

Abstract
Infant sleep consolidates rapidly during the first half year of life in the context of a dynamic, bidirectional exchange between infant characteristics and the caregiving environment. The current study examined relations among mothers’ emotional availability (EA) at bedtime, infant temperament, and objectively assessed infant sleep development from 1 to 6 months, and in particular focused on whether infant temperament moderated linkages between EA at bedtime and infant sleep development. The sample consisted of seventy-two mother-infant dyads, and measures included actigraphy-assessed infant sleep at 1 and 6 months, observed maternal EA coded from bedtime videos at 3 and 6 months, and maternal reports of infant temperament at 3 and 6 months. Analysis showed significant positive effects of maternal EA at bedtime on developmental changes in infant sleep minutes. Additionally, infant temperamental surgency moderated the influence of EA at bedtime on the increase in infant sleep minutes. In other words, highly surgent infants increased their sleep time more than other infants if their mothers were emotionally available at bedtime. Results were discussed in terms of the transactional model of infant sleep development.
Keywords: Infant sleep, emotional availability, temperament, the transactional model
1. Introduction
Infant sleep consolidates rapidly during the first half year of life, lengthening in nighttime sleep and reducing in waking frequency and duration (Burnham, Goodlin-Jones, Gaylor, & Anders, 2002; Henderson, France, & Blampied, 2011). While infant sleep follows a maturational trend and displays moderate stability over time (Anders & Keener, 1985; Scher, Epstein, & Tirosh, 2004), individual differences in sleep development are considerable (Burnham et al., 2002). Drawing from the transactional model of child development (Sameroff, 1989), Sadeh and colleagues proposed that infant sleep is influenced by dynamic, bidirectional exchanges between intrinsic infant characteristics and the caregiving environment (Sadeh & Anders, 1993; Sadeh, Tikotsky, & Scher, 2010). Although this model has been around for over two decades, most studies to date have examined the effect of parenting practices on infant sleep separately or additively from the effect of infant temperament on infant sleep, inadvertently dismissing their interaction effect. Moreover, despite the vast literature on parenting practices and infant sleep, parenting quality at bedtime has been rarely examined (Sadeh et al., 2010). The present study investigated the influences of bedtime parenting quality (emotional availability), infant temperament, and their interaction on the developmental changes in objectively assessed infant sleep from 1 to 6 months of life.
1.1. Parenting and Infant Sleep
Environment contributes substantially to sleep behaviors of infants and young children, according to recent behavioral genetic studies (Ando et al., 2006; Brescianini et al., 2011; Fisher, van Jaarsveld, Llewellyn, & Wardle, 2012; Touchette et al., 2013). Among environmental influences, parent-infant interactions at bedtime and during the night have been identified as significant predictors of infant sleep problems (Sadeh & Anders, 1993). For example, high level of parental involvement, short response latency to infant awakenings, and active soothing at bedtime have been related to frequent infant night wakings in correlational and experimental studies (Johnson, 1991; Mindell, Telofski, Wiegand, & Kurtz, 2009; Sadeh et al., 2010).
Most studies of linkages between parenting and infant sleep have focused on parenting practices, or what parents do, rather than on parenting quality (e.g., sensitivity, warmth, non-intrusiveness, etc.). At least two studies have shown that daytime parenting quality such as sensitivity (Priddis, 2009) and reduced dyadic tension (Minde, Faucon, & Falkner, 1994) was associated with better quality of infant sleep. Other studies (Teti, Kim, Mayer, & Countermine, 2010; Scher, 2001) have examined parenting quality as operationalized as emotional availability (EA) and infant sleep. The EA framework (Biringen, 2000) integrates attachment theory’s emphasis on parental sensitivity and infants’ secure base behavior, and emotional availability theory’s emphasis on dyadic affective attunement and emotional communication. Parental EA examines the ability of parents to understand their children’s cues and to give appropriate emotional responses, and it incorporates dimensions such as sensitivity, structuring, non-intrusiveness, and non-hostility. Parental EA has been demonstrated to contribute to child development in various domains and to child-parent attachment (Biringen, 2000; Easterbrooks, Bureau, & Lyons-Ruth, 2012). Child EA reflects the child’s affective quality and secure base behavior, and consists of dimensions of responsiveness to and involvement with the parent (Biringen, 2000). Using this framework, Scher (2001) found that higher levels of daytime infant EA, rather than parental EA, predicted more (not less) sleep disruptions in 12-month-old infants.
Only one published study to date has examined maternal EA at bedtime. Teti et al. (2010) adapted the Emotional Availability Scale (EAS; Biringen, Robinson, & Emde, 1998), which was originally developed in context of daytime parent-child interactions, to assess parenting quality at bedtime. In their study, mothers judged to be emotionally available were those who recognized and responded to infant cues appropriately (sensitivity), guided infants toward sleep using soothing bedtime routines (structuring), restrained from initiating active plays or talks with infants (non-intrusiveness), and expressed no overt or covert impatience or irritation (non-hostility). The study found that bedtime EA, but not specific parenting practices, predicted fewer infant sleep disruptions reported by mothers. The investigators proposed that maternal EA at bedtime would promote infants’ feelings of security and trust in their sleep environment, which in turn would help infants adapt to separation from their attachment figures during sleep. A potential weakness of their study, however, was the use of mothers’ reports of infant sleep (a daily sleep diary) rather than a more “objective” measure. Research showed that parental reports of infant sleep may provide useful estimates for sleep onset but tend to underestimate infant awakenings and overestimate actual sleep time (Scher, Epstein, Sadeh, Tirosh, & Lavie, 1992), perhaps because parents are unlikely to notice infant wakings that occurred without signaling. On the other hand, although movement-based actigraphy does not perfectly differentiate quiet wakefulness from sleep, it has been validated against polysomnography and used as a noninvasive, continuous measure of infant sleep (So, Buckley, Adamson, & Horne, 2005). Therefore, it is necessary to examine the effect of maternal EA during the bedtime period on infant sleep quality and quantity assessed by actigraphy. We hypothesized that higher maternal EA would predict increased sleep quantity and quality, above the effect of sleep maturation.
1.2. Infant Temperament and Infant Sleep
The development of infant sleep is likely to be influenced not only by parenting, but also by infant intrinsic characteristics, such as temperament, maturation, and other biomedical factors (Sadeh & Anders, 1993; Sadeh et al, 2010). Temperament has been variously conceptualized and defined (Buss & Plomin, 1984; Chess & Thomas, 1984; Goldsmith & Campos, 1982; Shiner et al., 2012). The present study makes use of Rothbart’s conceptualization of temperament, which defines it as “constitutionally based individual differences in reactivity and self-regulation, in the domains of affect, activity, and attention” (Rothbart & Bates, 1998, p. 100). This model describes infant temperament with three “superfactors” (Positive Emotionality/Surgency, Negative Affectivity, and Orienting/Regulation) (Gartstein & Rothbart, 2003), each of which contains a number of subdimensions. Our choice of Rothbart’s temperament model was based on its emphasis on the hierarchical structure of temperament and its conceptualization of temperament as indexing infant capacities for self-regulation (Shiner et al., 2012).
No published study has to date examined linkages between infant sleep and infant temperament using Rothbart’s measurement model. However, a number of previous studies using other temperament measures have found linkages between infant sleep and specific temperament dimensions that appear to map straightforwardly onto one of the three Rothbart superfactors. For example, infants characterized by positive mood, high approach, and high sociability have been found to sleep longer at night or have fewer sleep problems than infants characterized by negative mood, high withdrawal, and poor regulatory capacity (Atkinson, Vetere, & Grayson, 1995; Halpern, Anders, Garcia Coll, & Hua, 1994; Scher, Tirosh, & Lavie, 1998; Spruyt et al., 2008,Weissbluth, 1981). Positive mood, high approach, and high sociability appear to map straightforwardly onto Rothbart’s temperament superfactor of Positive Emotionality/Surgency, which describes infants who are emotionally positive, physically and verbally active, easily excited by and likely to approach novel or social stimuli. However, other temperament dimensions which are also nested in Rothbart’s model under Positive Emotionality/Surgency have not been associated with better infant sleep. For example, Kelmanson (2004) reported that infants with high activity level (characteristic of surgent infants) showed more variability in nighttime sleep than did infants with low activity level (Kelmanson, 2004). In addition, Carey (1974) and Sadeh et al. (1994) reported that infants and toddlers with low sensory thresholds (also characteristic of surgent infants) tended to wake up more frequently at night. Moreover, unlike negative affectivity and orienting/regulation, for which higher and lower scores, respectively, indicate poorer regulatory capacity, the link between surgency and regulatory capacity is unclear (Gartstein & Rothbart, 2003). Thus, hypotheses regarding the link of surgency and infant sleep development were withheld.
