

Abstract
ECG monitoring is common place in the hospital and even pre-hospital setting. The need for different types of lead systems in different settings has been emphasised. Simple three electrode bipolar recording is ubiquitous for monitoring. This can be used to record modified bipolar chest leads as well. Using five leads gives the option of getting a chest lead in addition to bipolar limb leads, enhancing detection of ischemia during procedures. Lead stability is important when the movement of the subject is maximum as in exercise testing. Mason-Likar modification with limb leads shifted to the torso is popular for exercise testing, though the diagnostic value of the ECG is altered. Lund system with leads on proximal part of limbs have both stability and fair diagnostic value. EASI lead system permits derivation of 12 leads from just five electrodes. Lewis lead and the newly devised modified limb lead system are useful in enhancing detection of atrial activity. Fontaine lead has been designed to improve visualization of Epsilon wave in arrhythmogenic right ventricular dysplasia.
Keywords: ECG monitoring, Mason-Likar modification, EASI leads, Lund leads, Lewis lead, Fontaine lead, Modified limb lead
1. Introduction
ECG monitoring is used in various situations starting from intensive coronary care units, critical care units, post operative wards and during surgical/interventional procedures. ECG monitoring during treadmill exercise test, Holter monitoring and event monitoring are other applications. In each of these situations, there is a need for modifying the leads used for monitoring. In ambulatory monitoring or monitoring during treadmill test, the lead stability and stability of the baseline of the ECG recording during movement of the subject is important. Movement is also an important factor introducing artefacts in the intensive care units, often triggering false alarms. It is less important in the operating environment when the patient is under anaesthesia. But new concerns arise in the operating environment with interference from electrosurgical equipment. Hence different monitoring lead systems are needed for each application. In the earlier era of coronary care units, all standard 12 leads were sometimes used and the patient asked to stay quiet with limb leads on the extremities, to achieve reasonable quality 12 lead monitoring. Several special leads have been developed for specific purposes over the decades. In this brief review, we will discuss the modified monitoring leads and special leads.
2. Simple 3 electrode bipolar monitoring
Simple three electrode monitoring uses two electrodes at a time for active monitoring and third one as ground electrode. But the electrodes can be used in different configurations to get lead I, II or III, one at a time. The signal acquisition is bipolar, between the chosen two electrodes for the given lead. The electrodes are placed in such a location as to obtain the required lead, usually on the torso near the corresponding limb. This is to reduce movement artefacts during continuous monitoring and to avoid tethering of the subject. MCL1 lead configuration can be obtained by keeping the right arm electrode in left infraclavicular region and the left arm electrode in the right fourth intercostal space parasternally (V1 location). Ground electrode can be placed in any convenient location away from the active electrodes [1]. Three electrode system was quite common with telemetry monitors.
2.1. Modified chest leads
The most commonly used modified chest lead is MCL1 with the configuration mentioned above and lead selector at lead I position. MCL6 will have one active electrode located at V6 position instead. These leads simulate V5 and V6, though not perfectly well. CS5 lead popular in operating rooms has the right arm electrode placed below the right clavicle and left arm electrode placed at V5 location while the left leg electrode acts as ground electrode [2]. Lead selector is at lead I. CS5 is useful in detection of anterior wall myocardial ischemia. In CM5, the right arm electrode is at the manubrium sternum while the remaining configuration is same as CS5. CB5 has the right arm electrode at right scapula and CC5 has it in right anterior axillary line, with similar configuration of other electrodes. CB5 is good for detection of myocardial ischemia and supraventricular arrhythmias.
3. Common five electrode monitoring
Most current day intensive care monitors use a five electrode monitoring cable. Four electrodes are placed on the torso corresponding to the limbs, with the electrode corresponding to the right lower limb serving as the ground electrode. Fifth electrode is used on one of the standard chest lead positions, usually in V1 location for better arrhythmia monitoring. It can be placed in any other chest lead location depending on the need. Adding a regular chest lead helps in detection of bundle branch blocks and is useful for the diagnosis of pacemaker rhythms and wide QRS complex tachycardias. All limb leads ECGs can be obtained in this five electrode system, though only one chest lead is possible at a time. Five electrode system can pick up rhythm abnormalities and ST segment deviations fairly well. This system is more often used in two channel monitors in which one limb lead and one chest lead are displayed simultaneously [1].
