

Introduction
A pressing need exists to characterize mechanisms that underlie suicidal behaviors, particularly those that may be subject to therapeutic intervention. Multiple lines of evidence indicate that latent infection with toxoplasmosis may comprise such a measure. This is a parasitic disease that is caused by the protozoan toxoplasma gondii and that can infect most warm-blooded animals. Exposure may occur through contact with cat feces or through ingestion of contaminated water, soil or undercooked meat. Infection with toxoplasmosis is life-long, though variable over time in intensity, and is prevalent in all countries (Tenter, Heckeroth et al. 2000). It has long been considered a risk only to pregnant women and immuno-suppressed individuals but evidence is accumulating that infection may influence behavior in adverse ways.
Ecological investigations have shown correlations between national rates of toxoplasma antibody seropositivity and suicide (Lester 2010, Ling, Lester et al. 2011). A Danish prospective study of 45,788 newborns found that positive toxoplasmosis titers at birth significantly raised the likelihood of future suicide attempts and completed suicides (Pedersen, Mortensen et al. 2012). Similarly, a study of post-mortem titers found higher rates of seropositivity among those aged 38 to 58 who died by suicide in comparison to control subjects who had died from causes other than accidents (Samojlowicz, Borowska-Solonynko et al. 2013). As shown in Table 1, a number of case-control comparisons of suicide attempters to controls have shown significant differences in either toxoplasmosis IgG titers and/or seroprevalence, though in some reports this was true only in subgroups, or with the application of alternate thresholds for seropositivity.
Table 1.
Case-Control Studies of Toxoplasmosis Titers in Suicide Attempters
| Suicide Attempters | Controls | |
|---|---|---|
| Alvarado-Esquivel et al. 201317 | ||
| n | 156 | 127 |
| diagnosis | mixed | mixed |
| mean ± SD IgG | N/A | N/A |
| # (%) positive titer1 | 7 (4.5) | 10 (7.9) |
| Arling et al. 200912 | ||
| n | 81 | 158 |
| diagnosis | mood disorder | mood disorder & healthy |
| geometric mean (CI) IgG2 | 0.48 (0.40, 0.57) | 0.33 (0.28, 0.39) |
| # (%) positive titer | 11 (13.6) | 17 (10.8) |
| Okusaga et al. 201118 | ||
| n | 351 | 599 |
| diagnosis | schizophrenia | schizophrenia |
| mean ± SD IgG3 | N/A | N/A |
| # (%) seropositive3 | 146 (41.6) | 226 (37.7) |
| Yagmur et al. 201019 | ||
| n | 200 | 200 |
| diagnosis | mixed | healthy |
| mean ± SD IgG | N/A | N/A |
| # (%) seropositive4 | 82 (41.0) | 56 (28.0) |
| Zhang et al. 201220 | ||
| n | 54 | 30 |
| diagnosis | mixed | healthy |
| mean ± SD IgG5 | N/A | N/A |
| # (%) seropositive6 | 22 (40.7) | 6 (20.0) |
properties with IgG ≥ 150 IU/ml significantly diff., p=0.04
p=0.004
among subjects < median age of 38, significant differences for titers, p = 0.006 and, seroprevalence, p=0.01
p= 0.004
p=0.04, adjusted for age
p=0.008
The presence of toxoplasma also appears to increase proclivities toward accidents, possibly though mechanisms that resemble those that predispose to suicidal behaviors. In three independent samples, individuals involved in traffic accidents had higher rates of toxoplasmosis seropositivity (Yereli, Balcioglu et al. 2006) (Kocazeybek, Oner et al. 2009), or higher antibody titers (Flegr, Havlicek et al. 2002), than did healthy control individuals selected from the community. Recent reports have shown direct associations between toxoplasmosis seropositivity and trait measures of aggression and impulsivity (Cook, Brenner et al. 2015).