Other studies of temperament-sleep linkages have reported associations between high infant irritability and inhibition and frequent infant awakenings at night (Halpern et al., 1994), and between high infant negative mood and short sleep duration (Kelmanson, 2004; Weissbluth, 1981). These dimensions appear to map onto Rothbart’s temperament superfactor of Negative Affectivity, which incorporates infants’ sadness, fearfulness, withdrawal, easy frustration due to limitations, and difficulty in recovering from stress. Therefore, we expected that higher negative affectivity would predict decreased sleep length and sleep quality from 1 to 6 months. Finally, previous research has associated higher-quality infant/toddler sleep with higher infant persistence, adaptability, soothability, and rhythmicity, and lower infant distractibility (Kelmanson, 2004; Sadeh, Lavie, & Scher, 1994; Scher et al., 1992; Scher et al., 1998). These temperament factors correspond to Rothbart’s superfactor of Orienting/Regulation, which taps infants’ attention span, low-intensity pleasure, and soothability. Based on these findings and the hypothesis of overlapping regulatory systems of sleep, affect, and attention (Dahl, 1996), we expected that better orienting/regulation would predict increased sleep length and quality.
1.3. Temperament as a Potential Moderator in the Relation of Parenting and Infant Sleep
In addition to examining direct linkages between the emotional quality of bedtime parenting, infant temperament, and infant sleep, we were also interested in exploring infant temperament as a potential moderator of associations between parenting quality and infant sleep. Indeed, as a constitutionally based individual characteristic, temperament has been hypothesized to be a potential moderator of socialization experience (Rothbart & Bates, 2006). Children with different temperamental profiles may be sensitive to different types of parenting (Sanson & Rothbart, 1995). Two extant theoretical models that inform expectations about the moderating impact of infant temperament on parenting-infant sleep relations are the diathesis-stress model and the differential susceptibility model. The diathesis-stress model proposes that individuals with highly reactive temperamental profiles will be more vulnerable to negative environment than those with less reactive profiles (Monroe & Simons, 1991). The differential susceptibility hypothesis (Belsky & Pluess, 2009) expands upon the diathesis-stress hypothesis and proposes that temperamentally highly reactive individuals will not only be strongly and detrimentally affected by negative environmental influences but, for the same reason, be strongly and positively affected by favorable environmental influences. In terms of specific temperament factors, high negative affectivity has been identified by many studies as either a marker of vulnerability or plasticity in response to rearing influences (for review, see Belsky & Pluess, 2009). Other studies have shown that exuberance (similar to Rothbart’s superfactor of surgency) and effortful control (including attentional focusing and inhibitory control of behavior) can serve as moderators of parenting effects on child socioemotional development and behavior problems (for review, see Kiff, Lengua, and Zalewski (2011), and Rothbart and Bates (2006)).
Despite the wealth of studies demonstrating that child characteristics moderate the effect of parenting on child outcomes, there has been no study, to our best knowledge, examining the moderating role of infant temperament in the relation between parenting quality and infant sleep. Such a study is overdue. Infant sleep matures remarkably during the first half year of life; however, rates of sleep maturation are not uniform (Burnham et al., 2002; Henderson et al., 2011), which may be due to differences in parenting quality at bedtime, infant temperament, and their interactions. The current study thus examined temperament as a potential moderator of links between maternal EA at bedtime and objectively assessed infant sleep development from 1 to 6 months. Infant sleep at 1 month was controlled, and as a result, the study focused on residualized changes in infant sleep, which reflected how an infant’s sleep developed relative to group trends of sleep maturation. We did not specify a certain interaction pattern. The following pattern, if emerging, would be compatible with the diathesis-stress model: low maternal EA at bedtime would predict decreased sleep length and quality from 1 to 6 months only for infants with high negative affectivity or poor regulatory capacity, but would not predict sleep development for infants with low negative affectivity or good regulatory capacity. Another pattern, if emerging, would be compatible with the differential susceptibility hypothesis: compared with infants with low negative affectivity or good regulatory capacity, infants with high negative affectivity or poor regulatory capacity would develop longer and better sleep if their mothers showed high EA at bedtime, but they would develop shorter and poor sleep if their mothers showed low EA. Again, because of the ambiguous link between surgency and regulatory capacity, hypotheses concerning the potential moderating role of surgency were withheld.
2. Method
2.1. Participants
Data were drawn from a longitudinal study of parenting, infant sleep, and infant development, Project SIESTA II (Study of Infants’ Emergent Sleep TrAjectories II). The study has been approved by the institutional review board in the authors’ university. 167 families from central Pennsylvania were recruited through local hospitals when mothers were pregnant. Infants and both parents participated in the study when infants were one month old until 24 months.
All the families that had complete data on the Infant Behavior Questionnaire-Revised (IBQ-R, Gartstein, & Rothbart, 2003) and maternal EA at bedtime at both 3 and 6 months and infant sleep actigraphy at both 1 and 6 months were included in the current study, which resulted in a final sample of 72 families. We chose not to impute missing data, because we wished to base our findings on EA and infant sleep data that we actually observed, not imputed from covariates. Number of families that had data for key variables and demographics of the final sample are listed in Table 1. The final sample did not differ from the total sample in terms of key variables (including infant temperament, maternal EA, and infant sleep), infant gender, maternal age, number of children the mother has, mothers’ education, family income, or mothers’ depressive symptoms. However, mothers in the final sample were more likely to be European American (89% vs. 78%) and married and living with partner (89% vs. 75%), but less likely to be employed at 1 month (51% vs. 71%) compared with mothers in the total sample.
Table 1.
Number of families in the original sample that had data for key variables, and demographics of the final sample.
| Variable | |
|---|---|
|
Number of families in the original sample that had data for key variables Infants that had sleep actigraphy data at 1 months |
n = 154 |
| Infants that had sleep actigraphy data at 6 months | n = 143 |
| Families that had maternal EA data at 3 months | n = 106 |
| Families that had maternal EA data at 6 months | n = 105 |
| Infants that had temperament data at 3 months | n = 151 |
| Infants that had temperament data at 6 months | n = 149 |
| Demographics of the final sample (n = 72) | |
| Race | |
| European American | 89% |
| African American | 4% |
| Asian American | 3% |
| Latino American | 1% |
| Other | 3% |
| Mothers married and living with partner at 1 month | 87% |
| Mothers’ age | M = 29.5 (SD = 5.09) |
| Number of children the mother has | M = 1.89 (SD = .83) |
| Mothers with college education and above | 79% |
| Mothers employed at one month | 51% |
| Family annual income | M = $73,940 (SD = $55,546) |
2.2. Procedures
Families in the larger study were visited at home for three times during one full week when the children were 1, 3, 6, 9, 12, 18, and 24 months, while the current study used data of 1, 3, and 6 months. Bedtime parenting videos were usually taken on the first night of each week.
2.3. Measures and coding
Demographic data
When infants were 1 month, parents filled out demographic questionnaires which collected information on the infant’s day of birth, gender, parental age, education, employment, family annual income, ethnicity, number of siblings, etc.
Infant sleep
Infants wore the Mini-Mitter Actigraphy wristwatches (Model AW-64) on their calves throughout the home visit week. This device recorded infants’ physical activity level, from which information on infant sleep and awakenings was derived. After the visit, the recordings from Actigraphy were downloaded onto the project computer and read by the software Actiware version 5.59. Summary scores of infant sleep were calculated by averaging data across the seven days in order to provide more reliable data than single-day data. Three sleep variables were used in current analysis to reflect two distinct characteristics of sleep: quantity and quality (Pilcher, Ginter, & Sadowsky, 1997): average infant nocturnal sleep minutes (total duration of infant sleep subtracted by infant awake minutes between sleep onset and final wakeup) was the indicator for sleep quantity, while average wake minutes (total duration of waking time between sleep onset and final wakeup) and average sleep efficiency (identical to percent of sleeping time between sleep onset and final wakeup) were indicators for sleep quality.
