

Abstract
Purpose
The purpose of this study was to assess the causes and possible solutions for patient dissatisfaction after the implantation of presbyopia-correcting intraocular lenses (IOLs).
Methods
This study was a retrospective review of clinical records. All patients who were seen between January 2009 and December 2013 whose primary reason for consultation was dissatisfaction with visual performance after presbyopia-correcting IOL implantation were included in the study. A single treating physician, who determined the most probable cause of dissatisfaction, decided which interventions to pursue following the initial consultation.
Results
Data from 74 eyes of 49 patients were analyzed. The most common cause for complaint was blurry or foggy vision both for distance and near (68%). Complaints were most frequently attributed to residual refractive error (57%) and dry eye (35%). The most common interventions pursued were treatment of refractive error with glasses or contact lenses (46%) and treatment for dry eye (24%). Corneal laser vision correction was done in 8% of eyes; 7% required an IOL exchange. After the interventions, 45% of patients had completed resolution of symptoms, 23% of patients were partially satisfied with the results, and 32% remained completely dissatisfied with the final results.
Conclusion
The most identifiable causes of dissatisfaction after presbyopia-correcting IOL implantation are residual refractive error and dry eye. Most patients can be managed with conservative treatment, though a significant number of patients remained unsatisfied despite multiple measures.
Keywords: intraocular lens, cataract, presbyopia, multifocal intraocular lens
Introduction
Over the past several decades, due to rapid technological advances and changing practice patterns, cataract surgery has become a form of refractive surgery. As a result, patients have come to expect excellent unaided distance vision. With the introduction of multifocal and pseudo-accommodating intraocular lenses (IOLs), many patients request and expect spectacle independence for near tasks as well. Typically, options include monovision or presbyopia-correcting IOLs (PC-IOL).1 It has been reported that monovision has a lower rate of explantation, but PC-IOLs might achieve higher rates of spectacle independence for near tasks.2
Most patients who undergo PC-IOL implantation are satisfied with the results.3 In spite of optical tradeoffs, like lower contrast sensitivity or photic phenomena expected after their implantation, most patients either do not notice these aberrations or understand the compromise in quality that was required to achieve spectacle independence.4–8
Advanced technology lenses tend to be less forgiving with regard to technique, power calculation, ocular comorbidities, and patient selection (Figure 1).9 Comorbidities such as dry eye, vitreomacular pathology, or a decentered lens, which might cause only minor issues after a monofocal IOL implantation, may become intolerable for the multifocal IOL patient.9–15
Figure 1.
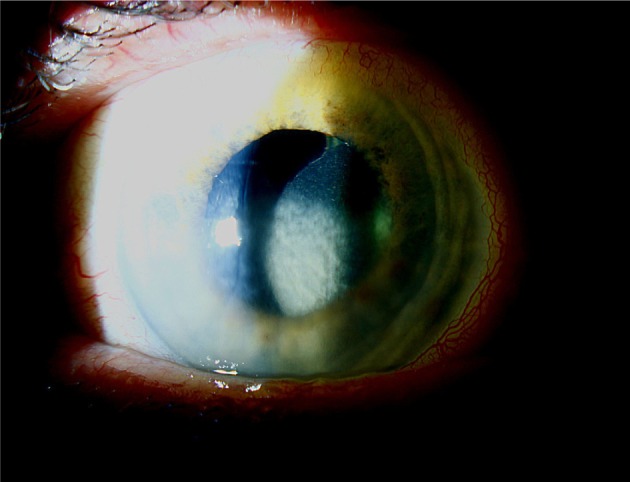
Clinical photograph of a patient presenting to our clinic with complaints of blurred vision after cataract surgery with a multifocal IOL.
Notes: There is a decentered lens with marked inferior corneal edema due to a broken haptic in the inferior angle. The patient was very satisfied even after an IOL exchange; the corneal edema subsided after the removal of the haptic.
Abbreviation: IOL, intraocular lens.
Unrealistic expectations, residual refractive error, posterior capsular opacification, ocular surface disease, macular pathology, and intraoperative complications can lead to dissatisfaction after presbyopia-correcting IOLs.12–14,16,17
The purpose of this study was to assess the causes and possible solutions for patient dissatisfaction after the implantation of presbyopia-correcting IOLs.
