

ABSTRACT
Mixed chimerism discovered in Freemartin cattle by Ray Owen 70 years ago paved the way for research on immune tolerance. Since his discovery, significant progress has been made in the effort to induce allograft tolerance via mixed chimerism in various murine models. However, induction of persistent mixed chimerism has proved to be extremely difficult in major histocompatibility complex mismatched humans. Chimerism induced in humans tends to either disappear or convert to full donor chimerism, depending on the intensity of the conditioning regimen. Nevertheless, our studies in both NHPs and humans have clearly demonstrated that renal allograft tolerance can be induced by transient mixed chimerism. Our studies have shown that solid organ allograft tolerance via transient mixed chimerism 1) requires induction of multilineage hematologic chimerism, 2) depends on peripheral regulatory mechanisms, rather than thymic deletion, for long-term maintenance, 3) is organ specific (kidney and lung but not heart allograft tolerance are feasible). A major advantage of tolerance induction via transient mixed chimerism is exclusion of the risk of graft-versus-host disease. Our ongoing studies are directed toward improving the consistency of tolerance induction, reducing the morbidity of the conditioning regimen, substituting clinically available agents, such as Belatacept for the now unavailable anti-CD2 monoclonal antibody, and extending the protocol to recipients of deceased donor allografts.
Keywords: ATG, combined Kidney/BMT, Donor BMT; Freemartin cattle; full chimerism, GVHD, HLA-match, HLA-mismatch, mixed chimerism, multilineage chimerism, neonatal tolerance, NHP, nonmyeloablative, operational tolerance, persistent (durable) mixed chimerism, TBI, TI, TLI, transient mixed chimerism, TMEM
Discovery of chimerism in freemartin cattle
The Chimera of Greek mythology is described as possessing the head of a lion, the body of a goat and the hindquarters of a dragon. As an immunological term, a chimera can be defined as an individual in whom genetically different tissues or cells co-exist without causing detrimental immunological responses. No one believed that a “Chimera” could naturally exist until Ray Owen at University of Wisconsin discovered red cell chimerism in Freemartin cattle in 1945 (Fig. 1).1 About 40 years earlier, Frank Lillie had reported that placental fusion of twin bovine embryos united the 2 circulatory systems and affected development of the reproductive system of the opposite sibling, if the twin's gender was not identical.2 Owen speculated that cross-circulation between such twins through placental fusion resulted in bidirectional, acquired immunologic tolerance that allowed for postnatal survival of allogeneic red blood cells in both twins. This chimerism turned out to exist not only in red blood cells but also in the entire haematopoietic cell population. Around the same time, Peter Medawar, then at University College London, independently reported that dizygotic cattle twins can accept skin grafts from each other.3 When Medawar subsequently reviewed the Owen's finding, he hypothesized that “mammals and birds never develop the power to react immunologically against foreign homologous tissue or cells to which they have been exposed sufficiently early in fetal life.” To prove this hypothesis, he executed seminal studies on neonatal tolerance which demonstrated that skin allograft tolerance can be induced during the early postnatal period by intravenous injection of donor cells into the eventual graft recipient.4 Since Medawar's hypothesis of neonatal tolerance had been based upon the Owen's previous findings in Freemartin cattle, where chimerism and tolerance were long lasting, subsequent investigators attempted to exploit the possibility of tolerance induction via haematopoietic chimerism established initially in the postnatal period. Unfortunately, most studies determined that chimerism induced in neonates was not stable and donor haematopoietic cells eventually became undetectable.5,6
Figure 1.
