

Abstract
Physical activity has been inconsistently associated with risk of gestational diabetes mellitus in epidemiological studies, and questions remain about the strength and shape of the dose–response relationship between the two. We therefore conducted a systematic review and meta-analysis of cohort studies and randomized trials on physical activity and gestational diabetes mellitus. PubMed, Embase and Ovid databases were searched for cohort studies, and randomized controlled trials of physical activity and risk of gestational diabetes mellitus, up to August 5th 2015. Summary relative risks (RRs) were estimated using a random effects model. Twenty-five studies (26 publications) were included. For total physical activity the summary RR for high versus low activity was 0.62 (95 % CI 0.41–0.94, I2 = 0 %, n = 4) before pregnancy, and 0.66 (95 % CI 0.36–1.21, I2 = 0 %, n = 3) during pregnancy. For leisure-time physical activity the respective summary RRs for high versus low activity was 0.78 (95 % CI 0.61–1.00, I2 = 47 %, n = 8) before pregnancy, and it was 0.80 (95 % CI 0.64–1.00, I2 = 17 %, n = 17) during pregnancy. The summary RR for pre-pregnancy activity was 0.70 (95 % CI 0.49–1.01, I2 = 72.6 %, n = 3) per increment of 5 h/week and for activity during pregnancy was 0.98 (95 % CI 0.87–1.09, I2 = 0 %, n = 3) per 5 h/week. There was evidence of a nonlinear association between physical activity before pregnancy and the risk of gestational diabetes mellitus, pnonlinearity = 0.005, with a slightly steeper association at lower levels of activity although further reductions in risk were observed up to 10 h/week. There was also evidence of nonlinearity for physical activity in early pregnancy, pnonlinearity = 0.008, with no further reduction in risk above 8 h/week. There was some indication of inverse associations between walking (before and during pregnancy) and vigorous activity (before pregnancy) and the risk of gestational diabetes mellitus. This meta-analysis suggests that there is a significant inverse association between physical activity before pregnancy and in early pregnancy and the risk of gestational diabetes mellitus. Further studies are needed to clarify the association between specific types and intensities of activity and gestational diabetes mellitus.
Electronic supplementary material
The online version of this article (doi:10.1007/s10654-016-0176-0) contains supplementary material, which is available to authorized users.
Keywords: Physical activity, Exercise, Walking, Gestational diabetes, Abnormal glucose tolerance, Review, Meta-analysis
Introduction
Gestational diabetes mellitus is an important cause of maternal and perinatal complications including preeclampsia, gestational hypertension, caesarean section, macrosomia, and stillbirths [1]. Gestational diabetes mellitus is a glucose intolerance discovered for the first time in pregnancy and is by the National Institute for Health and Care Excellence (NICE) defined as a fasting plasma glucose of 5.6 mmol/L or higher or a 2-h plasma glucose level of 7.8 mmol/L or higher [2]. However, there is still no international agreement about the definition of gestational diabetes mellitus [3]. The prevalence of gestational diabetes mellitus is increasing worldwide [4] parallel to the increase in prevalence of overweight and obesity among pregnant women. Overweight and obesity is the strongest risk factor for gestational diabetes mellitus with 2–3 and 5–6 fold increases in the relative risk (RR) compared to normal weight women [5, 6]. Some evidence suggests an increased risk even within the high-normal range of body mass index compared to the low-normal range [7, 8], similar to what is observed for type 2 diabetes [9]. Gestational diabetes and type 2 diabetes have many pathophysiological features in common.
Although physical activity has been established as a protective factor for type 2 diabetes [10], the data regarding physical activity and gestational diabetes mellitus are less extensive and less convincing [11–37]. Several [16, 19, 21, 23–27, 29, 34–40], but not all studies [11–15, 17, 18, 20, 22, 28, 30], have reported inverse associations between higher physical activity and gestational diabetes mellitus risk, however, even among the studies that did report inverse associations the strength of the associations have varied considerably with reductions in the relative risk ranging from 10–30 [24–26, 37] up to 50–90 % [16, 19, 21, 23, 27, 34–36, 38]. It is not clear whether the variability in the results could be due to differences in the ranges and amounts of physical activity between studies, or if it varies by subtypes or intensity of physical activity, or whether it is the total amount of physical activity that is the most important factor. A previous meta-analysis of case–control and cohort studies reported an inverse association between high versus low physical activity and gestational diabetes mellitus [41], but no dose–response analyses were conducted. Two more recent meta-analyses [42, 43], which only included randomized trials came to opposite conclusions to whether physical activity reduces gestational diabetes risk with one showing no association [42] and another showing an inverse association [43], but none of the published meta-analyses reported whether the amount of physical activity was related to the outcome. Some studies have reported dose-dependent inverse associations between physical activity and gestational diabetes mellitus risk [23, 24, 31, 35, 37], however, other studies suggested that most of the benefit observed was when increasing physical activity level from a low level to a moderate level [25, 27, 34]. Clarifying whether there is a linear dose–response relationship or whether there are threshold levels of activity could be important to provide more detailed recommendations for the physical activity level needed for women to reduce the risk of gestational diabetes mellitus, and could also provide crucial information for the planning of future large-scale randomized trials of physical activity for prevention of the disease.
Several additional studies have been published since the previous meta-analyses [12–14, 16, 19–22, 28–33] and for this reason we conducted an updated systematic review and meta-analysis of physical activity and gestational diabetes mellitus with a particular aim of clarifying whether there is a dose–response relationship between increasing physical activity level and lower risk of gestational diabetes mellitus. We also summarized studies that have been published on physical activity and abnormal glucose tolerance (elevated glucose levels in the non-diabetic range) [22, 25, 33, 39, 44, 45].
Methods
Search strategy
The PubMed, Embase and Ovid databases were initially searched up to December 10th 2014 for cohort studies and randomized trials of physical activity and gestational diabetes mellitus risk and the searches were later updated to August 5th 2015. We used the following search terms: (physical activity OR exercise OR sports OR walking OR biking OR running OR fitness OR “exercise test” OR inactivity OR sedentary OR “risk factor” OR “risk factors”) AND (“gestational diabetes” OR “gestational diabetes mellitus”) AND (“case–control” OR retrospective OR cohort OR cohorts OR prospective OR longitudinal OR “follow-up” OR “cross-sectional” OR trial). We also searched the reference lists of previous reviews on the subject [41–43] and of the studies included in the analysis for any further studies.
Study selection
To be included, the study had to be a randomized controlled trial, or a cohort study, and to investigate the association between physical activity and risk of gestational diabetes mellitus or abnormal glucose tolerance. Estimates of the relative risk (hazard ratio, risk ratio, odds ratio) had to be available with the 95 % confidence intervals, and for the dose–response analysis, a quantitative measure of activity level for 3 or more categories of activity and the total number of cases and person-years or participants had to be available in the publication. When multiple publications were available from the same study we used the study with the most detailed analyses of physical activity and the largest number of participants. We identified 26 studies that were included in total [11–37, 39, 44, 45], 23 studies that could be included in the analysis [11–37] of gestational diabetes mellitus and six studies that could be included in the analysis of abnormal glucose tolerance [22, 25, 33, 39, 44, 45]. A list of the excluded studies and reasons for exclusion is found in Supplementary Table 1. The search was conducted by DA and study selection was conducted by DA and AS.
Data extraction
We extracted the following data from each study: The first author’s last name, publication year, country where the study was conducted, follow-up period, sample size, age, number of cases, exposure, physical activity level, RRs and 95 % CIs, and variables adjusted for in the analysis. Data extractions were done by DA and checked for accuracy by AS.
Study quality assessment
The quality of the studies included was assessed using the Newcastle–Ottawa scale [46] for cohort studies and the Cochrane Collaboration’s tool for assessing risk of bias in randomised trials [47]. The Newcastle–Ottawa scale assesses the study quality based on the selection (representativeness of the exposed cohort, selection of the non-exposed cohort, ascertainment of exposure, demonstration that the outcome of interest was not present at the start of the study), comparability (adjustment for confounding factors), and the outcome (outcome assessment, long enough follow-up, adequacy of follow-up of cohorts). The randomized trials were assessed for risk of bias based on random sequence generation, allocation concealment, blinding of participants and personal, blinding of outcome assessment, incomplete outcome data, selective reporting, and other biases. Subgroup analyses by study quality scores or risk of bias were conducted separately for the observational studies and the randomized trials because of the different scales for the two study designs. For the observational studies we grouped studies with 0–3, 4–6, and 7–9 points to indicate low, medium and high quality studies, while the randomized trials studies were grouped according to whether they were at high, low or unclear risk of bias in the subgroup analyses.
Statistical methods
We used random effects models to calculate summary RRs and 95 % CIs for the highest versus the lowest level of physical activity and for the dose–response analysis [48]. The average of the natural logarithm of the RRs was estimated and the RR from each study was weighted by the inverse of its variance and then un-weighted by a variance component which corresponds to the amount of heterogeneity in the analysis. A two-tailed p < 0.05 was considered statistically significant.
We used the method described by Greenland and Longnecker [49] for the dose–response analysis and computed study-specific slopes (linear trends) and 95 % CIs from the natural logs of the RRs and CIs across categories of physical activity. The method requires that the distribution of cases and person-years or non-cases and the RRs with the variance estimates for at least three quantitative exposure categories are known. We estimated the distribution of cases or person-years in studies that did not report these, but reported the total number of cases/person-years, as described previously [50, 51]. The median or mean physical activity level in each category was assigned to the corresponding relative risk for each study. For studies that reported physical activity by ranges of activity we estimated the midpoint for each category by calculating the average of the lower and upper bound. When the highest or lowest category was open-ended we assumed the open-ended interval length to be the same as the adjacent interval. For one study which only provided a continuous estimate of physical activity per 100 kcal of energy expenditure we re-calculated the odds ratio so it corresponded to an increment equal to the highest compared to the lowest quartile so it could be included in the high versus low analysis [26], and the same was done for another study [30]. For the dose–response analysis we conducted separate analyses for studies reporting results in metabolic equivalent task (MET)-hours and hours/week. The MET is an index of the intensity of physical activity and is defined as the caloric expenditure per kilogram of body weight per hour of activity, divided by the equivalent per hour at rest [52]. One MET is equal to the energy cost of a person during quiet sitting, walking slowly has a MET value of 2 and jogging and bicycling have MET values of 7–8. MET-hours are the number of hours spent in each activity multiplied with the MET value of that activity. For one study [37] we converted frequency of physical activity/week to hours/week by assigning a dose of 45 min per session [10, 53]. We examined a potential nonlinear dose–response relationship between physical activity and gestational diabetes mellitus by using restricted cubic splines with three knots at 10, 50 and 90 % percentiles of the distribution which was combined using multivariate meta-analysis [54, 55]. A likelihood ratio test was used to assess the difference between the nonlinear and linear models to test for nonlinearity [56]. Although formal dose–response analyses were not possible for the randomized controlled trials we fitted a linear regression of the RR estimates against the total number of hours/week the interventions lasted.
Heterogeneity between studies was assessed by the Q test and I2 [57]. I2 is the amount of total variation that is explained by between study variation. I2 values of approximately 25, 50 and 75 % are considered to indicate low, moderate and high heterogeneity, respectively. To investigate sources of heterogeneity subgroup analyses were conducted according to study design, geographic location, number of cases and adjustment for confounding factors. Meta-regression analyses were used to test for heterogeneity between subgroups.
Publication bias was assessed with Egger’s test [58] and the results were considered to indicate publication bias when p < 0.10. We conducted sensitivity analyses excluding one study at a time to ensure that the results were not simply due to one large study or a study with an extreme result. The statistical analyses were conducted using Stata, version 13.0 software (StataCorp, College Station, TX, USA). The following Stata commands were used: metan7 (high versus low analyses and dose–response analyses), glst (dose–response analyses), metareg (meta-regression analyses), metabias6 (Egger’s test), metafunnel (funnel plot), metaninf (influence or sensitivity analyses).