Methods
A retrospective review was conducted for 49 consecutive patients, comprising 74 affected eyes, with visual complaints after multifocal IOL implantation presenting to Bascom Palmer Eye Institute between January 2009 and December 2013. Patients who had surgery performed at Bascom Palmer Eye Institute and those referred from other centers were included in the study. Data collected included the type of IOL implanted, nature of the visual complaint, uncorrected and best spectacle-corrected visual acuity for distance and near after cataract surgery, key features of the clinical examination, cause of symptoms, nature of the treatment modality selected for each complaint, and presence or absence of clinical improvement after treatment.
The protocol was approved by the Institutional Review Board of Medical Science, University of Miami Miller School of Medicine (N°: 20140300; June 19, 2014). Patient data were collected and maintained in accordance with Health Insurance Portability and Accountability Act guidelines. Due to the retrospective nature of the study and as the clinical pictures contain no identifying information, no patient consent was required.
The different model lenses included in the study were (in order of descending frequency; Table 1) ReSTOR (SN6AD1 and SN6AD3; Alcon Laboratories, Inc.), Crystalens (Bausch & Lomb Incorporated), Tecnis ZMA00 (Abbott Medical Optics Inc.), ReZoom (Abbott Medical Optics Inc.), and Array lens (SA40N; Abbott Medical Optics Inc.). Further breakdown by specific lens model (ie, SN60D1 versus SN60D3) was not possible in every case, due to the fact that some patients had their surgery at an outside institution and the information of the specific lens model was not available.
Table 1.
Different models of presbyopia-correcting IOLs included in this series of patients dissatisfied with presbyopia-correcting IOLs
| Presbyopia-correcting IOL | N (%) |
|---|---|
| Multifocal | 57 (77.0) |
| ReSTOR | 44 (59.4) |
| Tecnis | 9 (12.2) |
| ReZoom | 3 (4.1) |
| Array | 1 (1.3) |
| Pseudo accommodating | |
| Crystalens | 17 (23.0) |
Abbreviation: IOL, intraocular lens.
When possible, the presumed cause of the dissatisfaction, which was determined on the basis of history and physical exam, was divided into preoperative, intraoperative, and postoperative causes.
For the purpose of discussion, dry eye was classified as a preoperative occurrence. Even though dry eye symptoms have been reported to appear de novo in previously asymptomatic individuals, in most patients it consists of worsening of a previous condition.18 Dry eye was diagnosed by surface staining with fluorescein and/or topographic indexes. Also, for the purpose of this study, residual refractive error was grouped with postoperative causes, due to the fact that we can safely assume the surgeon did everything in his power to avoid residual ametropia.
Statistical analysis was performed using SPSS for Windows (version 15.0, SPSS Inc.). The appropriate statistical test was chosen for each data set (Fisher’s exact test, Kruskal–Wallis test, and Mann–Whitney test), and a P-value <0.05 was considered significant. In the analysis of visual acuity, three eyes had missing data, either for distance or for near; thus, they were excluded from the visual acuity analysis.
Results
This study included 74 eyes from 49 patients; Table 2 summarizes the demographics and presenting characteristics of the patients included in this study. Of the total number of patients, 25 (51%) of them presented with bilateral complaints. Sixteen eyes (22%) had undergone surgery at Bascom Palmer Eye Institute; the remaining were referred or arrived as self-referrals from other institutions. A number of different models of IOLs were included, with the ReSTOR (SN6AD1 and SN6AD3) lens being the most represented in this study (Table 1).
Table 2.
Demographic characteristics of patients dissatisfied with presbyopia-correcting IOLs presenting to our clinic for evaluation
| Demographic characteristic | N (% or range) |
|---|---|
| Eyes | 74 |
| Age (years) | 67.2±9.1 |
| Sex | |
| Male eyes | 25 (36.7) |
| Female eyes | 49 (63.3) |
| Time to presentation (months) | 25.5±25.3 |
| Mean manifest refraction | |
| Sphere (D) | −0.6±0.8 (−3.3–1.5) |
| Cylinder (D) | 0.7±0.6 (0–2.5) |
| Mean SE (D) | −0.3±0.8 (−3.0–2.3) |
Abbreviations: IOL, intraocular lens; SE, standard error.