Infant temperament
Temperament at 3 and 6 months was measured by mothers’ report on the revised version of the Infant Behavior Questionnaire (IBQ-R, Gartstein & Rothbart, 2003), one of the mostly widely used measurement of infant temperament. IBQ-R is a 191-item, comprehensive measure of infant temperament designed for use among infants under 12 months. It yields three broad-band factors of Positive Emotionality/Surgency, Negative Affectivity, and Orienting/Regulation. The three superfactors were used as summary scores, calculated by averaging scores of primary loading scales (Gartstein & Rothbart, 2003). The superfactor Negative Affectivity was the average score of subscales of Sadness, Distress to Limitations, Fear, and reverse-scored Rate of Recovery (α = .68 at 3 months and .62 at 6 months). The superfactor Positive Emotionality/Surgency was the average of subscales of Approach, Vocal Reactivity, High Intensity Pleasure, Smiling and Laughter, Activity Level, and Perceptual Sensitivity (αs = .81 at both 3 and 6 months). The superfactor Orienting/Regulation was the average of subscales of Low Intensity Pleasure, Cuddliness/Affiliation, Duration of Orienting, and Soothability (α = .58 at 3 months and .60 at 6 months). IBQ-R has established good internal consistency and inter-parent agreement, as well as convergent validity with behavioral measurements of temperament (Gartstein & Rothbart, 2003; Parade, & Leerkes, 2008).
Maternal Emotional Availability (EA)
Video and audio equipment was set up in participating families’ homes where bedtime and infant sleep usually took place. A Bosch Divar XF 8-Channel Digital Versatile Recorder was used for video and audio recording, infrared security cameras by ARM Electronics (Model No. C420BCVFIR) for video information collecting, and Channel Vision microphones (Model No. 5104-MIC) for audio information collecting. In most homes, two to four cameras were set up to capture the parent-infant interaction during bedtime and nighttime. At least one camera was set up above the infant’s crib or bed where infant sleep took place. Other cameras were usually set up to capture the infant’s changing table, the chair where parents fed the infant, or an overview of the infant’s room, depending on parent-reported locations of bedtime and nighttime. Parents were instructed to turn on the camera about one hour before bedtime began and turn off the camera after the infant woke up in the morning to ensure complete recordings of bedtime and nighttime infant activities.
Videotaped parent-infant interactions at bedtime that lasted for at least two minutes were coded for maternal EA (coders considered shorter videos too brief to provide sufficient information about EA), using the Emotional Availability Scales (EAS; Biringen, Robinson, & Emde, 1998). Parental EA included four subscales: sensitivity (parent’s capacity to be aware of, interpret accurately, and give temporally contingent and appropriate responses to the child’s signals, which was derived from the conceptualization of parenting sensitivity by Ainsworth and colleagues (1974)), structuring (parent’s capacity to support and scaffold the child’s activities while following the child’s needs), non-intrusiveness (parent’s capacity to not restrict or interfere with the child’s exploration of the environment during the interaction), and non-hostility (parent’s capacity to interact with the child patiently and peacefully, without anger or irritation). Child EA (responsiveness and involvement) were not used in current analysis, because the behavioral repertoire of infants between 3 to 6 months is too limited to reliably code EA from.
The current study utilized the EA coding system which has been adapted to the bedtime context in the pilot study (Teti et al., 2010). Maternal sensitivity was rated high when the mother detected immediately, interpreted accurately, and responded promptly and appropriately to the infant’s signals by fulfilling the infant’s needs such as feeding, soothing, and diaper changing, but it was rated low when mothers did not respond to the infant’s signals quickly, did not understand what the infant wanted, or her response did not reduce the infant’s stress for a long time. Maternal structuring was rated high when the mother engaged the infant in bedtime routines in a quiet, soothing, and organized manner that gently induced the infant to sleep, but it was rated low when the infant’s bedtime was interrupted by activities unrelated to them or when they were left unattended for a long time. Maternal non-intrusiveness was rated high when the mother did not initiate arousing activities with the baby or other family members such as tossing baby in the air or yelling/talking loudly to the baby or family members, or did not insist that the baby fall asleep when the baby was not ready. Maternal non-hostility was rated high when the mother did not display covert or overt impatience, frustration, or anger during the bedtime.
The main coder and the principal investigator of the larger study were trained and certified on the EAS (3rd edition; Biringen et al., 1998). The interrater reliability (intraclass correlations for absolute agreement) for maternal sensitivity, structuring, non-intrusiveness, and non-hostility at bedtime at 3 and 6 months ranged from .87 to .99, based on 10% of the sample.
2.4. Data Analytic Plan
A series of hierarchical multiple regressions were carried out to predict infant sleep development from 1 to 6 months, using infant temperament, maternal EA at bedtime, and their interactions as predictors. Because temperament superfactors were highly correlated between 3 and 6 months (see Table 3), they were standardized and then averaged across the two time points to create reliable indicators of temperament. Maternal EA at bedtime were sum scores of standardized values of its four subscales, i.e., sensitivity, structuring, non-intrusiveness, and non-hostility. Based on the same reason for creating composite temperament scores, maternal EA at 3 and 6 months were standardized respectively and then averaged. These composite 3-and-6-month temperament scores and EA scores were then standardized and multiplied to create interaction terms of temperament and EA. One-month sleep variables corresponding to 6-month sleep outcomes were used as control variables. Infant gender was also controlled, partly because gender difference emerged in prior work in terms of infant sleep state transitions and sleep efficiency (Scher et al., 2004), and also because gender difference emerged in the current sample in terms of infant sleep minutes, wake minutes, and sleep efficiency (see 1st row in Table 3).
Table 3.
Pearson correlations between infant gender, infant temperament, maternal emotional availability at bedtime, and infant sleep.
| Variable | Month | Infants’ age (months)
|
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgency | Negative Affectivity | Orientating/Regulation | Emotion Availability | Sleep minutes | Wake minutes | Sleep efficiency | |||||||||
|
| |||||||||||||||
| 3 | 6 | 3 | 6 | 3 | 6 | 3 | 6 | 1 | 6 | 1 | 6 | 1 | 6 | ||
| Gender | .16 | .20 | .05 | −.05 | .09 | .13 | −.19 | −.01 | .01 | .32** | .16 | −.27* | −.12 | .32** | |
| Surgency | 3 | – | .85*** | .11 | .15 | .64*** | .54*** | −.41*** | −.28* | −.34** | −.09 | .22† | −.06 | −.29* | .01 |
| 6 | – | −.05 | .09 | .59*** | .68*** | −.47*** | −.28* | −.19 | .05 | .08 | −.17 | −.13 | .14 | ||
| Negative Affectivity | 3 | – | .66*** | −.19 | −.17 | −.10 | −.07 | .02 | −.02 | .05 | −.03 | −.03 | .06 | ||
| 6 | – | −.09 | −.34** | −.21† | −.24* | −.10 | −.16 | .03 | .20† | −.05 | −.20† | ||||
| Orientating/Regulation | 3 | – | .61*** | −.02 | .01 | −.17 | .10 | .07 | −.04 | −.13 | .03 | ||||
| 6 | – | −.20† | −.08 | −.09 | .14 | −.03 | −.17 | −.02 | .16 | ||||||
| Emotion Availability | 3 | – | .63*** | .06 | .15 | −.16 | .11 | .11 | −.06 | ||||||
| 6 | – | −.13 | .13 | .01 | .01 | −.09 | .03 | ||||||||
| Sleep minutes | 1 | – | .37** | −.57*** | −.18 | .81*** | .25* | ||||||||
| 6 | – | −.11 | −.51*** | −.21 | .70*** | ||||||||||
| Wake minutes | 1 | – | .12 | −.94** | −.12 | ||||||||||
| 6 | – | −.14 | −.96** | ||||||||||||
| Sleep efficiency | 1 | – | .16 | ||||||||||||
| 6 | – | ||||||||||||||
Note. For infant gender, 1 = male, 2 = female.
p < .10.
p < .05.
p < .01.
p < .001.