Results
Out of the 7616 records which were identified by the literature search, 7501 were excluded based on the title and abstract (one author screened all references), and 115 full text articles were assessed in detail (in duplicate) as they reported on physical activity or risk factors and gestational diabetes mellitus in the title/abstract (Fig. 1). Out of these articles, 26 publications (25 studies) were finally included in the meta-analysis, including twelve randomized trials [11–22] and eleven cohort studies [23–33] that could be included in the meta-analysis of physical activity and gestational diabetes mellitus (Tables 1, 2, 3; Fig. 1), and one randomized trial [22] and five cohort studies [25, 33, 39, 44, 45] that were included in the meta-analysis of physical activity and risk of abnormal glucose tolerance (Table 4; Fig. 1).
Fig. 1.

Flow-chart of study selection
Table 1.
Randomized controlled trials of physical activity and gestational diabetes mellitus risk
| Author, publication year, country/region | Follow-up period | Study size, gender, age, number of cases | Exposure | Quantity | RR (95 % CI)a | Adjustment for confounders |
|---|---|---|---|---|---|---|
| Callaway LK et al., 2010, Australia | NA | 22 obese women, exercise intervention: 5 cases | Physical activity during pregnancy | 900 kcal/week of energy expenditure | 1.44 (0.43–4.98) | – |
| 19 controls: 3 cases | Individualised exercise program with the goal of an energy expenditure of 900 kcal/week | |||||
| Price BB et al., 2012, USA | 2006–2010 | 43 (31 analysed) women, exercise intervention: 3 cases | Physical activity during pregnancy | 45–60 min × 4/week | 0.75 (0.20–2.78) | – |
| 48 (31 analysed) women, control group: 4 cases | Supervised aerobic training of 45–60 min 4 times per week at moderate intensity (12–14 on Borg Scale of perceived exertion) | |||||
| Oostdam N et al., 2012, Netherlands | 2007–2011 | 62 (48) women, exercise group: 7 cases | Physical activity during pregnancy | 60 min × 2/week | 0.65 (0.27–1.55) | – |
| 59 (51) women, control group: 11 cases | Exercise program 2 days/week, 60 min per session. Aerobic and strength exercises aimed to control blood glucose levels | |||||
| Stafne SN et al., 2012, Norway | 2007–2009 | 429 (375 analysed) women, exercise group: 25 cases | Physical activity during pregnancy | 60 min × 1/week | 1.21 (0.68–2.16) | – |
| 426 (327 analysed) women, control group: 18 cases | Standardized exercise program including aerobic activity, strength training, balance exercises, 60 min training sessions one time per week between gestational week 20–36 | |||||
| Barakat R et al., 2012, Spain | NA | 40 women, exercise group: 0 cases | Physical activity during pregnancy | 35–45 min × 3/week | 0.15 (0.01–1.32) | – |
| 43 women, control group: 3 cases | Physical conditioning programme with two land aerobic sessions and one aquatic session of 35–45 min sessions for a total of 3 times per week from gestational weeks 6–9 to weeks 38–39 | |||||
| Barakat R et al., 2013, Spain | 2007–2011 | 255 women, exercise group: 41 cases | Physical activity during pregnancy | 50–55 min × 3/week | 0.84 (0.50–1.40) | Maternal age, pre-pregnancy body weight |
| 255 women, control group: 61 cases | Physical activity intervention 50–55 min per session, 3 times per week including aerobic exercise, muscle strengthening and flexibility exercises from weeks 10–12 of pregnancy to weeks 38–39 | |||||
| Tomic V et al., 2013, Croatia | 2008–2009 | 166 women, physical exercise group: 3 cases | Physical activity during pregnancy | 50 min × 3/week | 0.22 (0.07–0.69) | – |
| 168 women, control group: 14 cases | Aerobic exercise of moderate intensity, 50 min/session, 3 times/week during the whole pregnancy period | |||||
| Barakat R et al., 2014, Spain | NA | 137 women, exercise group: 5 cases | Physical activity during pregnancy | 55–60 min × 3/week | 0.83 (0.26–2.63) | – |
| 114 women, control group: 5 cases | Physical conditioning program of three 55–60 min sessions per week that started between 9 and 13 weeks gestation to weeks 39–40 | |||||
| Ko CW et al., 2014, USA | NA | 591 women, physical activity group: 25 cases | Physical activity during pregnancy | 30 min × 3/week − 45–60 min/week × 4–5/week | 0.78 (0.47–1.28) | – |
| 605 women, control group: 33 cases | Exercise intervention of moderate to vigorous intensity, 30 min/session, 3 times per week with a goal to increase to 45–60 min/session, 4–5 times/week | |||||
| Renault KM et al., 2014, Denmark | 2009–2012 | 125 women, physical activity group: 2 cases | Physical activity during pregnancy | 11,000 steps/day | 0.27 (0.06–1.16) | – |
| 134 women, control group: 7 cases | Physical activity intervention to increase daily step count to 11,000 (monitored by pedometer) | |||||
| Cordero Y et al., 2014, Spain | NA | 101 women, exercise group: 1 case | Physical activity during pregnancy | 50–60 min × 3/week | 0.10 (0.01–0.80) | – |
| 156 women, control group: 13 cases | Physical activity program with 50–60 min sessions, 3 times per week from weeks 10–14 to the end of the third trimester | |||||
| Nobles C et al., 2015, USA | 2007–2012 | 124 women, exercise group: 12 cases | Physical activity during pregnancy | 30 min most days of the week | 0.60 (0.27–1.32) | Education, parity |
| 127 women, control group: 19 cases | Intervention to increase activity level to moderate-intensity physical activity of 30 min on most days of the week |
Table 2.
Prospective cohort studies of physical activity and gestational diabetes mellitus risk
| Author, publication year, country/region | Follow-up period | Study size, gender, age, number of cases | Exposure | Quantity | RR (95 % CI) | Adjustment for confounders |
|---|---|---|---|---|---|---|
| Dempsey JC et al., 2004, USA | 1996–2000 | 909: 42 cases | Physical activity before pregnancy | |||
| Any recreational physical activity | No | 1.00 | Age, race, parity | |||
| Yes | 0.36 (0.18–0.76) | |||||
| Time spent performing recreational physical activity | None | 1.00 | ||||
| <4.2 hrs/wk | 0.51 (0.24–1.09) | |||||
| ≥4.2 | 0.20 (0.08–0.51) | |||||
| Energy expended performing recreational physical activity | None | 1.00 | ||||
| <21.1 MET-hours/week | 0.51 (0.24–1.08) | |||||
| ≥21.1 | 0.20 (0.08–0.51) | |||||
| Any recreational physical activity | No | 1.00 | Age, race, parity, prepregnancy BMI | |||
| Yes | 0.44 (0.21–0.91) | |||||
| Time spent performing recreational physical activity | None | 1.00 | ||||
| <4.2 hrs/wk | 0.58 (0.27–1.24) | |||||
| ≥4.2 | 0.24 (0.10–0.64) | |||||
| Energy expended performing recreational physical activity | None | 1.00 | ||||
| <21.1 MET-hours/week | 0.57 (0.27–1.21) | |||||
| ≥21.1 | 0.26 (0.10–0.65) | |||||
| Physical activity during pregnancy | ||||||
| Any recreational physical activity | No | 1.00 | Age, race, parity | |||
| Yes | 0.60 (0.33–1.10) | |||||
| Time spent performing recreational physical activity | None | 1.00 | ||||
| <6.0 hrs/wk | 0.43 (0.19–0.99) | |||||
| ≥6.0 | 0.76 (0.38–1.50) | |||||
| Energy expended performing recreational physical activity | None | 1.00 | ||||
| <28 MET-hours/week | 0.65 (0.32–1.34) | |||||
| ≥28 | 0.55 (0.26–1.17) | |||||
| Any recreational physical activity | No | 1.00 | Age, race, parity, prepregnancy BMI | |||
| Yes | 0.69 (0.37–1.29) | |||||
| Time spent performing recreational physical activity | None | 1.00 | ||||
| <6.0 hrs/wk | 0.49 (0.21–1.13) | |||||
| ≥6.0 | 0.90 (0.45–1.80) | |||||
| Energy expended performing recreational physical activity | None | 1.00 | ||||
| <28 MET-hours/week | 0.71 (0.35–1.47) | |||||
| ≥28 | 0.67 (0.31–1.43) | |||||
| Recreational physical activity before and during pregnancy | Neither | 1.00 | Age, race, parity | |||
| Active last year only | 0.45 (0.17–1.20) | |||||
| Active last week only | 0.83 (0.23–2.94) | |||||
| Active both periods | 0.28 (0.11–0.73) | |||||
| Recreational physical activity before and during pregnancy | Neither | 1.00 | Age, race, parity, prepregnancy BMI | |||
| Active last year only | 0.40 (0.15–1.07) | |||||
| Active last week only | 0.59 (0.16–2.14) | |||||
| Active both periods | 0.31 (0.12–0.79) | |||||
| Oken E et al., 2006, USA | 1999–2002 | 1805: 91 cases | Physical activity before pregnancy | |||
| Walking | ≤1 hrs/wk | 1.00 | Age, race/ethnicity, prepregnancy BMI, history of gestational diabetes mellitus in a previous pregnancy, mother’s history of gestational diabetes mellitus | |||
| >1 | 0.67 (0.34–1.34) | |||||
| Light moderate activity | None | 1.00 | ||||
| Any | 1.16 (0.67–1.99) | |||||
| Vigorous activity | None | 1.00 | ||||
| Any | 0.56 (0.33–0.95) | |||||
| Light/moderate or vigorous activity | None | 1.00 | ||||
| Any | 0.91 (0.51–1.65) | |||||
| Total leisure-time physical activity | ≤2 hrs/wk | 1.00 | ||||
| 3–6 | 0.78 (0.34–1.76) | |||||
| 7–13 | 0.63 (0.28–1.39) | |||||
| ≥14 | 0.70 (0.30–1.68) | |||||
| Physical activity during pregnancy | ||||||
| Walking, during pregnancy | ≤1 hrs/wk | 1.00 | ||||
| >1 | 0.67 (0.35–1.30) | |||||
| Light moderate activity | None | 1.00 | ||||
| Any | 0.70 (0.41–1.21) | |||||
| Vigorous activity | None | 1.00 | ||||
| Any | 0.90 (0.47–1.70) | |||||
| Light/moderate or vigorous activity | None | 1.00 | ||||
| Any | 0.73 (0.43–1.25) | |||||
| Total leisure-time physical activity | ≤2 hrs/wk | 1.00 | ||||
| 3–6 | 0.72 (0.37–1.40) | |||||
| 7–13 | 0.59 (0.28–1.23) | |||||
| ≥14 | 0.91 (0.37–2.21) | |||||
| Physical activity before and during pregnancy | No/no | 1.00 | ||||