There are intriguing links between the above lines of evidence and those derived from rodent models of high-risk behaviors. The toxoplasma organism is believed to have evolved to promote the transmission of cysts from the tissue of various other mammals to a feline host, the only animal in which the parasite can progress to an oocyte stage. Toxoplasma cysts in the CNS have particularly high concentrations in the amygdala and frontal cortex (Vyas, Kim et al. 2007). In mice their presence results in a decrease in both aversion to the odor of cat urine (Vyas, Kim et al. 2007) and in the avoidance of novelty (Webster, Brunton et al. 1994) because novelty seeking appears to be highly correlated with impulsivity in suicide attempters (Ghanem, Gamaluddin et al. 2013) it is possible that the existence of toxoplasma in the CNS of humans promotes the impulsivity that characterizes many humans who attempt or complete suicide (Gvion and Apter 2011).
The mechanisms may lie in inflammatory response mounted against the parasite. Inflammatory cytokines are known to interfere with the production of tryptophan and to hasten its degradation. These effects serve to starve T. gondii of what is one of its essential amino acids (Miller, Boulter et al. 2009). However, low tryptophan supplies limit serotonin production and low serotonin levels are clearly linked to risk for suicide, in large part through increases in impulsivity and aggressivity (Mann and Currier 2007). In particular, none has assessed toxoplasmosis titers as a predisposing factor in this age group.
The rate of suicide attempts rises dramatically during adolescence but few studies have addressed risk factors in this important age group (Nock, Green et al. 2013). It may be difficult to show a relationship between toxoplasmosis and history of suicide attempt in this age group because the infection rate increases steadily with age and is relatively low among teenagers. A survey in the U.S., for example, showed a fourfold difference in risk between white, non-Hispanic individuals in their teens and those 60 and older (Jones, Kruszon-Moran et al. 2001). It may also be possible that a relationship between toxoplasmosis and suicidal behavior will be relatively difficult to demonstrate in the U.S. because the prevalence of toxoplasmosis infection is lower than in many other countries (Tenter, Heckeroth et al. 2000). Only one of the case-control studies of toxoplasmosis titers and suicide attempt history was based in the U.S., and this sample had an average age of 43 years. Importantly, it found significant group differences in mean toxoplasmosis titers but not in the proportions that were seropositive (Arling, Yolken et al. 2009). The seropositivity rate in the controls described in that study was 11.1% while the weighted mean in controls across the other four studies in Table 1 was 25.8%.
Given the lack of studies in this age group, we undertook the following analysis to explore whether a relationship between suicidal behavior and toxoplasmosis exposure can be demonstrated in a relatively young sample in the U.S.
Methods
Participants
One hundred ten participants, 15 to 20 years old, who were within one month of starting a selective serotonin reuptake inhibitor (SSRI), were enrolled from outpatient and inpatient clinical settings as well as by email solicitation and word of mouth, into an ongoing two-year longitudinal observational study designed to examine the skeletal effects of SSRIs. Treatment with other psychotropic medications over the two years prior to study entry resulted in exclusion, with the exception of benzodiazepines, antihistaminic agents, trazodone, α2-agonists, mirtazapine, or a stable dose of psychostimulants. The cumulative exposure to SSRIs that antedated the two years prior to study enrollment could not exceed six months. Other grounds for exclusion were the presence of eating disorders, substance dependence, pregnancy, significant medical or surgical history, the chronic use of medications potentially affecting bone metabolism (e.g., extended corticosteroid use), or plans to move out of state in the following year. The University of Iowa Institutional Review Board approved the study and adult participants provided written informed consent. The parent/guardian of minor participants provided written informed consent while the minors gave written assent to the study. The investigation was carried out in accordance with the latest version of the Declaration of Helsinki.
Procedures
Diagnoses, based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR), incorporated information from the review of medical records, from self- and researcher-completed symptom rating scales, the NIMH Diagnostic Interview Schedule for Children (DISC-IV), and an unstructured interview by a child psychiatrist (CAC). A 5.1 scale was used to assign parental socioeconomic status categories; ”5” indicated that the parent with the higher rating was unskilled or semi-skilled or had only an elementary education. All participants with at least one lifetime suicide attempt prior to study intake comprised the suicide attempt group. A suicide attempt was defined as any self-harm that was intended to cause death regardless of premeditation or potential lethality.
Serum samples were sent to the laboratory of Dr. Robert Yolken for toxoplasmosis titer determination.
