

Abstract
Children who exhibit elevated levels of the temperament trait behavioural inhibition (BI) across time may be at greatest risk for anxiety. However, little research has investigated the influence of other temperamental traits, particularly positive emotionality (PE), on the continuity of BI in childhood, nor whether parental overprotection influences associations between early and later child BI. To explore whether PE and overprotection shape associations between early and later BI, this longitudinal study of three-year-olds (N = 446) followed up at age 6 included tasks tapping child temperament, and parental overprotection was assessed via interview ratings and parent-report. Lower levels of child PE and higher levels of caregiver overprotection at baseline predicted stronger associations between laboratory-assessed BI at ages 3 and 6. Findings elucidate influences shaping the developmental continuity of BI.
Keywords: behavioural inhibition, positive emotionality, child temperament, parenting
Behavioural inhibition (BI) is a temperament trait that refers to individual differences in fearfulness and reticence in the context of novel social and non-social situations (e.g., Fox, Henderson, Marshall, Nichols, & Ghera, 2005). Temperament researchers and developmental psychopathologists have a longstanding interest in BI, given its associations with various internalizing disorders (e.g., Rotge et al., 2011). For example, a recent meta-analysis found a greater than sevenfold increase in risk for developing social anxiety disorder among individuals with elevated BI (Claus & Blackford, 2012). This heightened risk has been found in studies using different methods and measures, including longitudinal studies (e.g., Hirshfeld-Becker et al., 2007).
A considerable body of research establishes the trait-like (i.e., stable) properties of BI. For example, Gest (1997) found evidence for the stability of interviewer-rated BI in both childhood and adolescence, reporting an average correlation of.57 between BI scores across 5.5-year follow-ups, and Scarpa, Raine, Venables, and Mednick (1995) reported moderate stability of informant-and observer-rated BI assessed from toddlerhood to late childhood. However, there is also evidence for change in BI over time, such that some children transition from being relatively inhibited to being less so, and vice-versa (e.g., Essex, Klein, Slattery, Goldsmith, & Kalin, 2010; Rubin, Burgess, & Hastings, 2002). Understanding factors that account for such shifts is important given evidence that it is the persistence of elevated BI over time that marks children’s risk for anxiety more so than elevated BI at a single time point. For example, Chronis-Tuscano et al. (2009) assessed maternal reports of BI in infancy and early childhood, finding that stable, elevated BI was related to elevated risk for social anxiety in adolescence; children with maternally reported BI in the top one-third of the sample across all four time points (i.e., 14 months, 24 months, 4 years, and 7 years) showed a nearly four times increased risk for a social anxiety disorder diagnosis at ages 14–16 compared to children in the bottom two-thirds. Essex, Slattery, Goldsmith, Hill, and Kalin (2010) observed similar findings, finding that persistently high inhibition (i.e., BI scores in the upper 25% of the sample at a minimum of four of the five assessments, and no BI score in the lower 25% of the sample) was associated with greater risk for social anxiety disorder in adolescence (Essex et al., 2010). Therefore, stably elevated BI seems especially relevant to risk for anxiety disorders.
A greater understanding of factors that influence the course of BI over time would help identify those children at greatest temperamental risk for anxiety, and could potentially inform prevention and early intervention strategies that are targeted and cost-effective. Other temperament/personality traits, particularly those contributing to engagement with novel environmental stimuli, may influence BI over time. For example, positive emotionality (PE) includes positive affect, approach-related and exploratory behaviours, and interest and engagement with the environment as important facets (e.g., Laptook, Klein, Olino, Dyson, & Carlson, 2010). Children who are initially high in both BI and PE may become less inhibited over time as elevated PE facilitates exposure and acclimatization to novelty. This would be consistent with conceptually related models; for example, Gray (1970) described two orthogonal motivation systems, the Behavioral Inhibition System (BIS) and the Behavioral Activation System (BAS), linking BIS to negative affect and fearful responding, and BAS to extraversion and positive affect (e.g., Coplan, Wilson, Frohlick, & Zelenski, 2006. In Gray’s model, these systems control avoidance and approach and jointly influence behavioural outcomes. Relatedly, Asendorf (1990) suggested that shy children are caught in an approach-avoidance conflict and their subsequent inhibited or uninhibited behaviour depends on the result of this conflict. Further, models positing such trait interactions are consistent with research indicating a weakened association between shyness and internalizing problems in young boys with elevated levels of both shyness and activity levels, which suggests that increased activity levels may buffer the risk of internalizing disorders associated with elevated shyness (Karevold, Coplan, Stoolmiller, & Mathiesen, 2011).
Also relevant is the small literature indicating that high PE buffers the impact of other vulnerabilities to negative outcomes (Clark, 2005; Mackrell et al., 2014; Park, Belsky, Putnam, & Crnic, 1997; Tugade & Fredrickson, 2004; Wichers et al., 2007; see Davis & Suveg, 2014 for a comprehensive review). For example, Mackrell et al. (2014) found that high PE in children interacted with maternal depression to predict lower cortisol stress reactivity in children, and Wichers et al. (2007) found that high positive affect buffered negative affect reactivity to stress. Like BI, PE appears moderately stable in childhood (e.g., Davis & Suveg, 2014; Durbin, Hayden, Klein, & Olino, 2007). However, we are unaware of any studies examining whether PE and BI interact to predict later BI, despite separate literatures on the stability of these traits. Indeed, Rothbart and Bates (2006) noted the lack of empirical studies examining interactions between multiple temperament traits; as temperament traits do not exist in isolation within an individual, they emphasized the importance of examining how traits work together to shape outcomes. They suggested that fearful temperament might differentially influence an individual’s socio-emotional adjustment based on other temperament traits present within the individual (e.g., tendency toward dysregulation) as well as environmental factors (Rothbart & Bates, 2006). Increased understanding of interactions between temperament traits, particularly BI and PE, could provide a broader understanding of factors that contribute to child risk and resilience, with both theoretical and practical implications.
Like PE, certain parenting behaviours might serve to either facilitate or suppress children’s exploratory and approach-related behaviours (e.g., Buss & Kiel, 2013). Such parenting patterns may be influential in shaping the stability of trait BI over time, determining whether inhibited children remain so throughout childhood. Some literature implicates specific parenting styles in the stability of childhood BI, including maternal intrusiveness (Park, Belsky, Putnam, & Crnic, 1997; Rubin, Burgess, & Hastings, 2002), oversolicitousness (i.e., parenting characterized by warmth, intrusiveness, and low responsiveness; Degnan, Henderson, Fox, & Rubin, 2008; Rubin, Hastings, Stewart, Henderson, & Chen, 1997), and negativity (i.e., hostility and negative control; Hane, Cheah, Rubin, & Fox, 2008). Degnan, Henderson, Fox, and Rubin (2008) found that maternal oversolicitousness moderated the relationship between observationally assessed social reticence at age 4 and social wariness at age 7, such that reticent preschoolers tended to be high in wariness when their mothers also exhibited high levels of solicitous behaviour.
Despite research examining related parenting constructs and child outcomes, no studies have looked specifically at whether the relationship between children’s BI across time is moderated specifically by parental overprotection, typically defined as parenting behaviours that eliminate, or shelter children from, stress, as well as parents’ excessively comforting and affectionate reactions when their children exhibit fear (e.g., Hutt, Buss, & Kiel, 2013; Kiel & Buss, 2010). Past research in preschoolers has focused on the role of overprotection as a mediator of links between fearful temperament and shyness/inhibition (Kiel & Buss, 2012). However, research on the moderating effects of overprotection on BI over time is lacking.
This gap in the BI literature is surprising given research implicating parental overprotection and related parenting behaviours in childhood anxiety (e.g., Kiel & Buss, 2010). Indeed, moderation effects have been reported in the child anxiety literature, finding interactions between child BI and parental overprotection when predicting child anxiety (e.g., Degnan, Almas, & Fox, 2010; Murray, Creswell, & Cooper, 2009). Elevated BI combined with high parental overprotection has been found to predict children’s anxiety (e.g., Degnan, Almas, & Fox, 2010; Murray, Creswell, & Cooper, 2009). Parental overcontrol, a construct that overlaps with overprotective parenting and includes inappropriate and excessively protective, directive, and controlling behaviours, may also exacerbate the risk for anxiety associated with BI, such that stable, elevated BI in childhood has been associated with greater social anxiety in adolescence when mothers were overcontrolling (e.g., Lewis-Morrarty et al., 2012). Such findings suggest that childhood BI may confer greatest risk for anxiety in the presence of overprotective care. Although BI and anxiety share some features (e.g., heightened fear response; physiological correlates), the two constructs are distinguished by the extent to which such responses are pervasive and confer clinically significant, maladaptive repercussions (Goldsmith & Lemery, 2000). Little is known about whether overprotective care also serves to maintain early BI, such that inhibited young children exhibit persisting high levels of this trait when parents are overprotective prior to the development of clinically significant anxiety. Research has not examined parental overprotection specifically in the context of moderation models investigating BI assessed longitudinally in early childhood, despite its roles in moderating links between BI and children’s anxiety and in mediating BI assessed at different time points during toddlerhood.