| No/yes | 1.28 (0.54–3.02) | |||||
| Yes/no | 0.83 (0.36–1.90) | |||||
| Yes/yes | 0.49 (0.24–1.01) | |||||
| Zhang C et al., 2006, USA | 1989–1999, 10 years follow-up | 21,765: 1428 cases | Physical activity before pregnancy | |||
| Leisure-time physical activity, prepregnancy | 2.3 MET-hours/week | 1.00 | Age, race/ethnicity, smoking status, family history of diabetes mellitus in 1st degree relative, parity, alcohol intake, total energy, cereal fiber, total fat, glycemic load | |||
| 7.8 | 0.94 (0.83–1.14) | |||||
| 15.9 | 0.83 (0.70–0.97) | |||||
| 29 | 0.86 (0.73–1.02) | |||||
| 63.2 | 0.71 (0.60–0.84) | |||||
| Vigorous physical activity | 0 MET-hours/week | 1.00 | ||||
| 1.4 | 0.94 (0.71–1.26) | |||||
| 6 | 0.81 (0.67–1.16) | |||||
| 15 | 0.70 (0.60–0.82) | |||||
| 38.8 | 0.72 (0.62–0.84) | |||||
| Usual walking pace, among women without vigorous activity | Casual | 1.00 | ||||
| Normal | 0.79 (0.57–1.08) | |||||
| Brisk, very brisk | 0.60 (0.42–0.86) | |||||
| Stair climbing, among women without vigorous activity | ≤2 flights/day | 1.00 | ||||
| 3–4 | 1.03 (0.80–1.33) | |||||
| 5–9 | 0.97 (0.75–1.26) | |||||
| 10–14 | 0.73 (0.51–1.05) | |||||
| ≥15 | 0.44 (0.24–0.79) | |||||
| Leisure-time physical activity | 2.3 MET-hours/week | 1.00 | Age, race/ethnicity, smoking status, family history of diabetes mellitus in 1st degree relative, parity, alcohol intake, total energy, cereal fiber, total fat, glycemic load, BMI | |||
| 7.8 | 0.97 (0.87–1.20) | |||||
| 15.9 | 0.88 (0.75–1.04) | |||||
| 29 | 0.90 (0.80–1.11) | |||||
| 63.2 | 0.81 (0.68–1.01) | |||||
| Vigorous physical activity | 0 MET-hours/week | 1.00 | ||||
| 1.4 | 0.95 (0.71–1.28) | |||||
| 6 | 0.84 (0.71–1.20) | |||||
| 15 | 0.75 (0.64–0.87) | |||||
| 38.8 | 0.77 (0.69–0.94) | |||||
| Usual walking pace, among women without vigorous activity | Casual | 1.00 | ||||
| Normal | 0.81 (0.59–1.12) | |||||
| Brisk, very brisk | 0.66 (0.46–0.95) | |||||
| Stair climbing, among women without vigorous activity | ≤2 flights/day | 1.00 | ||||
| 3–4 | 1.03 (0.80–1.33) | |||||
| 5–9 | 1.00 (0.77–1.30) | |||||
| 10–14 | 0.77 (0.54–1.11) | |||||
| ≥15 | 0.50 (0.27–0.90) | |||||
| Iqbal R et al., 2007, Pakistan | 2002–2004 | 611 South Asian women: 49 cases | Physical activity before pregnancy | |||
| Total physical activity | Per 100 kcal energy expenditure | 0.89 (0.79–0.99) | Age, BMI, family history of diabetes, education, parity, height, rate of weight gain during pregnancy | |||
| Total physical activity | Per 100 kcal energy expenditure | 0.89 (0.79–0.99) | Age, body fat, family history of diabetes, education, parity, height, rate of weight gain during pregnancy | |||
| Chasan-Taber L et al., 2008, USA | 2000–2004 | 1006 Hispanic women: 33 cases | Physical activity before pregnancy | |||
| Household activity, caregiving | 1.9 KPAS score | 1.0 | Age, BMI | |||
| 2.3 | 0.3 (0.1–0.9) | |||||
| 2.7 | 0.3 (0.1–0.9) | |||||
| 3.2 | 0.2 (0.1–0.8) | |||||
| Occupational physical activity | 1.0 KPAS score | 1.0 | ||||
| 2 | 0.4 (0.1–2.2) | |||||
| 3 | 2.1 (0.7–6.0) | |||||
| 3.9 | 1.7 (0.6–5.1) | |||||
| Sports, exercise | 1.3 KPAS score | 1.0 | ||||
| 1.5 | 1.8 (0.5–6.0) | |||||
| 2.8 | 1.5 (0.4–5.8) | |||||
| 4 | 2.1 (0.6–7.1) | |||||
| Active living | 1.7 KPAS score | 1.0 | ||||
| 2.5 | 1.1 (0.3–3.7) | |||||
| 3 | 1.3 (0.4–3.8) | |||||
| 3.8 | 2.0 (0.6–6.2) | |||||
| Total physical activity | 7.9 KPAS score | 1.0 | ||||
| 9.5 | 0.5 (0.1–2.3) | |||||
| 10.8 | 2.0 (0.7–5.8) | |||||
| 12.3 | 0.8 (0.2–2.7) | |||||
| Physical activity during early pregnancy | ||||||
| Household activity, caregiving | 1.7 KPAS score | 1.0 | ||||
| 2.1 | 0.3 (0.1–1.3) | |||||
| 2.4 | 0.7 (0.2–1.9) | |||||
| 3 | 0.8 (0.3–2.3) | |||||
| Occupational physical activity | 1.0 KPAS score | 1.0 | ||||
| 2.3 | 0.6 (0.2–1.9) | |||||
| 3.3 | 1.5 (0.7–3.5) | |||||
| Sports, exercise | 1.0 KPAS score | 1.0 | ||||
| 1.3 | 1.5 (0.5–4.5) | |||||
| 1.5 | 0.9 (0.3–2.9) | |||||
| 2.3 | 0.7 (0.2–2.5) | |||||
| Active living | 1.3 KPAS score | 1.0 | ||||
| 2 | 0.5 (0.1–1.7) | |||||
| 2.7 | 1.5 (0.5–4.6) | |||||
| 3.3 | 1.2 (0.4–3.4) | |||||
| Total physical activity | 6.8 KPAS score | 1.0 | ||||
| 8.1 | 0.5 (0.1–1.6) | |||||
| 9.2 | 0.6 (0.2–1.7) | |||||
| 10.7 | 0.8 (0.2–2.3) | |||||
| Physical activity during midpregnancy | ||||||
| Household activity, caregiving | 1.6 KPAS score | 1.0 | ||||
| 2 | 0.8 (0.3–2.4) | |||||
| 2.4 | 0.2 (0.1–0.7) | |||||
| 2.9 | 0.2 (0.1–0.8) | |||||
| Occupational physical activity | 1.0 KPAS score | 1.0 | ||||
| 2.2 | 0.7 (0.2–3.0) | |||||
| 3.1 | 1.0 (0.4–2.6) | |||||
| Sports, exercise | 1.0 KPAS score | 1.0 | ||||
| 1.3 | 0.4 (0.1–1.4) | |||||
| 1.5 | 1.3 (0.5–3.7) | |||||
| 2.5 | 0.1 (0.0–0.7) | |||||
| Active living | 1.5 KPAS score | 1.0 | ||||
| 2 | 0.6 (0.1–2.6) | |||||
| 2.7 | 1.9 (0.7–5.6) | |||||
| 3.3 | 0.6 (0.2–2.1) | |||||
| Total physical activity | 6.7 KPAS score | 1.0 | ||||
| 8.1 | 0.6 (0.2–1.8) | |||||
| 9.2 | 0.3 (0.1–1.1) | |||||
| 10.6 | 0.4 (0.1–1.2) | |||||
| Van der Ploeg HP et al., 2011, Australia | 1978–2003 | 2913: 180 cases | Physical activity before pregnancy | |||
| Moderate and vigorous physical activity | <180 MET min/wk | 1.00 | Age, number of children, age at 1st birth, country of birth, education, total energy intake | |||
| 180–600 | 1.28 (0.80–2.06) | |||||
| 600–1320 | 1.53 (0.95–2.47) | |||||
| >1320 | 1.22 (0.70–2.11) | |||||
| Ramos-Levi AM et al., 2012, Spain | 2009–2010 | 2194: 213 cases | Physical activity before pregnancy | |||
| Sports | ≥2 versus <2 days/wk | 0.67 (0.45–0.96) | Age, biscuits and pastries, red and processed meats, fruit, dried fruits and nuts, skimmed dairy products, legumes, blue fish, whole wheat bread, sauces, vegetables and salads, water, alcohol, sugary drinks, coffee, light walking, climbing up stairs | |||
| Mørkrid K et al., 2014, Norway | 2008–2010 | 759 women: 239 cases | Physical activity before pregnancy | |||
| Regular physical activity before pregnancy | No | 1.00 | Age, gestational week, pre-pregnancy BMI, ethnic origin, early life socioeconomic position score | |||
| Yes | 0.65 (0.46–0.94) | |||||
| Physical activity during early pregnancy | ||||||
| Objectively recorded moderate-vigorous physical activity | Per 1 SD (60 min/d) | 1.02 (0.85–1.23) | ||||
| Objectively recorded steps | Per 1 SD (3159 steps/d) | 0.81 (0.66–0.99) | ||||
| Zhang C et al., 2014, USA | 1989–2001 | 14,437 women: 823 cases | Physical activity before pregnancy | |||
| Moderate/vigorous physical activity | <30 min/wk | 1.00 | Age, parity, family history of diabetes, history of infertility, race/ethnicity, questionnaire period, total energy, alcohol, Alternate Healthy Eating Index-2010 diet score, BMI, smoking status | |||
| 30–59 | 0.90 (0.72–1.13) | |||||
| 60–89 | 0.91 (0.71–1.16) | |||||
| 90–149 | 0.89 (0.71–1.10) | |||||
| 150–209 | 0.85 (0.66–1.10) | |||||
| ≥210 | 0.78 (0.64–0.94) | |||||
| Currie LM et al., 2014, Canada | 2002–2005 | 1749 women: 36 cases | Physical activity before pregnancy | |||
| Total physical activity | <7.72 KPAS score | 1.00 | Maternal age, prepregnancy BMI, education, parity, history of gestational diabetes | |||
| 7.72- < 9.39 | 0.71 (0.33–1.56) | |||||
| ≥9.39 | 0.60 (0.24–1.48) | |||||
| Physical activity in the 1st half of pregnancy | ||||||
| Total physical activity | <6.44 KPAS score | 1.00 | ||||
| 6.44–<7.97 | 1.08 (0.50–2.32) | |||||
| ≥7.97 | 0.56 (0.22–1.47) | |||||
| Chasan-Taber L et al., 2014, USA | 2006–2011 | 1241 women: 175 cases | Physical activity before pregnancy | |||
| Met exercise guidelines, prepregnancy | No | 1.00 | Age, pre-pregnancy BMI, education, generation in the US | |||
| Yes | 1.01 (0.55–1.83) | |||||
| Total physical activity | 1 | 1.00 | ||||
| 2 | 1.20 (0.52–2.76) | |||||
| 3 | 1.13 (0.50–2.57) | |||||
| 4 | 0.79 (0.32–1.97) | |||||
| Moderate-intensity physical activity | 1 | 1.00 | ||||
| 2 | 0.97 (0.44–2.14) | |||||
| 3 | 1.07 (0.49–2.35) | |||||
| 4 | 0.69 (0.29–1.66) | |||||
| Vigorous intensity physical activity | No | 1.00 | ||||
| Yes | 0.90 (0.48–1.69) | |||||
| Household/caregiving physical activity | 1 | 1.00 | ||||
| 2 | 1.25 (0.58–2.69) | |||||
| 3 | 0.73 (0.31–1.71) | |||||
| 4 | 0.61 (0.26–1.45) | |||||
| Occupational physical activity | 1 | 1.00 | ||||
| 2 | 2.98 (1.26–7.03) | |||||
| 3 | 1.38 (0.51–3.76) | |||||
| 4 | 2.05 (0.86–4.90) | |||||
| Sports/exercise | 1 | 1.00 | ||||
| 2 | 1.76 (0.78–3.95) | |||||
| 3 | 0.96 (0.39–2.36) | |||||
| 4 | 1.26 (0.52–3.05) | |||||
| Physical activity during early pregnancy | ||||||
| Met exercise guidelines, early pregnancy | No | 1.00 | ||||
| Yes | 0.91 (0.45–1.83) | |||||
| Total physical activity | 1 | 1.00 | ||||
| 2 | 0.43 (0.14–1.27) | |||||
| 3 | 0.92 (0.39–2.18) | |||||
| 4 | 0.69 (0.27–1.73) | |||||
| Moderate-intensity physical activity | 1 | 1.00 | ||||
| 2 | 1.12 (0.47–2.65) | |||||
| 3 | 0.76 (0.30–1.94) | |||||
| 4 | 0.64 (0.24–1.76) | |||||
| Vigorous intensity physical activity | No | 1.00 | ||||
| Yes | 1.07 (0.39–2.89) | |||||
| Household/caregiving physical activity | 1 | 1.00 | ||||
| 2 | 2.75 (0.99–7.58) | |||||
| 3 | 1.08 (0.34–3.41) | |||||
| 4 | 1.88 (0.66–5.36) | |||||
| Occupational physical activity | Unemployed | 1.00 | ||||
| Low | 0.82 (0.38–1.77) | |||||
| High | 0.39 (0.15–0.99) | |||||
| Sports/exercise | 1 | 1.00 | ||||
| 2 | 1.51 (0.31–7.30) | |||||
| 3 | 1.11 (0.49–2.51) | |||||
| 4 | 1.07 (0.47–2.44) |
Hrs hours, wk week, KPAS Kaiser Physical Activity Survey, MET metabolic equivalent task, min minutes
Table 3.
