

Abstract
Objective: This study is the second of four to prepare International Classification of Functioning, Disability and Health (ICF; and Children and Youth version, ICF(‐CY)) Core Sets for Autism Spectrum Disorder (ASD).The objective of this study was to survey the opinions and experiences of international experts on functioning and disability in ASD. Methods: Using a protocol stipulated by the World Health Organization (WHO) and monitored by the ICF Research Branch, an email‐based questionnaire was circulated worldwide among ASD experts, and meaningful functional ability and disability concepts were extracted from their responses. These concepts were then linked to the ICF(‐CY) by two independent researchers using a standardized linking procedure. Results: N = 225 experts from 10 different disciplines and all six WHO‐regions completed the survey. Meaningful concepts from the responses were linked to 210 ICF(‐CY) categories. Of these, 103 categories were considered most relevant to ASD (i.e., identified by at least 5% of the experts), of which 37 were related to Activities and Participation, 35 to Body functions, 22 to Environmental factors, and 9 to Body structures. A variety of personal characteristics and ASD‐related functioning skills were provided by experts, including honesty, loyalty, attention to detail and creative talents. Reported gender differences in ASD comprised more externalizing behaviors among males and more internalizing behaviors in females. Conclusion: The ICF(‐CY) categories derived from international expert opinions indicate that the impact of ASD on functioning extends far beyond core symptom domains. Autism Res 2016, 9: 959–969. © 2016 The Authors Autism Research published by Wiley Periodicals, Inc. on behalf of International Society for Autism Research
Keywords: autism, neurodevelopmental disorder, assessment, child psychiatry, heterogeneity, quality of life
Introduction
A multitude of research provides information on the impact of Autism Spectrum Disorder (ASD) on functioning in everyday life. Poor outcomes are reported in terms of education, employment, social relationships, independent living, mental health, and quality of life [Bölte & Poustka, 2002; Howlin & Moss, 2012; Lai & Lombardo, Baron‐Cohen, 2014]. Studies also reveal substantial interindividual differences in outcomes and levels of functioning for individuals with ASD, with factors such as intelligence quotient, language abilities, and comorbid conditions (e.g., ADHD, epilepsy, and generalized anxiety disorder), in combination with factors pertaining to the environment like access to intervention programs and availability of support services accounting for the largest part of the variability [Brundson & Happé, 2014; Levy & Perry, 2011]. There is also evidence that ASD is associated with certain gender differences [Bölte, Dukretis, Poustka, & Holtmann, 2011; Halladay et al., 2015; Holtmann, Bölte, & Poustka, 2007] and strengths [Happé & Frith, 2009; Mottron, Dawson, & Soulières, 2009] such as visual spatial, analytical or savant skills that may positively impact on an individual's level of functioning and quality of life. Although the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM‐5) [American Psychiatric Association, 2013] provides novel options for individualizing diagnosis in ASD through specifiers and severity/need of support ratings, it does neither provide explicit definitions for disability nor for adaptive functioning. The International Classification of Functioning (ICF; [WHO, 2001]) complements the International Classification of Diseases‐Tenth Revision [ICD‐10; World Health Organization (WHO), 1992], conceptualizing functioning and disability as being separate from pathology. It applies a biopsychosocial perspective to operationalize an individual's level of functioning as the interplay of abilities and disabilities that emerge in the contexts of physical constitution, social participation, personal as well as environmental resources [WHO, 2001]. Moreover, the ICF facilitates standardized assessment of functioning and health by providing detailed classifications in the areas of Body functions (i.e., physiological functions of body systems), Body structures (i.e., anatomical parts of the body), Activities (i.e., execution of tasks), Participation (i.e., involvement in life situations), and Environmental factors (i.e., physical, social and attitudinal environment). The bio‐psycho‐social model also includes Personal factors, but these have not yet been classified in the ICF given how these are grounded in social and cultural context. To capture the particular situation of a developing individual, the ICF Children and Youth version [ICF(‐CY); WHO, 2007] was derived from the ICF by adding development‐relevant categories and expanding on the descriptions of existing ICF categories.
The ICF and ICF(‐CY) (hereafter, “ICF(‐CY)”) consist of hierarchically structured categories describing aspects of functioning in the three key components of the bio‐psycho‐social model described above (i.e., Body Functions and Structures, Activities & Participation, Environmental factors) in up to four levels of increasing detail. The first level categories are known as chapters, and provide a general overview of the areas of functioning that are covered in the ICF(‐CY). The chapters consist of second, third and fourth level categories. The following example of an ASD‐relevant classification from the Body functions component shows the hierarchical structure of the ICF(‐CY):
Level 1 chapter: b1 Mental functions
Level 2 category: b167 Mental functions of language
Level 3 category: b1671 Expression of language
Level 4 category: b16710 Expression of spoken language
Consisting of over 1600 categories, the ICF(‐CY) provides a comprehensive framework for the classification of an individual's functioning. However, despite its potential value to health care and research [Bölte, 2009; Escorpizo et al., 2013], the ICF(‐CY)'s use is still rather limited, mostly because in its current full form it appears too generic for certain health conditions and impractical for daily use. To address this issue the development of ICF Core Sets was initiated. ICF Core Sets are shortlists of ICF(‐CY) categories that are considered most relevant to individuals with a certain health condition in clinical contexts. These ICF Core Sets are developed following a rigorous qualitative and quantitative, scientific protocol stipulated by the WHO and ICF Research Branch [Kostanjsek et al., 2011]. Its main objective is to use existing research data, involve a large and multi‐professional selection of researchers and clinicians, as well as service users/patients and their caregivers from all over the world to ensure universal applicability of the ICF Core Sets. The protocol consists of a systematic literature review (“research perspective”), an expert survey (current study, “opinion leader perspective”), focus groups (“client and caregiver perspective”), and a cross‐sectional clinical study (“clinical perspective”). Thus, the present study is embedded into the process of a larger research and development project, aimed at developing standardized ICF Core Sets for ASD. ICF Core Sets for ADHD are being developed as well in this project, but the results are reported in separate publications [Bölte et al., 2014a; De Schipper et al., 2015a]. In order to accomplish ICF Core Sets that cover functioning as well as disabilities in ASD across the life span, the development will be based on the ICF(‐CY), the extended version of the ICF, that captures not only functioning in adulthood but also childhood and youth. A complete description of the overall ASD ICF Core Set development process has been published in a previous issue of this journal [Bölte et al., 2014b].