Various mechanisms potentially underlie the ways in which overprotective parenting may contribute to BI over time. For example, behavioural models suggest low parental overprotection may result in children’s increased exposure to novelty, thereby increasing children’s opportunities to develop abilities to cope with novel, anxiety-eliciting situations in the future, resulting in a decrease of BI over time (e.g., Muris et al., 2011). Behavioural treatments of anxiety similarly stress the roles of exposure in reducing anxious behaviours (e.g., Abramowitz, Deacon, & Whiteside, 2010), while the principle of “steeling” also proposes that mild stress exposure is advantageous when considering children’s resilience (e.g., Rutter, 2012). Research involving both animals and children also supports this idea that mild stress exposure, which could occur when parental overprotection is lacking, can decrease negative outcomes when one is confronted with later stress (e.g., Rutter, 2012). Increased exposure to stress and the subsequent acquisition of coping skills could also occur within the context of higher PE as well. Taken together, these literatures suggest that experiences of overcoming mild stressors may promote new learning and coping skills, as well as a sense of psychological mastery, leading to increased resilience and adaptive reactions when confronted with later stress (e.g., Wu et al., 2013). Overprotective parenting may, therefore, limit children’s ability to learn coping skills during times of mild stress exposure. In addition, overprotective parenting may reflect parental genetic risk for BI or anxiety, such that gene-environment correlations are operating (e.g., Knafo & Jaffee, 2013), thereby influencing children’s BI over time.
In light of this literature, the objective of the present study was to better understand factors that shape the temperament trait BI over time. More specifically, to complement extant work on mediators of BI stability (e.g., Kiel & Buss, 2012), we examined whether child temperamental PE and caregiver overprotection served a moderating function with respect to the continuity of children’s BI over time. Given the challenges of assessing temperament and related constructs in infancy (e.g., Hubert, Wachs, Peters-Martin, & Gandour, 1982) and taking into account that early childhood is a developmental period during which there is evidence for increased stability of temperament as well as plasticity (e.g, Caspi et al., 2003; Van den Akker, Deković, Prinzie, & Asscher, 2010), we assessed children first at age 3 and subsequently at age 6. We expected that PE would interact with BI such that higher levels of age 3 PE would be associated with weaker associations between BI at ages 3 and 6. In accordance with past literature (e.g., Kiel & Buss, 2012; Lewis-Morrarty et al., 2012), we also predicted that parental overprotection would moderate the relationship between BI at ages 3 and 6, such that children exposed to higher overprotection would show stronger associations between BI assessed at these ages. Although overprotection has been implicated in child anxiety, we hypothesized that it may also play a crucial role in influencing early pathways by which elevated BI places children on high-risk trajectories, prior to the development of clinically significant anxiety disorders, by consolidating temperamental inhibition.
Method
Participants
Participants were an unselected sample of 559 children and their parents (446 of whom participated at follow-up) from Long Island, New York, recruited through a commercial mailing list when children were approximately 3 years old. The mean age of children (301 boys; 54.0%) was 3.52 years (SD = 0.26). Mothers were 35.99 years old on average (SD = 4.45) and fathers were 38.27 years old (SD = 5.40). Families were screened to ensure that children did not have significant medical or developmental impairments and that at least one biological parent spoke English. Most families were White/European-American (87.1%) and comprised of both parents (94.2%); approximately half (52.1%) of the mothers worked outside of the home. Families were predominantly middle-class, as assessed by the Hollingshead’s Four Factor Index of Social Status (Hollingshead, 1975; M = 2.18; SD = 0.89). Children scored within the average range (M= 102.80; SD = 11.00) on the Peabody Picture Vocabulary Test (PPVT; Dunn & Dunn, 1997). Written consent from the primary caregiver was obtained, and they received monetary compensation for their participation.
Follow-up participants were 446 of the initial 559 pairs of children and primary caregivers, an attrition rate of 20%. The mean age of children (240 boys; 53.8%) at follow-up was 6.08 years (SD = 0.42). Children who did not participate in the follow-up did not differ significantly from those who participated on age 3 BI, PE, or demographic variables (i.e., family income, race, PPVT scores; all ps >.19); however, there was a trend for children who were not followed up to be higher in parental overprotection, t(545) = −1.89, p =.059.
Age Three Assessment
Laboratory assessment of BI and PE
Children participated in 12 standardized laboratory tasks at baseline, 11 of which were drawn from the Laboratory Temperament Assessment Battery (Lab-TAB; Goldsmith, Reilly, Lemery, Longley, & Prescott, 1995), with a female experimenter. Tasks were designed to elicit a wide array of temperamental characteristics and were videotaped through a one-way mirror for future coding. The complete assessment spanned a total of approximately two and a half hours. Individual tasks lasted approximately three minutes, with a few exceptions (e.g., risk room lasted approximately 5 minutes), and children were given brief breaks to play in between each task in order to return to a baseline state. Carryover effects were minimized by ensuring that no tasks designed to elicit similar affective reactions occurred sequentially. Of the 12 tasks, PE was coded in all, and BI in three tasks (risk room, stranger approach, and exploring new objects) that were selected based on prior research using similar procedures to assess behaviors relevant to this trait. A parent was present in the main experimental area with his/her child for all episodes except stranger approach and box empty (see below). A description of each episode is provided below.
Risk room
The experimenter left the child alone to explore a set of novel and ambiguous stimuli (e.g., cloth tunnel, balance beam, Halloween mask, etc.) in a large room. After 5 minutes, the experimenter returned and asked the child to touch each of the stimuli.
Tower of patience
The child and experimenter took turns building a tower with large blocks. During each of her turns, the experimenter adhered to a schedule of increasingly lengthy delays before placing her block on the tower.
Arc of toys
The child was allowed to play freely by him or herself with toys for a few minutes. The experimenter then returned and asked the child to put the toys away.
Stranger approach
After leading the child into the main experimental area, the experimenter left the child alone under the pretense that she needed to get new toys for them to play with. After a brief delay, an unfamiliar male research assistant entered the room and spoke to the child in a neutral tone while gradually walking closer to the child.
Car go
The child and experimenter played with two remote-controlled cars.
Transparent box
The child selected a toy, which the experimenter locked in a transparent box. The child was then left to work to open the box with a set of keys that were, unbeknownst to the child, inoperable. After a few minutes, the experimenter returned with the correct key, and helped the child access the toy.
Exploring new objects
The child explored a set of novel and ambiguous stimuli, including a mechanical spider and bird, and sticky, soft gel balls.
Pop-up snakes
The experimenter showed the child what appeared to be a can of potato chips, actually containing coiled spring snakes. The experimenter demonstrated the trick, and encouraged the child to surprise his or her mother with the snakes.
Impossibly perfect green circles
The child was repeatedly asked to draw a circle on a large piece of paper. After each drawing, the experimenter mildly criticized each circle.
Popping bubbles
The child and experimenter played with a bubble-shooting toy.
Snack delay
The child was instructed to wait for the experimenter to ring a bell before eating a bite of a snack. The experimenter adhered to a schedule of varied delays before ringing the bell.
Box empty
The child was given a gift-wrapped box, under the pretence that an appealing toy was inside. After a brief interval in which the child was left alone to discover that the box was empty, the experimenter returned with several small toys for the child to keep, explaining that she had forgotten to place the toys inside.
Temperament coding
Video-recordings of the laboratory tasks were coded by trained graduate and undergraduate raters who were blind to other study data. Coders had to reach at least 80% agreement with a “master” coder before coding independently. A large number of raters, trained on specific episodes, coded the data to minimize the extent to which the same rater coded multiple episodes of the same child. To code BI, we used a system based heavily on previous coding designed specifically to assess behaviours relevant to this construct (e.g., Durbin, Klein, Hayden, Buckley, & Moerk, 2005; Goldsmith et al., 1995). Given that BI is defined by response to particular contexts (i.e., novel or threatening situations) it was only coded in the three episodes specifically designed to be especially novel and ambiguous (i.e., risk room, stranger approach, and exploring new objects). Different teams of raters coded BI, PE and other study constructs for interrater reliability; thus, the number of cases upon which interrater reliability was based differed due to the number of children for whom double-coded data existed for the subset of Lab-TAB tasks. For example, 28 children were double-coded on all BI tasks at age 3, indicating that interrater reliability for age 3 BI was established based on 28 cases, which is comparable to previous work (e.g., Durbin, Klein, Hayden, Buckley, & Moerk, 2005; Rubin, Burgess, & Hastings; Van den Akker, Deković, Prinzie, & Asscher, 2010).