Data Analysis
Two of the 110 with prodromal psychosis (possible schizophrenia) were excluded from this analysis. The distribution of toxoplasmosis IgG titers was highly right-skewed so natural logarithms were used for statistical analysis. The University of Iowa Hospitals and Clinics laboratory considers an IgG threshold of 10IU/ml to indicate toxoplasmosis seropositivity. Analyses used SPSS (version 21).
Group comparisons were made with Mann-Whitney U-tests and chi-square tests. Logistic regression analyses controlled for age and sex in group comparisons of IgG titers. A two-tailed alpha of 0.05 was used throughout.
Results
Seventeen (15.4%) of the patients who had recently begun treatment with an SSRI had a history of at least one lifetime suicide attempt (Table 2). Two (11.8%) of the seventeen with a suicide attempt history and two (2.2%) without a suicide attempt history were seropositive for toxoplasmosis (p=0.112), Fisher’s exact test. A logistic regression analysis that included age and sex in the model showed a marginally significant group difference likelihood ratio of 2.6 (p=0.090). Five had more than one suicide attempt but only one of these had an IgG > 10 IU/ml.
Table 2.
Toxoplasmosis Titers and Suicide Attempt History Among Young Patients Treated for Mood Disorders
| Suicide Attempt History | |||
|---|---|---|---|
| Absent | Present | Significance | |
| N | 91 | 17 | |
| Age, mean ± SD | 19.0±1.6 | 17.5±1.7 | t==3.6, df=106, p=0.001 |
| # (%) Female | 13 (76.5%) | 65 (70.7%) | |
| Annual parental income, | $92,916 | 67,271 | |
| mean ±SD | (65,238) | (58,605) | |
| Parental SES, mean ±ISO | 2.5 (.73) | 2.8 (.75) | |
| # (%) with consensus diagnosis of: | |||
| MDD1 | 82 (90.1%) | 17 (100%) | |
| bipolar I | 0 (0%) | 0 (0%) | |
| bipolar II | 1 (0.9%) | 0 (0%) | |
| alcohol abuse/dep. | 11(12.1%) | 4 (23.5%) | |
| drugabuse/dep. | 1 (1.1%) | 0 (0%) | |
| GAD2 | 42 (46.2%) | 5 (29.4%) | |
| log toxoplasmosis titer mean (SD) | −1.14 (0.48) | −0.78 (0.67) | t=−2.67, df=106, p=0.009 |
| # (%) 10 IU/ml | 2 (2.1) | 2 (11.8) | |
Major Depressive Disorder
Generalized Anxiety Disorder
The group difference in IgG toxoplasmosis titers was significant (t=−2.67, df=106, p=0.009) and remained so in a logistic regression analysis with age and sex (β=−0.371, CI=−0.656, −0.097, p=0.008). The addition to the model of the proportion of weeks in depressive episodes over the previous 4 months had little effect on this relationship (β=1.2, CI=2.3, 0.2, p=0.019) with age and sex in the model (β=1.2, CI= −2.2, −0.2, p=0.019). The relation was also little changed when parental SES was added to age and sex in the model (β=−2.8, CI= −5.3, −.23, p=0.03). When seropositivity was substituted for titer in model with age and sex it was marginally significant (β=2.20, CI=0.074, 4.48, p=0.058).
An ROC analysis (Figure 1) of IgG titers and the separation of suicide attempters from non-attempter showed a significant area under the curve (0.68, p=0.018) and suggested an optimal value for discrimination of 3.6 IU/ml with a specificity=0.26 and sensitivity=0.65.
Figure 1.