The objective of this study was to capture the experiences and opinions of experts in the assessment and treatment of ASD. Together with the other three preparatory studies mentioned above, this expert survey generates content for an international ICF Core Sets Consensus Conference, during which a group of ASD experts from all WHO regions will follow a formal decision‐making process to arrive at ICF(‐CY) categories to be included in the ICF Core Sets for ASD.
Methods
Design
In an email‐based survey, professionals from various disciplines worldwide provided their perspectives on which features of ability, disability and context are to be considered essential for functioning in everyday life of individuals with ASD.
Recruitment Procedure
An internet search was performed to identify contact information for internationally known ASD experts and for centers (academic and community‐based), clinics and university departments in all WHO‐regions regularly involved in the assessment and management of individuals with ASD. Identified organizations were contacted via email with information about the study and a request to provide contact information of eligible experts. Contact information of experts was also provided by the project Steering Committee (see acknowledgement), a group of key opinion leaders in ASD from all WHO‐regions providing guidance on the project, and by the authors' personal professional networks. Finally, snowball sampling was applied, as all contacted experts were requested to recommend additional experts to be recruited for the survey. To be considered an “expert” for the purposes of this study, potential participants were required to (a) practice in one or more of the following professions: coach, counselor, nurse, occupational therapist, physician (e.g., psychiatrists, neurologists, etc.), physiotherapist, psychologist, psychotherapist, social worker, special educator, or speech and language therapist; (b) have at least five years of experience in the assessment and/or treatment of individuals with ASD; (c) fluency in English. These identified experts were then contacted via email and received information about the study along with a request to participate in the survey. If they agreed to participate, they were asked to fill in a reply sheet with information about their work experience to confirm their eligibility. After confirmation, the experts received the survey as a Word or PDF file via email, which they were requested to fill in and return within one month. Experts who did not submit the survey on time received up to three reminders to return their survey response and, if requested, they received extended time to respond. Data collection took place between September 2013 and October 2014.
Participating Experts
Experts were approached via email with an invitation to participate in the survey. The majority of them accepted the invitation. There were also some who did not respond to the invitation or declined the invitation. Reasons for declining the invitation were mostly a lack of time, but there were also some who felt their expertise was more theoretical than practical. Moreover, there were also experts who were ineligible to participate in the study (<5 years of experience). Participating experts received up to two reminders to return their survey response. An overview of the recruitment process is provided in Figure 1.
Figure 1.
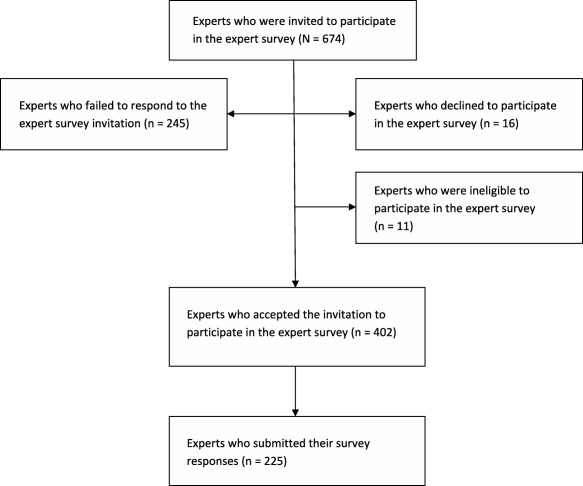
An overview of the recruitment process.
Thus, complete survey responses were obtained from 225 experts. A small minority of participating experts stated that they were practicing more than one profession, for example, worked both as a psychologist and as a psychotherapist. Participating experts represented 10 different professions and all six of the WHO‐regions (43 different countries). See Figure 2 for an overview of the representation of professions per WHO region and Table 1 for participants per professional group.
Figure 2.
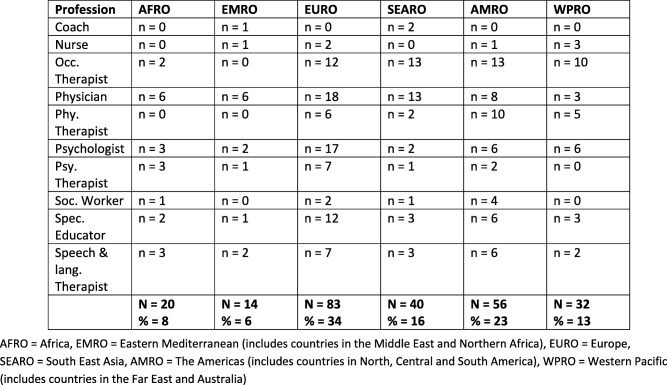
Representation of professions per WHO region (n = 245).
Table 1.
Representation of participants per professional group (some experts have been duplicated due to their multiprofessional background)
| Profession | N (%) |
|---|---|
| Physician | 54 (22%) |
| Occupational therapist | 50 (20%) |
| Psychologist | 36 (15%) |
| Special educator | 27 (11%) |
| Physiotherapist | 23 (9%) |
| Speech & language therapist | 23 (9%) |
| Psychotherapist | 14 (6%) |
| Social worker | 8 (4%) |
| Nurse | 7 (3%) |
| Coacha | 3 (1%) |
| 245 |
A profession in which an individual supports clients in achieving different goals in life, for example, improving school grades, finding a job, and so forth.