BI coding
Tasks were coded using a system based on that of Goldsmith et al. (1995), in which specific behaviours and emotions relevant to BI were coded at 20–30-second intervals (“epochs”) for each episode. This approach is used in many studies that use laboratory observations to assess BI (e.g., Durbin, Klein, Hayden, Buckley, & Moerk, 2005; Olino, Klein, Dyson, Rose, & Durbin, 2010; Pfeifer, Goldsmith, Davidson, & Rickman, 2002). In each epoch, the maximum intensity of each relevant behaviour was coded, and a summary variable was calculated for each variable coded in each episode based on average ratings across the whole episode. Aggregate variables were then calculated as averages based on all episodes that coded that variable. Variables coded across all three episodes included fearful facial (e.g., eyebrows raised in distress, mouth drawn back in fear), bodily (e.g., wary gait, bodily tension, nervous fidgeting), and vocal (e.g., timid tone of voice, comments with fearful content) affect, as well as latency to first fear response. In risk room and exploring new objects, coded variables also included latency to touch objects, total number of objects touched, tentative play, references and proximity to parent, references to experimenter (e.g., timid glances toward experimenter or fearful questioning of experimenter before complying with experimenter’s request to touch objects), time spent playing, and latency to verbalize; a startle variable was further included from exploring new objects. Coded variables from stranger approach included gaze aversion, latency to vocalize, approach to and avoidance of stranger, and verbal/nonverbal interaction with stranger (e.g., talking with stranger, nodding in response to stranger). Variables reflecting positive affect (e.g., smiling) were not included in the BI composite in order to avoid confounding these constructs. The BI scale consisted of an average of z-scored codes (α = .80; ICC =.88; n = 28) from risk room, exploring new objects, and stranger approach. This scale was log-transformed to achieve normality.
PE Coding
As positive emotionality is not conceptualized as a context-specific behaviour (in contrast to BI, see Laptook, Klein, Olino, Dyson, & Carlson, 2010), positive affect and interest were coded during all episodes of the Lab-TAB. We have extensively documented the validity and reliability of this coding scheme in previous work (e.g., Durbin, Hayden, Klein, & Olino, 2007; Mackrell et al., 2014; Olino, Klein, Dyson, Rose, & Durbin, 2010). Further, this approach capitalizes on the principle of aggregation of multiple behavioural ratings to derive more stable estimates of a trait, and assesses individual differences in the tendency to respond to the general environment with PE, rather than just in tasks believed a priori to elicit positive affect. Within each episode, each relevant display of facial (e.g., smiling, contractions of outer eye corners), vocal (e.g., exuberant tone of voice, giggling, statement with overtly positive content), and bodily (e.g., clapping in excitement, jubilant motions) positive affect was coded on a three-point intensity scale. Ratings for the affective displays in each channel were summed within each episode, the totals for the 12 episodes were then standardized and summed, and the three channels were aggregated to create a score for positive affect reflecting facial, vocal, and bodily indicators. Interest scores were coded on a 4-point scale based on the frequency and intensity of relevant behaviors throughout the episode and the ratings were summed across the 12 episodes to form a total interest score. Children’s scores on the final PE scale were the standardized composite of positive affect and interest (α =.82; ICC =.89; n = 35).
Parental overprotection
As a questionnaire measure of overprotection, both caregivers independently completed the Parenting Styles and Dimensions Questionnaire (PSDQ; Robinson, Madleco, Olsen, & Hart, 2001), a 37-item measure assessing parenting behaviours based on a 5-point scale ranging from 1 (never) to 5 (always). For the present study, we used parents’ and co-parents’ self-reports on the 5-item overprotectiveness scale (parent PSDQ α =.69; co-parent PSDQ α =66), which includes items tapping parental control, concerns surrounding their child’s potential failure at tasks and attempts at new activities, and concerns that their child will garner the disapproval of others. In addition, primary caregivers participated in a semi-structured interview (i.e., the Preschool Age Psychiatric Assessment; PAPA; Egger, Ascher, & Angold, 1999), in which children’s psychiatric symptoms and behaviours were assessed; these data are not used in the present study. Based on the information provided during this interview, interviewers coded the presence of parental overprotection (e.g., comments reflecting parental need for control, fears of harm befalling the child, and tendencies such as the refusal to let the child out of sight) making a global rating ranging from 0 (not at all characteristic of caregiver) to 4 (highly characteristic of caregiver) for overprotection; interrater reliability was fair (ICC =.50; n = 21; Shrout, 1998). Both the content of the parents’ responses and the manner in which they responded (e.g., tone, emphasis) were captured in this global rating of parental overprotection.
Maternal PSDQ overprotection and paternal overprotection showed a small, albeit significant, positive correlation with each other (r =.20, p <.001), but neither was significantly correlated with interviewer ratings of overprotection (r =.04, p =.367 for maternal PSDQ; r = −.03, p=560 for paternal PSDQ). For this reason, we treated interviewer overprotection as a separate marker of overprotection and averaged the two parent-report overprotection scores into a single score (i.e., parent-reported overprotection).
Age Six Assessment
Laboratory assessment of BI
Children participated in another battery of laboratory tasks. As the current study is focused on predicting age 6 BI, only tasks relevant to its assessment are discussed here. Given the need for the follow-up laboratory tasks to be both novel and appropriate for older children, different tasks from the age 3 assessment were used to elicit BI. These tasks were based on an adapted version of the Lab-TAB (e.g., Durbin, Hayden, Klein, & Olino, 2007; Mackrell et al., 2014; Olino, Klein, Dyson, Rose, & Durbin, 2010), and were designed to be analogous to the original laboratory tasks but developmentally appropriate for older children. Good concurrent, discriminant, and predictive validity has been demonstrated for these tasks in previous studies with other samples of children aged 5 and 6 (e.g., Durbin, Hayden, Klein, & Olino, 2007).
Story time
The experimenter asked the child to tell a story to an unfamiliar research assistant using the picture book A Boy, a Dog, and a Frog. The child was told that the research assistant was a “story expert” and that the assistant would assign the child a grade based on how well he or she told the story. The experimenter returned after four minutes and the assistant praised the child’s story and gave him/her a grade of an ‘A’.
Object fear
The child was instructed to explore a room that was filled with fear-eliciting objects, including a box filled with plastic insects and from which cricket sounds were emitted, a cage with plastic rats inside it, and a large, fuzzy, black spider covered with a cloth.
BI coding
BI tasks at follow-up were coded using similar coding procedures as those used for the baseline assessment. Video-recordings of BI tasks were again coded by trained undergraduate and graduate raters. Variables coded across both episodes included fearful facial, bodily, and vocal affect, as well as stilling/freezing. In story time, coded variables also included distress vocalizations, latency to vocalize, approach to the research assistant, and verbal/nonverbal interaction with the research assistant. Coded variables from object fear included latency to touch objects, total number of objects touched, tentative play, references to experimenter (e.g., timid glances toward experimenter or fearful questioning of experimenter before complying with experimenter’s request to touch objects), time spent playing, time spent talking, fearful or wary comments and questions, latency to comply, and noncompliance. The BI scale consisted of an average of z-scored codes (α =.72) from story time and object fear. Interrater reliability indexed by ICC was moderate (ICC = .64, n = 35; Shrout, 1998).
Overprotection
In order to rule out the possibility that any potential relationship between age 3 overprotection and age 6 BI was accounted for by the association between overprotection at ages 3 and 6, overprotection measures at age 6 were collected and used as covariates in models using age 3 overprotection as a predictor of age 6 BI. Thus, at the age 6 follow-up, primary and secondary caregivers again completed the PSDQ. Similar to the baseline assessment, primary caregivers participated in a semi-structured interview (i.e., the PAPA; Egger, Ascher, & Angold, 1999), in which children’s psychiatric symptoms and behaviours were assessed; these data are not used in the present study. Based on the content provided during this interview and parents’ styles of responding, interviewers used the same global rating system as that used during the baseline assessment to code the presence of parental overprotection; although the frequency of overprotection was too low in the sample coded for reliability to calculate an ICC, we note the moderate reliability of the same rating system at baseline.