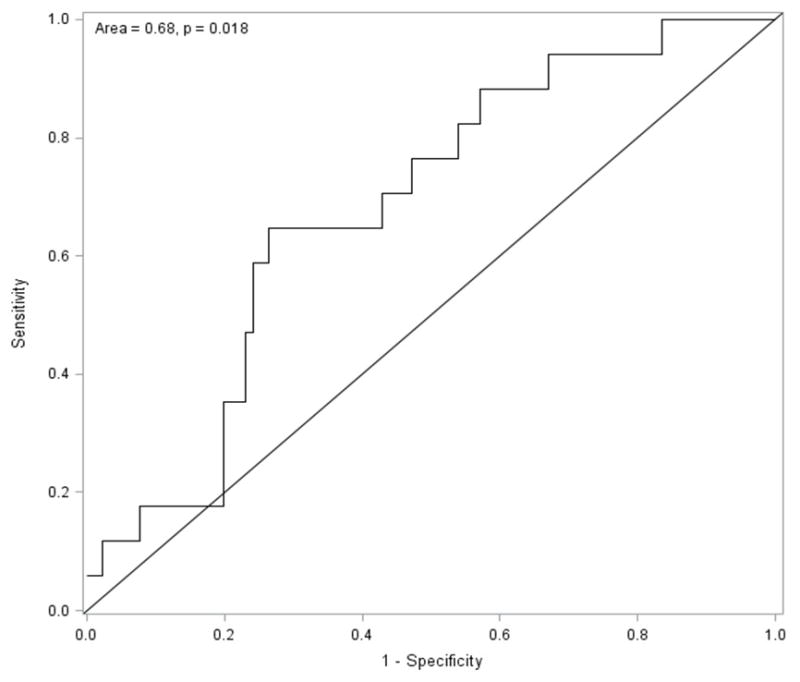
ROC of Toxoplasmosis Titers and a History of Suicide Attempt
Discussion
To our knowledge, this is the first study to examine the association between toxoplasmosis IgG titers and suicide attempts in older adolescents. We found a significantly higher toxoplasmosis IgG titer among individuals who had recently begun a trial of SSRIs and had a history of suicide attempts. This difference emerged despite the relatively low overall seroprevalence of 3.6%. Indeed, an ROC analysis suggested that a substantially lower threshold for seroprevalence might be appropriate for the assessment of risk for suicidal behavior.
A number of investigators have suggested that the inflammatory reaction produced by the toxoplasmosis organism may mediate its effect on serotonin availability, and thus on impulsivity (Postolache and Cook 2013). Titers reflect the level of an individual’s immune response to an infectious organism and thus the level of consequent inflammatory cytokine generation. This, in turn, is likely to correlate with reductions in tryptophan supply, the chief mechanism through which the body defends against toxoplasmosis (Miller, Boulter et al. 2009). Thus the relationship of toxoplasmosis titers to impulsive behavior may be better viewed as a continuum than as a dichotomy because higher titers are likely to produce more inflammation. The influence of toxoplasmosis infection on behavior is likely further complicated by these variability of toxoplasmosis titers within an individual. Titers are relatively higher following initial exposure. They then fall but may increase again if the parasite is reactivated. Such reactivation is known to occur with immunosuppression, but little is known on the variability of toxoplasmosis titers over time otherwise.
Chief among this study’s weaknesses is the small number of suicide attempts described. The resulting lack of power may well account for the failure to find a significant group difference in seroprevalence despite a likelihood ratio of 3.4. The limited statistical power of these analyses certainly recommends caution in the interpretation of the ROC analysis. This is presented primarily to show that the most useful IgG threshold for the presumed infection by toxoplasmosis may differ by the use to which it is being put.
The small sample size also limits the ability to control for possible confounds by showing whether certain demographic variables are associated with both risk for suicide attempts and exposure to toxoplasmosis. Because the sample consisted of individuals within a narrow age range and living in or near Iowa City, principally a university town, we believe the range of such variables was relatively limited. Reverse causality in which behavioral instabilities somehow increase risks for toxoplasmosis exposure is also conceivable and the literature has so far not addressed this.
The retrospective assessment of suicide attempts comprises another weakness. Convincing evidence that high toxoplasmosis titers may be a useful addition to other factors in assessing suicide attempt risk will require studies in which a prospectively observed suicide attempt is the outcome variable.
Strengths include the focus on an age range in which the risk for suicide attempts increases rapidly. The sample was also comprised of young individuals that very recently began SSRI treatment. An association between antidepressant treatment in this age group and suicidality (Carpenter, Fong et al. 2011) resulted in an FDA-mandated black box warning for all antidepressants and, according to some authors, a consequent decrease in antidepressant usage in adolescents and young adults (Clarke, Dickerson et al. 2012, Isacsson and Rich 2014). While the justification for this concern is a matter of controversy, it makes the assessment of suicide risk in this particular population of widespread concern.