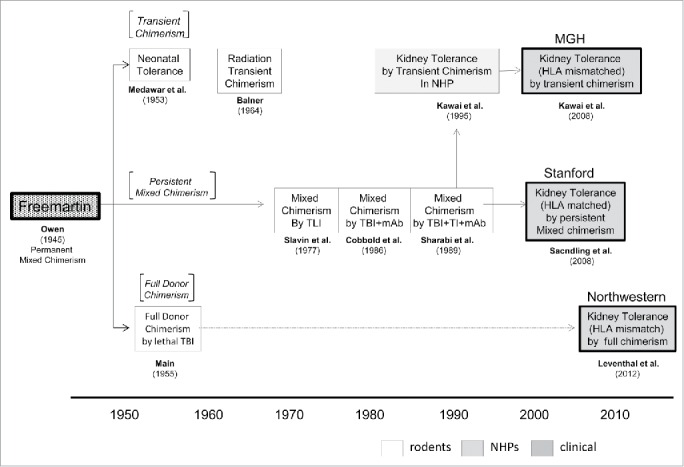
An historical scheme of chimerism. Since Owen discovered persistent mixed chimerism in Freemartin cattle, 3 strategies have been pursued in the attempt to induce allograft tolerance. These include 1) persistent mixed chimerism, 2) transient mixed chimerism and 3) full donor chimerism. Allograft tolerance via mixed chimerism has been achieved in various murine models (Slavin et al.9 in 1977 and Sharabi et al.13 in 1989). However, persistent mixed chimerism has been extremely difficult to achieve in primates and has only been achieved in HLA-matched transplant recipients by the Stanford group. of note, the neonatal tolerance achieved by Medawar in 1953 was not a complete reproduction of the Freemartin cattle observation. The chimerism achieved in neonatal tolerance was transient and the mechanism of tolerance may be different from that in Freemartin cattle. In 1964, Balner reported the possibility of inducing allograft tolerance via transient chimerism. However, his finding remained unheeded until we (MGH) found that transient mixed chimerism is sufficient to induce renal allograft tolerance in nonhuman primates. Our strategy with transient mixed chimerism has been successfully translated to both HLA-matched and HLA-mismatched human kidney transplantation. Full donor chimerism was until recently considered too risky to apply clinically for tolerance induction of transplanted organs. However, full donor chimerism and renal allograft tolerance have been achieved by the Northwestern group in HLA-mismatched kidney transplant recipients without an unacceptable incidence of GVHD.
Initial observations from studies attempting to extend the applicability of tolerance induced by mixed chimerism
Soon after Medawar's report on neonatal tolerance, successful induction of skin allograft tolerance by induction of full donor chimerism was reported.7 In this study, skin allograft tolerance was achieved in animals that received donor bone marrow transplantation (BMT) only after myeloablative total body irradiation (TBI). However, different from the Freemartin cattle, chimerism induced in these radiation chimeras was full, with recipient haematopoietic cells being completely replaced with donor haematopoietic cells. Not surprisingly, a significant number of these animals developed graft-versus-host disease (GVHD). In 1964, Balner reported a series of studies in adult rat radiation chimeras prepared by high dose TBI and donor BMT. Interestingly, he found that some animals, that developed only transient chimerism, nevertheless permanently accepted the skin allograft.8 Balner emphasized in his report that the avoidance of durable chimerism would be advantageous because the risk of GVHD should be minimal. His observations clearly showed the possibility of specific tolerance being induced independent of a permanent chimeric state. Nevertheless, tolerance induced by transient chimerism was not extensively pursued with most efforts being directed toward establishing durable mixed chimeras in adult animals (Fig. 1), the state Owen had discovered in the Freemartin cattle. More recently, some progress has been made in the induction of allograft tolerance through durable mixed chimerism. In 1977, Slavin et al. first reported successful induction of persistent mixed chimerism which led to skin or heart allograft tolerance in mice after conditioning with a potentially clinically applicable regimen that included total lymphoid irradiation.9 However, when this conditioning regimen with TLI was subsequently tested in dogs and baboons, successful induction of persistent chimerism could not be demonstrated in large animal models.10,11
In 1986, Cobbold et al. reported successful induction of mixed chimerism and donor-specific skin allograft tolerance again in a murine model, using a conditioning regimen that included sublethal TBI (6 Gy) and T-cell depleting monoclonal antibody (mAb).12 Sharabi et al. subsequently reported successful induction of stable mixed chimerism and skin allograft acceptance in mice treated with 3 Gy of TBI and addition thymic irradiation (TI; 7 Gy) plus T cell depleting mAbs.13
Allograft tolerance induced by only transient mixed chimerism in NHP
Based on the rodent studies reported by Sharabi et al., we developed a nonmyeloablative regimen that induces mixed chimerism and renal allograft tolerance in major histocompatibility complex (MHC)-mismatched cynomolgus monkeys (Fig. 1).14-16 Components of the initial preparative regimen for nonhuman primates (NHPs) were similar to those that had been developed in mice, which included TBI (1.5 Gy × 2), TI (7 Gy), and anti-T cell antibody [horse anti-thymocyte globulin (hATG)]. However, this initial regimen that was effective in mice, failed to induce even transient mixed chimerism in NHPs because significant residual T cells survived in lymph nodes and spleen after the conditioning. Therefore, splenectomy and a one-month course of cyclosporine (CyA) were added in subsequent studies. With this modification, 11 of 13 recipients of combined kidney and bone marrow transplantation (combined Kidney/BMT) developed multilineage chimerisms and 9 survived long-term with normal renal function.16 Of note, different from mice, mixed chimerism induced in these NHPs was only transient, typically becoming undetectable within months after donor BMT.14-16 Continued survival of the kidney allograft despite the loss of chimerism suggested that peripheral mechanisms were primarily involved. To improve the consistency of chimerism induction and renal allograft tolerance, we subsequently further modified the protocol by replacing splenectomy with a short course of anti-CD40L (CD154) mAb. With this modification, most recipients developed significantly improved, but still transient, mixed chimerism and approximately 60% of them achieved long-term renal allograft survival without ongoing immunosuppression.17