Results
Means, standard deviations, and bivariate correlations between demographic and other study variables are presented in Table 1. Age 3 and age 6 BI showed a small, significant positive correlation; this association was comparable to laboratory-based studies of BI of unselected participants reported across similar follow-up intervals (Rubin, Burgess, & Hastings, 2002; Scarpa, Raine, Venables, & Mednick, 1995) albeit smaller than associations reported in other studies, particularly those using extreme groups (Broberg, Lamb, & Hwang, 1990). Age 3 BI was significantly and positively associated with child sex, such that girls had a higher level of BI than boys1. Age 3 and age 6 BI were significantly and negatively associated with age 3 PE, such that children with higher levels of BI tended to display lower levels of PE, although correlations were again small. There were no significant associations between age 3 BI and parental overprotection at age 3 or age 6. Age 6 BI showed small albeit significant positive correlations with parent-reported overprotection at age 6, such that children with higher levels of parental overprotection tended to be higher in BI at age 6. Not surprisingly, age 3 parent-reported overprotection also showed a significant medium-sized positive correlation with age 6 parent-reported overprotection. There were no significant correlations between age 3 PE and parental overprotection at age 3 or age 6.
Table 1.
Correlations between child temperament, parental overprotection, and child sex.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Age 3 BI | – | ||||||||
| 2. Age 6 BI | .19** | – | |||||||
| 3. Age 3 PE | −.22** | −.15** | – | ||||||
| 4. Age 6 PE | −.17** | −.04 | .41** | – | |||||
| 5. Age 3 PSDQ | −.01 | .08 | −.02 | .05 | – | ||||
| Overprotection | |||||||||
| Composite | |||||||||
| 6. Age 6 PSDQ Overprotection Composite | −.01 | .12* | −.07 | −0.04 | .51** | – | |||
| 7. Age 3 Interviewer-rated Overprotection | −.02 | .08 | −.06 | −.07 | .01 | .04 | – | ||
| 8. Age 6 Interviewer-rated Overprotection | −.01 | .03 | .04 | −.05 | −.03 | −.01 | −.03 | – | |
| 9. Child Sex | .17** | .07 | .08 | .13** | .01 | −.04 | −.03 | .004 | – |
| N | 559 | 447 | 559 | 452 | 507 | 436 | 528 | 460 | 563 |
| Mean | 0.63 | −0.13 | 0.00 | −0.01 | 0.03 | −0.004 | 1.27 | 0.21 | – |
| Standard Deviation | 0.20 | 0.43 | 1.80 | 0.57 | 2.57 | 2.77 | 0.70 | 0.56 | – |
p <.05,
p <.01.
Note: Age 3 and Age 6 Overprotection reflected by composite variables; Sex coded as male = 1, female = 2.
Multiple regression was used to determine whether age 3 PE and parental overprotection moderated the association between children’s BI at age 3 and age 6 (Aiken & West, 1991). Prior to running the analyses, continuous variables were standardized. Given work suggesting sex differences in aspects of BI (e.g., Doey, Coplan, & Kingsbury, 2014; Fox, Henderson, Marshall, Nichols, & Ghera, 2005), child sex was initially entered as a covariate in all models; as there were no significant main effects of sex and it did not interact with study variables, it was dropped from final models. In cases of significant interactions, tests of simple slopes and regions of significance were used. All simple slopes used the mean value of the moderator variable from the sample as well as values one standard deviation above and below the mean of the moderator variable. To test regions of significance, we used Hayes and Matthes’ (2009) guidelines for the Johnson-Neyman technique (Johnson & Fay, 1950). This method uses the asymptotic variances, covariances, and other regression parameters to determine the value(s) of the focal predictor variable at which groups at varying levels of the moderator (e.g., low, moderate, high) are significantly different (p <.05) in terms of the outcome variable. Here, this technique could indicate levels in our sample at which age 3 BI is associated with group differences in age 6 BI based on the level of the moderator. Partial correlations (pr) are provided as measures of effect size in our analyses.
In our first model, age 3 BI and age 3 PE were entered on the first step, followed by the product of BI and PE. The main effects of age 3 BI and age 3 PE were significant in this model (see Table 2). However, these main effects were qualified by the presence of a significant interaction between age 3 BI and age 3 PE. As predicted, the association between age 3 and age 6 BI was strongest in children with lower levels of PE, and diminished as levels of PE increased: tests of simple slopes indicated that the relationship between levels of BI at age 3 and age 6 was significant at low (b = 0.60, p <.0001, pr =.21) and moderate (b = 0.34, p =0009, pr =.16) levels of PE, but not at high levels of PE (b = 0.07, p =.614, pr =.02). This interaction is depicted in Figure 1. Tests of regions of significance showed that significant differences in age 6 BI as a function of age 3 PE were evident above an age 3 BI value of −0.02, slightly lower than average age 3 BI. The plots suggested that the impact of child PE was more salient at relatively higher levels of age 3 child BI, rather than when BI was low. Thus, PE seemed to influence the association between age 3 and age 6 BI only when children exhibited moderate to high BI at age 3.
Table 2.
Children’s age 3 behavioral inhibition (BI), age 3 positive emotionality (PE), and their interaction as predictors of children’s BI levels at age 6.
| Overall Model | Change Statistic | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| b | df | R2 | F | Cohens f2 | df | R2 | F | |
| Step 1 | 2, 444 | .05 | 11.52*** | .05 | ||||
| Age 3 BI | 0.36† | |||||||
| Age 3 PE | −0.03* | |||||||
| Step 2 | 3, 443 | .07 | 10.39*** | .08 | 1, 443 | .02 | 7.78** | |
| Age 3 BI | 0.35† | |||||||
| Age 3 PE | −0.03* | |||||||
| Age 3 BI × Age 3 PE | −0.16** | |||||||
Note: Ns=356–447;
p <.05,
p <.01,
p <.001,
p =.001.
Figure 1.
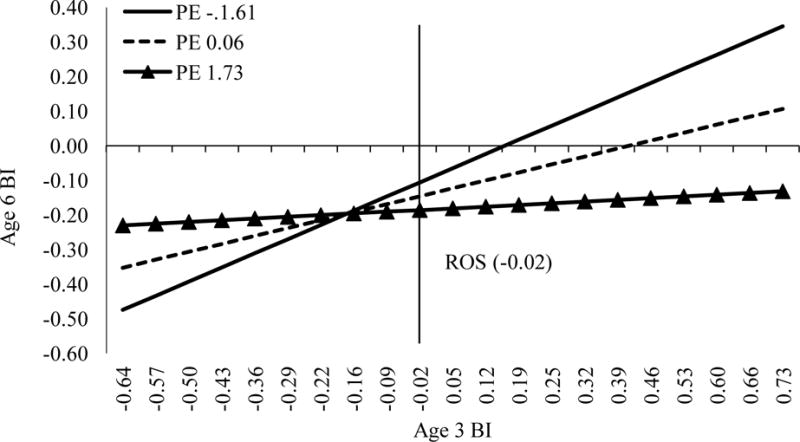
Interaction between age 3 BI and age 3 PE predicting age 6 BI. The value x = −0.02, derived using the Johnson-Neyman technique (Johnson & Fay, 1950), indicates the value of age 3 BI above which significant differences in age 6 BI emerge for children with varying levels of age 3 PE. Simple slopes use the mean value of PE, as well as values one standard deviation above and below the mean. Age 3 BI, age 6 BI, and age 3 PE are mean-centred. ROS = region of significance.
In our second set of models, we tested the moderating effects of parental overprotection on the association between age 3 and age 6 BI. As concurrent overprotection may influence child BI (e.g., Burkhouse, Gibb, Coles, Knopik, & McGeary, 2011; Muris, van Brakel, Arntz, & Schouten, 2011), we entered age 6 overprotection as a covariate to examine the predictive effects of overprotection at age 3 over and above its contemporaneous effects (see Table 3). Because there is an association between parental anxiety disorder and overprotection (e.g., Clarke, Cooper, & Creswell, 2013), we initially included a variable indicating whether mothers or fathers had ever met criteria for any DSM-IV anxiety disorder, assessed using structured diagnostic interviews with both parents (following Olino, Klein, Dyson, Rose, & Durbin, 2010) as a covariate. As these covariates did not significantly change the interactions reported, we dropped them from the model.
Table 3.
Children’s age 3 behavioral inhibition (BI), age 3 parent-reported overprotection (PSDQ composite), and their interaction as predictors of children’s BI levels at age 6.
| Overall Model | Change Statistic | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| b | df | R2 | F | Cohens f2 | df | R2 | F | |
| Step 1 | 3, 395 | .04 | 6.07*** | .04 | ||||
| Age 3 BI | 0.37*** | |||||||
| Age 3 PSDQ Overprotection | 0.01 | |||||||
| Age 6 PSDQ Overprotection | 0.01 | |||||||
| Step 2 | 4, 394 | .05 | 5.63*** | .05 | 1, 394 | .01 | 4.16* | |
| Age 3 BI | 0.40*** | |||||||
| Age 3 PSDQ Overprotection | 0.01 | |||||||
| Age 6 PSDQ Overprotection | 0.01 | |||||||
| Age 3 BI × PSDQ Overprotection | 0.09* | |||||||
Note: Ns=356–447;
p <.05,
p <.01,
p <.001.