In each regression, infant gender and the 1-month sleep variable were entered at step 1; maternal EA at bedtime and one of the three temperament superfactors were entered at step 2; the interaction of this temperament superfactor and EA was entered at step 3. Therefore for each sleep outcome, a set of three regressions was tested. If a superfactor or its interaction with EA emerged as a significant predictor, in order to fathom which specific temperament dimension underlying the superfactor was relevant, all of the sub-dimensions were subject to individual regressions, in which the superfactor was replaced with the one of its sub-dimensions.
Because some IBQ-R items inquire about infant sleep, four subscales of the IBQ containing sleep-related items—Activity Level, Distress to Limit, Rate of Recovery, and Sadness—and the two superfactors to which they contributed—Surgency and Negative Affectivity, were re-computed without these sleep items. Multiple regressions were then conducted using these recalculated scales. Results reported below were obtained using these “purified” temperament measures, unless otherwise specified.
3. Results
3.1. Preliminary Analyses
The descriptives for study variables are listed in Table 2. Repeated measures analysis of variance showed that all the infant sleep variables changed significantly over time, according to multivariate test’s Wilk’s Lamda and univariate tests of within-subject effects. Post-hoc (Bonferroni) comparisons showed that, for the current sample, infant sleep minutes significantly lengthened from 1 to 3 months (p < .05), with an average increase of 20.63 minutes, and from 3 to 6 months (p < .001), with an average increase of 80.60 minutes; wake minutes were similar between 1 to 3 months but decreased significantly from 3 to 6 months (p < .001), with an average decrease of 46.97 minutes; sleep efficiency remained unchanged between 1 and 3 months but increased significantly from 3 to 6 months (p < .001), with an average increase of 9.17 percent.
Table 2.
Means and standard deviations for infant sleep, maternal emotional availability at bedtime, and infant temperament, and repeated measures ANOVA (including post-hoc (Bonferroni) comparisonsa) of infant sleep from 1 to 6 months.
| Infants’ age (months)
|
Wilk’s Lamda | Within-subjects effects | |||
|---|---|---|---|---|---|
| 1 | 3 | 6 | |||
|
| |||||
| Variable |
M (SD) |
M (SD) |
M (SD) |
F(2, 67) | Fb |
| Sleep minutes | 389.411 (82.02) |
410.042 (65.82) |
490.643 (65.41) |
68.16*** | 71.46*** |
| Wake minutes | 171.151 (59.36) |
170.751 (48.09) |
123.782 (41.14) |
35.56*** | 28.01*** |
| Sleep efficiency | 69.151 (10.60) |
70.551 (7.69) |
79.722 (6.45) |
58.79*** | 44.23*** |
| Surgency | 3.97 (.85) |
4.83 (.69) |
|||
| Negative Affectivity | 2.76 (.48) |
2.98 (.59) |
|||
| Orientating/Regulation | 4.95 (.54) |
5.05 (.51) |
|||
| Emotion Availabilityc | |||||
| Sensitivity | 6.45 (1.40) |
6.22 (1.50) |
|||
| Structuring | 3.70 (.64) |
3.63 (.80) |
|||
| Non-intrusiveness | 4.74 (.53) |
4.78 (.43) |
|||
| Non-hostility | 4.74 (.74) |
4.71 (.63) |
|||
The post-hoc comparison results were indicated by superscripts of the means. Same number denote an insignificant difference and different numbers denote a significant difference.
Sleep minutes did not violate the assumption of sphericity, so the F of within-subjects effects was calculated under the sphericity-assumed condition. Wake minutes and sleep efficiency violated the assumption of sphericity, so the Fs were calculated with the Greenhouse-Geisser correction.
Since emotional availability is the average score of its standardized subscales, its mean is close to 0, and standard deviation, close to 1, both of which have little interpretative value. Therefore the means and standard deviations of EA are not listed.
p < .05.
p < .01.
p < .001.
Zero-order Pearson correlations (Table 3) showed that three superfactors of infant temperament displayed strong to very strong stability from 3 to 6 months (rs = .61 ~. 85, ps < .005), and so did maternal EA at bedtime (r = .63, p < .005). Therefore infant temperament and maternal EA at bedtime were averaged across 3 and 6 months respectively, and the resulting composite scores were used as predictors in later regression analysis. Infant sleep minutes were modestly correlated between 1 month and 6 months (r = .37, p < .01), while wake minutes and sleep efficiency did not show significant stability across time (r = .12, r = .16, ns). In terms of correlations between control variables, predictors, and outcome variables, infant gender (1 = male, 2 = female) modestly correlated with 6-month infant sleep variables (r = .32 for sleep minutes, r = −.27 for wake minutes, r = .32 for sleep efficiency, ps < .05), indicating that female infants tended to spend more time sleeping, less time waking, and sleep more efficiently (i.e., have higher percent of sleeping time between sleep onset and final wakeup) at 6 months than did male infants. Infant temperament factors were not significantly correlated with infant sleep at 6 months, but higher 3-month surgency was correlated with shorter 1-month sleep minutes (r = −.34, p < .01) and lower 1-month sleep efficiency (r = −.29, p < .05). Maternal EA at bedtime was not correlated with infant sleep variables.
3.2. Hierarchical multiple regression analyses
Hierarchical multiple regression analyses were conducted to test the hypotheses regarding main effects and interactive effects of maternal EA at bedtime and infant temperament on developmental changes of infant sleep from 1 to 6 months. In step 1, gender explained significant portions of variance in sleep development. Specifically, female infants tended to develop longer sleep minutes (βs = .29 ~ .31, ps < .01), shorter waking minutes (βs = −.30 ~ .28, ps < .05), and higher sleep efficiency (β = .34 ~ .35, ps < .01) than did male infants from 1 to 6 months. One-month sleep minutes positively predicted 6-month sleep minutes (βs = .37 ~ .43, ps < .001), whereas 1-month wake minutes and sleep efficiency did not, or only marginally predicted 6-month wake minutes and sleep efficiency, respectively. The significance pattern of these control variables remained the same after maternal EA at bedtime, temperament superfactors, and their interaction terms were entered in the regressions in later steps.
3.2.1. The effect of maternal EA at bedtime on the development of sleep quantity and quality from 1 to 6 months
Before interaction terms were entered into regressions, higher 3-and-6-month bedtime maternal EA composite scores significantly or marginally predicted increases in infant sleep minutes from 1 to 6 months (βs = .20 ~ .26, ps = .03 ~ .08; coefficients varied depending on the temperament factor included in the regression), above and beyond the influences of infant sleep baseline levels, gender, and temperament. After interaction terms were entered into the regressions, higher maternal EA at bedtime remained a significant (β = .21, p < .05) or marginally significant (β = .21, p = .06) predictor of increase in infant sleep minutes in the regression with temperament dimensions of orienting/regulation and negative affectivity, but with not surgency. This suggests that higher emotional availability of mothers at bedtime predicted greater increase in sleep minutes (quantity) for their babies from 1 to 6 months. However, maternal EA at bedtime was not predictive of changes in infant wake minutes or sleep efficiency before or after the interaction terms were added, and therefore the hypothesis that maternal EA would predict increased sleep quality was not supported.
3.2.2. The effect of infant temperament on sleep development from 1 to 6 months
Contrary to the hypothesis, 3-and-6-month infant temperament superfactors did not predict developmental changes in infant sleep minutes, wake minutes, or sleep efficiency from 1 to 6 months, either before or after the interaction term was entered in the regression.
3.2.3. The moderating effect of infant temperament in the links between bedtime maternal EA and developmental changes of infant sleep
Multiple regression analysis showed that the interaction between maternal EA at bedtime and surgency significantly predicted developmental changes of infant sleep minutes from 1 to 6 months (β = .38, p < .05; see Table 4), but not wake minutes or sleep efficiency. Adding the interaction term in the regressions rendered maternal EA at bedtime to be no longer a significant predictor of changes in infant sleep minutes.