The mechanisms underlying the induction of renal allograft tolerance by transient chimerism have not been fully clarified. Thymic deletion has been demonstrated to be a major pathway to tolerance induced by the persistent mixed chimerism that is achieved in murine models.18,19 However, as suggested above, peripheral regulatory mechanisms seem to be critical for renal allograft tolerance after transient mixed chimerism. This hypothesis is supported by our recent study which demonstrated that renal allograft tolerance can be abrogated even years later by IL-2 infusion. Although high-dose (0.6-3.0 × 106 IU/m2/day) IL-2 administration20-22 for more than one week is necessary to break previously established tolerance, this finding indicates that donor reactive T cells were not completely deleted by the original conditioning regimen.23
We also found that tolerance induction via transient mixed chimerism in NHPs is organ specific. In contrast to the observations with renal allografts, the same conditioning regimen failed to induce heart allograft tolerance despite the development of transient mixed chimerism.24 On the other hand, we recently observed that lung allograft tolerance is inducible even with transient mixed chimerism.25 Therefore, we speculate that some intrinsic factors that exist in the kidney and lung, but not in the heart play an additional role in induction of allograft tolerance via this approach.
Extension of the mixed chimerism approach to deceased donor transplantation
A limitation of our initial approach to tolerance induction includes its inapplicability to deceased donor transplantation, as the conditioning was initiated one week before the planned combined Kidney/BMT. To extend our approach to deceased donor kidney transplantation, we developed the “Delayed Tolerance” approach, in which kidney transplant recipients are initially maintained on conventional immunosuppression, and then undergo conditioning and donor BMT several months later.26,27 With this approach, renal allograft tolerance could potentially be induced in any stable recipient of either living donor or deceased donor kidney transplantation, if donor bone marrow cells are available.
Our initial observations indicated that faster homeostatic recovery of CD8+ memory T cells (TMEM) prevented induction of chimerism in the delayed tolerance approach, therefore, we added anti-CD8 mAb to the conditioning regimen.26 This modified regimen significantly delayed homeostatic recovery of CD8+ TMEM and most recipients (11/13) successfully developed transient mixed chimerism. Approximately 70% of the NHP recipients survived long-term following withdrawal of all immunosuppression.26 Another important observation involved the timing of the donor BMT relative to the kidney transplantation. When delayed conditioning and donor BMT were performed at 1 month after Kidney transplantation, all recipients failed to develop renal allograft tolerance despite successful induction of chimerism.27 When compared to observations in the recipients treated at 4 months, significantly higher inflammatory cytokines were detected in the peripheral blood of the recipients conditioned at 1 month, which may contribute to failure of tolerance induction.27 These studies indicate that deletion of CD8+ TMEM and the timing of donor BMT are critical for successful delayed induction of tolerance.26,27
Defining a clinically applicable conditioning regimen
Although our NHP studies have established that CD40-CD40L blockade reliably induces mixed chimerism and renal allograft tolerance, anti-CD40L mAb is not clinically available due to its thrombogenic side effects.28 Therefore, we have recently evaluated a clinically-available, costimulatory-blockade agent, CTLA4-Ig (Belatacept), as a replacement for anti-CD40L mAb in our conditioning regimen.29 Four out of 5 recipients treated with the Belatacept regimen developed even higher levels of chimerism than those observed in recipients treated with the anti-CD40L mAb regimen and 3 of them achieved long-term renal allograft survival without maintenance immunosuppression. These NHP results suggest that CD28/B7 blockade with Belatacept can provide a clinically applicable alternative to anti-CD40L mAb for promoting chimerism and renal allograft tolerance. In NHP studies for the “Delayed Tolerance” approach, addition of anti-CD8 mAb was necessary since hATG cross-reacts poorly with NHPs. However, we anticipate that sufficient CD8+ TMEM deletion will be achievable in humans treated with either hATG or rabbit ATG (Thymoglobulin) without the need for anti-CD8 mAb.