4. Mason-Likar 10 electrode 12 lead monitoring
Mason-Likar modification of standard 12 leads is quite popular for treadmill testing. In this system, chest electrodes are placed in the standard positions, but limb electrodes are transposed to the torso to reduce movement artefacts [3]. Right and left arm electrodes are placed in the infraclavicular fossae, medial to the deltoid muscle, 2 cm below the lower border of the clavicle. Right and left leg electrodes are kept in the anterior axillary line, halfway between costal margin and iliac crest (Fig. 1). Right lower electrode serves as the ground as in standard 12 lead ECG. There will be a total of ten electrodes from which all 12 leads can be obtained. This lead system is good for real time ST segment monitoring during thrombolytic therapy as well [4]. But the diagnostic value of 12 lead electrocardiogram obtained using this lead system is altered by the change in the location of limb electrodes. Q waves in the inferior leads may be masked and there is mild right ward shift in the QRS axis.
Fig. 1.
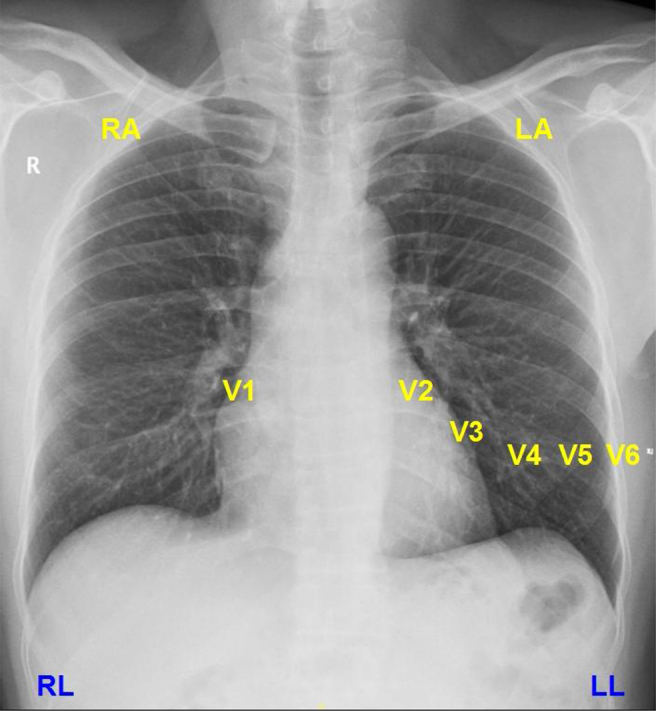
Mason-Likar 12 Lead (See text for details). RA: Right arm, LA: Left arm, RL: Right leg, LL: Left leg. (Left leg and right leg or ground electrode positions are representatory, actual positions are lower than what is shown in the figure).
Mason-Likar system gives the option of multiple chest leads so that both arrhythmia (V1) and ischemia (V3 or V5 depending on territory of interest) can be monitored in post angioplasty cases. Downside is the presence of multiple chest electrodes which interfere with echocardiography, defibrillation and chest X-ray evaluation. Obtaining stable chest electrode position over a long period in females and males with hairy chest is also a concern.
5. Lund lead system
While the limb electrodes are transposed to the torso in Mason-Likar modification, they are placed on the proximal regions of the limbs in the Lund lead system [5]. The advantage is that movement artefacts are reduced as in Mason-Likar system while changes in the 12 lead ECG pattern are lesser and more comparable to standard 12 lead ECG. Hence Lund system can be used both for diagnostic ECG and monitoring [6]. The difference in noise levels on ECG between the Lund system and Mason-Likar system was not significant, though both were better than standard 12 lead, during monitoring [7].