Cohort studies and randomized trials of physical activity and impaired or abnormal glucose tolerance
| Author, publication year, country/region | Study period | Study size, gender, age, number of cases | Exposure | Quantity | RR (95 % CI) | Adjustment for confounders |
|---|---|---|---|---|---|---|
| Oken E et al., 2006, USA | 1999–2002 | 1805 women: 312 abnormal glucose tolerance cases | Physical activity before pregnancy | |||
| Walking | ≤1 h/week | 1.00 | Age, race/ethnicity, prepregnancy BMI, history of gestational diabetes mellitus in a previous pregnancy, mother’s history of gestational diabetes mellitus | |||
| >1 | 0.77 (0.52–1.13) | |||||
| Light moderate activity | None | 1.00 | ||||
| Any | 1.15 (0.86–1.53) | |||||
| Vigorous activity | None | 1.00 | ||||
| Any | 0.76 (0.57–1.00) | |||||
| Light/moderate or vigorous activity | None | 1.00 | ||||
| Any | 1.00 (0.73–1.37) | |||||
| Total leisure-time physical activity | ≤2 h/week | 1.00 | ||||
| 3–6 | 0.84 (0.54–1.31) | |||||
| 7–13 | 0.82 (0.53–1.25) | |||||
| ≥14 | 0.79 (0.49–1.26) | |||||
| Physical activity during pregnancy | ||||||
| Walking, during pregnancy | ≤1 h/week | 1.00 | ||||
| >1 | 0.71 (0.49–1.02) | |||||
| Light moderate activity | None | 1.00 | ||||
| Any | 0.79 (0.60–1.05) | |||||
| Vigorous activity | None | 1.00 | ||||
| Any | 0.73 (0.52–1.03) | |||||
| Light/moderate or vigorous activity | None | 1.00 | ||||
| Any | 0.76 (0.57–1.00) | |||||
| Total leisure-time physical activity | ≤2 h/week | 1.00 | ||||
| 3–6 | 0.94 (0.65–1.34) | |||||
| 7–13 | 0.80 (0.54–1.19) | |||||
| ≥14 | 0.68 (0.40–1.16) | |||||
| Physical activity before and during pregnancy | No/no | 1.00 | ||||
| No/yes | 1.19 (0.74–1.91) | |||||
| Yes/no | 1.04 (0.67–1.60) | |||||
| Yes/yes | 0.70 (0.49–1.01) | |||||
| Gollenberg AL et al., 2010, USA | 2000–2003 2006–2008 |
1231 Latina women: 104 abnormal glucose tolerance cases | Physical activity before pregnancy | |||
| Sports, exercise | 1 | 1.00 (0.51–1.96) | Maternal age, smoking, pre-pregnancy BMI, maternal education, parity | |||
| 2 | 1.67 (0.94–2.97) | |||||
| 3 | 1.04 (0.54–2.03) | |||||
| 4 | 1.00 | |||||
| Physical activity during early pregnancy | ||||||
| Sports, exercise | 1 | 1.16 (0.60–2.24) | ||||
| 2 | 1.66 (0.92–2.98) | |||||
| 3 | 1.30 (0.69–2.45) | |||||
| 4 | 1.00 | |||||
| Baptiste-Roberts K et al., 2011, USA | 152 women: not available | Physical activity before pregnancy | ||||
| Leisure-time physical activity | ≥2.75 versus <2.75 score | 0.32 (0.12–0.86) | Age, race, parity, gestational weight gain, pre-pregnancy BMI | |||
| Deierlein AL et al., 2012, USA | 2001–2005 | 1437 women: 269 hyperglycemia cases | Physical activity during early pregnancy | |||
| Total moderate and vigorous physical activity | None | 1.00 | Age at conception, pre-pregnancy BMI, race/ethnicity | |||
| Any | 0.93 (0.74–1.17) | |||||
| Recreational moderate and vigorous physical activity | None | 1.00 | ||||
| Any | 0.73 (0.54–0.99) | |||||
| Outdoor household moderate and vigorous physical activity | None | 1.00 | ||||
| Any | 0.90 (0.49–1.66) | |||||
| Indoor household moderate and vigorous physical activity | None | 1.00 | ||||
| Any | 1.10 (0.76–1.60) | |||||
| Caregiving moderate and vigorous physical activity | None | 1.00 | ||||
| Any | 0.80 (0.43–1.51) | |||||
| Work-related moderate and vigorous physical activity | None | 1.00 | ||||
| Any | 1.26 (0.90–1.78) | |||||
| Chasan-Taber L et al., 2014, USA | 2006–2011 | 1241 women: 161 abnormal glucose tolerance cases | Physical activity before pregnancy | |||
| Met exercise guidelines, prepregnancy | No | 1.00 | Age, pre-pregnancy BMI, education, generation in the US | |||
| Yes | 1.09 (0.76–1.56) | |||||
| Total physical activity | 1 | 1.00 | ||||
| 2 | 0.67 (0.40–1.13) | |||||
| 3 | 0.81 (0.49–1.33) | |||||
| 4 | 0.94 (0.57–1.53) | |||||
| Moderate-intensity physical activity | 1 | 1.00 | ||||
| 2 | 1.07 (0.67–1.72) | |||||
| 3 | 0.72 (0.43–1.19) | |||||
| 4 | 0.91 (0.56–1.50) | |||||
| Vigorous intensity physical activity | No | 1.00 | ||||
| Yes | 1.05 (0.73–1.51) | |||||
| Household/caregiving physical activity | 1 | 1.00 | ||||
| 2 | 0.88 (0.54–1.44) | |||||
| 3 | 0.91 (0.56–1.49) | |||||
| 4 | 0.89 (0.55–1.45) | |||||
| Occupational physical activity | 1 | 1.00 | ||||
| 2 | 1.12 (0.68–1.82) | |||||
| 3 | 0.97 (0.58–1.64) | |||||
| 4 | 0.97 (0.58–1.64) | |||||
| Sports/exercise | 1 | 1.00 | ||||
| 2 | 1.18 (0.72–1.92) | |||||
| 3 | 0.98 (0.59–1.62) | |||||
| 4 | 1.01 (0.61–1.68) | |||||
| Physical activity in early pregnancy | ||||||
| Met exercise guidelines, early pregnancy | No | 1.00 | ||||
| Yes | 1.12 (0.73–1.73) | |||||
| Total physical activity | 1 | 1.00 | ||||
| 2 | 0.70 (0.40–1.24) | |||||
| 3 | 0.60 (0.34–1.07) | |||||
| 4 | 0.63 (0.36–1.12) | |||||
| Moderate-intensity physical activity | 1 | 1.00 | ||||
| 2 | 0.61 (0.35–1.05) | |||||
| 3 | 0.65 (0.38–1.12) | |||||
| 4 | 0.49 (0.27–0.89) | |||||
| Vigorous intensity physical activity | No | 1.00 | ||||
| Yes | 0.70 (0.35–1.39) | |||||
| Household/caregiving physical activity | 1 | 1.00 | ||||
| 2 | 0.65 (0.37–1.14) | |||||
| 3 | 0.58 (0.32–1.03) | |||||
| 4 | 0.67 (0.38–1.18) | |||||
| Occupational physical activity | Unemployed | 1.00 | ||||
| Low | 0.92 (0.57–1.47) | |||||
| High | 0.47 (0.27–0.82) | |||||
| Sports/exercise | 1 | 1 | ||||
| 2 | 1.70 (0.64–4.52) | |||||
| 3 | 1.25 (0.77–2.03) | |||||
| 4 | 1.04 (0.62–1.74) | |||||
| Nobles C et al., 2015, USA | 2007–2012 | 124 women, exercise group: 17 cases of impaired glucose tolerance | Physical activity during pregnancy | |||
| 127 women, control group: 24 cases | Intervention to increase activity level to moderate-intensity physical activity of 30 min on most days of the week | 30 min most days of the week | 0.68 (0.35–1.34) | Education, parity |
Table 4.