Clinical studies
Our approach to tolerance induction via transient mixed chimerism has been successfully translated to human leukocyte antigen (HLA)-mismatched recipients of living donor kidney transplants.30-32 As in our previous studies of HLA-matched combined Kidney/BMT in patients with end-stage renal disease due to refractory myeloma,33 the initial conditioning regimen for HLA-mismatched combined Kidney/BMT was modified from that used in NHP study to include cyclophosphamide (Cytoxan, CTX ) and anti-CD2 mAb in place of TBI and hATG, respectively. TI was included but post-transplant calcineurin inhibitor (CNI) administration was tapered more slowly (over 9-14 months in humans vs. one month in NHP). Because humoral rejection was observed in 2 of the first 3 subjects, all subsequent patients were treated with a regimen that added rituximab and early post-transplant prednisone (Modified NKD03 and ITN036). A total of 10 subjects were enrolled in these initial studies. All recipients developed transient mixed chimerism for up to 3 weeks. By 14 months post combined Kidney/BMT 7 of them had successfully discontinued all maintenance immunosuppression ongoing good renal allograft function for 5-13 years. Four of these recipients remain immunosuppression-free for 5−13 years post-transplant. However, 3 resumed immunosuppression at 5, 7, and 8 years after kidney transplantation as a result of chronic rejection or recurrence of the original disease.32 A major adverse event observed in these clinical trials was acute kidney injury (AKI), which was observed in most recipients.34 This event was observed after day 10 and was associated with loss of chimerism and recipient haematopoietic cell recovery. Since AKI was not observed in the NHP studies that utilized TBI rather than CTX, we recently tested a revised regimen in which CTX was replaced with low dose TBI. Two patients who received this revised regimen have done well, without AKI, and their immunosuppression is currently being tapered (manuscript in preparation). Further clinical trials are planned using a new regimen with Belatacept which, as detailed above, has been developed in the NHP studies.29
Summary
We have shown that renal allograft tolerance can be induced by establishment of only transient mixed chimerism in both preclinical and clinical studies. The advantage of tolerance by transient mixed chimerism has been elimination of the risk of GVHD. Continuing efforts to improve the consistency of tolerance induction with less morbidity is necessary for wider clinical application. Clarification of the mechanisms underlying induction of tolerance by transient chimerism as well as extension of this approach to deceased donor renal and non-renal organ transplantation is current important objectives.
Abbreviations
- AKI
acute kidney injury
- ATG
antithymocyte globulin
- BMT
bone marrow transplantation
- CNI
calcineurin inhibitor
- GVHD
graft-vs.-host disease
- HLA
human leukocyte antigen
- mAb
monoclonal antibody
- MGH
Massachusetts General Hospital
- MHC
major histocompatibility complex
- NHP
nonhuman primate
- TBI
total body irradiation
- TI
thymic irradiation
- TLI
total lymphoid irradiation
- TMEM
memory T cell
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Funding
The present work was supported by grants from the Immune Tolerance Network (NIH/NIAID NO1 AI1541), NIH 5U01DK080653-04, and the National Institute of Diabetes and Digestive and Kidney Disease (NIDDK) 1U19DK080652-01.