In conclusion, these results indicate that the relationship between toxoplasmosis titers and a history of suicide attempt applies to a younger group in a geographical area with low rates of toxoplasmosis exposure. They justify prospective studies that use larger samples to examine the mechanisms underlying the relationship and the possibility of its application as a clinical tool. Future studies should address whether IgG titers correlate with numbers of attempts. Larger samples would also allow exploration of possible differences between acute and chronic toxoplasmosis infection as reflected in IgM vs. IgG titers.
Contributor Information
William Coryell, Department of Psychiatry, University of Iowa, Iowa City, Iowa, USA.
Robert Yolken, Stanley Division of Developmental Neurovirology, Johns Hopkins University, Baltimore, Maryland, USA.
Brandon Butcher, Department of Psychiatry, University of Iowa, Iowa City, Iowa, USA.
Trudy Burns, Department of Epidemiology, University of Iowa, Iowa City, Iowa, USA.
Lilian Dindo, Department of Psychiatry, Baylor College of Medicine, Houston, Texas, USA.
Janet Schlechte, Department of Endocrinology, University of Iowa, Iowa City, Iowa, USA.
Chadi Calarge, Department of Psychiatry and Behaviorial Sciences, Baylor College of Medicine, Houston, Texas, USA.
References
- Arling TA, Yolken RH, Lapidus M, Langenberg P, Dickerson FB, Zimmerman SA, Balis T, Cabassa JA, Scrandis DA, Tonelli LH, Postolache TT. Toxoplasma gondii antibody titers and history of suicide attempts in patients with recurrent mood disorders. J Nerv Ment Dis. 2009;197(12):905–908. doi: 10.1097/NMD.0b013e3181c29a23. [DOI] [PubMed] [Google Scholar]
- Carpenter DJ, Fong R, Kraus JE, Davies JT, Moore C, Thase ME. Meta-analysis of efficacy and treatment-emergent suicidality in adults by psychiatric indication and age subgroup following initiation of paroxetine therapy: a complete set of randomized placebo-controlled trials. J Clin Psychiatry. 2011;72(11):1503–1514. doi: 10.4088/JCP.08m04927blu. [DOI] [PubMed] [Google Scholar]
- Clarke G, Dickerson J, Gullion CM, DeBar LL. Trends in youth antidepressant dispensing and refill limits, 2000 through 2009. J Child Adolesc Psychopharmacol. 2012;22(1):11–20. doi: 10.1089/cap.2011.0048. [DOI] [PubMed] [Google Scholar]
- Cook TB, Brenner LA, Cloninger CR, Langenberg P, Igbide A, Giegling I, Hartmann AM, Konte B, Friedl M, Brundin L, Groer MW, Can A, Rujescu D, Postolache TT. “Latent” infection with Toxoplasma gondii: association with trait aggression and impulsivity in healthy adults. J Psychiatr Res. 2015;60:87–94. doi: 10.1016/j.jpsychires.2014.09.019. [DOI] [PubMed] [Google Scholar]
- Flegr J, Havlicek J, Kodym P, Maly M, Smahel Z. Increased risk of traffic accidents in subjects with latent toxoplasmosis: a retrospective case-control study. BMC Infect Dis. 2002;2:11. doi: 10.1186/1471-2334-2-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghanem M, Gamaluddin H, Mansour M, Samiee AA, Shaker NM, El Rafei H. Role of impulsivity and other personality dimensions in attempted suicide with self-poisoning among children and adolescents. Arch Suicide Res. 2013;17(3):262–274. doi: 10.1080/13811118.2013.805645. [DOI] [PubMed] [Google Scholar]
- Gvion Y, Apter A. Aggression, impulsivity, and suicide behavior: a review of the literature. Arch Suicide Res. 2011;15(2):93–112. doi: 10.1080/13811118.2011.565265. [DOI] [PubMed] [Google Scholar]
- Isacsson G, Rich CL. Antidepressant Drugs and the Risk of Suicide in Children and Adolescents. Paediatr Drugs. 2014 doi: 10.1007/s40272-013-0061-1. [DOI] [PubMed] [Google Scholar]