Table 4.
Regressions With Significant Interaction Terms Predicting 6-Month Infant Sleep Minutes, Using Averaged 3-And-6-Month Infant Temperament, Maternal Bedtime Emotional Availability at Bedtime, and Their Interactions as Predictors.
| Step and Predictors | Sleep minutes Overall F(5,66) = 6.21***
|
Step and Predictors | Sleep minutes Overall F(9,61) = 4.20***
|
Step and Predictors | Sleep minutes Overall F(9,61) = 4.20***
|
||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | R2 | ΔF | β | R2 | ΔF | β | R2 | ΔF | |||
| Step 1 | .22 | 9.90*** | Step 1 | .20 | 9.90*** | Step 1 | .20 | 9.90*** | |||
| Gender | .29** | Gender | .29** | Gender | .29** | ||||||
| 1mo sleep | .38*** | 1mo sleep | .38*** | 1mo sleep | .38*** | ||||||
| Step 2 | .28 | 2.45† | Step 2 | .22 | 1.88 | Step 2 | .22 | 1.97 | |||
| Gender | .30** | Gender | .30** | Gender | .31** | ||||||
| 1mo sleep | .42*** | 1mo sleep | .40*** | 1mo sleep | .40*** | ||||||
| EA | .26* | EA | .22† | EA | .23† | ||||||
| Surgency | .14 | Smile & laughter | .06 | Vocal reactivity | .08 | ||||||
| Step 3 | .32 | 4.43* | Step 3 | .28 | 6.15* | Step 3 | .32 | 5.18* | |||
| Gender | .30** | Gender | .30** | Gender | .32** | ||||||
| 1mo sleep | .43*** | 1mo sleep | .41*** | 1mo sleep | .42*** | ||||||
| EA | .15 | EA | .09 | EA | .11 | ||||||
| Surgency | .13 | Smile & laughter | .02 | Vocal reactivity | .05 | ||||||
| EA×Surgency | .24* | EA×Smile & laughter | .28* | EA×Vocal reactivity | .26* | ||||||
Note. n = 72. For infant gender, 1 = male, 2 = female. 1mo sleep = infant sleep minutes at one month. EA = maternal emotional availability at bedtime.
p < .10.
p < .05.
p < .01.
p < .001.
Simple slope tests (Aiken & West, 1991) were conducted to follow up on this interaction. For infants with high levels of surgency (1 standard deviation above the mean), higher maternal EA at bedtime predicted greater increase in sleep minutes (B = 22.47, t(66) = 2.85, p < .01), which means that for highly surgent infants, one standard deviation improvement in maternal EA at bedtime predicted an increase of 22.47 minutes in infants’ actual sleep time from 1 to 6 months. However, for infants with low levels of surgency (1 SD below the mean), maternal EA did not influence the change in sleep minutes (B = −3.03, t(66) = −.25, ns) (see Figure 1). Post-hoc comparisons of endpoint values of the regression lines (indicating the sleep minutes for infants who were ±1 SD on surgency scores and whose mothers were ±1 SD on EA scores, as denoted by point A, B, C, D in Figure 1) revealed that, with mothers who were highly emotionally available at bedtime, infants with higher levels of surgency (point A) increased more in number of minutes asleep from 1 to 6 months compared with infants with lower levels of surgency (point B); however, with mothers who were less emotionally available at bedtime, change in sleep minutes did not differ between infants with high or low level of surgency (point C and point D). In other words, infants with +1 SD surgency and receiving +1 SD maternal EA at bedtime (point A) increased more in number of minutes asleep from 1 to 6 months than the three other groups of infants (those with +1 SD surgency and −1 SD EA, those with −1 SD surgency and +1 SD EA, and those with −1 SD surgency and −1 SD EA). Therefore only highly surgent infants benefited from highly emotionally available maternal care at bedtime in terms of increasing sleep length.
Figure 1.
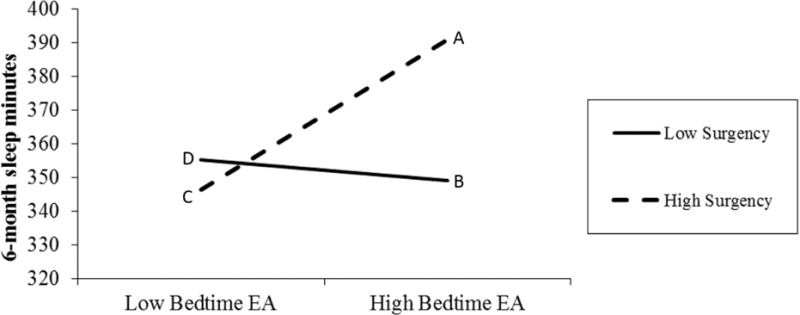
Predicting 6-month infant sleep minutes after controlling for 1-month sleep minutes and gender: simple slopes for interaction of maternal EA at bedtime and infant surgency (sleep-related items were excluded from the Surgency measure).
Additional analysis of sub-dimensions underlying the surgency superfactor showed that Vocal Reactivity and Smile and Laughter contributed to the moderating effect of surgency in the link between maternal EA at bedtime and changes in sleep minutes (β = .26, p < .05; β = .28, p < .05) (see Table 4). Simple slope analysis (see Figure 2) indicated that, for infants who were more likely to vocalize or to smile and laugh, their mothers’ EA at bedtime positively predicted increases in minutes asleep from 1 to 6 months (B = 21.40, t(66) = 2.76, p < .01; B = 23.70, t(66) = 2.96, p < .01), which means that, for these infants, one standard deviation improvement in maternal EA would predict an increase of 21.4 or 23.7 minutes in their sleep time from 1 to 6 months. However, for infants who were less vocally reactive or less likely to smile and laugh, maternal EA at bedtime did not significantly predict changes in minutes asleep from 1 to 6 months (B = −7.23, t(66) = −.60, ns; B = −12.47, t(66) = −.98, ns). Post-hoc comparisons of endpoint values of the regression lines indicated that, with mothers who were highly emotionally available at bedtime, infants with higher levels of vocal reactivity or smile and laughter marginally or significantly increased the number of minutes asleep from 1 to 6 months more than infants with lower levels of these traits (B = 17.55, t(66) = 1.88, p = .07; B = 19.08, t(66) = 2.04, p < .05). In summary, infants with +1 SD vocal reactivity or smile and laughter and receiving +1 SD emotionally available parenting at bedtime significantly increased the amount of sleep time across the first six months more than other infants.
Figure 2.
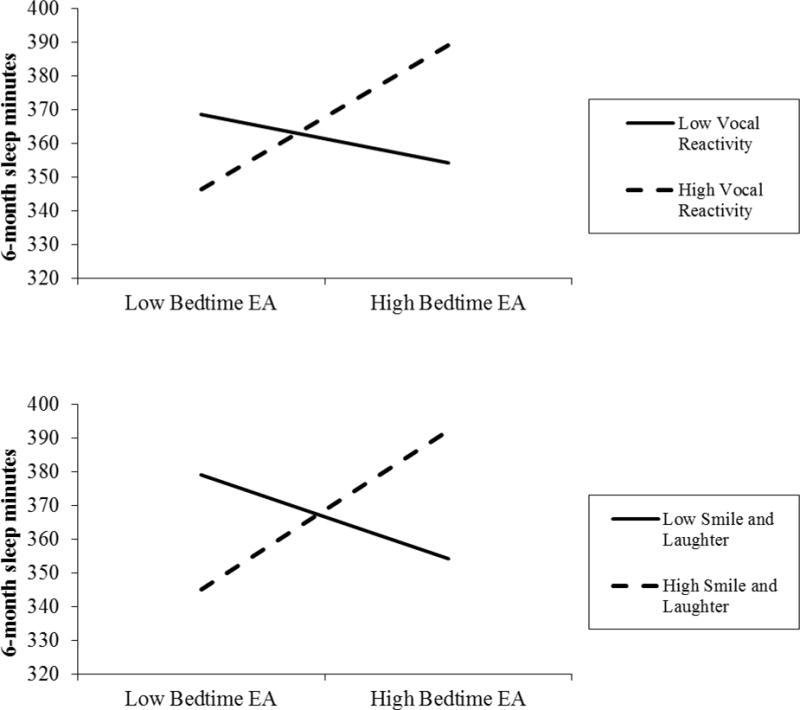
Predicting 6-month infant sleep minutes after controlling for 1-month sleep minutes and gender: simple slopes for interaction of maternal EA at bedtime and infant Vocal Reactivity, and interaction of maternal EA at bedtime and infant Smile and Laughter.