Participating experts ranged in age between 26 and 74 years, with a mean age of 47 years (SD=10.8). They had on average 16 years of experience in working with individuals with ASD (SD=8.0), ranging between 5 and 43 years. The majority of participating experts were females (76%). At the time of the survey, the participants spent the majority of their time working in clinical departments (45%), education (16%), or research (11%). A small group of experts worked mainly in management, or in other fields, such as training or supervision of other professionals (5%). The remaining experts divided their work time among more than one field (19%), mostly combining their work in the clinic with education or research. A proportion of 39% of experts worked with children and adolescents exclusively, 38% with children only, and 12% with ASD across the lifespan. A minority of the participants (2%) worked exclusively with adolescents and 4% with adults only, or a combination of these two age groups (4%). Three experts (1%) did not specify the age group of clients they encountered the most.
Expert Survey
The expert survey consisted of three parts (see Supporting Information Appendix S1). Part one contained questions about the participating expert's demography. Part two consisted of six questions regarding functioning and disability in individuals with ASD. The questions were specifically formulated to cover each component of the bio‐psycho‐social of the ICF(‐CY), using a similar approach as in previous ICF core set developments [Coenen et al., 2011]. Part two of the survey included two further questions, one concerning the possible functional strengths in ASD and the second possible gender differences in functioning and disability. Part three of the survey contained information regarding privacy and terms of agreement for taking part in the expert survey.
Identification of Meaningful Concepts and linking to the ICF(‐CY)
“Meaningful Concepts” are concise descriptions of specific behaviors, skills or other aspects of functioning that are to be linked to ICF(‐CY) categories. These concepts were extracted from the experts' survey responses and then linked to ICF(‐CY) categories following formalized linking rules and procedures determined by the WHO ICF Research Branch [Cieza et al., 2002; Cieza et al., 2005]. The linking rules provide guidance on how to link concepts to ICF(‐CY) categories, and what to do when that is not possible. Specific codes assigned to these concepts in the latter situation are (a) Personal factor, if the concept is not contained in the ICF(‐CY), but is clearly a Personal factor as defined in the ICF(‐CY); (b) non‐ covered, if the concept is not contained in the ICF(‐CY) and also is not a Personal factor; (c) non‐definable, when the information provided in the concept is not sufficient to assign it to a specific ICF(‐CY) category; and (d) health condition, if the concept refers to a diagnosis or health condition. Given that there are many different ways to describe the same aspect of functioning, it is possible for different meaningful concepts to be assigned to the same ICF(‐CY) category.
To assure the quality and consistency of results, both the identification of meaningful concepts (e.g., difficulties in decision making) and the linking to ICF(‐CY) categories (e.g., d177 Making decisions) was conducted independently by two researchers (ES and SM), who had received extensive linking training by the ICF Research Branch prior to the project. Linking results of each of the researchers were compared and consensus discussions were used to resolve disagreements. If consensus could not be reached, the coordinator of the ICF Research Branch (MS) was available to make final decisions. However, this option was never used because disagreements were resolved by discussion between the two researchers. The overall percentage of agreement between the two researchers (prior to consensus in case of disagreement) for the linking process was calculated. This was 81% for the second‐level ICF(‐CY) categories and 85% at the level of ICF(‐CY) chapters. Cohen's kappa and confidence intervals were calculated to examine the extent to which the agreements exceed chance. The kappa value was κ=0.81 (SE=0.004) with a 95% confidence interval of 0.80–0.81 for the second‐level categories. At the level of ICF(‐CY) chapters the Kappa value was κ=0.84 (SE=0.004) with a confidence interval of 0.83–0.84. These Kappa values indicate excellent interrater agreement.
Data Analysis
Frequency analysis was used to analyze the responses to the six ICF(‐CY) based questions of the survey. The absolute number of expert survey responses in which each of the ICF(‐CY) categories were identified, along with the corresponding percentages relative to the total number of responses received, was examined. ICF(‐CY) categories are presented at the second‐level. If a concept was linked to a third‐ or fourth‐level ICF(‐CY) category, the corresponding second‐level category was reported. Because the ICF(‐CY) is organized hierarchically, aspects of the more specific third‐ and fourth‐level categories were included in the less specific second‐level categories. Following the ICF Core Sets development guidelines [Selb et al., 2014], a second‐level ICF(‐CY) category that was identified repeatedly in the same expert survey response was counted only once. Consistent with WHO and previous core set development conventions [Escorpizo et al., 2011; Granberg et al., 2014], only ICF(‐CY) categories that were identified in at least 5% of the expert survey responses were included in the list of potential categories to be included in the Core Set for ASD. This is done to ensure that only those categories that are most relevant to a certain condition, in this case ASD, are included. Additional frequency analysis was used to explore the possible relation between experts' self‐identified expertise with respect to stage of development and the ICF(‐CY) categories identified in their survey responses. The last questions regarding specific abilities related to ASD and possible gender differences in functioning were not linked due to the fact that responses were inconsistent and heterogeneous, and therefore it was impossible to define meaningful concepts for linking. Instead, the answers were carefully reviewed independently by two researchers (ES and SM) before recurring themes or patterns of answers were summarized.
Results
Linking Results
In total, 8792 meaningful concepts were extracted from 225 survey responses. These concepts were linked to 210 second‐level ICF(‐CY) categories, 191 Personal factors (e.g., self‐esteem, restricted interests), 611 non‐definable codes (e.g., structured environment, behavior problems), 208 noncovered codes (e.g., stress, social rejection), and 41 health condition‐codes (e.g., depression, dyspraxia, epilepsy). The nondefinable codes and noncovered codes were mostly identified in the questions that captured the environmental factors of functioning and disability, whereas the health‐condition codes were mostly applied in questions related to Body functions and Body structures component.
Of the identified ICF(‐CY) categories, 103 were found in the responses of at least 5% of the experts (range: 5–87%) and are included in the list of candidate categories. Each of the four components of the ICF(‐CY) are represented in these categories, with 37 categories from Activities and Participation, 35 from Body functions, 22 from Environmental factors, and 9 from Body structures. The second‐level categories that were identified in the Activities and Participation component are presented in Table 2, along with the number and percentage of expert survey responses in which they were identified. They cover eight of the nine chapters making up the component, that is, (d5) self‐care, (d7) interpersonal interactions and relationships, (d8) major life areas, (d2) general tasks and demands, (d3) communication, (d1) learning and applying knowledge, (d4) mobility, and (d9) community, social and civic life.