We ran two models in which parent overprotection was operationalized as either (a) averaged maternal and paternal PSDQ overprotection (i.e., parent-reported overprotection), or (b) interviewer ratings of overprotection. In our first overprotection model, age 3 BI, age 3 parent-reported overprotection, and age 6 parent-reported overprotection were entered on the first step, followed by the product of age 3 BI and age 3 PSDQ overprotection. The main effect of age 3 BI was significant in this model (see Table 3). However, this main effect was qualified by the presence of a significant interaction between age 3 BI and age 3 parent-reported overprotection. As predicted, the association between age 3 and age 6 BI was strongest in children with higher levels of parental overprotection, and decreased as levels of overprotection decreased: tests of simple slopes indicated that the relationship between levels of BI at age 3 and age 6 was significant at moderate (b = 0.40, p <.0001, pr =.19) and high (b = 0.62, p <.001, pr =.19) levels of overprotection, but not at low levels of overprotection (b = 0.18, p =.18, pr =.07). This interaction is depicted in Figure 2. Tests of regions of significance showed that significant differences in age 6 BI as a function of age 3 parent-reported overprotection were evident above an age 3 BI value of 0.12, slightly higher than average age 3 BI. The plots suggested that the impact of parent-reported overprotection was more salient at relatively higher levels of age 3 child BI, rather than when BI was low. Thus, parental overprotection seemed to influence the association between age 3 and age 6 BI only when children exhibited moderate to high BI at age 3.
Figure 2.
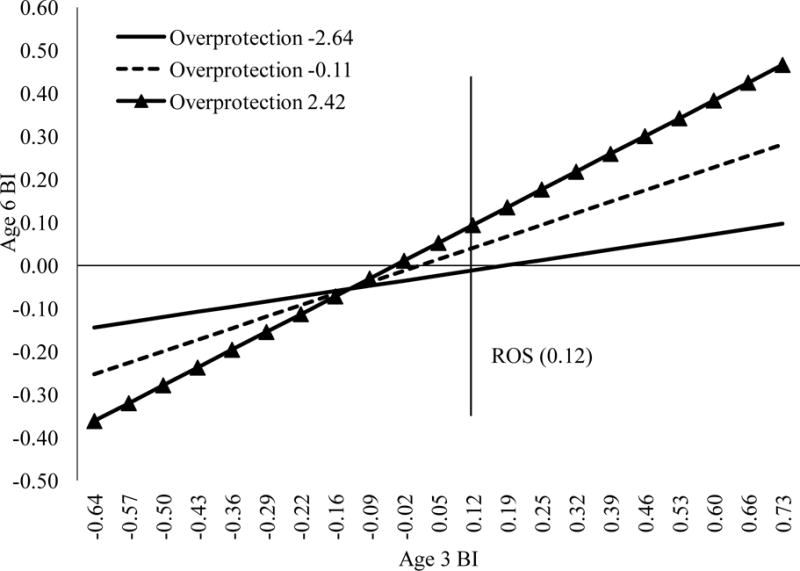
Interaction between age 3 BI and parent-reported overprotection predicting age 6 BI. The value x = 0.12, derived using the Johnson-Neyman technique (Johnson & Fay, 1950), indicates the value of age 3 BI above which significant differences in age 6 BI emerge for children exposed to varying levels of parental overprotection. Simple slopes use the mean value of parent-reported overprotection, as well as values one standard deviation above and below the mean. Age 3 BI, age 6 BI, and parent-reported overprotection are mean-centred. ROS = region of significance.
Our second overprotection model was similar to the model described above, but with interviewer-rated overprotection used as the measure of overprotection. Again, the main effect of age 3 BI was significant in this model (see Table 4). The main effect of age 3 interviewer-rated overprotection was also significant. These main effects were qualified by the presence of a significant interaction between age 3 BI and age 3 interviewer-rated overprotection. Again, the association between age 3 and age 6 BI was strongest in children with higher levels of parental overprotection, and diminished as levels of overprotection decreased: tests of simple slopes indicated that the relationship between levels of BI at age 3 and age 6 was significant at moderate (b = 0.32, p =.001, pr =.18) and high (b = 0.53, p <.001, pr =.26) levels of overprotection, but not at low levels of overprotection (b = 0.11, p =.36, pr =05). This interaction is depicted in Figure 3. Tests of regions of significance showed that significant differences in age 6 BI as a function of age 3 overprotection were evident above an age 3 BI value of −0.05 or below an age 3 BI value of −0.63. The plots suggested that the impact of interviewer-rated overprotection was more salient at relatively higher levels of age 3 child BI and at extremely low levels of age 3 child BI. Thus, interviewer-rated overprotection seemed to influence the association between age 3 and age 6 BI only when children exhibited moderate to high BI at age 3 or when children exhibited very low age 3 BI.
Table 4.
Children’s age 3 behavioral inhibition (BI), age 3 interviewer-rated parental overprotection, and their interaction as predictors of children’s BI levels at age 6.
| Overall Model | Change Statistic | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| b | df | R2 | F | Cohens f2 | df | R2 | F | |
| Step 1 | 3, 352 | .05 | 6.57*** | .05 | ||||
| Age 3 BI | 0.35*** | |||||||
| Age 3 Interviewer-Rated | 0.06* | |||||||
| Overprotection | ||||||||
| Age 6 Interviewer-Rated | 0.03 | |||||||
| Overprotection | ||||||||
| Step 2 | 4, 351 | .08 | 7.69*** | .09 | 1, 351 | .03 | 10.51† | |
| Age 3 BI | 0.32† | |||||||
| Age 3 Interviewer-Rated | 0.07* | |||||||
| Overprotection | ||||||||
| Age 6 Interviewer-Rated | 0.03 | |||||||
| Overprotection | ||||||||
| Age 3 BI × Age 3 Interviewer-Rated Overprotection | 0.30† | |||||||
Note: Ns=356–447;
p < 05,
p < 01,
p < 001,
p = 001.
Figure 3.
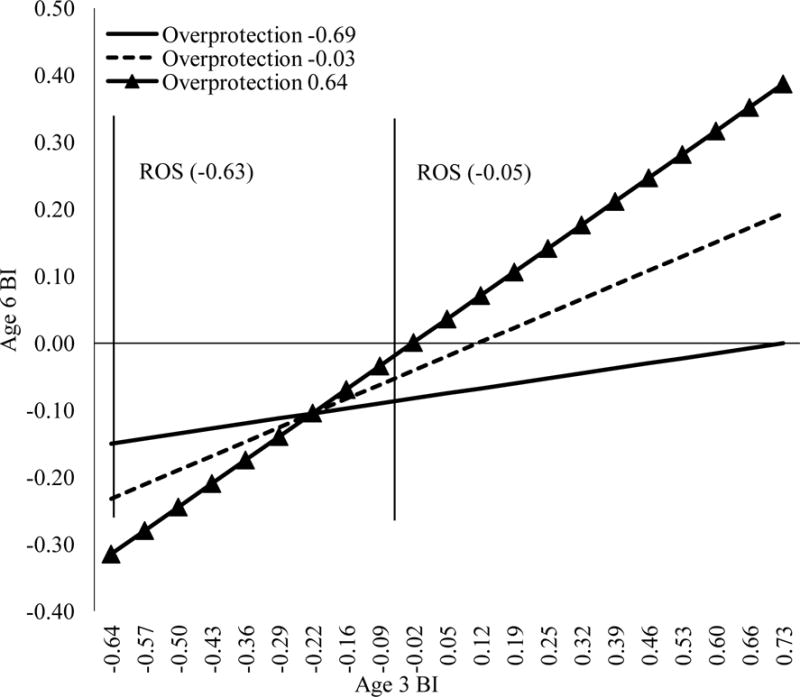
Interaction between age 3 BI and interviewer-rated overprotection predicting age 6 BI. The values x = −0.63 and x = −0.05, derived using the Johnson-Neyman technique (Johnson & Fay, 1950), indicate the values of age 3 BI below and above which significant differences in age 6 BI emerge for children exposed to varying levels of parental overprotection. Simple slopes use the mean value of interviewer-rated overprotection, as well as values one standard deviation above and below the mean. Age 3 BI, age 6 BI, and interviewer-rated overprotection are mean-centred. ROS = region of significance.
While we had no a priori hypothesis for a three-way interaction between BI, PE, and overprotection, an exploratory analysis including this term (i.e., age 3 BI, age 3 PE, age 3 overprotection, child sex, age 3 BI X age 3 PE, age 3 BI X age 3 overprotection, and age 3 BI X age 3 PE X age 3 overprotection) showed that it was not significant, p =.13 in the parent-reported overprotection model and p =.82 in the interviewer-rated overprotection model.
