharmacy. RULE §295 Continuing Education Requirements. at: http://texreg.sos.state.tx.us/public/readtac$ext.TacPage?sl=R&app=9&p_dir=&p_rloc=&p_tloc=&p_ploc=&pg=1&p_tac=&ti=22&pt=15&ch=295&rl=8 .
- 4.Lung Cancer Screening Summary of Recommendation and Evidence. United States Preventative Services Task Force. 2013 Dec; [Google Scholar]
- 5.James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O9, Smith SC, Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT, Jr, Narva AS, Ortiz E. 2014 evidence-based guideline for the management of high blood pressure in adults:report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311(5):507–520. doi: 10.1001/jama.2013.284427. doi:10.1001/jama.2013.284427. [DOI] [PubMed] [Google Scholar]
- 6.Schindel TJ, Kehrer JP, Yuksel N, Hughes CA. University-based continuing education for pharmacists. Am J Pharm Educ. 2012;76(2):769. doi: 10.5688/ajpe76220. doi:10.5688/ajp.e76220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Anderson S. The state of the world’s pharmacy:a portrait of the pharmacy profession. J Interprof Care. 2002;16(4):391–404. doi: 10.1080/1356182021000008337. [DOI] [PubMed] [Google Scholar]
- 8.Driesen A, Leemans L, Baert H, Laekeman G. Flemish community pharmacists’ motivation and views related to continuing education. Pharm World Sci. 2005;27(6):447–452. doi: 10.1007/s11096-005-0950-7. [DOI] [PubMed] [Google Scholar]
- 9.Tran D, Tofade T, Thakkar N, Rouse M. US and international health professions’ requirements for continuing professional development. Am J Pharm Educ. 2014;78(6):769. doi: 10.5688/ajpe786129. doi:10.5688/ajp.e7↤9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jorgenson D, Lamb D, MacKinnon NJ. Practice change challenges and priorities:A national survey of practising pharmacists. Can Pharm J. 2011;144(3):125–131. [Google Scholar]
- 11.LeClaire J Pharmacy Specialties. [accessed on September 28 2015];All Healthcare Making it in Medicine. at: http://allhealthcare.monster.com/training/articles/3803-pharmacy-specialties .
- 12.American College of Clinical Pharmacy. Burke JM, Miller WA, Spencer AP, Crank CW, Adkins L, Bertch KE, Ragucci DP, Smith WE, Valley AW. Clinical pharmacist competencies. Pharmacotherapy. 2008;28(6):806–815. doi: 10.1592/phco.28.6.806. doi:10.1592/phco.28.6.806. [DOI] [PubMed] [Google Scholar]
- 13.Hasan S. Continuing education needs assessment of pharmacists in the United Arab Emirates. Pharm World Sci. 2009;31(6):670–676. doi: 10.1007/s11096-009-9330-z. doi:10.1007/s11096-009-9330-z. [DOI] [PubMed] [Google Scholar]
- 14.Accreditation Council for Pharmacy Education. [accessed on June 24 2015];Definition of Continuing Education. at: http://www.acpe-accredit.org .
- 15.Occupational Employment Statistics. [accessed on June 24 2015];Bureau of Labor Statistics, U.S. Department of Labor. 2014 May; at: http://www.bls.gov/oes/current/oes291051.htm .
- 16.Mohamed Ibrahim OH. Assessment of Egyptian pharmacists’ attitude, behaviors, and preferences related to continuing education. Int J Clin Pharm. 2012;34(2):358–363. doi: 10.1007/s11096-012-9616-4. doi:10.1007/s11096-012-9616-4. [DOI] [PubMed] [Google Scholar]
- 17.Accreditation Council for Pharmacy Education. [accessed on October 28 2015];Strategic Goals. at: https://www.acpe-accredit.org/ceproviders/CPD.asp .