Table 2.
Absolute and relative frequencies of ICF(‐CY) categories from the Activities and Participation component
| Second level category | N (%) |
|---|---|
| d720 complex interpersonal interactions | 101 (45%) |
| d440 fine hand use | 89 (40%) |
| d710 basic interpersonal interactions | 85 (38%) |
| d446 fine foot use | 70 (31%) |
| d230 carrying out daily routine | 68 (30%) |
| d310 communicating with—receiving—spoken messages | 62 (28%) |
| d335 producing nonverbal messages | 59 (26%) |
| d570 looking after one's health | 59 (26%) |
| d820 school education | 59 (26%) |
| d920 recreation and leisure | 56 (25%) |
| d750 informal social relationships | 55 (24%) |
| d177 making decisions | 47 (21%) |
| d250 managing one's own behavior | 47 (21%) |
| d330 speaking | 47 (21%) |
| d315 communicating with—receiving—nonverbal messages | 46 (20%) |
| d240 handling stress and other psychological demands | 31 (14%) |
| d530 toileting | 30 (13%) |
| d830 higher education | 27 (12%) |
| d510 washing oneself | 26 (12%) |
| d350 conversation | 25 (11%) |
| d550 eating | 24 (11%) |
| d880 engagement in play | 24 (11%) |
| d130 copying | 23 (10%) |
| d760 family relationships | 23 (10%) |
| d825 vocational training | 23 (10%) |
| d845 acquiring, keeping and terminating a job | 21 (9%) |
| d220 undertaking multiple tasks | 20 (9%) |
| d520 caring for body parts | 20 (9%) |
| d540 dressing | 20 (9%) |
| d571 looking after one's safety | 19 (8%) |
| d163 thinking | 18 (8%) |
| d740 formal relationships | 16 (7%) |
| d210 undertaking a single task | 15 (7%) |
| d850 remunerative employment | 15 (7%) |
| d455 moving around | 14 (6%) |
| d160 focusing attention | 12 (5%) |
| d770 intimate relationships | 12 (5%) |
Table 3 presents the absolute and relative frequencies of the second‐level categories that were identified in the Body functions component. Five out of the eight chapters making up this component are represented in these categories. The majority of categories were identified in the chapter (b1) mental functions. The remainder of categories was identified in four additional chapters, that is, (b2) sensory functions and pain, (b7) neuromusculoskeletal and movement‐related functions, (b3) voice and speech functions, and (b5) functions of the digestive, metabolic and endocrine systems. Four out of the five most often identified categories in this component are mental functions. The most often identified category pertains to movement‐related function.
Table 3.
Absolute and relative frequencies of ICF(‐CY) categories from the Body Functions component
| Second level category | N (%) |
|---|---|
| b760 control of voluntary movement functions | 156 (69%) |
| b164 higher‐level cognitive functions | 151 (67%) |
| b147 psychomotor functions | 117 (52%) |
| b156 perceptual functions | 108 (48%) |
| b152 emotional functions | 105 (47%) |
| b125 dispositions and intra‐personal functions | 97 (43%) |
| b167 mental functions of language | 82 (36%) |
| b765 involuntary movement functions | 81 (36%) |
| b140 attention functions | 80 (36%) |
| b265 touch function | 75 (33%) |
| b230 hearing functions | 71 (32%) |
| b117 intellectual functions | 62 (28%) |
| b260 proprioceptive function | 61 (27%) |
| b210 seeing functions | 60 (27%) |
| b255 smell function | 52 (23%) |
| b270 sensory functions related to temperature and other stimuli | 52 (23%) |
| b130 energy and drive functions | 49 (22%) |
| b250 taste function | 49 (22%) |
| b163 basic cognitive functions | 48 (21%) |
| b235 vestibular functions | 45 (20%) |
| b735 muscle tone functions | 45 (20%) |
| b122 global psychosocial functions | 41 (18%) |
| b180 experience of self and time functions | 37 (16%) |
| b160 thought functions | 35 (16%) |
| b134 sleep functions | 34 (15%) |
| b770 gait pattern functions | 34 (15%) |
| b126 temperament and personality functions | 31 (14%) |
| b176 mental function of sequencing complex movements | 24 (11%) |
| b144 memory functions | 22 (10%) |
| b515 digestive functions | 19 (8%) |
| b330 fluency and rhythm of speech functions | 18 (8%) |
| b114 orientation functions | 17 (8%) |
| b280 sensation of pain | 17 (8%) |
| b320 articulation functions | 15 (7%) |
| b310 voice functions | 12 (5%) |
Absolute and relative frequencies of the second‐level categories identified in the Environmental factors component are presented in Table 4. All five of this component's chapters are represented by these categories, that is, (e3) support and relationships, (e4) attitudes, (e1) products and technology, (e5) services, systems and policies, and (e2) natural environment and human‐made changes to environment.
Table 4.