6. Computerized regeneration of 12 leads from reduced lead set
Sometimes it may not be technically feasible to keep all electrodes on the chest due to various reasons. Computerized algorithms have been developed to reconstruct the ECG of missing leads [8]. Reconstruction can be by using either general or patient specific templates. It is technically feasible to derive a 12 lead ECG using all limb electrodes and just 2 precordial electrodes, with reasonable diagnostic accuracy [9].
7. EASI lead system
EASI lead system uses five electrodes and derives 12 leads by a computer algorithm [10]. In EASI lead system, A, E and I are same as that of Frank vectorcardiographic system [11]. E is located at the lower end of body of sternum. A and I are located in left and right midaxillary lines in the same horizontal level as E. Electrode S is placed on the manubrium sternum (Fig. 2). Ground electrode for the EASI system is on the torso in same location as in Mason-Likar system. Algebraic transfer coefficients are used to generate a derived 12 lead ECG using 5 electrode EASI system [12]. When the EASI system is used for continuous monitoring, excessive artefacts while turning from supine position to right has been documented [13]. This is due to artefacts picked up by the electrode in the right mid axillary line (I). But myoelectric noise in the limb leads during physical activity was lesser with EASI system than Mason-Likar system. It may be noted that derivation of 12 leads from EASI electrodes is an approximation and a 12/12 match with standard 12 lead ECG should not be expected.
Fig. 2.
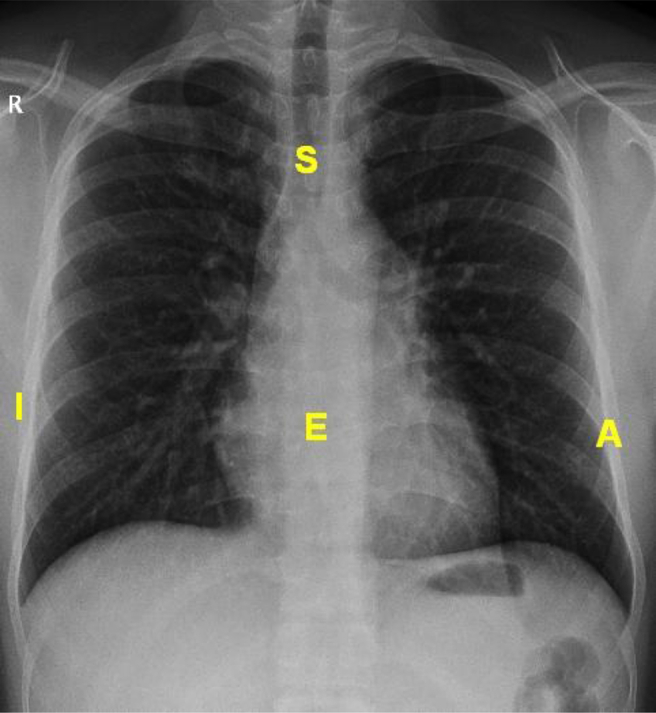
EASI lead system (See text for details).
Many of the ischemic episodes which are missed by two lead monitoring (lead II and V1) can be picked up by derived 12 lead monitoring. In one study 67% of the ischemic events detected by EASI derived 12 lead monitoring were not captured by monitoring of V1 and lead II [14].
8. Lewis lead and modified Lewis lead
Lewis lead (Fig. 3) is used to enhance the recording of atrial activity in the ECG [15]. Originally it was just a modified lead I with right arm electrode placed in second right intercostal space close to sternum and left arm lead placed in fourth right intercostal space close to sterunum. Lewis lead is useful in recognizing P waves during wide QRS tachycardia and thereby aiding an accurate diagnosis [16]. A modification of Lewis lead in which all 12 leads are recorded, with the right arm and left arm electrodes transposed to the original Lewis lead configuration [17] has been used to detect the type of ventriculoatrial conduction during ventricular pacing.
Fig. 3.