The chief complaint of 29 (59%) of our patients was blurry vision, both for distance and near; this was seen in 50 eyes (68%). Also, of the eight (16%) patients who complained of problems only with insufficient near vision, all had bilateral Crystalens implantation. After blurry vision, the next most frequent complaints included photic phenomena and multiple images (Table 3).
Table 3.
Chief complaint of patients presenting to our clinic who were dissatisfied with presbyopia-correcting IOLs
| Chief complaint, per eye | N (%) |
|---|---|
| Blurry/waxy/foggy vision | |
| Distance and near | 50 (67.6) |
| Only near | 16 (21.6) |
| Only distance | 6 (8.1) |
| Photic phenomena | |
| Negative dysphotopsia | 1 (1.4) |
| Halo/glare | 8 (10.8) |
| Multiple images/ghosting | 8 (10.8) |
Abbreviation: IOL, intraocular lens.
Uncorrected distance visual acuity was on average 20/40 (logarithm of the minimum angle of resolution [logMAR] 0.3±0.2), and 20/25 vision or better was achieved by 26.8% of eyes. The corrected distance visual acuity was on average 20/25 (logMAR 0.1±0.1), and it was 20/25 or better in 69% of eyes. The uncorrected near visual acuity of J1 was achieved by 45% of eyes; when corrected for near this improved to 86% of eyes (Table 4).
Table 4.
Presenting visual acuities of patients presenting to our clinic dissatisfied with presbyopia-correcting IOLs
| Visual acuity | N (%) | N (%) |
|---|---|---|
| Distance acuity | Uncorrected | Distance corrected |
| 20/25 or more | 19 (26.8) | 49 (69.0) |
| 20/30 or less | 52 (73.2) | 22 (31.0) |
| Near visual acuity | Uncorrected | Near corrected |
| J1 or better | 32 (45.1) | 61 (85.9) |
| J2–J3 | 16 (22.5) | 6 (8.5) |
| J4 or worse | 23 (32.4) | 4 (5.6) |
Abbreviation: IOL, intraocular lens.
Sixty-three percent of eyes had a presumed preoperative cause of dissatisfaction. The leading preoperative cause was dry eye syndrome (35%); both aqueous deficient and evaporative dry eye were prevalent in this group (Table 5). Another group had a definable and preexisting ocular pathology, such as Fuchs’ endothelial dystrophy, epiretinal membrane, cystoid macular edema, age-related macular degeneration, anterior basement membrane dystrophy, or strabismus. In addition, we identified a group of patients with unrealistic expectations. With regard to the latter group, quotes like “my doctor said I would see like when I was 20 years old” or “I was led to believe that I wouldn’t have to use glasses ever again” were used to describe their heightened expectations. Other patients expected to see clearly at all focal points and were disappointed with either their near or intermediate vision when the near focal point was either closer or further than their expected target. One patient reported that he was unable to read in dim lighting with his multifocal IOL.
Table 5.
Chief complaint of patients presenting to our clinic dissatisfied with presbyopia-correcting IOLs
| Presumed cause of dissatisfaction | N (%) |
|---|---|
| Preoperative issues | |
| Dry eyes | 26 (35) |
| Other preexisting pathologiesa | 15 (20) |
| Unreasonable expectations | 6 (8) |
| Intraoperative issues | |
| Evidence of surgical complications | 6 (8) |
| Postoperative issues | |
| Residual refractive error | 42 (57) |
| Visual disturbance | 19 (26) |
| Postoperative complications | 3 (4) |
Note:
Other preexisting pathologies: Fuchs’ endothelial dystrophy, epiretinal membrane, cystoid macular edema, age-related macular degeneration, anterior basement membrane dystrophy, strabismus.
Abbreviation: IOL, intraocular lens.
Intraoperative causes (Table 5) were relatively infrequent, presenting in only 8% of the eyes; they mainly consisted of vitreous loss with a sulcus lens placement. These were usually accompanied by a myopic shift, presumably from the anterior displacement of the effective lens position. Three eyes had an accompanying epiretinal membrane that further distorted image quality. In one patient, we identified a damaged IOL accompanying a decompensated cornea (Figure 1).
Postoperative causes of dissatisfaction (Table 5) were explained by residual refractive error, which by itself constituted 28.4% of attributed causes and in combination with other causes explained 57% of dissatisfaction. Postoperative complications also accounted for some causes of dissatisfaction: uveitis, retinal detachment, EKC, and lens dislocation occurred in one eye each.