Discussion
The purpose of the current study was twofold. First, we tested whether the association between age 3 and age 6 BI was influenced by PE; like BI, PE plays a prominent role in children’s exploratory behavior and reactions to novelty, and may therefore shape how children’s early inhibition unfolds over time. We also examined whether overprotective parenting contributes to the association between children’s BI assessed longitudinally in early childhood, building on the extant literature on early caregiving and the stability of BI, as well as research implicating overprotection in the relationship between BI and subsequent anxiety (e.g., Kiel & Buss, 2010). Although investigators have tested mediation models linking overprotection to the stability of BI (Kiel & Buss, 2012), to our knowledge, no one has previously examined whether parental overprotection moderates associations between children’s BI over time. Findings indicated that both child PE and parental overprotection moderated the relationship between BI at age 3 and BI at age 6, with both lower PE and greater overprotection increasing the association between earlier and later BI. Notably, the effect of caregiver overprotection was found across two different methods of assessment that were uncorrelated with each other, indicating that this is a robust effect.
Despite the longstanding interest in childhood BI as a vulnerability factor, surprisingly little research has considered whether other traits moderate the continuity of this marker of risk over time. In an extension of the literature implicating PE as a moderator of other vulnerabilities (e.g., Wills, Sandy, Yaeger, & Shinar, 2001), we investigated associations between PE and the association between age 3 and age 6 BI, finding that age 3 BI was only predictive of age 6 BI when children also displayed low to moderate levels of PE. Although our study is the first to test this hypothesis, these findings complement theory and previous research. Research in adults has shown associations between social anxiety and a number of facets of PE (Naragon-Gainey, Watson, & Markon, 2009); it is possible that low PE is associated with social anxiety by virtue of its moderating influence on high BI. Children who are high in both BI and PE may overcome their inhibited behaviour over time as elevated PE encourages approach and exploratory behaviors, thereby facilitating exposure and acclimatization to novelty, thus reducing BI over time. Such an explanation is consistent both with literature finding elevated activity levels in young boys to reduce the association between elevated shyness and increased internalizing problems (Karevold, Coplan, Stoolmiller, & Mathiesen, 2011), and with literature indicating that high PE may act as a buffer against other vulnerabilities to negative outcomes (e.g., Clark, 2005; Tugade & Fredrickson, 2004; Wichers et al., 2007). It is also consistent with other models of individual difference factors that emphasize the joint effects of approach/avoidance systems on behavior (e.g., Gray, 1970 as well as Asendorf’s 1990 orthogonal social approach and social avoidance motivation system). The current study adds support for the notion that interactions between BI and other child temperament traits contribute to child risk and resilience, although further work is needed to identify the specific mechanisms that account for how PE moderates BI stability.
In addition, parental overprotection predicted the association between age 3 and age 6 BI, such that an increased association was found between age 3 and age 6 BI when parent overprotection was at least moderate. This finding is consistent with previous work showing that parental overprotection is associated with elevated BI in early childhood assessed using cross-sectional designs (e.g., Burkhouse, Gibb, Coles, Knopik, & McGeary, 2011; Muris, van Brakel, Arntz, & Schouten, 2011). Additionally, Edwards, Rapee, and Kennedy (2010) found longitudinal evidence for the role of parental overprotection in predicting anxiety in children aged 3 to 5 years, such that parental reports of overprotective parenting predicted anxiety in children 12 months later. Our findings are consistent with Degnan, Henderson, Fox, and Rubin (2008), who reported that observed greater maternal solicitousness was associated with higher levels of social wariness at age 7 when children displayed higher levels of social reticence at age 4.
Overprotective parenting may influence the stability of childhood BI through various paths. In terms of causal mechanisms, low levels of overprotective parenting may lead to greater child exposure to novelty, thus facilitating inhibited children’s acquisition of adaptive coping strategies and skills, which then leads these children to be better equipped to manage novel, anxiety-provoking situations and become less inhibited over time (e.g., Muris et al., 2011). This would be consistent with behavioural treatments of anxiety that emphasize exposure and extinction (e.g., Abramowitz, Deacon, & Whiteside, 2010), as well as the concept of “steeling,” which suggests there is a benefit of mild stress exposure on child resilience (e.g., Rutter, 2012). In addition, studies of both animals and children have found that exposure to mild stressors can reduce negative outcomes in the context of subsequent stress (e.g., Rutter, 2012). Considered together, this research suggests that overcoming mild stressors may encourage new learning and coping strategies, in addition to enhanced feelings of psychological mastery, thus resulting in greater resilience and adaptive behaviours when faced with subsequent stress (e.g., Wu et al., 2013). It is also worth noting that overprotective parenting may be a marker of parental genetic risk for BI or anxiety, indicating the presence of gene-environment correlations (e.g., Knafo & Jaffee, 2013). Although the current pattern of findings remained even when controlling for parent anxiety disorder history, there is no reason to expect that such analyses fully address the influence of parental genetic risk for BI in our models. Given the heritability of BI (e.g., Robinson, Kagan, Reznick, & Corley, 1992), it is possible that the current pattern of effects represents interactions between genetic influences that contribute to associations between BI over time.
While current research suggests that parental overprotection may be a mechanism by which children with high BI develop anxiety disorders, our findings suggest that overprotection may influence children’s risk for anxiety by interacting with early BI to affect later BI, thus placing children on a high-risk trajectory. While replication of our findings is important, the moderating effect of overprotective parenting on the association between age 3 and age 6 BI may provide an early opportunity for prevention by identifying parenting practices that put children high in BI at risk. However, given that moderation analyses do not speak directly to mechanisms, additional process-oriented research is an important complement to the current findings.
It is intriguing that the influence of both moderators on the association between age 3 and age 6 BI generally appeared most important when children were near or above the mean in BI at age 3; the one exception to this is discussed in the next paragraph. Analyses indicated that children low in BI at age 3 were similarly low in age 6 BI, regardless of the degree of age 3 PE or parental overprotection; however, as age 3 BI increased, children who varied in PE and parental overprotection became increasingly distinct in terms of age 6 BI. As high BI is clearly implicated in child vulnerability, our findings speak to the consolidation of risk related to elevated BI, suggesting some children (i.e., children with higher initial BI) may be more vulnerable to the impact of low PE and high parental overprotection on later BI. Given the literature supporting the link between stable BI and child outcomes across socio-emotional domains (e.g., Chronis-Tuscano et al., 2009; Essex, Klein, Slattery, Goldsmith, & Kalin, 2010), future research should explore the role of both PE and overprotective parenting in moderating the relationship between BI in toddlerhood and socio-emotional functioning in early childhood.
Analyses of regions of significance also indicated that interviewer-rated overprotection was related to significantly different levels of age 6 BI in children very low in age 3 BI. While the influence of overprotection on disinhibition was not a focus of the current study, this finding suggests that uninhibited children tend to remain so over time when parent overprotection is low. This could mean that normative care (i.e., low overprotection) results in more typical levels of inhibition as children mature, or that overprotection in disinhibited children tends to maintain children’s disinhibition over time.
We found a small, albeit positive, correlation between BI at age 3 and age 6. This modest association in our study likely reflects differences in the tasks used to assess BI at the two assessments; in addition, three tasks were used to assess BI at age 3 and two tasks were used at age 6. As noted, the use of different tasks during different assessments stemmed from the need for tasks to be both novel to children, and hence evocative of BI, and developmentally appropriate. Nevertheless, the magnitude of the correlation was comparable to other studies of BI that used observational methods (Rubin, Burgess, & Hastings, 2002; Scarpa, Raine, Venables, & Mednick, 1995).
The present study had multiple strengths, including observational measures of child temperament at both baseline and follow-up, multimethod assessment of parenting, and a relatively large sample. In addition, we used a longitudinal design that assessed children over a 3-year follow-up period, enabling a stringent test of associations between age 3 and age 6 BI. However, there were also limitations of our study. We did not include an observational measure of overprotective parenting; replication of the current findings using observational measures of parental overprotection will be important in future research. Second, trend level differences in overprotection were evident in attrition in our sample, such that children who did not participate in the follow-up assessment tended to be higher in baseline parental overprotection. Thus, it is possible that missing data related to attrition or other causes could have led to unknown biases. Third, parental overprotection at age 6 was very infrequent. Fourth, some of our ICCs indicated only “fair” interrater reliability (Shrout, 1998). Fifth, only a small proportion of parents reported a change in marital status between baseline and follow-up assessments, which may limit the generalizability of our findings to children who show greater changes in family composition. Finally, our sample consisted largely of participants from middle-class, White-European American families, limiting the generalizability of our findings to other cultures and socioeconomic classes.