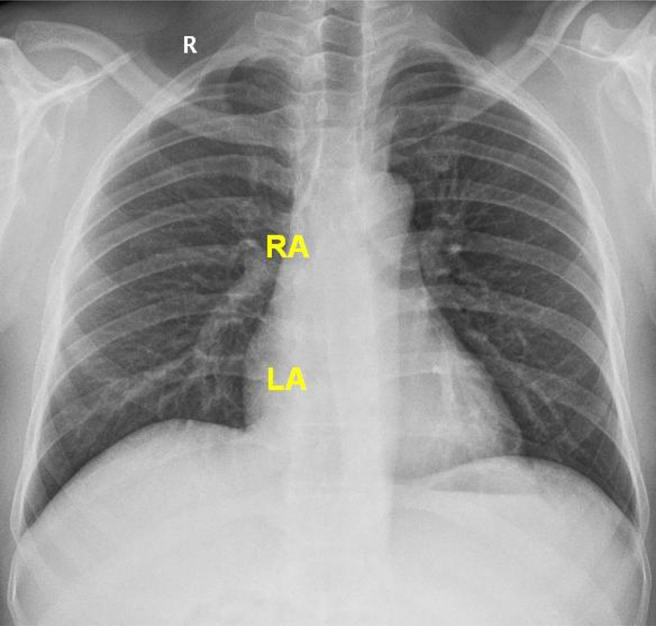
Lewis lead (See text for details).
9. Fontaine leads (Fontaine bipolar precordial lead ECG)
It was in 1977 that Guy Fontaine described the Epsilon waves in arrhythmogenic right ventricular dysplasia (ARVD) [18]. Fontaine leads are useful in increasing the sensitivity of detection of Epsilon waves in ARVD [19]. The Fontaine precordial electrodes are placed at the manubrium sternum, xiphoid and V4 positions (Fig. 4). The electrodes are connected to the right arm, left arm and left foot electrode connections of the electrocardiograph respectively [20]. The three Fontaine bipolar precordial leads are FI (manubrium sterum negative, xiphoid positive), FII (manubrium sternum negative, V4 location positive) and FIII (xiphoid negative, V4 positive).
Fig. 4.
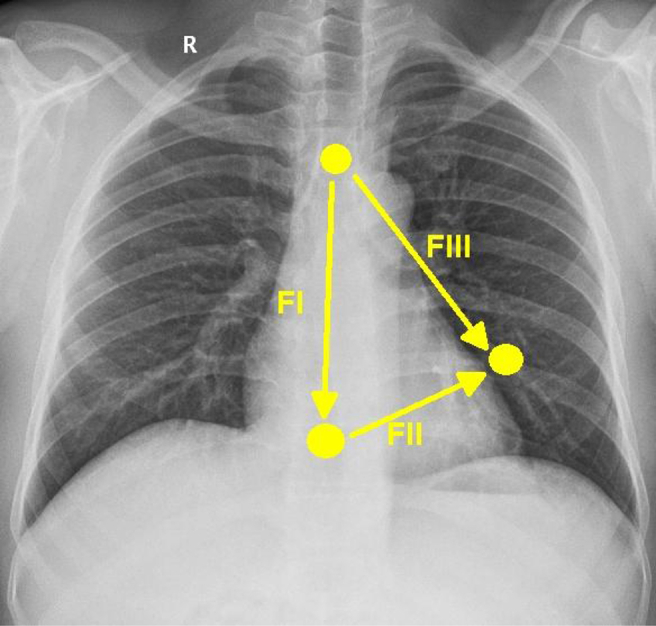
Fontaine leads (See text for details).