References
- [1].Owen RD. Immunogenetic consequences of vascular anastomoses between bovine twins. Science 1945; 102:400-1; PMID:17755278; http://dx.doi.org/ 10.1126/science.102.2651.400 [DOI] [PubMed] [Google Scholar]
- [2].Lillie FR. The theory of the free-martin. Science 1916; 43:611-13; PMID:17756274; http://dx.doi.org/ 10.1126/science.43.1113.611 [DOI] [PubMed] [Google Scholar]
- [3].Anderson D, Billingham RE, Lampkin GH, Medawar PB.. The use of skin grafting to distinguish between monozygotic and dizygotic twins in cattle. Heredity 1951; 5:379-97; http://dx.doi.org/ 10.1038/hdy.1951.38 [DOI] [Google Scholar]
- [4].Billingham RE, Brent L, Medawar PB.. Actively acquired tolerance of foreign cells. Nature 1953; 172:603-6; PMID:13099277; http://dx.doi.org/ 10.1038/172603a0 [DOI] [PubMed] [Google Scholar]
- [5].Doria G. Identification of the immune system responsible for the specificity of actively acquired tolerance in mice. Proc Natl Acad Sci U S A 1963; 49:281-6; PMID:16591052; http://dx.doi.org/ 10.1073/pnas.49.3.281 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Michie D, Woodruff MF, Zeiss IM.. An investigation of immunological tolerance based on chimaera analysis. Immunology 1961; 4:413-24; PMID:14473459. [PMC free article] [PubMed] [Google Scholar]
- [7].Main JM, Prehn RT.. Successful skin homografts after the administration of high dosage x radiation and homologous bone marrow. J Natl Cancer Inst 1955; 15:1023-9; PMID:13233946. [PubMed] [Google Scholar]
- [8].Balner H. Persistence of tolerance towards donor-type antigens after temporary chimerism in rats. Transplantation 1964; 2:464-74; PMID:14181030; http://dx.doi.org/ 10.1097/00007890-196407000-00003 [DOI] [PubMed] [Google Scholar]
- [9].Slavin S, Strober S, Fuks Z, Kaplan HS.. Induction of specific tissue transplantation tolerance using fractionated total lymphoid irradiation in adult mice: Long-term survival of allogeneic bone marrow and skin grafts. J Exp Med 1977; 146:34-48; PMID:17647; http://dx.doi.org/ 10.1084/jem.146.1.34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Strober S, Modry DL, Hoppe RT, Pennock JL, Bieber CP, Holm BI, Jamieson SW, Stinson EB, Schroder J, Suomalainen H, et al.. Induction of specific unresponsiveness to heart allografts in mongrel dogs treated with total lymphoid irradiation and antithymocyte globulin. J Immunol 1984; 132:1013-8; PMID:6361129. [PubMed] [Google Scholar]
- [11].Smit JA, Hill RR, Myburgh JA, Browde S.. Transplantation tolerance in primates after total lymphoid irradiation and allogeneic bone marrow injection. Iii. Lymphocyte responsiveness and suppressor cell activity. Transplantation 1980; 30:107-10; PMID:6451965; http://dx.doi.org/ 10.1097/00007890-198008000-00005 [DOI] [PubMed] [Google Scholar]
- [12].Cobbold SP, Martin G, Qin S, Waldmann H.. Monoclonal antibodies to promote marrow engraftment and tissue graft tolerance. Nature 1986; 323:164-6; PMID:3528866; http://dx.doi.org/ 10.1038/323164a0 [DOI] [PubMed] [Google Scholar]
- [13].Sharabi Y, Sachs DH.. Mixed chimerism and permanent specific transplantation tolerance induced by a nonlethal preparative regimen. J Exp Med 1989; 169:493-502; PMID:2562984; http://dx.doi.org/ 10.1084/jem.169.2.493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Kawai T, Cosimi AB, Colvin RB, Powelson J, Eason J, Kozlowski T, Sykes M, Monroy R, Tanaka M, Sachs DH.. Mixed allogeneic chimerism and renal allograft tolerance in cynomolgus monkeys. Transplantation 1995; 59:256-62; PMID:7839449; http://dx.doi.org/ 10.1097/00007890-199501000-00018 [DOI] [PubMed] [Google Scholar]