4. Discussion
The current study is among the first to examine whether observed maternal emotional availability at bedtime and infant temperament predicted, either additively or multiplicatively, objectively assessed infant sleep development across the first six months of life. Our study found little evidence for the impact of infant temperament alone on sleep development, some support for the main effects of 3-and-6-month maternal EA at bedtime on increased infant sleep minutes, but compelling evidence that the influence of maternal EA at bedtime on increased infant sleep minutes was moderated by infant temperament, in particular surgency. These results are consistent with the transactional model of infant sleep (Sadeh & Anders, 1993; Sadeh et al., 2010), which posits that infant sleep is ecologically based and multiply and complexly determined by both environmental and individual, constitutional factors.
4.1. Main effects of maternal emotional availability at bedtime
In the interests of parsimony (Bates, 1989), we address the additive effects of parenting and temperament before turning to the moderating effects of infant surgency. Regression analysis revealed that higher maternal EA at bedtime significantly or marginally significantly predicted larger increases in infant sleep minutes from 1 to 6 months. This finding, along with previously established linkages between higher maternal EA at bedtime and mothers’ report of better infant sleep quality (Teti et al., 2010), underscores the beneficial impact of emotionally available parenting at bedtime on infant sleep development. At least two differences between the present study and Teti et al. (2010) are worth noting. First, the current study used actigraphy to record infant sleep, whereas Teti et al. (2010) used maternally reported daily diary accounts of infant sleep. Second, the current study focused on developmental changes in infant sleep during the first half year of infants’ life, whereas Teti et al. (2010) examined concurrent associations between maternal EA and infant sleep among infants ranging from 1 to 24 months old. In spite of these differences, the results of the present study and of Teti et al. (2010) indicate that emotionally available parenting at bedtime may promote longer and better infant sleep during the night.
4.2. Main effects of infant temperament
The current study did not find predictive associations between early temperament dimensions and later sleep variables, but instead showed correlational associations between infant sleep quantity (number of minutes infants slept) and quality (sleep efficiency) at 1 month and lower levels of surgency at 3 months. These correlations, however, should be interpreted with caution, because infant temperament could not be reliably assessed before 3 months, and thus we were unable to examine concurrent relations between infant sleep and temperament at 1 month. Regression analyses revealed that infant temperament superfactors did not predict developmental changes of infant sleep quantity or quality from 1 to 6 months. This null finding of direct associations between infant temperament and infant sleep, however, is not necessarily incompatible with past literature, because although some patterns of associations between infant temperament and infant sleep have emerged, they tend to be modest and inconsistent across studies (Halpern et al., 1994; Scher et al., 1998).
4.3. Infant temperament as a moderator
For the most part, previous studies have investigated the contribution of parenting (e.g., Scher, 2001; Teti et al., 2010) and infant temperament (e.g., Halpern et al., 1994; Sadeh et al., 1994; Scher et al., 1992; Scher et al., 1998; Spruyt et al., 2008) on infant/child sleep either separately or additively, but not multiplicatively. This “main-effect” approach precludes opportunity to identify potentially more complex, transactional relations between parenting, temperament, and infant sleep, which would be more consistent with the transactional model of development (Sameroff, 1989) and the transactional model of child sleep (Sadeh & Anders, 1993; Sadeh et al., 2010). The present study was an attempt to redress this issue, following the proposition that individuals with different temperamental profiles would be differentially sensitive to parenting (Sanson & Rothbart, 1995) and making use of extant theoretical models (diathesis-stress and differential susceptibility) to develop hypotheses about the potential role of infant temperament in moderating the impact of bedtime parenting quality on infant sleep development.
Analyses revealed no moderating effect of negative affectivity or orienting/regulation on the relation between maternal EA at bedtime and infant sleep development. Thus, there was no support for either the diathesis-stress model or the differential susceptibility model of parenting-temperament interaction. However, a moderating effect of infant surgency on the link between bedtime EA and infant sleep length was obtained, such that highly surgent infants were more responsive to the positive effects of maternal EA at bedtime than were infants low in surgency. Specifically, when their mothers were highly emotionally available at bedtime, infants high in surgency showed greater increases in sleep minutes from 1 to 6 months than infants low in surgency, even after controlling for 1-month sleep minutes.
In trying to understand this moderation effect, we first note that high levels of positive emotionality/surgency does not equate with poor regulation. In the present study, surgency correlated highly and positively with orientating/regulation (rs = .64 ~ .68, ps < .001, see Table 3), which is compatible with prior work that found their positive association in infancy and toddlerhood (Gartstein & Rothbart, 2003; Putnam, Rothbart, & Gartstein, 2008). Second, young children’s positive emotions expressed in naturalistic parent-child interactions may be different from approach and novelty seeking behavior elicited by novel stimuli, in that the former may indicate the individual’s tendency of affiliation and warmth, which was found predictive of better rather than worse self-regulation (Kochanska, Aksan, Penney, & Doobay, 2007). Thus, vocal reactivity and smile and laughter, the two significant sub-dimensions of surgency that emerged in our moderation analysis, may reflect positivity in interpersonal interactions, and may not be strongly connected with the approach system based on the content of IBQ-R items. Therefore, the significant moderating effect of surgency in the present study may be explained by the fact that infants high in surgency are more expressive and warm in interpersonal interactions than are infants low in surgency, and thus they reap the positive influence of maternal EA at bedtime, probably through developing feelings of security and trust in their sleep environment, which are conducive to developing longer sleep. Other dimensions of surgency such as activity and approach may not be clearly manifest in infants under 6 months of age, and therefore may not have a salient impact on the bedtime parent-child transactional system until much later in development.
It remains unclear why infant negative affectivity or regulatory capacity did not moderate maternal EA’s effect on infant sleep development, especially since the former has been often identified as a vulnerability or plasticity factor of environmental influences (Belsky & Pluess, 2009). The reason may be related to the developmental phase that was investigated in the present study. It is possible that negative affectivity or orienting/regulation may function as a salient moderator of EA – infant sleep relations at later points in development. Indeed, many studies that found associations between infant temperament and infant sleep measured temperament after 6 months of age (Atkinson et al., 1995; Novosad, Freudigman, & Thoman, 1999; Scher et al., 1992; Sadeh et al., 1994; Scher et al., 1998).
4.4. Strengths and Limitations
Compared to prior work, the present study had several methodological strengths that are worth noting. While most past research only examined first-order correlations between parenting, infant temperament, and infant sleep (e.g., Sadeh et al., 1994; Scher et al., 1992; Scher et al., 1998; Spruyt et al., 2008), the current study investigated parenting and temperament in relation to developmental changes of infant sleep. One-month sleep variables were controlled, allowing the regression analysis to target on predicting residualized changes in infant sleep. We also assessed predictors and outcomes using different sources of information (infant sleep was measured by actigraphy, maternal EA was blindly rated by coders, and infant temperament was reported by mothers), which reduced shared method variance (Podsakoff, MacKenzie, Lee, & Podsakoff, 2003). Moreover, in order to eliminate the potential bias in results caused by the common variance shared between sleep-related temperament items and infant sleep measures, sleep items were dropped from IBQ-R, and regression analyses were conducted again based on “sleep-free” temperament measures.
The present study also had several limitations. Although recruitment efforts were made to oversample participants from ethnic minority groups and diverse SES backgrounds, the current sample was predominantly white and reasonably well-educated. Thus, the generalizability of the present results to populations with higher socioeconomic risk remains unclear. The final study sample (n = 72) was also relatively small, which may have excluded more sophisticated analytical approaches, such as structural equation modeling, and restrained the power of the analysis. For instance, in some regressions maternal EA showed a marginally significant effect, which could be better detected using a larger sample size. However, given the nature of intense longitudinal measures and the use of multiple sources of measures (observation, actigraphy, and parent-report), the current sample size is still considerable and already improved over many previous studies with actigraphy measure of infant sleep (e.g., Halpern et al., 1994; Scher et al., 1992; Scher et al., 1998; Spruyt et al., 2008).
