

Case Report
An 86-year-old man with atrial fibrillation on anticoagulation was admitted to another hospital for an upper gastrointestinal bleed after accidental ingestion of a plastic bread clip. He required 11 units of packed red blood cells for resuscitation. Esophagogastroduodenoscopy demonstrated the clip firmly wedged onto a duodenal fold (Figure 1) with bleeding from adjacent mucosa. Attempts to remove the clip with standard technique using alligator forceps were unsuccessful due to large size of the clip and inadequate grip on a smooth surface. The patient was transferred to our institution for surgical management or repeat attempt at endoscopic management. We decided to attempt breaking the plastic clip with a mechanical lithotripter (LithoCrushV, Olympus America, Center Valley, Pennsylvania), typically used for lithotripsy of bile duct stones. This appeared successful when performed ex vivo on a similar plastic clip (Figure 2). The lithotripsy basket was introduced through a therapeutic upper endoscope (GIF-1TQ160, Center Valley, Pennsylvania), and the wires were manipulated around the clip. The wires were tightened until the clip was successfully broken into 2 fragments (Figure 3). The fragments were then easily manipulated off the duodenal fold. The endoscope was withdrawn then reintroduced through an overtube. Final retrieval of the clip fragments was accomplished using a Roth net (Figure 4).
Figure 1.
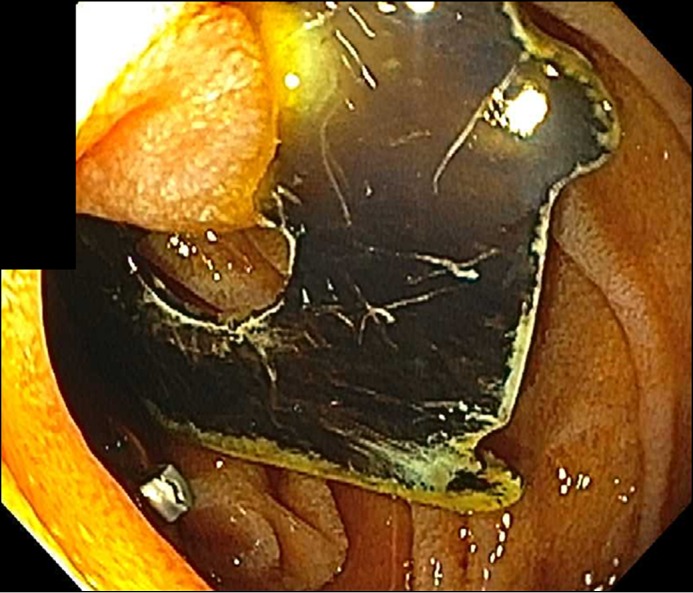
Plastic bread clip wedged onto duodenal fold.
Figure 2.

Ex vivo fragmentation of plastic clip using lithotripsy basket. Metal wires are secured around an object and tightened until the object is fragmented.
Figure 3.

LithoCrushV wires around the plastic clip.
Figure 4.

Final fragments of plastic clip, ex vivo.
Foreign body ingestion is common in both the pediatric and adult population. Early studies suggest that 80% or more of foreign objects pass without a need for endoscopic intervention.1 Even the majority of sharp-pointed objects in the stomach will pass without incident, but the risk of a complication is as high as 35%.1 Therefore, The American Society for Gastrointestinal Endoscopy guidelines recommend that sharp-pointed objects that have passed into the stomach or proximal duodenum should be retrieved endoscopically.2 Use of various retrieval devices have been described, most commonly rat-tooth and alligator forceps, polypectomy snares, polyp graspers, baskets, and retrieval nets.2 Biliary lithotripsy baskets are highly effective at fragmenting common bile duct stones. There have been a few case reports of lithotripsy utilization for the removal of oddly shaped and sharp objects.3,4 We describe the successful, off label use of a biliary lithotripsy basket to enable fragmentation and retrieval of a foreign body.
Disclosures
Author contributions: I. Lee wrote the manuscript. P. Darwin reviewed the final manuscript and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.
References
- 1.Carp L. Foreign bodies in the intestine. Ann Surg. 1927; 85:575–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.ASGE Standards of Practice Committee, Ikenberry SO, Jue TL, Anderson MA, et al . Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011; 73(6):1085–91. [DOI] [PubMed] [Google Scholar]
- 3.Kedia P, Jacob B, DiMaio CJ. Mechanical lithotriptor-assisted endoscopic removal of an eroded gastric lap band. Gastrointest Endosc. 2015; 81(5):1256–7. [DOI] [PubMed] [Google Scholar]
- 4.Ma S, Gao F, Zhang N, Zhao Z, Yang Z. Use of a mechanical lithotripter to aid in the removal of an impacted razor blade in the esophagus. Gastrointest Endosc. 2012; 76(1):217–9. [DOI] [PubMed] [Google Scholar]