- Jones JL, Kruszon-Moran D, Wilson M, McQuillan G, Navin T, McAuley JB. Toxoplasma gondii infection in the United States: seroprevalence and risk factors. Am J Epidemiol. 2001;154(4):357–365. doi: 10.1093/aje/154.4.357. [DOI] [PubMed] [Google Scholar]
- Kocazeybek B, Oner YA, Turksoy R, Babur C, Cakan H, Sahip N, Unal A, Ozaslan A, Kilic S, Saribas S, Aslan M, Taylan A, Koc S, Dirican A, Uner HB, Oz V, Ertekin C, Kucukbasmaci O, Torun MM. Higher prevalence of toxoplasmosis in victims of traffic accidents suggest increased risk of traffic accident in Toxoplasma-infected inhabitants of Istanbul and its suburbs. Forensic Sci Int. 2009;187(1–3):103–108. doi: 10.1016/j.forsciint.2009.03.007. [DOI] [PubMed] [Google Scholar]
- Lester D. Brain parasites and suicide. Psychol Rep. 2010;107(2):424. doi: 10.2466/12.13.PR0.107.5.424. [DOI] [PubMed] [Google Scholar]
- Ling VJ, Lester D, Mortensen PB, Langenberg PW, Postolache TT. Toxoplasma gondii seropositivity and suicide rates in women. J Nerv Ment Dis. 2011;199(7):440–444. doi: 10.1097/NMD.0b013e318221416e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mann JJ, Currier D. A review of prospective studies of biologic predictors of suicidal behavior in mood disorders. Arch Suicide Res. 2007;11(1):3–16. doi: 10.1080/13811110600993124. [DOI] [PubMed] [Google Scholar]
- Miller CM, Boulter NR, Ikin RJ, Smith NC. The immunobiology of the innate response to Toxoplasma gondii. Int J Parasitol. 2009;39(1):23–39. doi: 10.1016/j.ijpara.2008.08.002. [DOI] [PubMed] [Google Scholar]
- Nock MK, Green JG, Hwang I, McLaughlin KA, Sampson NA, Zaslavsky AM, Kessler RC. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry. 2013;70(3):300–310. doi: 10.1001/2013.jamapsychiatry.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedersen MG, Mortensen PB, Norgaard-Pedersen B, Postolache TT. Toxoplasma gondii infection and self-directed violence in mothers. Arch Gen Psychiatry. 2012;69(11):1123–1130. doi: 10.1001/archgenpsychiatry.2012.668. [DOI] [PubMed] [Google Scholar]
- Postolache TT, Cook TB. Is latent infection with Toxoplasma gondii a risk factor for suicidal behavior? Expert Rev Anti Infect Ther. 2013;11(4):339–342. doi: 10.1586/eri.13.20. [DOI] [PubMed] [Google Scholar]
- Samojlowicz D, Borowska-Solonynko A, Golab E. Prevalence of Toxoplasma gondii parasite infection among people who died due to sudden death in the capital city of Warsaw and its vicinity. Przegl Epidemiol. 2013;67(1):29–33. 115–118. [PubMed] [Google Scholar]
- Tenter AM, Heckeroth AR, Weiss LM. Toxoplasma gondii: from animals to humans. Int J Parasitol. 2000;30(12–13):1217–1258. doi: 10.1016/s0020-7519(00)00124-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vyas A, Kim SK, Giacomini N, Boothroyd JC, Sapolsky RM. Behavioral changes induced by Toxoplasma infection of rodents are highly specific to aversion of cat odors. Proc Natl Acad Sci U S A. 2007;104(15):6442–6447. doi: 10.1073/pnas.0608310104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Webster JP, Brunton CF, MacDonald DW. Effect of Toxoplasma gondii upon neophobic behaviour in wild brown rats, Rattus norvegicus. Parasitology. 1994;109( Pt 1):37–43. doi: 10.1017/s003118200007774x. [DOI] [PubMed] [Google Scholar]
- Yereli K, I, Balcioglu C, Ozbilgin A. Is Toxoplasma gondii a potential risk for traffic accidents in Turkey? Forensic Sci Int. 2006;163(1–2):34–37. doi: 10.1016/j.forsciint.2005.11.002. [DOI] [PubMed] [Google Scholar]