Pseudophakic dysphotopsias, defined as any positive or negative photic phenomena, as previously defined by Woodward et al,14 were present in 26% of our eyes. It constituted the sole cause of complaint in only two patients, in whom the rest of the examination was normal.
It was determined that 46 eyes (62%) had only one identified cause for the presenting cause of dissatisfaction. The other 28 eyes had either two identifiable causes (22 eyes, 30%) or three defined causes (six eyes, 8%). The most frequent concurrent complaints were residual refractive errors in combination with dry eyes (12 eyes, 16%).
As seen in Table 6, there were multiple interventions attempted, according to the presumed cause of unhappiness. Most patients were managed medically, with treatment of their dry eye and/or residual refractive error; some patients received pilocarpine 1% drops. Dry eye patients were managed with artificial tears, gel tears, topical cyclosporine, and punctal plugs, depending on the severity of presentation. Residual refractive error was treated conservatively according to patient preference, with glasses or contact lenses. Other interventions included YAG capsulotomy, corneal laser vision correction, and IOL exchange.
Table 6.
Main intervention and outcomes of patients presenting to our clinic dissatisfied with presbyopia-correcting IOLs
| Interventions and outcomes | N (%) |
|---|---|
| Intervention | |
| Glasses/contacts | 34 (46.0) |
| Treatment of dry eye | 18 (24.3) |
| YAG capsulotomy | 9 (12.2) |
| LASIK or PRK | 6 (8.1) |
| IOL exchange | 5 (6.8) |
| Pilocarpine | 9 (12.2) |
| Outcomes | |
| Happy/resolved issue | 33 (44.6) |
| Partially resolved | 17 (23.0) |
| Dissatisfied | 24 (32.4) |
Abbreviation: IOL, intraocular lens.
The outcomes after intervention varied. Forty-five percent of the patients had complete resolution of symptoms, 23% were partially satisfied, and 32% remained completely dissatisfied with the final results (Table 6). Of the patients who were treated with pilocarpine 1%, only one out of nine found it useful, but even that patient, with bilateral complaints, discontinued it after a short period. The YAG laser group (12% of eyes) responded quite well to the intervention; all but one was satisfied after the procedure, and this patient had a coexisting epiretinal membrane. Of the patients who underwent corneal laser vision correction (six in total; 8% of eyes), all were satisfied with the results and complaints disappeared after the intervention. The patients who underwent an IOL exchange for a monofocal lens targeted at distance (five in total; 7% of eyes) had poor perceived outcomes, as four of them remained dissatisfied with their vision. After the IOL exchange, a patient with a decompensated cornea had a favorable outcome only after a Descemet’s stripping endothelial keratoplasty was performed.
When analyzed by lens type or model, we could find no statistically significant difference in the post-intervention satisfaction rates among different IOLs (NSS). Of the patients presenting with a Crystalens (17 eyes), 47% were satisfied after the intervention, 12% were partially satisfied, and 41% persisted unsatisfied in spite of all treatment modalities. Of the eyes presenting with ReSTOR lenses (44 eyes), 34% were satisfied after intervention, 32% were partially satisfied, and 34.1% were not satisfied with any treatment offered.
Discussion
This study confirms that uncorrected blurry vision is the main cause of dissatisfaction after presbyopia-correcting IOL implantation. The main identifiable cause of blurred vision was residual refractive error and dry eye syndrome. Even though dissatisfaction after a presbyopia-correcting IOLs constitutes a relatively uncommon reason for consultation, as these IOLs continue to penetrate the market, even uncommon events could become prevalent due to the high number of cataract surgeries performed annually.
The first step in preventing patient dissatisfaction involves proper patient selection. In this series, we found that 20% of eyes had preexisting pathology that could have made the surgeon reconsider implanting a PC-IOL (Table 5). Furthermore, the lack of evidence of outcomes with any ocular comorbidity should make surgeons cautious when choosing advanced technology IOLs.19,20 Another 8% of patients had intraoperative complications that, even though managed appropriately, should have made the surgeon consider the possibility of implanting a monofocal IOL. In the literature, sulcus placement of multifocal IOLs results in a 27% rate of glare and haloes.21 In actuality, none of these lenses are approved or recommended for sulcus placement as they are one piece acrylic lenses, which may be associated with iris chafing, iritis, and glaucoma when placed in the sulcus.