Subgroup analyses of leisure-time physical activity and gestational diabetes mellitus risk, high versus low analysis
| Leisure-time physical activity before pregnancy | Leisure-time physical activity during pregnancy | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | RR (95 % CI) | I 2 (%) | P ah | P bh | n | RR (95 % CI) | I 2 (%) | P ah | P bh | |
| All studies | 8 | 0.78 (0.61–1.00) | 47.1 | 0.07 | 17 | 0.80 (0.64–1.00) | 17.0 | 0.26 | ||
| Study design | ||||||||||
| Randomized controlled trials | 0 | 0.36 | 12 | 0.69 (0.50–0.96) | 30.2 | 0.15 | 0.61 | |||
| Cohort studies | 8 | 0.78 (0.61–1.00) | 47.1 | 0.07 | 5 | 0.97 (0.73–1.28) | 0 | 0.80 | ||
| Geographic location | ||||||||||
| Europe | 2 | 0.66 (0.51–0.86) | 0 | 0.91 | 0.41 | 9 | 0.67 (0.44–1.01) | 52.0 | 0.03 | 0.88 |
| America | 5 | 0.79 (0.48–1.29) | 55.6 | 0.06 | 7 | 0.79 (0.58–1.08) | 0 | 0.94 | ||
| Asia | 0 | 0 | ||||||||
| Australia | 1 | 1.22 (0.70–2.11) | 1 | 1.44 (0.43–4.98) | ||||||
| Number of cases | ||||||||||
| Cases <200 | 5 | 0.88 (0.47–1.65) | 62.2 | 0.03 | 0.48 | 16 | 0.75 (0.59–0.96) | 13.2 | 0.30 | 0.24 |
| Cases ≥200 | 3 | 0.75 (0.64–0.88) | 0 | 0.46 | 1 | 1.04 (0.73–1.49) | ||||
| Study quality (observational studies) | ||||||||||
| 0–3 | 0 | 0.45 | 0 | 0.71 | ||||||
| 4–6 | 4 | 0.91 (0.59–1.42) | 44.6 | 0.14 | 2 | 0.83 (0.40–1.73) | 0 | 0.74 | ||
| 7–9 | 4 | 0.70 (0.48–1.01) | 59.6 | 0.06 | 3 | 0.99 (0.73–1.34) | 0 | 0.51 | ||
| Risk of bias (randomized trials) | ||||||||||
| High risk of bias | – | – | 6 | 0.62 (0.31–1.24) | 57.9 | 0.04 | 0.98 | |||
| Low risk of bias | – | 1 | 0.65 (0.27–1.55) | |||||||
| Unclear risk of bias | – | 5 | 0.74 (0.53–1.03) | 0 | 0.44 | |||||
| Adjustment for confounding factors c | ||||||||||
| Age | ||||||||||
| Yes | 8 | 0.78 (0.61–1.00) | 47.1 | 0.07 | NC | 7 | 0.84 (0.62–1.13) | 22.4 | 0.26 | NC |
| No | 0 | 0 | ||||||||
| Education | ||||||||||
| Yes | 2 | 1.23 (0.77–1.97) | 0 | 0.95 | 0.14 | 4 | 0.50 (0.21–1.24) | 56.5 | 0.08 | 0.31 |
| No | 6 | 0.70 (0.54–0.91) | 45.2 | 0.10 | 4 | 0.94 (0.70–1.26) | 0 | 0.74 | ||
| Income | ||||||||||
| Yes | 0 | NC | 0 | NC | ||||||
| No | 8 | 0.78 (0.61–1.00) | 47.1 | 0.07 | 5 | 0.96 (0.71–1.29) | 0 | 0.80 | ||
| Parity | ||||||||||
| Yes | 2 | 0.51 (0.17–1.51) | 81.6 | 0.02 | 0.33 | 3 | 0.59 (0.33–1.05) | 0 | 0.52 | 0.17 |
| No | 6 | 0.84 (0.62–1.13) | 35.9 | 0.17 | 4 | 1.02 (0.76–1.38) | 0 | 0.89 | ||
| Alcohol | ||||||||||
| Yes | 2 | 0.78 (0.65–0.93) | 0 | 0.38 | 0.82 | 0 | NC | |||
| No | 6 | 0.82 (0.51–1.30) | 59.9 | 0.03 | 5 | 0.97 (0.73–1.28) | 0 | 0.80 | ||
| Smoking | ||||||||||
| Yes | 1 | 0.81 (0.68–1.01) | 0.93 | 0 | NC | |||||
| No | 7 | 0.78 (0.55–1.10) | 53.4 | 0.05 | 5 | 0.97 (0.73–1.28) | 0 | 0.80 | ||
| Body mass index | ||||||||||
| Yes | 6 | 0.75 (0.54–1.04) | 50.3 | 0.07 | 0.71 | 7 | 0.84 (0.62–1.13) | 22.4 | 0.26 | NC |
| No | 2 | 0.87 (0.49–1.56) | 67.5 | 0.08 | 0 | |||||
n denotes the number of studies, NC not calculable
aP for heterogeneity within each subgroup
bP for heterogeneity between subgroups with meta-regression analysis
c n may not add up to the total because most of the randomized trials did not adjust for confounding factors
Total physical activity before pregnancy
Four cohort studies [26, 27, 32, 33] were included in the analysis of total physical activity (sum of leisure-time, household and occupational activity) before pregnancy and gestational diabetes mellitus and included 293 cases and 4607 participants. The summary RR for high versus low activity was 0.62 (95 % CI 0.41–0.94, I2 = 0 %, pheterogeneity = 0.88) (Fig. 2a). Because of differences in the way the results were reported it was not possible to conduct dose–response analyses of total physical activity.
Fig. 2.

Total physical activity before and during pregnancy and gestational diabetes, high versus low comparison. a Total physical activity before pregnancy and gestational diabetes mellitus, high versus low analysis. b Total physical activity during pregnancy and gestational diabetes mellitus, high versus low analysis
Total physical activity during pregnancy
Three cohort studies [27, 32, 33] were included in the analysis of total physical activity during pregnancy and gestational diabetes mellitus and included 244 cases and 3996 participants. The summary RR for high versus low activity was 0.66 (95 % CI 0.36–1.21, I2 = 0 %, pheterogeneity = 0.90) (Fig. 2b). Because of differences in the way the results were reported it was not possible to conduct dose–response analyses of total physical activity.
Leisure-time physical activity before pregnancy
Eight cohort studies [23–25, 27–30, 33] were included in the analysis of pre-pregnancy physical activity and the risk of gestational diabetes mellitus and included 2401 cases and 32,592 participants. The summary RR for high versus low pre-pregnancy physical activity was 0.78 (95 % CI 0.61–1.00, I2 = 47 %, pheterogeneity = 0.07) (Fig. 3). There was no evidence of publication bias with Egger’s test, p = 0.87. In the dose–response analysis of MET-hours/week the summary RR was 0.84 (95 % CI 0.59–1.21, I2 = 80.9 %, pheterogeneity = 0.001) per 20 MET-hours/week [23, 24, 28] (Fig. 4a) and there was no evidence of nonlinearity, p = 0.31 (Fig. 4b; Supplementary Table 2). In the dose–response analysis of hours/week the summary RR was 0.70 (95 % CI 0.49–1.01, I2 = 72.6 %, pheterogeneity = 0.03) per 5 h/week [23, 25, 31] (Fig. 4c). There was evidence of nonlinearity, pnonlinearity = 0.005, with a steeper inverse association at the lower levels of physical activity, but further reductions in risk were observed with higher levels of activity (Fig. 4d; Supplementary Table 2).
Fig. 3.

Leisure-time physical activity before pregnancy and gestational diabetes mellitus, highest versus lowest comparison
Fig. 4.
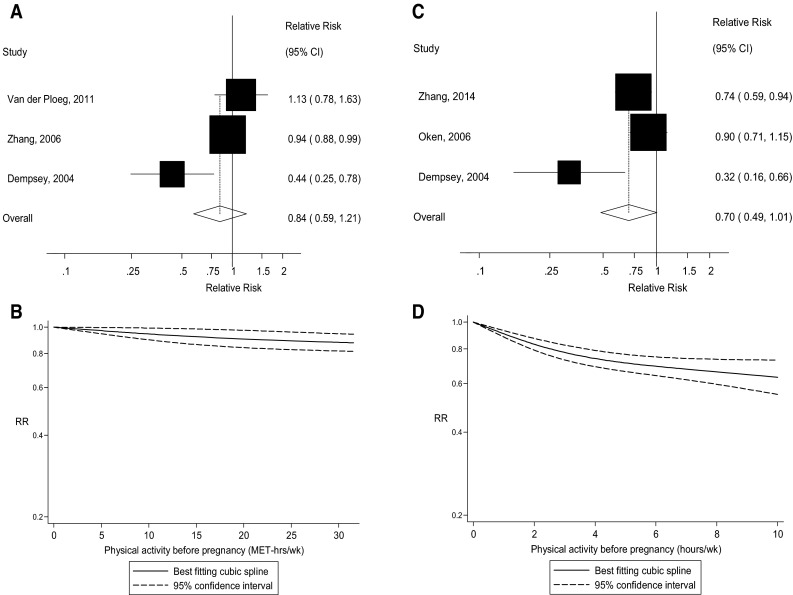
Leisure-time physical activity before pregnancy and gestational diabetes mellitus, linear (per 20 MET-hours/week and per 5 h/week) and nonlinear dose–response analysis. a Leisure-time physical activity before pregnancy and gestational diabetes mellitus, per 20 MET-hours/week. b Leisure-time physical activity before pregnancy and gestational diabetes mellitus, nonlinear dose–response, MET-hours/week. c Leisure-time physical activity before pregnancy and gestational diabetes mellitus, per 5 h/week. d Leisure-time physical activity before pregnancy and gestational diabetes mellitus, nonlinear dose–response, h/week
Leisure-time physical activity during pregnancy
Twelve randomized trials [11–22] and five cohort studies [23, 25, 27, 30, 33] were included in the analysis of early pregnancy physical activity and the risk of gestational diabetes mellitus and included 900 cases and 9804 participants. The summary RR for high versus low physical activity in early pregnancy was 0.80 (95 % CI 0.64–1.00, passociation = 0.046), with low heterogeneity, I2 = 17 %, pheterogeneity = 0.26 (Fig. 5). The summary RR was 0.69 (95 % CI 0.50–0.96, I2 = 30.2 %, pheterogeneity = 0.15) for the randomized trials and 0.97 (95 % CI 0.73–1.28, I2 = 0 %, pheterogeneity = 0.80) for the cohort studies. There was evidence of publication bias with Egger’s test, p = 0.007. We also repeated the analysis using mid-pregnancy physical activity data instead of early pregnancy data for two studies [27, 33] which provided both, and the results were slightly strengthened, summary RR = 0.75 (95 % CI 0.59–0.95, I2 = 27.7 %, pheterogeneity = 0.14). The summary RR per 5 h/week of physical activity was 0.98 (95 % CI 0.87–1.09, I2 = 0 %, pheterogeneity = 0.59) (Fig. 6c) [23, 25, 34], but there was evidence of a nonlinear inverse association, pnonlinearity = 0.008, with no further reduction in risk from approximately 7–8 h/week (Fig. 6d; Supplementary Table 2). Among the randomized trials we fitted a linear regression of the relative risks against the approximate total number of hours/week of the interventions, and although not statistically significant, p = 0.24, there was some indication of greater reductions in risk with a larger number of hours of activity (Supplementary Fig. 1). When the randomized trials were stratified by duration of activity among the studies for which we could estimate the approximate number of hours of activity per week the interventions lasted, the summary RR was 0.80 (95 % CI 0.37–1.71, n = 3) for studies with 1–2 h of activity per week, and 0.64 (0.44–0.93, n = 9) for studies with >2 h/week of activity, and 0.66 (95 % CI 0.44–1.01, n = 7) for >2–3 h/week, and 0.48 (95 % CI 0.18–1.27, n = 2) for >3 h/week.
Fig. 5.
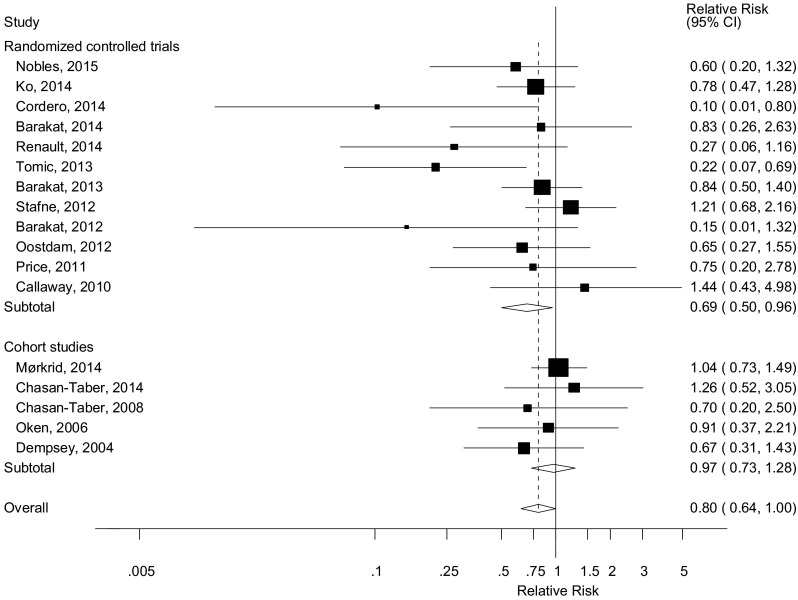
Leisure-time physical activity during early pregnancy and gestational diabetes mellitus, high versus low comparison
Fig. 6.

Leisure-time physical activity during early pregnancy and gestational diabetes mellitus, linear (per 5 h/week) and nonlinear dose–response analysis. a Leisure-time physical activity during pregnancy and gestational diabetes mellitus, per 5 h/week. b Leisure-time physical activity during pregnancy and gestational diabetes mellitus, nonlinear dose–response, h/week
Combined pre-pregnancy and early pregnancy physical activity
Two cohort studies [23, 25] investigated the association between combined physical activity before and during pregnancy and risk of gestational diabetes mellitus. The summary RR was 0.60 (95 % CI 0.30–1.23, I2 = 19.1 %, pheterogeneity = 0.27) for physical activity before pregnancy only, 1.01 (95 % CI 0.49–2.07, I2 = 0 %, pheterogeneity = 0.33) for physical activity during pregnancy only, and 0.41 (95 % CI 0.23–0.73, I2 = 0 %, pheterogeneity = 0.45) for physical activity both before and during pregnancy (Fig. 7).