- 18.Strickland-Hodge B. Continuing professional development goes hand-in-hand with pharmacy practice. Pharmacy in Practice. 2008;18(5):173–177. [Google Scholar]
- 19.International Pharmaceutical Federation. Statement of professional standards on continuing professional development. The Hague: FIP; 2002. [accessed on June 24 2015]. at: www.fip.org/www/uploads/database_file.php?id=221&table_id= [Google Scholar]
- 20.Kuo GM, Lee KC, Ma JD. Implementation and outcomes of a live continuing education program on pharmacogenomics. Pharmacogenomics. 2013;14(8):885–895. doi: 10.2217/pgs.13.77. doi:10.2217/pgs.13.77. [DOI] [PubMed] [Google Scholar]
- 21.Rouse MJ. Pillars and foundations of quality for continuing education in pharmacy. Am J Pharm Educ. 2015;79(3):769. doi: 10.5688/ajpe79345. doi:10.5688/ajp.e79345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Nesterowicz K, Librowski T, Edelbring S. Validating e-learning in continuing pharmacy education:user acceptance and knowledge change. BMC Med Educ. 2014;14:769. doi: 10.1186/1472-6920-14-33. doi:10.1186/1472-6920-14-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wheeler A, Fowler J, Hattingh L. Using an intervention mapping framework to develop an online mental health continuing education program for pharmacy staff. J Contin Educ Health Prof. 2013;33(4):258–266. doi: 10.1002/chp.21198. doi:10.1002/chp.21198. [DOI] [PubMed] [Google Scholar]
- 24.Grzeskowiak LE, To J, Thomas AE, Phillips AJ. An innovative approach to enhancing continuing education activities for practising pharmacists using clicker technology. Int J Pharm Pract. 2014;22(6):437–439. doi: 10.1111/ijpp.12092. [DOI] [PubMed] [Google Scholar]
- 25.Namara KP, Duncan GJ, McDowell J, Marriott JL. Community pharmacists’ preferences for continuing education delivery in Australia. J Contin Educ Health Prof. 2009;29(1):52–57. doi: 10.1002/chp.20006. doi:10.1002/chp.20006. [DOI] [PubMed] [Google Scholar]
- 26.Walters C, Raymont A, Galea S, Wheeler A. Evaluation of online training for the provision of opioid substitution treatment by community pharmacists in New Zealand. Drug Alcohol Rev. 2012;31(7):903–910. doi: 10.1111/j.1465-3362.2012.00459.x. doi:10.1111/j.1465-3362.2012.00459.x. [DOI] [PubMed] [Google Scholar]
- 27.Sweileh WM, Al-Jabi SW, Sawalha AF, Zyoud SH. Pharmacy education and practice in West Bank, Palestine. Am J Pharm Educ. 2009;73(2):769. [PMC free article] [PubMed] [Google Scholar]
- 28.Accreditation Council for Pharmacy Education. [accessed on October 28 2015];Accreditation Standards for Continuing Pharmacy Education Version 2. 2014 at: https://www.acpe-accredit.org/pdf/CPE_Standards_Final.pdf .
- 29.Buxton EC, De Muth JE. Pharmacists’ perceptions of a live continuing education program comparing distance learning versus local learning. Res Social Adm Pharm. 2013;9(2):230–235. doi: 10.1016/j.sapharm.2012.05.003. doi:10.1016/j.sapharm.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 30.Scott VG, Amonkar MM, Madhavan SS. Pharmacists’ preferences for continuing education and certificate programs. Ann Pharmacother. 2001;35(3):289–299. doi: 10.1345/aph.10191. [DOI] [PubMed] [Google Scholar]
- 31.Pharmacist Continuing Education Needs Survey. [accessed on September 27 2015];The James L Winkle College of Pharmacy Board of Advisors (Mike Puccini et al.) at: https://www.surveymonkey.com/r/?sm=QX2MwSmfnbho3TgwGJ7hhc3sZdTjFJ3DuDzaXk7LXbk%3d .
- 32.Hanson AL, Bruskiewitz RH, DeMuth JE. Pharmacists’ perceptions of facilitators and barriers to lifelong learning. Am J Pharm Educ. 2007;71(4):769. doi: 10.5688/aj710467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cain J, Fox BI. Web 2.0 and pharmacy education. Am J Pharm Educ. 2009;73(7):769. doi: 10.5688/aj7307120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Rouse MJ. Continuing professional development in pharmacy. J Pharm Technol. 2004;20(5):303–306. doi: 10.1331/1544345041475634. [DOI] [PubMed] [Google Scholar]
- 35.Jesson J. Cross-sectional studies in prescribing research. J Clin Pharm Ther. 2001;26(6):397–403. doi: 10.1046/j.1365-2710.2001.00373.x. [DOI] [PubMed] [Google Scholar]
- 36.Mott DA, Pederson CA, Doucette WR, Gaither CA, Schommer JC. A national survey of US pharmacists in 2000:assessing nonresponse bias of a survey methodology. AAPS PharmSci. 2001;3(4):769. doi: 10.1208/ps030433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Oppenheim AN. Questionnaire design, interviewing and attitude measurement. Bloomsbury Publishing. 2000 [Google Scholar]
- 38.Churchhill GA. Marketing research:methodological foundations. New York NY: Rinehart and Winston; 1987. [Google Scholar]