As in other series, residual refractive error had a high prevalence in our group of patients.13 It played a role alone or in conjunction with other conditions in over half of the cases in this series. Careful biometry with personalization of constants and meticulous management of astigmatism could potentially prevent patient dissatisfaction in a large number of cases. Fortunately, most refractive errors were on the myopic side, which helped to explain why the presenting unaided visual acuity for near was relatively good (J1 or better) in 45% of eyes, but excellent unaided distance vision (20/25 or better) was only present in 27%.
In this series, ocular surface issues (Figure 2) also played a significant role in patient dissatisfaction; this did not hold true in two previously published series.13,14 Identification and pretreatment of ocular surface issues could be another effective way of minimizing patient dissatisfaction. We know that dry eye has been shown to appear de novo in previously asymptomatic individuals, but it is agreed that in most patients it consists of worsening of a preexisting condition.18 An aggressive preoperative screening protocol for ocular surface disease and pretreatment in borderline or subclinical cases is appropriate.22 Even the possibility of withholding an advanced technology IOL in patients with overt ocular surface disease may be advised in severe cases.
Figure 2.
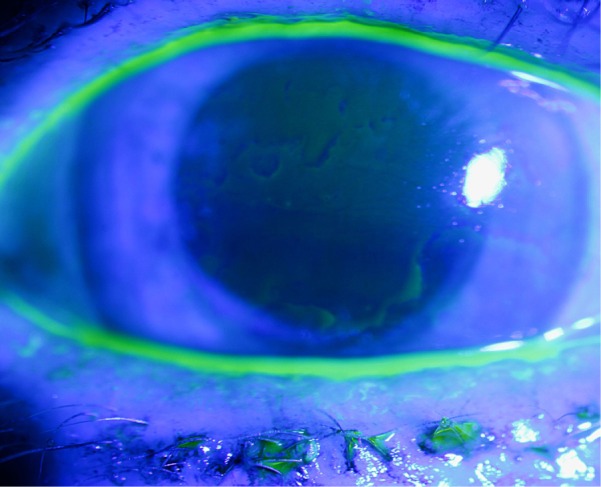
Clinical photograph of a patient presenting to our clinic with complaints of blurred vision after cataract surgery with a multifocal IOL.
Note: Signs of anterior basement dystrophy are present; the ocular surface disturbance is more evident when fluorescein is used to stain the cornea.
Abbreviation: IOL, intraocular lens.
Most causes of patient dissatisfaction can be managed conservatively without surgical intervention. Communication and an open discussion with the patient, acknowledging what the patient is experiencing and explaining the phenomenon, treatment of ocular surface disease, and spectacles for specific visual tasks all help promote better satisfaction without the need for surgical intervention. In this series, refractive error (57%) and dry eye (35%) were the two main causes of dissatisfaction amenable to conservative treatment.
After intervention, 68% of the eyes experienced complete or significant resolution of symptoms, but 32% of the eyes remained dissatisfied with the results. It must be said that this number includes patients who failed conservative treatment and refused further surgical intervention. This is in line with the previous literature, where Woodward et al14 found 81% improvement with conservative treatment and de Vries et al13 found that 84% of patients were able to improve with conservative measures.
It is established in the literature that rates of dissatisfaction as high as 83.3% and 94.6% can be resolved after IOL exchange.12–17 Still, one must be cautious when opting for this surgical intervention, as there are many etiologies for patient unhappiness. This is why we agree that the causes of dissatisfaction must be addressed in an orderly and standardized fashion, as many can be resolved without surgical intervention.14 For example, performing an IOL exchange in an eye with ocular surface disease will not solve the underlying problem and may be associated with significant risks associated with intraocular surgery.
This study is limited in its retrospective nature. Nonetheless, a prospective and randomized trial involving patients of this nature would be very difficult to implement. Also, the sample size is comparable to other series but the variety of IOLs represented here is greater than in previously reported studies. Consult bias also makes it difficult to make a study of this type in one institution, as dissatisfied patients tend to change the physician and/or the institutions caring for them.