Fig. 7.

Leisure-time physical activity before and during pregnancy and gestational diabetes mellitus, joint associations
Walking
Two cohort studies [24, 25] were included in the analysis of walking before pregnancy and gestational diabetes mellitus and two cohort studies [25, 30] were included in the analysis of walking during pregnancy and gestational diabetes mellitus. The summary RR was 0.66 (95 % CI 0.48–0.91, I2 = 0 %, pheterogeneity = 0.97) for walking before pregnancy (Fig. 8a). The summary RR was 0.80 (95 % CI 0.66–0.97, I2 = 0 %, pheterogeneity = 0.59) for walking during pregnancy (Fig. 8b).
Fig. 8.
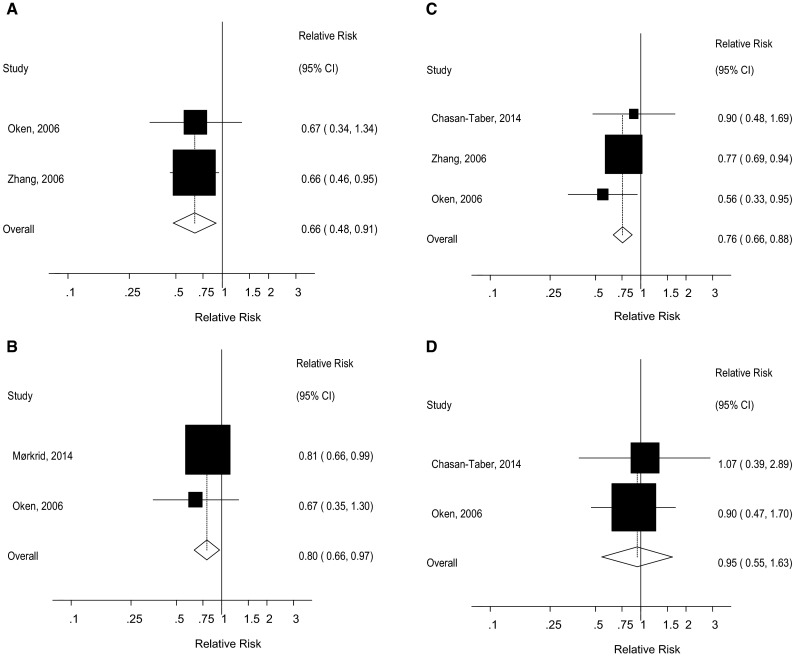
Walking and vigorous physical activity before and during pregnancy and gestational diabetes, high versus low comparison. a Walking before pregnancy and gestational diabetes mellitus, high versus low analysis. b Walking during pregnancy and gestational diabetes mellitus, high versus low analysis. c Vigorous physical activity before pregnancy and gestational diabetes mellitus, high versus low analysis. d Vigorous physical activity during pregnancy and gestational diabetes mellitus, high versus low analysis
Intensity of physical activity
Three cohort studies [24, 25, 33] investigated the association between vigorous physical activity before pregnancy and gestational diabetes mellitus, while two cohort studies [25, 33] investigated vigorous physical activity in early pregnancy and gestational diabetes mellitus. The summary RR was 0.76 (95 % CI 0.66–0.88, I2 = 0 %, pheterogeneity = 0.45) (Fig. 8c) for vigorous physical activity before pregnancy and 0.95 (95 % CI 0.55–1.63, I2 = 0 %, pheterogeneity = 0.78) (Fig. 8d) for vigorous physical activity in early pregnancy.
Occupational physical activity and household physical activity
Two cohort studies [27, 33] were included in the analysis of occupational physical activity before and during pregnancy. The summary RR for high versus low occupational physical activity was 1.90 (95 % CI 0.97–3.74, I2 = 0 %, pheterogeneity = 0.79) for activity before pregnancy (Supplementary Fig. 2a) and 0.78 (95 % CI 0.21–2.93, I2 = 78 %, pheterogeneity = 0.03) for activity during pregnancy (Supplementary Fig. 2b). Two cohort studies [27, 33] were included in the analysis of household physical activity before and during pregnancy. The summary RR for high versus low household physical activity was 0.36 (95 % CI 0.12–1.08, I2 = 61.9 %, pheterogeneity = 0.11) for activity before pregnancy (Supplementary Fig. 3a) and 1.22 (95 % CI 0.53–2.81, I2 = 23.6 %, pheterogeneity = 0.25) for activity during pregnancy (Supplementary Fig. 3b).
Physical activity and abnormal glucose tolerance
We conducted supplementary analyses of one randomized trial [22] and five cohort studies [25, 33, 39, 44, 45] which reported on physical activity and abnormal glucose tolerance as an outcome and the summary RRs were 0.81 (95 % CI 0.55–1.17, I2 = 34 % pheteroeneity = 0.21) for pre-pregnancy physical activity [25, 33, 39, 44] (Supplementary Fig. 4a) and 0.77 (95 % CI 0.63–0.95, I2 = 0 % pheteroeneity = 0.76) for physical activity during pregnancy [22, 25, 33, 44, 45], respectively (Supplementary Fig. 4b).
Subgroup, sensitivity, and meta-regression analyses
In subgroup and meta-regression analyses we found no significant heterogeneity between subgroups when studies were stratified by study design, geographic location, number of cases, study quality (cohort studies) or risk of bias (randomized trials) (Table 4). Further subgroup analyses by whether studies had adjusted for confounding factors did not reveal significant heterogeneity between most strata, although associations were not always statistically significant. We also conducted sensitivity analyses excluding one study at a time in the analyses of leisure-time physical activity, and although the summary relative risks did not vary substantially exclusion of some studies made the borderline significant associations statistically significant (Supplementary Figures 5, 6).
Mean (median) study quality scores were 7.0 (6.5) for cohort studies of leisure-time physical activity before pregnancy and 7.0 (7.0) for cohort studies of leisure-time physical activity during pregnancy. Of the 12 randomized trials 6 were deemed to be of high risk of bias, 1 of low risk of bias and 5 of unclear risk of bias.
We conducted further analyses of three studies on physical activity before pregnancy [23, 24, 27] and three studies on physical activity during pregnancy [23, 24, 27] and gestational diabetes mellitus which provided risk estimates adjusted and not adjusted for BMI, to clarify whether part of the association might be explained by reduced body fatness. The summary RR for pre-pregnancy physical activity was 0.63 (95 % CI 0.23–1.71) without BMI adjustment and 0.72 (95 % CI 0.30–1.76) with BMI adjustment, while for physical activity during pregnancy it was 0.49 (95 % CI 0.29–0.83) without BMI adjustment and 0.56 (95 % CI 0.33–0.95) with BMI adjustment.
Discussion
In this meta-analysis higher leisure-time physical activity before and during pregnancy was associated with a marginally significant 22 % reduction and 20 % reduction in the relative risk of gestational diabetes mellitus, respectively. Higher total physical activity before pregnancy was associated with a 36 % reduction in the relative risk of gestational diabetes, while the association for total physical activity during pregnancy was in the direction of reduced risk, but was not statistically significant, possibly due to few studies. Walking before and during pregnancy and vigorous activity before pregnancy were also inversely associated with gestational diabetes, but occupational and household physical activity were not associated with risk, although these results were based on few studies.
When stratified by study design the association between leisure-time physical activity during pregnancy and gestational diabetes was significant in randomized trials, but not significant in cohort studies. As the studies differed with regard to the level of physical activity level between studies it is difficult to base physical activity recommendations on the results from the high versus low analyses, and therefore we also conducted linear and nonlinear dose–response analyses. In the nonlinear dose–response analysis there was a 12 % reduction in the relative risk of gestational diabetes mellitus for 30 MET-hours of pre-pregnancy physical activity per week compared to no activity, and a 30 % reduction in risk for 7 h of pre-pregnancy activity per week compared to no activity, and for physical activity during pregnancy there was a 37 % reduction in the relative risk for 7 h of activity per week compared to no activity. In analyses of combined pre-pregnancy and early pregnancy physical activity there was a suggestive 40 % reduction in risk among women who were physically active before pregnancy, but no association among women who were active only during early pregnancy, while there was a 59 % reduction in relative risk for women who were physically active before and during pregnancy compared to women who were inactive in both periods. An interesting finding of the present meta-analysis is that some of the associations were stronger for pre-pregnancy physical activity than for physical activity during pregnancy, which is similar to the findings in our meta-analysis on physical activity and preeclampsia [53]. This is not unreasonable as the time available to intervene, and the degree of physical activity that is achievable is more limited in pregnancy. In addition, the physiologic insulin-resistance in pregnancy could attenuate the effects of physical activity during pregnancy. However, as this was not entirely consistently observed across the various physical activity exposures, further studies with both prepregnancy and early pregnancy physical activity measures are needed for further clarification.
The results from this meta-analysis provide further support for the hypothesis that physical activity decreases the risk of gestational diabetes mellitus and are consistent with two previous meta-analyses which also found inverse association [41, 43], but not with a third [42]. However, in contrast to the previous meta-analyses we further quantified the association between physical activity and gestational diabetes mellitus risk by conducting linear and nonlinear dose–response analyses and conducted more detailed analyses of different domains of activity. Such analyses are important to guide recommendations to pregnant women with regard to the amount and types of physical activity that may reduce risk, as well as to inform future physical activity interventions that aim to reduce gestational diabetes risk.
Our meta-analysis may have some limitations that could have affected the results. It is possible that the observed inverse association between physical activity and risk of gestational diabetes mellitus risk could be due to unmeasured or residual confounding. Higher physical activity is associated with other healthy behaviors including lower prevalence of overweight and obesity and healthier diets with higher dietary fiber intake, and lower red and processed meat intake. However, many of the studies included in this meta-analysis adjusted for confounding factors such as age, BMI, and energy intake and the associations persisted in subgroup analyses by stratification by adjustment for these confounding variables. We found no evidence of heterogeneity between these subgroups with meta-regression analyses. Any further studies should adjust for more dietary confounding factors. There was moderate heterogeneity among studies of leisure-time activity before pregnancy (I2 = 47 %), but when stratified by number of cases there was no heterogeneity among studies with 200 or more cases (I2 = 0 %), although there was no between subgroup heterogeneity with meta-regression analyses. Among studies of leisure-time physical activity during pregnancy there was low heterogeneity (I2 = 17 %). For some other subtypes of activity there was high heterogeneity, but there were not enough studies to conduct subgroup and meta-regression analyses, or to test for publication bias and conduct other sensitivity analyses for the subtypes of physical activity. Not all the studies included in the high versus low analysis could be included in the dose–response analyses because results either were reported using a different underlying measure than others or because there was only a dichotomized categorization of physical activity. Any further studies should report the results for 3–4 or more categories of activity and use a measure that allows for combination with other studies, preferably in hours/week and/or MET-hours/week. In addition, some of the randomized trials may have had a dose of physical activity that was too low (1–2 h/week) to observe an association, particularly because of the possibility of contamination of the control group. In subgroup analyses of the randomized trials there was some suggestion of a stronger association among studies with an estimated duration of >2–3 and >3 h/week of activity than among those with an estimated duration of 1–2 h/week. In addition to the activity level being too low, the compliance with the exercise interventions may have been poor in some studies, which may have attenuated any associations. A challenge for future intervention studies will be to increase both the duration of the activity and the compliance with the interventions. In addition, much larger studies are needed as few of the randomized trials found statistically significant reductions in risk individually. As a meta-analysis of published studies publication bias may also have affected the results. There was evidence of publication bias in the analysis of leisure-time physical activity during pregnancy and risk of gestational diabetes, thus it is possible that this could have led to an exaggerated summary estimate.