Absolute and relative frequencies of ICF(‐CY) categories from the Environmental Factors component
| Second level category | N (%) |
|---|---|
| e310 immediate family | 100 (44%) |
| e585 education and training services, systems and policies | 100 (44%) |
| e580 health services, systems and policies | 84 (37%) |
| e115 products and technology for personal use in daily living | 68 (30%) |
| e460 societal attitudes | 51 (23%) |
| e410 individual attitudes of immediate family members | 41 (18%) |
| e125 products and technology for communication | 37 (16%) |
| e250 sound | 37 (16%) |
| e590labor and employment services, systems and policies | 34 (15%) |
| e360 other professionals | 28 (12%) |
| e575 general social support services, systems and policies | 26 (12%) |
| e240 light | 22 (10%) |
| e165 assets | 19 (8%) |
| e340 personal care providers and personal assistants | 17 (8%) |
| e355 health professionals | 17 (8%) |
| e425 individual attitudes of acquaintances, peers, colleagues, neighbors and community members | 17 (8%) |
| e455 individual attitudes of health‐related professionals | 15 (7%) |
| e465 social norms, practices and ideologies | 15 (7%) |
| e155 design, construction and building products and technology of buildings for private use | 14 (6%) |
| e325 acquaintances, peers, colleagues, neighbors and community members | 12 (5%) |
| e315 extended family | 11 (5%) |
| e450 individual attitudes of health professionals | 11 (5%) |
Table 5 shows the second‐level categories that were identified in the Body structures component, together with their absolute and relative frequencies. These represent five out of eight chapters making up this component. By far the most frequently identified category was from chapter (s1) structures of the nervous system, which was mentioned by 87% of the experts, making it the most often identified of all ICF(‐CY) categories in this study. Other categories from this component were derived less often, and represent four additional chapters, that is, (s5) structures related to the digestive, metabolic and endocrine systems, (s7) structures related to movement, (s2) the eye, ear and related structures, and (s3) structures involved in voice and speech.
Table 5.
Absolute and relative frequencies of ICF(‐CY) categories from the Body Structures component
| Second level category | N (%) |
|---|---|
| s110 structure of brain | 195 (87%) |
| s540 structure of intestine | 34 (15%) |
| s730 structure of upper extremity | 18 (8%) |
| s750 structure of lower extremity | 16 (7%) |
| s530 structure of stomach | 15 (7%) |
| s520 structure of esophagus | 14 (6%) |
| s260 structure of inner ear | 12 (5%) |
| s320 structure of mouth | 11 (5%) |
| s770 additional musculoskeletal structures related to movement | 11 (5%) |
Additional frequency analysis of 10% of the expert survey responses was conducted in order to explore a possible relationship between the age group in which the experts are specialized in and the ICF(‐CY) categories that were identified in their survey responses. The analysis showed that a large majority of the categories in the survey responses were identified across the lifespan. There were, however, a few categories more often identified for children as compared to adults: e310 Immediate family, e585 Education and training services, systems and policies, d440 Fine hand use, d446 Fine foot use and d740 Informal social relationships. Given that children usually live with their immediate family and attend school on a regular basis, some of the categories (e.g., e310 Immediate family and e585 Education and training services, systems and policies) covered in the experts' survey responses are not surprising.
ASD‐Related Abilities
A large majority of experts (92%) indicated observed ASD‐related skills, many of which were reported to be mainly associated with higher functioning individuals. The experts further remarked that these skills need to be actively recognized and nurtured in order for the individuals to reach their full potential. Skills and abilities that were often mentioned by the experts are summarized in Table 6.
Table 6.
Overview of ASD‐related skills and abilities mentioned by the experts
| Abilities and skills |
|---|
| Attention to detail |
| Strong sense of morality (e.g., honesty, lack of judgmental attitude, etc.) |
| A preference to work on repeated or monotonous tasks |
| Expertise in a specific area |
| Mathematical abilities |
| Creative talents (e.g., look at the world differently) |
| Artistic skills (e.g., music, drawing, visual arts) |
| Visual perception |
| Intellectual functions |
| Technical abilities (computer skills, engineering) |
| Trustworthiness |
| Loyalty |
| Kindness |
| Good memory |
Gender Differences
Sixty percent of the surveyed experts reported gender‐related differences in ASD. Of those, more than half replied that they had observed gender differences in functioning and disabilities. Some experts highlighted that these differences were dependent on the age range and intellectual capacities, and that observed differences might not necessarily be specific to ASD, but rather, reflect gender differences in the general population. Other experts indicated that males with ASD tend to show more externalizing behavioral difficulties (hyperactivity, aggression) than females, making them easier to diagnose. On the other hand, females with ASD were described to be better socially adjusted, showing more prosocial behaviors, communication skills and friendships than males, making them easily overlooked. Additional experts perceived females and males with ASD to share core abilities and disabilities, but also experienced that females invested more efforts in blending in, complying with social demands and hiding their difficulties. Experts concluded that this might not only lead to underdiagnosing females, but also to higher expectations on females with ASD, which in turn results in increased levels of stress and anxiety, and a greater sense of failure, compared to males with ASD. Males with ASD were described as more pronounced in socially unadjusted and unaccepted behaviors, leading to more social exclusion, fewer friendships, and more bullying. Males as compared to females with ASD seemed on the other hand less emotionally affected by social exclusion, showing a lower average desire for social participation.
Discussion
The objective of the present study was to characterize functioning aspects and disabilities that are often associated with ASD, based on the perspectives of experts who assess and treat the disorder. To this end, an email‐based survey was conducted among a large sample of international experts from multiple professions. The experiences and opinions of such a large and diverse international group of ASD experts on this topic have not been systematically examined previously. The list of candidate ICF(‐CY) categories derived from the current study will be combined with the identified categories from three additional preparatory studies to form the basis for an “ICF Core Sets for ASD” consensus conference. At this conference a group of international ASD‐experts will determine which ICF(‐CY) categories should be included in the first official ICF Core Sets for ASD, on the basis of which diagnostic tools (observation schedules, questionnaire, interviews) will be derived and standardized for broad use in clinical and research settings. These tools will be ready made and easily implementable for clinicians.