- [15].Kimikawa M, Sachs DH, Colvin RB, Bartholomew A, Kawai T, Cosimi AB.. Modifications of the conditioning regimen for achieving mixed chimerism and donor-specific tolerance in cynomolgus monkeys. Transplantation 1997; 64:709-16; PMID:9311707; http://dx.doi.org/ 10.1097/00007890-199709150-00008 [DOI] [PubMed] [Google Scholar]
- [16].Kawai T, Poncelet A, Sachs DH, Mauiyyedi S, Boskovic S, Wee SL, Ko DS, Bartholomew A, Kimikawa M, Hong HZ, et al.. Long-term outcome and alloantibody production in a non-myeloablative regimen for induction of renal allograft tolerance. Transplantation 1999; 68:1767-75; PMID:10609955; http://dx.doi.org/ 10.1097/00007890-199912150-00022 [DOI] [PubMed] [Google Scholar]
- [17].Kawai T, Sogawa H, Boskovic S, Abrahamian G, Smith RN, Wee SL, Andrews D, Nadazdin O, Koyama I, Sykes M, et al.. Cd154 blockade for induction of mixed chimerism and prolonged renal allograft survival in nonhuman primates. Am J Transplant 2004; 4:1391-8; PMID:15307826; http://dx.doi.org/ 10.1111/j.1600-6143.2004.00523.x [DOI] [PubMed] [Google Scholar]
- [18].Sykes M. Chimerism and central tolerance. Curr Opin Immunol 1996; 8:694-703; PMID:8902396; http://dx.doi.org/ 10.1016/S0952-7915(96)80088-4 [DOI] [PubMed] [Google Scholar]
- [19].Wekerle T, Sayegh MH, Hill J, Zhao Y, Chandraker A, Swenson KG, Zhao G, Sykes M.. Extrathymic t cell deletion and allogeneic stem cell engraftment induced with costimulatory blockade is followed by central t cell tolerance. J Exp Med 1998; 187:2037-44; PMID:9625763; http://dx.doi.org/ 10.1084/jem.187.12.2037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Cesana GC, DeRaffele G, Cohen S, Moroziewicz D, Mitcham J, Stoutenburg J, Cheung K, Hesdorffer C, Kim-Schulze S, Kaufman HL.. Characterization of cd4+cd25+ regulatory t cells in patients treated with high-dose interleukin-2 for metastatic melanoma or renal cell carcinoma. J Clin Oncol 2006; 24:1169-77; PMID:16505437; http://dx.doi.org/ 10.1200/JCO.2005.03.6830 [DOI] [PubMed] [Google Scholar]
- [21].McDermott DF. The application of high-dose interleukin-2 for metastatic renal cell carcinoma. Med Oncol 2009; 1:13-7; http://dx.doi.org/ 10.1007/s12032-008-9152-1 [DOI] [PubMed] [Google Scholar]
- [22].Monk P, Lam E, Mortazavi A, Kendra K, Lesinski GB, Mace TA, Geyer S, Carson WE 3rd, Tahiri S, Bhinder A, et al.. A phase i study of high-dose interleukin-2 with sorafenib in patients with metastatic renal cell carcinoma and melanoma. J Immunother 2014; 37:180-6; PMID:24598448; http://dx.doi.org/ 10.1097/CJI.0000000000000023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Yamada Y, Nadazdin O, Boskovic S, Lee S, Zorn E, Smith RN, Colvin RB, Madsen JC, Cosimi AB, Kawai T, et al.. Repeated injections of il-2 break renal allograft tolerance induced via mixed hematopoietic chimerism in monkeys. Am J Transplant 2015; 17:13382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Kawai T, Cosimi AB, Wee SL, Houser S, Andrews D, Sogawa H, Phelan J, Boskovic S, Nadazdin O, Abrahamian G, et al.. Effect of mixed hematopoietic chimerism on cardiac allograft survival in cynomolgus monkeys. Transplantation 2002; 73:1757-64; PMID:12084998; http://dx.doi.org/ 10.1097/00007890-200206150-00011 [DOI] [PubMed] [Google Scholar]