Gestational diabetes and type 2 diabetes share many pathophysiological features and our previous findings of an inverse association between physical activity and type 2 diabetes [10] support the current results on gestational diabetes. Interestingly the strength and the shape of the dose–response relationships observed between leisure-time physical activity in relation to gestational diabetes and type 2 diabetes is similar with an approximate 20–30 % reduction in the relative risk observed with 5–7 h/week compared to no activity, and with a steeper reduction in the risk at lower levels of activity. Most likely several of the same mechanistic pathways are involved in explaining these results for gestational diabetes mellitus as for type 2 diabetes. Physical activity reduces adiposity [59] and has been associated with lower gestational weight gain [60–62], which is strongly related to increased risk of gestational diabetes mellitus [63]. Overweight and obesity increases inflammation, flux of free fatty acids, and may thereby lead to insulin resistance [64], which in turn increases the endogenous glucose production in the liver, while physical activity may counteract some of these adverse effects [25, 65]. In this analysis, we found that associations were 14–25 % weaker when adjusted for BMI compared with when not adjusted for BMI, suggesting that approximately 14–25 % of the association may be explained by reduced adiposity, and this is comparable with our previous meta-analysis on physical activity and type 2 diabetes where associations were 20–30 % weaker when adjusted for BMI compared with analyses not adjusted for BMI [10]. However, a clinically significant reduction remained after adjustment for BMI, suggesting that other mechanisms may be implicated. We also found a significant inverse association between pre-pregnancy physical activity and abnormal glucose tolerance. Physical activity increases glucose uptake and glycogen synthesis through increased glucose transport by the GLUT4 glucose transporters and increased activity of glycogen synthase [65]. Exercise increases the secretion of interleukin-6 (IL-6) from muscle cells, which has anti-inflammatory effects through inhibition of TNF-α and IL-1β, and reduces TNF-induced insulin resistance [65]. Physical activity has been associated with lower levels of total cholesterol, triglycerides, leptin, and improved glycemic control and reduced insulin resistance in pregnant women [25, 66–68]. The biological mechanism explaining the potential nonlinear association observed between physical activity and gestational diabetes mellitus is not clear and needs further study. In previous meta-analyses we have also observed similar nonlinear associations between physical activity and preeclampsia [53] and type 2 diabetes [10], with steeper reductions in risk at lower levels of activity, however, for all these three conditions reductions in risk have been observed up to between 5 and 7 h of activity per week. Given the similarities in the underlying pathophysiological features of preeclampsia, type 2 diabetes and gestational diabetes mellitus (e.g. insulin resistance, obesity), it is possible that some of the underlying mechanisms that may be common for all three conditions also partly could explain the nonlinearity. However, we can also not rule out the possibility that the nonlinearity partly could be due to few data points at higher levels of physical activity.
Our meta-analysis also has several strengths. Because we only included cohort studies and randomized trials, recall bias is not an issue and there is less potential for selection bias. We conducted dose–response analyses to investigate whether specific levels of physical activity were associated with gestational diabetes mellitus risk and found evidence of a dose–response relationship. Because of the increased sample size we had higher statistical power to detect an association than any individual study, however, most of the included studies had a moderate or small sample size. The quality of the cohort studies were in general high (mean scores of 7 out of 9 points), however, half of the randomized trials were at high risk of bias, and most of the remaining were at unclear risk of bias. Although, there was no heterogeneity by study quality scores or the risk of bias assessment when stratified, any future studies should improve the conduct and reporting of the results to provide better epidemiological evidence on physical activity and gestational diabetes mellitus.
Further large cohort studies and intervention trials are needed to conclusively establish the association between physical activity and specific types and intensities of physical activity and gestational diabetes, and for updated dose–response analyses it would be good if future studies could report results on a common scale, for example in hours/week and/or MET-hours/week. Any further intervention trials should aim to use a high enough dose or frequency of physical activity to be able to observe an effect (e.g. at least 2–3 h or more per week) and including multiple arms with different levels of physical activity might provide firm conclusions with regard to the dose–response relationship.
In conclusion, our results suggest that higher physical activity is associated with reduced risk of gestational diabetes mellitus. Any additional studies should assess the association between specific subtypes, amounts and intensities of physical activity and risk of gestational diabetes mellitus, adjust for more confounding factors and improve the reporting of the data.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgments
This project has been funded by Liaison Committee between the Central Norway Regional Health Authority (RHA) and the Norwegian University of Science and Technology (NTNU) and the Imperial College National Institute of Health Research (NIHR) Biomedical Research Centre (BRC). The funding organizations had no role in the conduct of the analyses, interpretation, or manuscript preparation. We thank Dr. Darren C. Greenwood (Biostatistics Unit, Centre for Epidemiology and Biostatistics, University of Leeds, Leeds, UK) for providing the Stata code for the nonlinear dose–response analyses.
Authors’ contribution
D.A. designed the project, conducted the literature search and statistical analyses and wrote the first draft of the paper. D.A. and A.S. conducted the study selection. D.A., T.H., A.S., S.T., and O.D.S. interpreted the data, revised the subsequent drafts for important intellectual content and approved the final version of the paper to be published.
Compliance with ethical standards
Conflict of interest
None.
References
- 1.Shand AW, Bell JC, McElduff A, Morris J, Roberts CL. Outcomes of pregnancies in women with pre-gestational diabetes mellitus and gestational diabetes mellitus: a population-based study in New South Wales, Australia, 1998–2002. Diabet Med. 2008;25:708–715. doi: 10.1111/j.1464-5491.2008.02431.x. [DOI] [PubMed] [Google Scholar]
- 2.Diabetes in pregnancy: management of diabetes and its complications from preconception to the postnatal period. NICE Clinical Guideline (February 2015) 2015. [PubMed]
- 3.Hartling L, Dryden DM, Guthrie A, Muise M, Vandermeer B, Donovan L. Diagnostic thresholds for gestational diabetes and their impact on pregnancy outcomes: a systematic review. Diabet Med. 2014;31:319–331. doi: 10.1111/dme.12357. [DOI] [PubMed] [Google Scholar]
- 4.Ferrara A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care. 2007;30(Suppl 2):S141–S146. doi: 10.2337/dc07-s206. [DOI] [PubMed] [Google Scholar]
- 5.Chu SY, Callaghan WM, Kim SY, et al. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care. 2007;30:2070–2076. doi: 10.2337/dc06-2559a. [DOI] [PubMed] [Google Scholar]
- 6.Torloni MR, Betran AP, Horta BL, et al. Prepregnancy BMI and the risk of gestational diabetes: a systematic review of the literature with meta-analysis. Obes Rev. 2009;10:194–203. doi: 10.1111/j.1467-789X.2008.00541.x. [DOI] [PubMed] [Google Scholar]
- 7.Choi SK, Park IY, Shin JC. The effects of pre-pregnancy body mass index and gestational weight gain on perinatal outcomes in Korean women: a retrospective cohort study. Reprod Biol Endocrinol. 2011;9:6. doi: 10.1186/1477-7827-9-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Leung TY, Leung TN, Sahota DS, et al. Trends in maternal obesity and associated risks of adverse pregnancy outcomes in a population of Chinese women. BJOG. 2008;115:1529–1537. doi: 10.1111/j.1471-0528.2008.01931.x. [DOI] [PubMed] [Google Scholar]
- 9.Rana JS, Li TY, Manson JE, Hu FB. Adiposity compared with physical inactivity and risk of type 2 diabetes in women. Diabetes Care. 2007;30:53–58. doi: 10.2337/dc06-1456. [DOI] [PubMed] [Google Scholar]
- 10.Aune D, Norat T, Leitzmann M, Tonstad S, Vatten LJ. Physical activity and the risk of type 2 diabetes: a systematic review and dose–response meta-analysis. Eur J Epidemiol. 2015;30:529–542. doi: 10.1007/s10654-015-0056-z. [DOI] [PubMed] [Google Scholar]
- 11.Callaway LK, Colditz PB, Byrne NM, et al. Prevention of gestational diabetes: feasibility issues for an exercise intervention in obese pregnant women. Diabetes Care. 2010;33:1457–1459. doi: 10.2337/dc09-2336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Price BB, Amini SB, Kappeler K. Exercise in pregnancy: effect on fitness and obstetric outcomes—a randomized trial. Med Sci Sports Exerc. 2012;44:2263–2269. doi: 10.1249/MSS.0b013e318267ad67. [DOI] [PubMed] [Google Scholar]
- 13.Oostdam N, van Poppel MN, Wouters MG, et al. No effect of the FitFor2 exercise programme on blood glucose, insulin sensitivity, and birthweight in pregnant women who were overweight and at risk for gestational diabetes: results of a randomised controlled trial. BJOG. 2012;119:1098–1107. doi: 10.1111/j.1471-0528.2012.03366.x. [DOI] [PubMed] [Google Scholar]
- 14.Stafne SN, Salvesen KA, Romundstad PR, Eggebo TM, Carlsen SM, Morkved S. Regular exercise during pregnancy to prevent gestational diabetes: a randomized controlled trial. Obstet Gynecol. 2012;119:29–36. doi: 10.1097/AOG.0b013e3182393f86. [DOI] [PubMed] [Google Scholar]
- 15.Barakat R, Cordero Y, Coteron J, Luaces M, Montejo R. Exercise during pregnancy improves maternal glucose screen at 24–28 weeks: a randomised controlled trial. Br J Sports Med. 2012;46:656–661. doi: 10.1136/bjsports-2011-090009. [DOI] [PubMed] [Google Scholar]
- 16.Tomic V, Sporis G, Tomic J, Milanovic Z, Zigmundovac-Klaic D, Pantelic S. The effect of maternal exercise during pregnancy on abnormal fetal growth. Croat Med J. 2013;54:362–368. doi: 10.3325/cmj.2013.54.362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Barakat R, Pelaez M, Lopez C, Lucia A, Ruiz JR. Exercise during pregnancy and gestational diabetes-related adverse effects: a randomised controlled trial. Br J Sports Med. 2013;47:630–636. doi: 10.1136/bjsports-2012-091788. [DOI] [PubMed] [Google Scholar]
- 18.Barakat R, Perales M, Bacchi M, Coteron J, Refoyo I. A program of exercise throughout pregnancy. Is it safe to mother and newborn? Am J Health Promot. 2014;29:2–8. doi: 10.4278/ajhp.130131-QUAN-56. [DOI] [PubMed] [Google Scholar]
- 19.Renault KM, Norgaard K, Nilas L, et al. The treatment of obese pregnant women (TOP) study: a randomized controlled trial of the effect of physical activity intervention assessed by pedometer with or without dietary intervention in obese pregnant women. Am J Obstet Gynecol. 2014;210:134–139. doi: 10.1016/j.ajog.2013.09.029. [DOI] [PubMed] [Google Scholar]