The present study identified a large number of categories covering all four components contained in the ICF(‐CY). It underlines that experts accept ASD to be a complex condition involving many physical, environmental and personal factors and areas of life. The most frequently identified category was (s110) structure of brain from the Body structures, indicating that there is consensus among international experts of various professions that ASD is a brain‐based condition. However, as indicated by other derived categories (s2, s3, s5, s7), body structures related to voice and speech, movement and digestive system are also presumed to be closely related to ASD. Not surprisingly, multiple categories from the Activities and Participation component were derived, such as problems with social relationships (d7) and communication (d3), which constitute the core symptoms of ASD as described in the DSM‐5. Nevertheless, the majority of identified categories represent other challenges, including the ability to take care of oneself and manage everyday life and tasks (d5, d2), participation in school, work and social life (d8, d9), and cognitive and motor skills (d1, d4). Categories identified in the Body functions component concern a rich variation of mental functions (b1), such as language (b167), perception (b156), emotion (b152), and attention (b140). Furthermore, categories from other chapters suggest a broader range of ASD‐related problems, for example, sensation (b2), problems with speech (b3), and with digestion (b5). Finally, the categories identified from the Environmental factors component indicate that the social context, both individual support and common attitudes towards individuals with ASD (e3, e4), organized support and services provided by professionals (e5), the physical context and environment (e1, e2) (products designed to be helpful for coping with challenges in everyday life; physical environment in general), interact with an individual's functioning and disabilities in determining their level of everyday functioning. These findings endorse the usefulness of the bio‐psycho‐social model of the ICF(CY), which describes functioning as a dynamic interaction between health condition and contextual factors.
This study is among the first to explore specific strengths and gender differences in ASD as perceived by experts from different professions and cultures. Overall, opinions put forward were too heterogeneous and inconsistent to derive meaningful concepts and link ICF categories. Thus, this survey data was analyzed qualitatively, in which recurring aspects of functioning and abilities mentioned by the experts were summarized without additional frequency analysis. Our survey data should, however, in the future be more comprehensively examined using thematic analyzes in a separate study. Many experts reported both certain abilities and positive traits linked to ASD and phenotypes related to gender in ASD. Some of the survey findings such as an overrepresentation of savant and scientific talents in ASD are supported by research [e.g., Treffert, 2014], while others, such as a strong sense of justice, loyalty and helpfulness currently have not been systematically investigated. Surprisingly, research findings of gender differences in ASD, such as repetitive behaviors being more pronounced in males than females with ASD (Szatmari et al., 2011), were not consistently reported by experts. On the other hand, differing comorbidity profiles were often mentioned by the experts, despite the fact that research has shown mixed results [Holtmann et al., 2007; Rubenstein, Wiggins, & Lee, 2015]. In summary, the expert survey data on these topics demonstrate not merely deficits, but also strengths oriented views on ASD among experts, and a widespread awareness that gender issues might be significant for understanding ASD. Furthermore, they generate novel hypotheses based on clinical experience to be tested in future studies.
Certain meaningful concepts in the expert survey responses which the experts identified could not be translated into ICF(‐CY) categories. Indeed, the large number of nondefinable codes (n=611) invites closer examination. Nondefinable codes are largely explained by the fact that experts were free to answer the questions in the survey in their own words and expressions. Even though the experts were instructed to be as concrete as possible in their survey responses, the answers provided by them were sometimes very brief or ambiguous (e.g., “behavior,” “participation”) or formulated in general terms (e.g., “social impairment,” “adaptive skills”). Consequently, this presented a challenge for the linking. Nevertheless, a closer look at the non‐definable codes revealed a few recurring themes, such as the level of structure and routine in the environment (e.g., “structured environment,” “daily routine”), the level of sensory input from the environment (e.g., “sensory overload,” “limited distractions”), and the general adjustment of the environment to the individual's needs and abilities (e.g., “autism‐friendly environment,” “balance between abilities and demands from environment”).
Whilst the current study provides a unique, worldwide, multidisciplinary expert perspective on functioning and disability in individuals with ASD, it cannot be assumed that it is complete, exhaustive or representative of the totality of experts around the globe. For instance, even though experts included in the study represented a broad range of different professions and all six of the WHO‐regions, some professions were represented by very few experts or no experts at all in certain regions. As such, the identified categories may reflect in part the composition of experts who were surveyed. Notably, there may be certain professions (e.g., psychologists) whose role is not yet established in the assessment or treatment of individuals with ASD in some countries (e.g., Azerbaijan). Restricting the survey to professionals proficient in the English language may have also limited participation in some WHO‐regions. For instance, in regions or countries where English is not commonly used, such as Central and South‐America (e.g., Mexico and Uruguay) and the Middle East (e.g., Qatar), some invited experts were unable to participate due to this restriction. The four preparatory studies combined will however make it possible for one study to fill in the gaps of another study. For example, certain countries (e.g., Brazil) or regions (e.g., the Middle East) may be underrepresented in this study and in the systematic literature review given the requirement for publications to be in English and more general research opportunity inequalities, but these will have a stronger representation in the upcoming qualitative and clinical studies. Language should not be a barrier in these studies, since collaborations with members from the Steering Committee and other international study sites will allow for the use of local languages. The focus group study will consist of group discussions with different stakeholders (clients with ASD, their families, professional caregivers), whereas the clinical study will involve investigation of problems as experienced by actual patients in real life clinical settings. All in all, the results of the four studies together should provide us with a comprehensive picture of the specific abilities and disabilities that are related to functioning in ASD for individuals across different countries, cultures and life situations.
The use of written survey might also have caused difficulties in verifying that the questions were always interpreted correctly by the experts, as it would have been possible in a face‐to‐face interview. Some experts (n = 17) indicated that they were unsure what was intended with a certain question and thus refrained from answering. In other cases experts (n = 5) explicitly stated that they may have misinterpreted the questions. Furthermore there were also technical issues to the study resulting in some of the participating experts being unable to open or work with several versions of the Word‐ and PDF‐files of the survey. These experts were therefore unable to submit their survey responses, as a result of which their expert opinion was not included in the final results of this study. However, these were just very few participants (n = 3), unlikely to have affected the study validity.