In short, we believe that patient satisfaction with presbyopia-correcting IOLs may be improved through the following four steps:
Education: have an open conversation with complete disclosure of the risks and benefits of these specific lenses. In this way, the patient will have reasonable expectations as to what is to be gained and the inevitable optical tradeoff for each lens.
Aggressive identification, prevention, and treatment of ocular surface disease can help improve patient satisfaction with presbyopia-correcting IOLs.22
Refractive target: must be within 0.5 D of the refractive target with a multifocal IOL and minimize residual astigmatism.23
Avoid patients with significant preexisting pathology or in whom intraoperative events can lead to dissatisfaction. A careful history and comprehensive ophthalmological examination, with appropriate ancillary studies when necessary (optical coherence tomography and corneal topography), should help identify most of the patients with ocular comorbidities in whom we should steer away from these lenses.
Prevention is the key, and one may consider alternatives to presbyopia-correcting IOLs like monovision.1 If a presbyopia-correcting IOL is placed and the surgeon faces a dissatisfied patient, open communication is vital. Furthermore, it is important to remember that such dissatisfaction is uncommon, presentation is varied, and causes are multiple. Most complaints can be resolved with simple interventions (ie, reassurance, drops, and/or spectacles), and explantation is rarely required, as seen in this series. Referral for a second opinion is very effective and may also be considered for those patients who remain dissatisfied despite the aforementioned measures.
Footnotes
Disclosure
Dr Donaldson is a consultant for Abbott Medical Optics and Alcon. The other authors report no conflicts of interest in this work.
References
- 1.Finkelman YM, Ng JQ, Barrett GD. Patient satisfaction and visual function after pseudophakic monovision. J Cataract Refract Surg. 2009;35(6):998–1002. doi: 10.1016/j.jcrs.2009.01.035. [DOI] [PubMed] [Google Scholar]
- 2.Wilkins MR, Allan BD, Rubin GS, et al. Randomized trial of multifocal intraocular lenses versus monovision after bilateral cataract surgery. Ophthalmology. 2013;120(12):2449.e1–2455.e1. doi: 10.1016/j.ophtha.2013.07.048. [DOI] [PubMed] [Google Scholar]
- 3.Pepose JS. Maximizing satisfaction with presbyopia-correcting intraocular lenses: the missing links. Am J Ophthalmol. 2008;146(5):641–648. doi: 10.1016/j.ajo.2008.07.033. [DOI] [PubMed] [Google Scholar]
- 4.de Vries NE, Franssen L, Webers CA, et al. Intraocular straylight after implantation of the multifocal AcrySof ReSTOR SA60D3 diffractive intraocular lens. J Cataract Refract Surg. 2008;34(6):957–962. doi: 10.1016/j.jcrs.2008.02.016. [DOI] [PubMed] [Google Scholar]
- 5.Hida WT, Motta AF, Kara-José N, Junior, et al. Comparison between OPD-scan results and visual outcomes of monofocal and multifocal intraocular lenses. Arq Bras Oftalmol. 2009;72(4):526–532. doi: 10.1590/s0004-27492009000400017. [DOI] [PubMed] [Google Scholar]
- 6.Mesci C, Erbil H, Ozdoker L, Karakurt Y, Bilge AD. Visual acuity and contrast sensitivity function after accommodative and multifocal intraocular lens implantation. Eur J Ophthalmol. 2010;20(1):90–100. doi: 10.1177/112067211002000112. [DOI] [PubMed] [Google Scholar]
- 7.Dick HB, Krummenauer F, Schwenn O, Krist R, Pfeiffer N. Objective and subjective evaluation of photic phenomena after monofocal and multifocal intraocular lens implantation. Ophthalmology. 1999;106(10):1878–1886. doi: 10.1016/S0161-6420(99)90396-2. [DOI] [PubMed] [Google Scholar]