- 20.Ko CW, Napolitano PG, Lee SP, Schulte SD, Ciol MA, Beresford SA. Physical activity, maternal metabolic measures, and the incidence of gallbladder sludge or stones during pregnancy: a randomized trial. Am J Perinatol. 2014;31:39–48. doi: 10.1055/s-0034-1384641. [DOI] [PubMed] [Google Scholar]
- 21.Cordero Y, Mottola MF, Vargas J, Blanco M, Barakat R. Exercise is associated with a reduction in gestational diabetes mellitus. Med Sci Sports Exerc. 2015;47:1328–1333. doi: 10.1249/MSS.0000000000000547. [DOI] [PubMed] [Google Scholar]
- 22.Nobles C, Marcus BH, Stanek EJ, III, et al. Effect of an exercise intervention on gestational diabetes mellitus: a randomized controlled trial. Obstet Gynecol. 2015;125:1195–1204. doi: 10.1097/AOG.0000000000000738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dempsey JC, Sorensen TK, Williams MA, et al. Prospective study of gestational diabetes mellitus risk in relation to maternal recreational physical activity before and during pregnancy. Am J Epidemiol. 2004;159:663–670. doi: 10.1093/aje/kwh091. [DOI] [PubMed] [Google Scholar]
- 24.Zhang C, Solomon CG, Manson JE, Hu FB. A prospective study of pregravid physical activity and sedentary behaviors in relation to the risk for gestational diabetes mellitus. Arch Intern Med. 2006;166:543–548. doi: 10.1001/archinte.166.5.543. [DOI] [PubMed] [Google Scholar]
- 25.Oken E, Ning Y, Rifas-Shiman SL, Radesky JS, Rich-Edwards JW, Gillman MW. Associations of physical activity and inactivity before and during pregnancy with glucose tolerance. Obstet Gynecol. 2006;108:1200–1207. doi: 10.1097/01.AOG.0000241088.60745.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Iqbal R, Rafique G, Badruddin S, Qureshi R, Cue R, Gray-Donald K. Increased body fat percentage and physical inactivity are independent predictors of gestational diabetes mellitus in South Asian women. Eur J Clin Nutr. 2007;61:736–742. doi: 10.1038/sj.ejcn.1602574. [DOI] [PubMed] [Google Scholar]
- 27.Chasan-Taber L, Schmidt MD, Pekow P, et al. Physical activity and gestational diabetes mellitus among Hispanic women. J Womens Health (Larchmt) 2008;17:999–1008. doi: 10.1089/jwh.2007.0560. [DOI] [PubMed] [Google Scholar]
- 28.van der Ploeg HP, van Poppel MN, Chey T, Bauman AE, Brown WJ. The role of pre-pregnancy physical activity and sedentary behaviour in the development of gestational diabetes mellitus. J Sci Med Sport. 2011;14:149–152. doi: 10.1016/j.jsams.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 29.Ramos-Levi AM, Perez-Ferre N, Fernandez MD, et al. Risk factors for gestational diabetes mellitus in a large population of women living in Spain: implications for preventative strategies. Int J Endocrinol. 2012;2012:312529. doi: 10.1155/2012/312529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Morkrid K, Jenum AK, Berntsen S, et al. Objectively recorded physical activity and the association with gestational diabetes. Scand J Med Sci Sports. 2014;24:e389–e397. doi: 10.1111/sms.12183. [DOI] [PubMed] [Google Scholar]
- 31.Zhang C, Tobias DK, Chavarro JE, et al. Adherence to healthy lifestyle and risk of gestational diabetes mellitus: prospective cohort study. BMJ. 2014;349:g5450. doi: 10.1136/bmj.g5450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Currie LM, Woolcott CG, Fell DB, Armson BA, Dodds L. The association between physical activity and maternal and neonatal outcomes: a prospective cohort. Matern Child Health J. 2014;18:1823–1830. doi: 10.1007/s10995-013-1426-3. [DOI] [PubMed] [Google Scholar]
- 33.Chasan-Taber L, Silveira M, Lynch KE, et al. Physical activity before and during pregnancy and risk of abnormal glucose tolerance among Hispanic women. Diabetes Metab. 2014;40:67–75. doi: 10.1016/j.diabet.2013.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dempsey JC, Butler CL, Sorensen TK, et al. A case–control study of maternal recreational physical activity and risk of gestational diabetes mellitus. Diabetes Res Clin Pract. 2004;66:203–215. doi: 10.1016/j.diabres.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 35.Liu J, Laditka JN, Mayer-Davis EJ, Pate RR. Does physical activity during pregnancy reduce the risk of gestational diabetes among previously inactive women? Birth. 2008;35:188–195. doi: 10.1111/j.1523-536X.2008.00239.x. [DOI] [PubMed] [Google Scholar]
- 36.Harizopoulou VC, Kritikos A, Papanikolaou Z, et al. Maternal physical activity before and during early pregnancy as a risk factor for gestational diabetes mellitus. Acta Diabetol. 2010;47(Suppl 1):83–89. doi: 10.1007/s00592-009-0136-1. [DOI] [PubMed] [Google Scholar]
- 37.Redden SL, LaMonte MJ, Freudenheim JL, Rudra CB. The association between gestational diabetes mellitus and recreational physical activity. Matern Child Health J. 2011;15:514–519. doi: 10.1007/s10995-010-0586-7. [DOI] [PubMed] [Google Scholar]
- 38.Rudra CB, Williams MA, Lee IM, Miller RS, Sorensen TK. Perceived exertion in physical activity and risk of gestational diabetes mellitus. Epidemiology. 2006;17:31–37. doi: 10.1097/01.ede.0000184474.33629.cd. [DOI] [PubMed] [Google Scholar]
- 39.Baptiste-Roberts K, Ghosh P, Nicholson WK. Pregravid physical activity, dietary intake, and glucose intolerance during pregnancy. J Womens Health (Larchmt) 2011;20:1847–1851. doi: 10.1089/jwh.2010.2377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Campbell SK, Lynch J, Esterman A, McDermott R. Pre-pregnancy predictors of diabetes in pregnancy among Aboriginal and Torres Strait Islander women in North Queensland, Australia. Matern Child Health J. 2012;16:1284–1292. doi: 10.1007/s10995-011-0889-3. [DOI] [PubMed] [Google Scholar]
- 41.Tobias DK, Zhang C, van Dam RM, Bowers K, Hu FB. Physical activity before and during pregnancy and risk of gestational diabetes mellitus: a meta-analysis. Diabetes Care. 2011;34:223–229. doi: 10.2337/dc10-1368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Yin YN, Li XL, Tao TJ, Luo BR, Liao SJ. Physical activity during pregnancy and the risk of gestational diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2014;48:290–295. doi: 10.1136/bjsports-2013-092596. [DOI] [PubMed] [Google Scholar]
- 43.Russo LM, Nobles C, Ertel KA, Chasan-Taber L, Whitcomb BW. Physical activity interventions in pregnancy and risk of gestational diabetes mellitus: a systematic review and meta-analysis. Obstet Gynecol. 2015;125:576–582. doi: 10.1097/AOG.0000000000000691. [DOI] [PubMed] [Google Scholar]
- 44.Gollenberg AL, Pekow P, Bertone-Johnson ER, Freedson PS, Markenson G, Chasan-Taber L. Sedentary behaviors and abnormal glucose tolerance among pregnant Latina women. Med Sci Sports Exerc. 2010;42:1079–1085. doi: 10.1249/MSS.0b013e3181c6dec8. [DOI] [PubMed] [Google Scholar]
- 45.Deierlein AL, Siega-Riz AM, Evenson KR. Physical activity during pregnancy and risk of hyperglycemia. J Womens Health (Larchmt) 2012;21:769–775. doi: 10.1089/jwh.2011.3361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Wells G, Shea B, O’Connell D, et al. The Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 13 Aug 2014.
- 47.Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 49.Greenland S, Longnecker MP. Methods for trend estimation from summarized dose–response data, with applications to meta-analysis. Am J Epidemiol. 1992;135:1301–1309. doi: 10.1093/oxfordjournals.aje.a116237. [DOI] [PubMed] [Google Scholar]
- 50.Aune D, Greenwood DC, Chan DS, et al. Body mass index, abdominal fatness and pancreatic cancer risk: a systematic review and non-linear dose–response meta-analysis of prospective studies. Ann Oncol. 2012;23:843–852. doi: 10.1093/annonc/mdr398. [DOI] [PubMed] [Google Scholar]
- 51.Aune D, Chan DS, Lau R, et al. Dietary fibre, whole grains, and risk of colorectal cancer: systematic review and dose–response meta-analysis of prospective studies. BMJ. 2011;343:d6617. doi: 10.1136/bmj.d6617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 Compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43:1575–1581. doi: 10.1249/MSS.0b013e31821ece12. [DOI] [PubMed] [Google Scholar]
- 53.Aune D, Saugstad OD, Henriksen T, Tonstad S. Physical activity and the risk of preeclampsia: a systematic review and meta-analysis. Epidemiology. 2014;25:331–343. doi: 10.1097/EDE.0000000000000036. [DOI] [PubMed] [Google Scholar]
- 54.Orsini N, Li R, Wolk A, Khudyakov P, Spiegelman D. Meta-analysis for linear and nonlinear dose–response relations: examples, an evaluation of approximations, and software. Am J Epidemiol. 2012;175:66–73. doi: 10.1093/aje/kwr265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Jackson D, White IR, Thompson SG. Extending DerSimonian and Laird’s methodology to perform multivariate random effects meta-analyses. Stat Med. 2010;29:1282–1297. doi: 10.1002/sim.3602. [DOI] [PubMed] [Google Scholar]
- 56.Royston P. A strategy for modelling the effect of a continuous covariate in medicine and epidemiology. Stat Med. 2000;19:1831–1847. doi: 10.1002/1097-0258(20000730)19:14<1831::AID-SIM502>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- 57.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–560. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Mozaffarian D, Hao T, Rimm EB, Willett WC, Hu FB. Changes in diet and lifestyle and long-term weight gain in women and men. N Engl J Med. 2011;364:2392–2404. doi: 10.1056/NEJMoa1014296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Haakstad LA, Voldner N, Henriksen T, Bo K. Physical activity level and weight gain in a cohort of pregnant Norwegian women. Acta Obstet Gynecol Scand. 2007;86:559–564. doi: 10.1080/00016340601185301. [DOI] [PubMed] [Google Scholar]
- 61.Haakstad LA, Bo K. Effect of regular exercise on prevention of excessive weight gain in pregnancy: a randomised controlled trial. Eur J Contracept Reprod Health Care. 2011;16:116–125. doi: 10.3109/13625187.2011.560307. [DOI] [PubMed] [Google Scholar]
- 62.Jiang H, Qian X, Li M, et al. Can physical activity reduce excessive gestational weight gain? Findings from a Chinese urban pregnant women cohort study. Int J Behav Nutr Phys Act. 2012;9:12. doi: 10.1186/1479-5868-9-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Rudra CB, Sorensen TK, Leisenring WM, Dashow E, Williams MA. Weight characteristics and height in relation to risk of gestational diabetes mellitus. Am J Epidemiol. 2007;165:302–308. doi: 10.1093/aje/kwk007. [DOI] [PubMed] [Google Scholar]
- 64.Friis CM, Paasche Roland MC, Godang K, et al. Adiposity-related inflammation: effects of pregnancy. Obesity (Silver Spring) 2013;21:E124–E130. doi: 10.1002/oby.20120. [DOI] [PubMed] [Google Scholar]
- 65.Golbidi S, Laher I. Potential mechanisms of exercise in gestational diabetes. J Nutr Metab. 2013;2013:285948. doi: 10.1155/2013/285948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Butler CL, Williams MA, Sorensen TK, Frederick IO, Leisenring WM. Relation between maternal recreational physical activity and plasma lipids in early pregnancy. Am J Epidemiol. 2004;160:350–359. doi: 10.1093/aje/kwh223. [DOI] [PubMed] [Google Scholar]
- 67.Ning Y, Williams MA, Butler CL, Muy-Rivera M, Frederick IO, Sorensen TK. Maternal recreational physical activity is associated with plasma leptin concentrations in early pregnancy. Hum Reprod. 2005;20:382–389. doi: 10.1093/humrep/deh615. [DOI] [PubMed] [Google Scholar]
- 68.Clapp JF. Effects of diet and exercise on insulin resistance during pregnancy. Metab Syndr Relat Disord. 2006;4:84–90. doi: 10.1089/met.2006.4.84. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.