Furthermore, our study examined only 1 to 6 months of infants’ life, so it remains unknown what pattern would emerge between maternal EA, infant temperament, and infant sleep in later phases of development. Recent studies suggest that the influence of shared environment on infant nighttime sleep may increase from 6 to 18 months (Touchette et al., 2013) and become a predominant predictor of infant sleep pattern compared with genetic influence (Brescianini et al., 2011; Fisher et al., 2012). Therefore, it is reasonable to hypothesize that the effect of maternal EA or its interaction with infant temperament on infant sleep becomes more prominent as children grow up. Future research can benefit from using a larger sample which is more diverse in terms of ethnic and socioeconomic background, and testing developmental stages beyond the first six months of infants’ life.
From a family system perspective, the dyadic interactions between mothers and fathers, fathers and infants, as well as triadic interactions between mothers, fathers, and infants, constitute indispensable aspects of bedtime interactions, but they were not examined in the present study. Unfortunately, although there were fathers taking care of infants at bedtime in our sample, data on paternal EA and coparenting at bedtime were too small to be included in the current analysis. New insights on the ecology of infant sleep can be generated by expanding the context of parenting to include both bedtime and nighttime, and by incorporating fathers and other bedtime and nighttime caregivers (e.g., grandparents) into the research framework.
The current study is among the first to examine the complex, transactional relations between parenting emotional quality at bedtime, infant temperament, and developmental changes of infant sleep, by exploring the moderating role of temperament in the relation between EA and infant sleep development. Results support the transactional model of infant sleep (Sadeh & Anders, 1993; Sadeh et al., 2010), which posits that infant sleep develops in dynamic and complex transactions between infant characteristics and parenting. The present findings are limited, however, to infant sleep development across the first 6 months of life, and to a population that is predominantly white and middle-class. Future studies on infant sleep should examine additive and multiplicative contributions of parenting and temperament at later points in infancy and in more diverse samples, taking into consideration other domains of parenting (e.g., specific parenting practices) and other dimensions of family ecology (e.g., father involvement and coparenting).
Highlights.
Maternal emotional availability (EA) was coded from videos of naturalistic mother-infant interactions at bedtime.
Maternal EA positively predicted developmental changes of infant sleep time from 1 to 6 months.
Infant surgency moderated the effect of maternal EA on infant sleep time.
Acknowledgments
This study was supported by an NIH grant (R01-HD052809), which was awarded to the second author. We thank the many members of the SIESTA team for contributing to this project, Kristin Buss for her comments on earlier drafts of this paper, and the parents and infants who participated in this study.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury, CA: Sage; 1991. [Google Scholar]
- Ainsworth MDS, Bell SM, Stayton D. Infant-mother attachment and social development. In: Richards MP, editor. The introduction of the child into a social world. London: Cambridge University Press; 1974. pp. 99–135. [Google Scholar]
- Anders TF, Keener M. Developmental course of nighttime sleep-wake patterns in full-term and premature infants during the first year of life: I. Sleep: Journal of Sleep Research & Sleep Medicine. 1985;8:173–192. doi: 10.1093/sleep/8.3.173. [DOI] [PubMed] [Google Scholar]
- Anders TF, Keener M, Bower TR, Shoaff BA. A longitudinal study of nighttime sleep-wake patterns in infants from birth to one year. In: Call JO, Galenson E, Tyson RL, editors. Frontiers of infant psychiatry. New York: Basic Books; 1983. pp. 150–170. [Google Scholar]
- Ando J, Nonaka K, Ozaki K, Sato N, Fujisawa KK, Suzuki K, Ooki S. The Tokyo twin cohort project: Overview and initial findings. Twin Research and Human Genetics. 2006;9(06):817–826. doi: 10.1375/183242706779462480. [DOI] [PubMed] [Google Scholar]
- Atkinson E, Vetere A, Grayson K. Sleep disruption in young children. The influence of temperament on the sleep patterns of pre-school children. Child: care, health and development. 1995;21(4):233–246. doi: 10.1111/j.1365-2214.1995.tb00754.x. [DOI] [PubMed] [Google Scholar]
- Bates JE. Applications of temperament concepts. In: Kohnstamm GA, Bates JE, Rothbart MK, editors. Temperament in childhood. Chichester, England: Wiley; 1989. pp. 321–355. [Google Scholar]
- Belsky J, Pluess M. Beyond diathesis stress: Differential susceptibility to environmental influences. Psychological Bulletin. 2009;135:885–908. doi: 10.1037/a0017376. [DOI] [PubMed] [Google Scholar]
- Biringen Z. Emotional availability: Conceptualization and research findings. American Journal of Orthopsychiatry. 2000;70(1):104–114. doi: 10.1037/h0087711. [DOI] [PubMed] [Google Scholar]
- Biringen Z, Robinson J, Emde RN. Emotional availability scales. 3rd. Fort Collins: Department of Human Development and Family Studies, Colorado State University; 1998. [Google Scholar]
- Brescianini S, Volzone A, Fagnani C, Patriarca V, Grimaldi V, Lanni R, Stazi MA. Genetic and environmental factors shape infant sleep patterns: a study of 18-month-old twins. Pediatrics. 2011;127(5):1296–1302. doi: 10.1542/peds.2010-0858d. [DOI] [PubMed] [Google Scholar]
- Burnham MM, Goodlin-Jones BL, Gaylor EE, Anders TF. Nighttime sleep-wake patterns and self-soothing from birth to one year of age: a longitudinal intervention study. Journal of Child Psychology and Psychiatry. 2002;43(6):713–725. doi: 10.1111/1469-7610.00076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss AH, Plomin H. Temperament: Early developing personality traits. Hillsdale, NJ: Erlbaum; 1984. [Google Scholar]
- Carey WB. Night waking and temperament in infancy. The Journal of pediatrics. 1974;84(5):756–758. doi: 10.1016/S0022-3476(74)80027-2. [DOI] [PubMed] [Google Scholar]
- Chess S, Thomas A. Origins and evolution of behavior disorders. New York: Bruner/Mazel; 1984. [Google Scholar]
- Dahl RE. The regulation of sleep and arousal: Development and psychopathology. Development and Psychopathology. 1996;8:3–28. doi: 10.1017/S0954579400006945. [DOI] [Google Scholar]
- Easterbrooks M, Bureau JF, Lyons-Ruth K. Developmental correlates and predictors of emotional availability in mother–child interaction: A longitudinal study from infancy to middle childhood. Development and psychopathology. 2012;24(1):65–78. doi: 10.1017/S0954579411000666. [DOI] [PubMed] [Google Scholar]
- Fisher A, van Jaarsveld CH, Llewellyn CH, Wardle J. Genetic and environmental influences on infant sleep. Pediatrics. 2012:1091–1096. doi: 10.1542/peds.2011-1571. [DOI] [PubMed] [Google Scholar]
- Gartstein MA, Rothbart MK. Studying infant temperament via the Revised Infant Behavior Questionnaire. Infant Behavior and Development. 2003;26(1):64–86. doi: 10.1016/S0163-6383(02)00169-8. [DOI] [Google Scholar]
- Goldsmith HH, Campos JJ. Toward a theory of infant temperament. In: Emde RN, Harmon RJ, editors. The development of attachment and affiliative systems. New York: Plenum; 1982. pp. 161–193. [DOI] [Google Scholar]