- 8.Häring G, Dick HB, Krummenauer F, Weissmantel U, Kroncke W. Subjective photic phenomena with refractive multifocal and monofocal intraocular lenses. Results of a multicenter questionnaire. J Cataract Refract Surg. 2001;27(2):245–249. doi: 10.1016/s0886-3350(00)00540-x. [DOI] [PubMed] [Google Scholar]
- 9.Braga-Mele R, Chang D, Dewey S, et al. Multifocal intraocular lenses: relative indications and contraindications for implantation. J Cataract Refract Surg. 2014;40(2):313–322. doi: 10.1016/j.jcrs.2013.12.011. [DOI] [PubMed] [Google Scholar]
- 10.Cho YK, Kim MS. Dry eye after cataract surgery and associated intraoperative risk factors. Korean J Ophthalmol. 2009;23(2):65–73. doi: 10.3341/kjo.2009.23.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kasetsuwan N, Satitpitakul V, Changul T, Jariyakosol S. Incidence and pattern of dry eye after cataract surgery. PLoS One. 2013;8(11):e78657. doi: 10.1371/journal.pone.0078657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kamiya K, Hayashi K, Shimizu K, Negishi K, Sato M, Bissen-Miyajima H, Survey Working Group of the Japanese Society of Cataract and Refractive Surgery Multifocal intraocular lens explantation: a case series of 50 eyes. Am J Ophthalmol. 2014;158(2):215.e1–220.e1. doi: 10.1016/j.ajo.2014.04.010. [DOI] [PubMed] [Google Scholar]
- 13.de Vries NE, Webers CA, Touwslager WR, et al. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg. 2011;37(5):859–865. doi: 10.1016/j.jcrs.2010.11.032. [DOI] [PubMed] [Google Scholar]
- 14.Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. doi: 10.1016/j.jcrs.2009.01.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Barsam A, Voldman A, Donnenfeld E. Advanced technology IOLs in cataract surgery: management of the unhappy patient. Int Ophthalmol Clin. 2012;52(2):95–102. doi: 10.1097/IIO.0b013e31824b439c. [DOI] [PubMed] [Google Scholar]
- 16.Shimizu K, Ito M. Dissatisfaction after bilateral multifocal intraocular lens implantation: an electrophysiology study. J Refract Surg. 2011;27(4):309–312. doi: 10.3928/1081597X-20100804-01. [DOI] [PubMed] [Google Scholar]
- 17.Galor A, Gonzalez M, Goldman D, O’Brien TP. Intraocular lens exchange surgery in dissatisfied patients with refractive intraocular lenses. J Cataract Refract Surg. 2009;35(10):1706–1710. doi: 10.1016/j.jcrs.2009.05.022. [DOI] [PubMed] [Google Scholar]
- 18.Han KE, Yoon SC, Ahn JM, et al. Evaluation of dry eye and meibomian gland dysfunction after cataract surgery. Am J Ophthalmol. 2014;157(6):1144.e1–1150.e1. doi: 10.1016/j.ajo.2014.02.036. [DOI] [PubMed] [Google Scholar]
- 19.Teichman JC, Ahmed II. Intraocular lens choices for patients with glaucoma. Curr Opin Ophthalmol. 2010;21(2):135–143. doi: 10.1097/ICU.0b013e3283365154. [DOI] [PubMed] [Google Scholar]
- 20.Gayton JL, Seabolt RA. Clinical outcomes of complex and uncomplicated cataractous eyes after lens replacement with the AcrySof toric IOL. J Refract Surg. 2011;27(1):56–62. doi: 10.3928/1081597X-20100325-01. [DOI] [PubMed] [Google Scholar]
- 21.Aralikatti AK, Tu KL, Kamath GG, Phillips RP, Prasad S. Outcomes of sulcus implantation of Array multifocal intraocular lenses in second-eye cataract surgery complicated by vitreous loss. J Cataract Refract Surg. 2004;30(1):155–160. doi: 10.1016/S0886-3350(03)00654-0. [DOI] [PubMed] [Google Scholar]
- 22.Donnenfeld ED, Solomon R, Roberts CW, Wittpenn JR, McDonald MB, Perry HD. Cyclosporine 0.05% to improve visual outcomes after multifocal intraocular lens implantation. J Cataract Refract Surg. 2010;36(7):1095–1100. doi: 10.1016/j.jcrs.2009.12.049. [DOI] [PubMed] [Google Scholar]
- 23.Zheleznyak L, Kim MJ, MacRae S, Yoon G. Impact of corneal aberrations on through-focus image quality of presbyopia-correcting intraocular lenses using an adaptive optics bench system. J Cataract Refract Surg. 2012;38(10):1724–1733. doi: 10.1016/j.jcrs.2012.05.032. [DOI] [PubMed] [Google Scholar]