- [25].Tonsho M, Lee S, Aoyama A, Boskovic S, Nadazdin O, Capetta K, Smith RN, Colvin RB, Sachs DH, Cosimi AB, et al.. Tolerance of lung allografts achieved in nonhuman primates via mixed hematopoietic chimerism. Am J Transplant 2015; 15:2231-9; PMID:25904524; http://dx.doi.org/ 10.1111/ajt.13274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Koyama I, Nadazdin O, Boskovic S, Ochiai T, Smith RN, Sykes M, Sogawa H, Murakami T, Strom TB, Colvin RB, et al.. Depletion of cd8 memory t cells for induction of tolerance of a previously transplanted kidney allograft. Am J Transplant 2007; 7:1055-61; PMID:17286617; http://dx.doi.org/ 10.1111/j.1600-6143.2006.01703.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Yamada Y, Boskovic S, Aoyama A, Murakami T, Putheti P, Smith RN, Ochiai T, Nadazdin O, Koyama I, Boenisch O, et al.. Overcoming memory t-cell responses for induction of delayed tolerance in nonhuman primates. Am J Transplant 2012; 12:330-40; PMID:22053723; http://dx.doi.org/ 10.1111/j.1600-6143.2011.03795.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Kawai T, Andrews D, Colvin RB, Sachs DH, Cosimi AB.. Thromboembolic complications after treatment with monoclonal antibody against cd40 ligand. Nat Med 2000; 6:114; http://dx.doi.org/ 10.1038/72162 [DOI] [PubMed] [Google Scholar]
- [29].Yamada Y, Ochiai T, Boskovic S, Nadazdin O, Oura T, Schoenfeld D, Cappetta K, Smith RN, Colvin RB, Madsen JC, et al.. Use of ctla4ig for induction of mixed chimerism and renal allograft tolerance in nonhuman primates. Am J Transplant 2014; 14:2704-12; PMID:25394378; http://dx.doi.org/ 10.1111/ajt.12936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Kawai T, Cosimi AB, Spitzer TR, Tolkoff-Rubin N, Suthanthiran M, Saidman SL, Shaffer J, Preffer FI, Ding R, Sharma V, et al.. Hla-mismatched renal transplantation without maintenance immunosuppression. N Engl J Med 2008; 358:353-61; PMID:18216355; http://dx.doi.org/ 10.1056/NEJMoa071074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Kawai T, Sachs DH, Sykes M, Cosimi AB.. Hla-mismatched renal transplantation without maintenance immunosuppression. N Engl J Med 2013; 9:1850-2; http://dx.doi.org/ 10.1056/NEJMc1213779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Kawai T, Sachs DH, Sprangers B, Spitzer TR, Saidman SL, Zorn E, Tolkoff-Rubin N, Preffer F, Crisalli K, Gao B, et al.. Long-term results in recipients of combined hla-mismatched kidney and bone marrow transplantation without maintenance immunosuppression. Am J Transplant 2014; 14:1599-611; PMID:24903438; http://dx.doi.org/ 10.1111/ajt.12731 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Spitzer TR, Delmonico F, Tolkoff-Rubin N, McAfee S, Sackstein R, Saidman S, Colby C, Sykes M, Sachs DH, Cosimi AB.. Combined histocompatibility leukocyte antigen-matched donor bone marrow and renal transplantation for multiple myeloma with end stage renal disease: The induction of allograft tolerance through mixed lymphohematopoietic chimerism. Transplantation 1999; 68:480-4; PMID:10480403; http://dx.doi.org/ 10.1097/00007890-199908270-00006 [DOI] [PubMed] [Google Scholar]
- [34].Farris AB, Taheri D, Kawai T, Fazlollahi L, Wong W, Tolkoff-Rubin N, Spitzer TR, Iafrate AJ, Preffer FI, Locascio SA, et al.. Acute renal endothelial injury during marrow recovery in a cohort of combined kidney and bone marrow allografts. Am J Transplant 2011; 11:1464-77; PMID:21668634; http://dx.doi.org/ 10.1111/j.1600-6143.2011.03572.x [DOI] [PMC free article] [PubMed] [Google Scholar]