- Halpern LF, Anders TF, Garcia Coll C, Hua J. Infant temperament: Is there a relation to sleep-wake states and maternal nighttime behavior? Infant Behavior and Development. 1994;17(3):255–263. doi: 10.1016/0163-6383(94)90004-3. [DOI] [Google Scholar]
- Henderson JM, France KG, Blampied NM. The consolidation of infants’ nocturnal sleep across the first year of life. Sleep Medicine Reviews. 2011;15(4):211–220. doi: 10.1016/j.smrv.2010.08.003. [DOI] [PubMed] [Google Scholar]
- Johnson CM. Infant and toddler sleep: a telephone survey of parents in one community. Journal of Developmental & Behavioral Pediatrics. 1991;12(2):108–114. doi: 10.1097/00004703-199104000-00007. [DOI] [PubMed] [Google Scholar]
- Kelmanson IA. Temperament and sleep characteristics in two-month-old infants. Sleep and Hypnosis. 2004;6:78–84. [Google Scholar]
- Kiff CJ, Lengua LJ, Zalewski M. Nature and nurturing: Parenting in the context of child temperament. Clinical child and family psychology review. 2011;14(3):251–301. doi: 10.1007/s10567-011-0093-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kochanska G, Aksan N, Penney SJ, Doobay AF. Early positive emotionality as a heterogenous trait: Implications for children’s self-regulation. Journal of personality and social psychology. 2007;93(6):1054–1066. doi: 10.1037/0022-3514.93.6.1054. [DOI] [PubMed] [Google Scholar]
- Minde K, Faucon A, Falkner S. Sleep problems in toddlers: effects of treatment on their daytime behavior. Journal of the American Academy of Child & Adolescent Psychiatry. 1994;33(8):1114–1121. doi: 10.1097/00004583-199410000-00007. [DOI] [PubMed] [Google Scholar]
- Mindell JA, Telofski LS, Wiegand B, Kurtz ES. A nightly bedtime routine: impact on sleep in young children and maternal mood. Sleep. 2009;32(5):599–606. doi: 10.1093/sleep/32.5.599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Monroe SM, Simons AD. Diathesis-stress theories in the context of life stress research: Implications for the depressive disorders. Psychological Bulletin. 1991;110:406–425. doi: 10.1037/0033-2909.110.3.406. [DOI] [PubMed] [Google Scholar]
- Novosad C, Freudigman K, Thoman EB. Sleep patterns in newborns and temperament at eight months: a preliminary study. Journal of Developmental & Behavioral Pediatrics. 1999;20(2):99–105. doi: 10.1097/00004703-199904000-00005. [DOI] [PubMed] [Google Scholar]
- Parade SH, Leerkes EM. The reliability and validity of the Infant Behavior Questionnaire-Revised. Infant behavior & development. 2008;31(4):637–646. doi: 10.1016/j.infbeh.2008.07.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pilcher JJ, Ginter DR, Sadowsky B. Sleep quality versus sleep quantity: relationships between sleep and measures of health, well-being and sleepiness in college students. Journal of psychosomatic research. 1997;42(6):583–596. doi: 10.1016/S0022-3999(97)00004-4. [DOI] [PubMed] [Google Scholar]
- Priddis LE. Tuned in parenting and infant sleep patterns. Early Child Development and Care. 2009;179(3):259–269. doi: 10.1080/03004430600912132. [DOI] [Google Scholar]
- Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. Journal of applied psychology. 2003;88(5):879–903. doi: 10.1037/0021-9010.88.5.879. [DOI] [PubMed] [Google Scholar]
- Putnam SP, Rothbart MK, Gartstein MA. Homotypic and heterotypic continuity of fine-grained temperament during infancy, toddlerhood, and early childhood. Infant and Child Development. 2008;17(4):387–405. doi: 10.1002/icd.582. [DOI] [Google Scholar]
- Rothbart MK, Bates JE. Handbook of child psychology: Vol 3. Social, emotional and personality development. 5th. New York: Wiley; 1998. Temperament; pp. 105–176. In W. Damon (Series Ed.), & N. Eisenberg (Vol. Ed.) [Google Scholar]
- Rothbart MK, Bates JE. Temperament. In: Damon W, Lerner R, Eisenberg N, editors. Handbook of child psychology: Vol 3. Social, emotional, and personality development. 6th. New York: Wiley; 2006. pp. 99–166. [Google Scholar]
- Sadeh A, Anders TF. Infant sleep problems: Origins, assessment, interventions. Infant Mental Health Journal. 1993;14(1):17–34. 10.1002/1097-0355(199321)14:1<17::AID-IMHJ2280140103>3.0.CO;2-Q. [Google Scholar]
- Sadeh A, Lavie P, Scher A. Sleep and temperament: maternal perceptions of temperament of sleep-disturbed toddlers. Early education and development. 1994;5(4):311–322. doi: 10.1207/s15566935eed0504_6. [DOI] [Google Scholar]
- Sadeh A, Tikotzky L, Scher A. Parenting and infant sleep. Sleep medicine reviews. 2010;14(2):89–96. doi: 10.1016/j.smrv.2009.05.003. [DOI] [PubMed] [Google Scholar]
- Sameroff AJ. Models of developmental regulation: The environtype. In: Cicchetti D, editor. The emergence of a discipline: Rochester Symposium on Developmental Psychopathology. Vol. 1. Hillsdale, NJ: Erlbaum; 1989. pp. 41–68. [Google Scholar]
- Sanson A, Rothbart M. Child Temperament and Parenting. In: Bornstein Marc., editor. Handbook of Parenting. Vol. 4. Mahwah, NJ: Erlbaum; 1995. Applied and Practical Parenting. [Google Scholar]
- Scher A. Mother-child interaction and sleep regulation in one-year-olds. Infant Mental Health Journal. 2001;22(5):515–528. doi: 10.1002/imhj.1015. [DOI] [Google Scholar]
- Scher A, Epstein R, Sadeh A, Tirosh E, Lavie P. Toddlers’ sleep and temperament: reporting bias or a valid link? A research note. Journal of Child Psychology and Psychiatry. 1992;33(7):1249–1254. doi: 10.1111/j.1469-7610.1992.tb00943.x. [DOI] [PubMed] [Google Scholar]
- Scher A, Epstein R, Tirosh E. Stability and changes in sleep regulation: A longitudinal study from 3 months to 3 years. International Journal of Behavioral Development. 2004;28(3):268–274. doi: 10.1080/01650250344000505. [DOI] [Google Scholar]
- Scher A, Tirosh E, Lavie P. Relationship between Sleep and Temperament Revisited: Evidence for 12-month-olds: A Research Note. Journal of child psychology and psychiatry. 1998;39(5):785–788. doi: 10.1017/S0021963098002546. [DOI] [PubMed] [Google Scholar]
- Shiner RL, Buss KA, McClowry SG, Putnam SP, Saudino KJ, Zentner M. What Is Temperament Now? Assessing Progress in Temperament Research on the Twenty-Fifth Anniversary of Goldsmith et al. (1987) Child Development Perspectives. 2012;6(4):436–444. doi: 10.1111/j.1750-8606.2012.00254.x. [DOI] [Google Scholar]
- So K, Buckley P, Adamson TM, Horne RS. Actigraphy correctly predicts sleep behavior in infants who are younger than six months, when compared with polysomnography. Pediatric research. 2005;58(4):761–765. doi: 10.1203/01.PDR.0000180568.97221.56. [DOI] [PubMed] [Google Scholar]
- Spruyt K, Aitken RJ, So K, Charlton M, Adamson TM, Horne RSC. Relationship between sleep/wake patterns, temperament and overall development in term infants over the first year of life. Early human development. 2008;84(5):289–296. doi: 10.1016/j.earlhumdev.2007.07.002. [DOI] [PubMed] [Google Scholar]
- Teti DM, Kim BR, Mayer G, Countermine M. Maternal emotional availability at bedtime predicts infant sleep quality. Journal of Family Psychology. 2010;24(3):307–315. doi: 10.1037/a0019306. [DOI] [PubMed] [Google Scholar]
- Touchette É, Dionne G, Forget-Dubois N, Petit D, Pérusse D, Falissard B, Montplaisir JY. Genetic and Environmental Influences on Daytime and Nighttime Sleep Duration in Early Childhood. Pediatrics. 2013:1874–1880. doi: 10.1542/peds.2012-2284. [DOI] [PubMed] [Google Scholar]
- Weissbluth M. Sleep duration and infant temperament. Annual Progress In Child Psychiatry. 1981;99(5):817–819. doi: 10.1016/s0022-3476(81)80422-2. [DOI] [PubMed] [Google Scholar]