In summary, we found evidence suggesting that the association between age 3 and age 6 BI is influenced by child temperamental PE and parental overprotection. While replication of our findings is important, given the relationship between stable BI and negative child outcomes, particularly anxiety disorders, our findings may be useful in developing and applying targeted prevention and intervention strategies for children at heightened risk.
Research Highlights.
Factors that influence behavioral inhibition (BI) over time were examined
Child positive emotionality moderated links between age 3 – age 6 BI
Parental overprotection also moderated age 3 – age 6 BI associations
Acknowledgments
This research was supported by National Institute of Mental Health grant R01 MH069942 (Klein), General Clinical Research Center grant M01 RR10710 (Stony Brook University, National Center for Research Resources), and the Children’s Health Research Institute.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
An independent samples t-test indicated that girls (M = 0.67, SD = 0.20) were significantly higher in age 3BI than boys (M = 0.60, SD = 0.19), t(557) = −3.945, p <.001.
References
- Abramowitz JS, Deacon BJ, Whiteside SPH. Exposure Therapy for Anxiety: Principles and Practice. New York: Guilford Press; 2010. [Google Scholar]
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Newbury Park, CA: Sage; 1991. [Google Scholar]
- Asendorpf JB. Beyond social withdrawal: Shyness, unsociability, and peer avoidance. Human Development. 1990;33(4–5):250–259. doi: 10.1159/000276522. [DOI] [Google Scholar]
- Broberg A, Lamb ME, Hwang P. Inhibition: its stability and correlates in sixteen-to forty-month-old children. Child Development. 1990;61(4):1153–1163. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/2209185. [PubMed] [Google Scholar]
- Buss KA, Kiel EJ. Temperamental risk factors for pediatric anxiety disorders. In: Vasa RA, Roy AK, editors. Pediatric anxiety disorders: A clinical guide. New York: Springer; 2013. pp. 47–68. [Google Scholar]
- Burkhouse KL, Gibb BE, Coles ME, Knopik VS, McGeary JE. Serotonin transporter genotype moderates the link between children’s reports of overprotective parenting and their behavioral inhibition. Journal of Abnormal Child Psychology. 2011;39(6):783–90. doi: 10.1007/s10802-011-9526-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caspi A, Harrington H, Milne B, Amell JW, Theodore RF, Moffit TE. Children’s behavioral styles at age 3 are linked to their adult personality traits at age 26. Journal of Personality. 2003;71(4):495–513. doi: 10.1111/1467-6494.7104001. [DOI] [PubMed] [Google Scholar]
- Chronis-Tuscano A, Degnan KA, Pine DS, Perez-Edgar K, Henderson HA, Diaz Y, Fox NA. Stable early maternal report of behavioral inhibition predicts lifetime social anxiety disorder in adolescence. Journal of the American Academy of Child & Adolescent Psychiatry. 2009;48(9):928–935. doi: 10.1097/CHI.0b013e3181ae09df. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark LA. Temperament as a unifying basis for personality and psychopathology. Journal of Abnormal Psychology. 2005;114(4):505–521. doi: 10.1037/0021-843X.114.4.505. [DOI] [PubMed] [Google Scholar]
- Clarke K, Cooper P, Creswell C. The parental overprotection scale: Associations with child and parental anxiety. Journal of Affective Disorders. 2013;151(2):618–624. doi: 10.1016/j/jad.2013.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clauss JA, Blackford JU. Behavioral inhibition and risk for developing social anxiety disorder: A meta-analytic study. Journal of the American Academy of Child and Adolescent Psychiatry. 2012;51(10):1066–1075.el. doi: 10.1016/j.jaac.2012.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coplan RJ, Wilson J, Frohlick SL, Zelenski J. A person-oriented analysis of behavioral inhibition and behavioral activation in children. Personality and Individual Differences. 2006;41(5):917–927. doi: 10.1016/j.paid.2006.02.019. [DOI] [Google Scholar]
- Davis M, Suveg C. Focusing on the positive: A review of the role of child positive affect in developmental psychopathology. Clinical Child and Family Psychology Review. 2014;17(2):97–124. doi: 10.1007/s10567-013-0162-y. [DOI] [PubMed] [Google Scholar]
- Degnan KA, Almas AN, Fox NA. Temperament and the environment in the etiology of childhood anxiety. Journal of Child Psychiatry and Psychology. 2010;51(4):497–517. doi: 10.1111/j.1469-7610.2010.02228.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Degnan KA, Henderson HA, Fox NA, Rubin KH. Predicting social wariness in middle childhood: The moderating roles of child care history, maternal personality and maternal behavior. Social Development. 2008;17(3):471–487. doi: 10.1111/j.14679507.2007.00437.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doey L, Coplan RJ, Kingsbury M. Bashful boys and coy girls: A review of gender differences in childhood shyness. Sex Roles. 2014;70(7):255–266. doi: 10.1007/s11199-0130317-9. [DOI] [Google Scholar]
- Dunn LM, Dunn LM. Peabody Picture Vocabulary Test. 3rd. Circle Pines, Minnesota: American Guidance Service; 1997. [Google Scholar]
- Durbin CE, Hayden EP, Klein DN, Olino TM. Stability of laboratory-assessed temperamental emotionality traits from ages 3 to 7. Emotion. 2007;7(2):388–399. doi: 10.1037/1528-3542.7.2.388. [DOI] [PubMed] [Google Scholar]
- Durbin CE, Klein DN, Hayden EP, Buckley ME, Moerk KC. Temperamental emotionality in preschoolers and parental mood disorders. Journal of Abnormal Psychology. 2005;114(1):28–37. doi: 10.1037/0021-843X.114.1.28. [DOI] [PubMed] [Google Scholar]
- Edwards SL, Rapee RM, Kennedy S. Prediction of anxiety symptoms in preschool-aged children: Examination of maternal and paternal perspectives. Journal of Child Psychology and Psychiatry, and Allied Disciplines. 2010;51(3):313–21. doi: 10.1111/j.1469-7610.2009.02160.x. [DOI] [PubMed] [Google Scholar]
- Egger HL, Ascher BH, Angold A. The Preschool Age Psychiatric Assessment: Version 1.1. Durham, NC: Center for Developmental Epidemiology, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center; 1999. [Google Scholar]
- Essex MJ, Slattery MH, Goldsmith MJ, Hill H, Kalin NH. Early risk factors and developmental pathways to chronic high inhibition and social anxiety disorder in adolescence. The American Journal of Psychiatry. 2010;167(1):40–46. doi: 10.1176/appi.ajp.2009.07010051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox NA, Henderson HA, Marshall PJ, Nichols KE, Ghera MM. Behavioural inhibition: Linking biology and behaviour within a developmental framework. Annual Review of Psychology. 2005;56:235–262. doi: 10.1146/annurev.psych.55.090902.141532. [DOI] [PubMed] [Google Scholar]
- Gest SD. Behavioural inhibition: Stability and associations with adaptation from childhood to early adulthood. Journal of Personality and Social Psychology. 1997;72(2):467–475. doi: 10.1037/0022-3514.72.2.467. [DOI] [PubMed] [Google Scholar]
- Goldsmith HH, Lemery KS. Linking temperamental fearfulness and anxiety symptoms: A behavior-genetic perspective. Biological Psychiatry. 2000;48(12):1199–1209. doi: 10.1016/S0006-3223(00)01003. [DOI] [PubMed] [Google Scholar]
- Goldsmith HH, Reilly J, Lemery KS, Longley S, Prescott A. Laboratory Temperament Assessment Battery: Preschool version. 1995 Unpublished manuscript. [Google Scholar]
- Gray JA. The psychophysiological basis of introversion-extraversion. Behaviour Research and Therapy. 1970;8(3):249–266. doi: 10.1016/0005-7967(70)90069-0. [DOI] [PubMed] [Google Scholar]
- Hane AA, Cheah C, Rubin KH, Fox NA. The role of maternal behaviour in the relation between shyness and social reticence in early childhood and social withdrawal in middle childhood. Social Development. 2008;17(4):795–811. doi: 10.1111/j.1467-9507.2008.00481.x. [DOI] [Google Scholar]
- Hayes AF, Matthes J. Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behavior Research Methods. 2009;41(3):924–936. doi: 10.3758/BRM.41.3.924. [DOI] [PubMed] [Google Scholar]
- Hirshfeld-Becker DR, Biederman J, Henin A, Faraone SV, Davis S, Harrington K, Rosenbaum JF. Behavioral inhibition in preschool children at risk is a specific predictor of middle childhood social anxiety: A five-year follow-up. Journal of Developmental and Behavioral Pediatrics. 2007;28(3):225–33. doi: 10.1097/01.DBP.0000268559.34463.d0. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB. Four factor index of social status 1975 [Google Scholar]