It is important to see the findings of the current study in the context of the larger project. This study is the second of four studies conducted in the process of developing ICF Core Sets for ASD. The first, a systematic literature review aimed to capture the research perspective of functioning and disability related to ASD, and was previously reported in this journal [De Schipper, et al., 2015b). The current study showed that ASD is not only related to disability, but also to strengths and abilities (e.g., honesty, attention to detail, persistence, etc.). These findings are inconsistent with the results that the systematic literature review study yielded, which only provided evidence for disabilities. One reason for the inconsistency might be related to the fact that in the expert survey a specific question was designed to capture the possible strengths and abilities pertaining to ASD, whereas in the systematic literature review this option was not available. Moreover, categories from the Body structures component (e.g., brain, intestine and upper extremities) were identified in this study, but not in the systematic literature review. These two studies also differed in respect to the categories that were identified in the Body functions component. While both studies found that mental functions were affected in ASD, the expert survey also showed aspects of movement‐related functioning (e.g., coordination and control of voluntary movement functions) and mobility (e.g., fine hand use) to be very relevant in ASD. Consistent with the literature review, the core defining features of ASD, social‐communication characteristics, were captured by ICF(‐CY) categories from the interpersonal interaction and communication chapters in the current study.
The results acquired from the expert survey demonstrate the complexity of ASD. Thus, enhanced communication between different stakeholders is required in order to improve functioning and quality of life for individuals with ASD. The ICF Core Sets for ASD can meet this objective by providing professionals and other stakeholders with terminology and definitions of functioning that are universally applicable and understandable irrespective of disciplinary, cultural and country borders.
Conflict of interest
Elles de Schipper declares that she has no conflict of interest related to this work. Soheil Mahdi declares that he has no conflict of interest related to this work. Petrus J de Vries declares no conflict of interest related to this work. He has served as study steering committee member, advisory board member, and working group member for a number of studies on Tuber Sclerosis Complex funded or part‐funded by Novartis. Mats Granlund declares no conflict of interest related to this work. Martin Holtmann declares no conflict of interest related to this work. In the last 5 years he served in an advisory or consultancy role for Lilly and Shire, and received conference attendance support or was paid for public speaking by Bristol‐Myers Squibb, Janssen‐Cilag, Lilly, Medice, Neuroconn, Novartis and Shire. Sunil Karande declares no conflict of interest related to this work. Omar Almodayfer declares no conflict of interest related to this work. Cory Shulman declares no conflict of interest related to this work. Bruce Tonge declares no conflict of interest related to this work. Virginia C.N. Wong declares no conflict of interest related to this work. Lonnie Zwaigenbaum declares no conflict of interest related to this work. He has in the last 3 years received grant funding from SynaptDx. Sven Bölte declares no conflict of interest related to this work. He has in the last 3 years acted as a consultant or lecturer for Shire, Roche, Eli Lilly, Prima Psychiatry, Kompetento, Expo Medica and Prophase, and receives royalties from Kohlhammer and Hogrefe/Huber publishers.
Supporting information
Additional Supporting Information may be found in the online version of this article at the publisher's web‐site:
Appendix S1. The ASD expert survey
Acknowledgments
The development of the ICF Core Sets for ASD is a cooperative effort of the WHO, the ICF Research Branch, a partner of the WHO Collaboration Centre for the Family of International Classifications in Germany (at DIMDI), the International Society for Autism Research (INSAR), and the Center of Neurodevelopmental Disorders at the Karolinska Institutet (KIND) in Sweden. Guidance on this project is provided by a Steering Committee comprised of key opinion leaders in the field of ASD from all six WHO regions. This Steering Committee consists of the co‐authors of this paper and John E. Robison, Melissa Selb, Nidhi Singhal, Susan Swedo and Bedirhan Üstün. The development of ICF Core Sets for ASD is supported by the Swedish Research Council (grant nr. 523‐2009‐7054), and the Swedish Research Council in partnership with FAS (now renamed FORTE), FORMAS, and VINNOVA (trans‐disciplinary research program on child and youth mental health, grant nr. 259‐2012‐24).
References
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders (5th ed). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Brundson, V.E.A. , & Happé, F. (2014). Exploring the ‘fractionation’ of autism at the cognitive level. Autism, 18, 17–30. [DOI] [PubMed] [Google Scholar]
- Bölte, S. (2009). The ICF and its meaning for child and adolescent psychiatry. Zeitschriftfür Kinder‐und Jugendpsychiatrie und Psychotherapie, 37, 495–497. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , de Schipper, E. , Holtmann, M. , Karande, S. , de Vries, P.J. , Selb, M. , & Tannock, R. (2014a). Development of ICF Core Sets to standardize assessment of functioning and impairment in ADHD: the path ahead. European Child and Adolescent Psychiatry, 23, 1139–1148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bölte, S. , de Schipper, E. , Robison, J.E. , Wong, V.C.N. , Selb, M. , Singhal, N. , de Vries, P.J. , & Zwaigenbaum, L. (2014b). Classification of functioning and impairment: The Development of ICF Core Sets for Autism Spectrum Disorder. Autism Research, 7, 167–172. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , Dukretis, E. , Poustka, F. , & Holtmann, M. (2011). Sex differences in cognitive domains and their clinical correlates in higher‐functioning autism spectrum disorders. Autism, 15, 497–511. [DOI] [PubMed] [Google Scholar]