- Hubert NC, Wachs TD, Peters-Martin P, Gandour MJ. The study of early temperament: Measurement and conceptual issues. Child Development. 1982;53(3):571–600. doi: 10.2307/1129370. [DOI] [Google Scholar]
- Hutt RL, Buss KA, Kiel EJ. Caregiver protective behavior, toddler fear and sadness, and toddler cortisol reactivity in novel contexts. Infancy. 2013;18(5):708–728. doi: 10.1111/j.1532-7078.2012.00141.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson PO, Fay LC. The Johnson-Neyman technique, its theory and application. Psychometrika. 1950;15:349–367. doi: 10.1007/BF02288864. [DOI] [PubMed] [Google Scholar]
- Karevold E, Coplan R, Stoolmiller M, Mathiesen KS. A longitudinal study of the links between temperamental shyness, activity, and trajectories of internalising problems from infancy to middle childhood. Australian Journal of Psychology. 2011;63:36–43. doi: 10.1111/j.1742-9536.2011.00005.x. [DOI] [Google Scholar]
- Kiel EJ, Buss KA. Maternal accuracy and behavior in anticipating children’s responses to novelty: Relations to fearful temperament and implications for anxiety development. Social Development. 2010;19(2):304–325. doi: 10.1111/j.1467-9507.2009.00538.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kiel EJ, Buss KA. Associations among context-specific maternal protective behavior, toddlers’ fearful temperament, and maternal accuracy and goals. Social Development. 2012;21(4):742–760. doi: 10.1111/j.1467-9507.2011.00645.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knafo A, Jaffee SR. Gene-environment correlation in developmental psychopathology. Development and Psychopathology. 2013;25(1):1–6. doi: 10.1017/S0954579412000855. [DOI] [PubMed] [Google Scholar]
- Laptook RS, Klein DN, Olino TM, Dyson MW, Carlson G. Low positive affectivity and behavioral inhibition in preschool-age children: A replication and extension of previous findings. Personality and Individual Differences. 2010;48(5):547–551. doi: 10.1016/j.paid.2009.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis-Morrarty E, Degnan KA, Chronis-Tuscano A, Rubin KH, Cheah CSL, Pine DS, Fox NA. Maternal over-control moderates the association between early childhood behavioral inhibition and adolescent social anxiety symptoms. Journal of Abnormal Child Psychology. 2012;40(8):1363–1373. doi: 10.1007/s10802-012-9663-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackrell SVM, Sheikh HI, Kotelnikova Y, Kryski KR, Jordan PL, Singh SM, Hayden EP. Child temperament and parental depression predict cortisol reactivity to stress in middle childhood. Journal of Abnormal Psychology. 2014;123(1):106–116. doi: 10.1037/a0035612. doi: http://dx/doi.org/10.1037/a0035612. [DOI] [PubMed] [Google Scholar]
- Muris P, van Brakel AML, Arntz A, Schouten E. Behavioral inhibition as a risk factor for the development of childhood anxiety disorders: A longitudinal study. Journal of Child and Family Studies. 2011;20(2):157–170. doi: 10.1007/s10826-010-9365-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murray L, Creswell C, Cooper PJ. The development of anxiety disorders in childhood: An integrative review. Psychological Medicine. 2009;39(9):1413–1423. doi: 10.1017/S0033291709005157. [DOI] [PubMed] [Google Scholar]
- Naragon-Gainey K, Watson D, Markon KE. Differential relations of depression and social anxiety symptoms to the facets of extraversion/positive emotionality. Journal of Abnormal Psychology. 2009;118(2):299–310. doi: 10.1037/a0015637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olino TM, Klein DN, Dyson MW, Rose SA, Durbin CE. Temperamental emotionality in preschool-aged children and depressive disorders in parents: Associations in a large community sample. Journal of Abnormal Psychology. 2010;119(3):468–78. doi: 10.1037/a0020112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park SY, Belsky J, Putnam S, Crnic K. Infant emotionality, parenting, and 3-year inhibition: Exploring stability and lawful discontinuity in a male sample. Developmental Psychology. 1997;33(2):218–27. doi: 10.1037/0012-1649.33.2.218. [DOI] [PubMed] [Google Scholar]
- Pfeifer M, Goldsmith HH, Davidson RJ, Rickman M. Continuity and change in inhibited and uninhibited children. Child Development. 2002;73(5):1474–1485. doi: 10.1111/1467-8624.00484. [DOI] [PubMed] [Google Scholar]
- Robinson CC, Mandleco B, Olsen SF, Hart CH. The Parenting Styles and Dimensions Questionnaire (PSDQ) In: Perlmutter BF, Touliatos J, Holden GW, editors. Handbook of family measurement techniques: Vol. 3. Instruments & index. Thousand Oaks: Sage; 2001. pp. 319–321. [Google Scholar]
- Robinson JL, Kagan J, Reznick JS, Corley R. The heritabliity of inhibited and uninhibited behavior: A twin study. Developmental Psychology. 1992;28(6):1030–1037. doi: 10.1037/0012-1649.28.6.1030. [DOI] [Google Scholar]
- Root AK, Stifter C. Temperament and maternal emotion socialization beliefs as predictors of early childhood social behavior in the laboratory and classroom. Parenting: Science and Practice. 2010;10(4):241–257. doi: 10.1080./15295192.2010.492035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rotge JY, Grabot D, Aouizerate B, Pélissolo A, Lépine JP, Tignol J. Childhood history of behavioral inhibition and comorbidity status in 256 adults with social phobia. Journal of Affective Disorders. 2011;129(1–3):338–41. doi: 10.1016/j.jad.2010.07.031. [DOI] [PubMed] [Google Scholar]
- Rothbart MK, Bates JE. Temperament. In: Eisenberg N, Damon W, Lerner RM, editors. Handbook of child psychology: Vol. 3. Social, emotional, and personality development. 6th. Hoboken, NJ: John Wiley and Sons Inc; 2006. pp. 99–166. [Google Scholar]
- Rubin KH, Burgess KB, Hastings PD. Stability and social-behavioralconsequences of toddlers’ inhibited temperament and parenting behaviors. Child Development. 2002;73(2):483–495. doi: 10.1111/1467-8624.00419. [DOI] [PubMed] [Google Scholar]
- Rubin KH, Hastings PD, Stewart SL, Henderson HA, Chen X. The consistency and concomitants of inhibition: Some of the children, all of the time. Child Development. 1997;68(3):467–483. doi: 10.2307/1131672. [DOI] [PubMed] [Google Scholar]
- Rutter M. Resilience as a dynamic concept. Development and Psychopathology. 2012;24:335–344. doi: 10.1017/S0954579412000028. [DOI] [PubMed] [Google Scholar]
- Scarpa A, Raine A, Venables PH, Mednick SA. The stability of inhibited/uninhibited temperament from ages 3 to 11 years in Mauritian children. Journal of Abnormal Child Psychology. 1995;23(5):607–618. doi: 10.1007/BF01447665. [DOI] [PubMed] [Google Scholar]
- Shrout PE. Measurement reliability and agreement in psychiatry. Statistical Methods in Medical Research. 1998;7(3):301–317. doi: 10.1177/096228029800700306. [DOI] [PubMed] [Google Scholar]
- Tugade MM, Fredrickson BL. Resilient individuals use positive emotions to bounce back from negative emotional experiences. Journal of Personality and Social Psychology. 2004;86(2):320–333. doi: 10.1037/0022-3514.86.2.320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van den Akker AL, Deković M, Prinzie P, Asscher JJ. Toddlers’ temperament profiles: Stability and relations to negative and positive parenting. Journal of Abnormal Child Psychology. 2010;38(4):485–495. doi: 10.1007/s10802-009-9379-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wichers MC, Myin-Germeys I, Jacobs N, Peeters F, Kenis G, Derom C, Vlietinck, Delespaul P, van Os J. Evidence that moment-to-moment variation in positive emotions buffer genetic risk for depression: A momentary assessment twin study. Acta Psychiatrica Scandinavica. 2007;115(6):451–457. doi: 10.1111/j.1600-0447.2006.00924.x. [DOI] [PubMed] [Google Scholar]
- Wills TA, Sandy JM, Yaeger A, Shinar O. Family risk factors and adolescent substance use: Moderation effects for temperament dimensions. Developmental Psychology. 2001;37(3):283–297. doi: 10.1037//0012-1649.37.3.283. [DOI] [PubMed] [Google Scholar]
- Wu G, Feder A, Cohen H, Kim JJ, Calderon S, Charney DS, Mathé AA. Understanding resilience. Frontiers in Behavioral Neuroscience. 2013;7:1–15. doi: 10.3389/fnbeh.2013.00010. [DOI] [PMC free article] [PubMed] [Google Scholar]