- Bölte, S. , & Poustka, F. (2002).The relation between general cognitive level and adaptive behavior domains in individualswith autism with and without co‐morbid mental retardation. Child Psychiatry and Human Development, 33, 165–172. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Brockow, T. , Ewert, T. , Amman, E. , Kollerits, B. , Chatterji, S. , Ustün, T.B. , & Stucki, G. (2002). Linking health‐status measurements to the international classification of functioning, disability and health. Journal of Rehabilitation Medicine, 34, 205–210. [DOI] [PubMed] [Google Scholar]
- Cieza, A. , Geyh, S. , Chatterji, S. , Kostanjsek, N. , Üstün, B. , & Stucki, G. (2005). ICF linking rules: An update based on lessons learned. Journal of Rehabilitation Medicine, 37, 212–218. [DOI] [PubMed] [Google Scholar]
- Coenen, M. , Cieza, A. , Freeman, J. , Khan, F. , Miller, D. , & Weise, A. Members of the Consensus Conference (2011). The development of ICF Core Sets for multiple sclerosis: results of the International Consensus Conference. Journal of Neurology, 258, 1477–1488. [DOI] [PubMed] [Google Scholar]
- De Schipper, E. , Lundequist, A. , Löfgren Wilteus, A. , Coghill, D. , de Vries, P.J. , Granlund, M. , Holtmann, M. , Jonsson, U. , Karande, S. , Levy, F. , Al‐Modayfer, O. , Rohde, L. , Tannock, R. , Tonge, B. , & Bölte, S. (2015a). A comprehensive scoping review of ability and disability in ADHD using the International Classification of Functioning, Disability and Health‐Children and Youth version (ICF(‐CY)). European Child & Adolescent Psychiatry, 24, 859–872. [DOI] [PubMed] [Google Scholar]
- De Schipper, E. , Lundequist, A. , Coghill, D. , de Vries, P.J. , Granlund, M. , Holtmann, M. , Jonsson, U. , Karande, S. , Robison, J.E. , Shulman, C. , Singhal, N. , Tonge, B. , Wong, V.C., Zwaigenbaum, L. & Bölte, S. (2015b). Ability and disability in autism spectrum disorder: A systematic literature review employing the international classification of functioning, disability and health‐children and youth version. Autism Research. doi 10.1002/aur. 1485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Escorpizo, R. , Finger, M.E. , Glässel, A. , & Cieza, A. (2011). An international expert survey on functioning in vocational rehabilitation using the international classification of functioning, disability and health. Journal of Occupational Rehabilitation, 21, 147–155. [DOI] [PubMed] [Google Scholar]
- Escorpizo, R. , Kostanjsek, N. , Kennedy, C. , Robinson Nicol, M.M. , Stucki, G. , Üstün, T.B. , & Functioning Topic Advisory Group (fTAG) of the ICD‐11 Revision . (2013). Harmonizing WHO's International Classification of Diseases (ICD) and International Classification of Functioning, Disability and Health (ICF): Importance and methods to link disease and functioning. BMC Public Health, 13, 742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granberg, S. , Swanepoel, D.W. , Englund, U. , Möller, C. , & Danermark, B. (2014).The ICF core sets for hearing loss project: International expert survey on functioning and disability of adults with hearing loss using the international classification of functioning, disability and health (ICF). International Journal of Audiology, 53, 497–506. [DOI] [PubMed] [Google Scholar]
- Halladay, A.K. , Bishop, S. , Constantino, J.N. , Daniels, A.M. , Koenig, K. , Palmer, K. , Messinger, D. , Pelphrey, K. , Sanders, S.J. , Singer, A.T. , Taylor, J.L. , & Szatmari, P. (2015). Sex and gender differences in autism spectrum disorder: Summarizing evidence gaps and identifying emerging areas of priority. Molecular Autism, 6, 36. doi:10.1186/s13229-015-0019-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Happé, F. , & Frith, U. (2009). The beautiful otherness of the autistic mind. Philosophical Transactions of the Royal Society B, 364, 1345–1350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holtmann, M. , Bölte, S. , & Poustka, F. (2007). Autism spectrum disorders: Sex differences in autistic behaviour domains and coexisting psychopathology? Developmental Medicine & Child Neurology, 49, 361–366. [DOI] [PubMed] [Google Scholar]
- Howlin, P. , & Moss, P. (2012). Adults with autism spectrum disorders. Canadian Journal of Psychiatry, 57, 275–283. [DOI] [PubMed] [Google Scholar]
- Kostanjsek, N. , Rubinelli, S. , Escorpizo, R. , Cieza, A. , Kennedy, C. , Selb, M. , Stucki, G. , & Üstün, T.B . (2011). Assessing the impact of health conditions using the ICF. Disability Rehabilitation, 33, 1475–1482. [DOI] [PubMed] [Google Scholar]
- Lai, M.C. , Lombardo, M.V. , & Baron‐Cohen, S. (2014). Autism. Lancet, 383, 896–910. [DOI] [PubMed] [Google Scholar]
- Levy, A. , & Perry, A. (2011). Outcomes in adolescents and adults with autism: A review of the literature. Research in Autism Spectrum Disorders, 5, 1271–1282. [Google Scholar]
- Mottron, L. , Dawson, M. , & Soulières, I. (2009). Enhanced perception in savant syndrome: Patterns, structure and creativity. Philosophical Transactions of the Royal Society B, 364, 1385–1391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rubenstein E, Wiggins L.D., & Lee L.C. (2015). A review of the differences in developmental, psychiatric, and medical endophenotypes between males and females with autism spectrum disorder. Journal of Developmental & Physical Disabilities, 27, 119–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Selb, M. , Escorpizo, R. , Kostanjsek, N. , Stucki, G. , Üstün, B. , & Cieza, A. (2014). A guide on how to develop an International Classification of Functioning, Disability and Health Core Set. European Journal of Physical and Rehabilitation Medicine, 51, 105–117. [PubMed] [Google Scholar]
- Szatmari, P. , Xiao‐Qing, L. , Goldberg, J. , Zwaigenbaum, L. , Paterson, A.D. , Woodbury‐Smith, M. , Georgiades, S. , Duku, E. , & Thompson, A. (2011). Sex differences in repetitive stereotyped behaviors in autism: Implications for genetic liability. American Journal of Medical Genetics Part B, 159, 5–12. [DOI] [PubMed] [Google Scholar]
- Treffert, D.A. (2014). Savant syndrome: realities, myths and misconceptions. Journal of Autism and Developmental Disorders, 44, 564–571. [DOI] [PubMed] [Google Scholar]
- World Health Organization . (1992). International statistical classification of diseases and related health problems (10th revision (ICD‐10)). Geneva: WHO. [Google Scholar]
- World Health Organization . (2001). International classification of functioning, disability and health: ICF. Geneva: World Health Organization. [Google Scholar]
- World Health Organization . (2007). International classification of functioning, disability and health: Children and youth version: ICF‐CY. Geneva: World Health Organization. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional Supporting Information may be found in the online version of this article at the publisher's web‐site:
Appendix S1. The ASD expert survey