10. Modified limb lead system for atrial repolarization wave
Usually atrial repolarization wave (Ta wave) is not evident on the surface electrocardiogram, though its presence may be indirectly assumed by the presence of upsloping ST segment depression. A recent study reported a modified limb lead (MLL) system for enhancing detection of atrial activity on surface ECG [21]. The right arm electrode is placed in the third right intercostal space just to the left of mid clavicular line. Left arm electrode is placed in the fifth right intercostal space just to the right of the midclavicular line. The left leg electrode is placed in fifth right intercostal space in the mid clavicular line. Chest electrodes and ground electrode are in the standard positions. This produces an ECG with low QRS amplitudes and good P waves. Since the left arm and left leg electrodes are close to each other, the tracing recorded in lead III is of very low amplitude. The MLL system is useful in detecting atrial repolarization on surface ECG, more so in cases of complete heart block where the activity is not masked by the ensuing QRS complex in case of independent P waves [22]. For the same reason, it was shown that atrial repolarization (Ta wave) has a longer duration than what is noted in sinus rhythm. Need for further studies on atrial repolarization in pericarditis and atrial infarction has been suggested.
11. Neonatal and pediatric ECG monitoring
Pediatric and neonatal ECG monitoring is often challenging. Small size of the subject makes application of multiple electrodes technically difficulty. Special pediatric electrodes in a cloth base can be used to reduce the trauma while pulling out the electrodes. In spite of the limitations, studies have shown that during neonatal reuscitation, ECG gives an indication of the heart rate faster than pulse oximetry [23].
12. Conclusion
Different lead systems have been proposed for different purposes, in addition to the standard 12 lead ECG. Though the most important aspect of ECG monitoring is detection of rhythm abnormalities, detection of ST shift is equally important. Detection of ST shift is important during a stress test, during and after a percutaneous coronary intervention. Special leads have been designed mostly for enhancement of atrial activity which can be of use in arrhythmia analysis as well as for assessment of atrial repolarization which is often ignored in surface ECG.
Footnotes
Peer review under responsibility of Indian Heart Rhythm Society.
References
- 1.Drew B.J., Califf R.M., Funk M., Kaufman E.S., Krucoff M.W., Laks M.M. Councils on cardiovascular nursing, clinical cardiology, and cardiovascular disease in the young. Practice standards for electrocardiographic monitoring in hospital settings: an american heart association scientific statement from the councils on cardiovascular nursing, clinical cardiology, and cardiovascular disease in the young: endorsed by the international society of computerized electrocardiology and the American association of critical-care nurses. Circulation. 2004 Oct 26;110(17):2721–2746. doi: 10.1161/01.CIR.0000145144.56673.59. [DOI] [PubMed] [Google Scholar]
- 2.Dash P.K. Electrocardiogram monitoring. Indian J Anaesth. 2002;46(4):251–260. [Google Scholar]
- 3.Mason R.E., Likar I. A new system of multiple-lead exercise electrocardiography. Am Heart J. 1966;71:196–205. doi: 10.1016/0002-8703(66)90182-7. [DOI] [PubMed] [Google Scholar]
- 4.Johanson P., Rossberg J., Dellborg M. Continuous ST monitoring: a bedside instrument? A report from the Assessment of the Safety of a New Thrombolytic (ASSENT 2) ST monitoring substudy. Am Heart J. 2001;142:58–62. doi: 10.1067/mhj.2001.116074. [DOI] [PubMed] [Google Scholar]
- 5.Pahlm O., Wagner G.S. Proximal placement of limb electrodes: a potential solution for acquiring standard electrocardiogram waveforms from monitoring electrode positions. J Electrocardiol. 2008 Nov-Dec;41(6):454–457. doi: 10.1016/j.jelectrocard.2008.06.019. [DOI] [PubMed] [Google Scholar]
- 6.Tragardh-Johansson E., Welinder A., Pahlm O. Similarity of ST and T waveforms of 12-lead electrocardiogram acquired from different monitoring electrode positions. J Electrocardiol. 2011 Mar-Apr;44(2):109–114. doi: 10.1016/j.jelectrocard.2010.11.012. [DOI] [PubMed] [Google Scholar]
- 7.Welinder A., Wagner G.S., Maynard C., Pahlm O. Differences in QRS axis measurements, classification of inferior myocardial infarction, and noise tolerance for 12-lead electrocardiograms acquired from monitoring electrode positions compared to standard locations. Am J Cardiol. 2010 Aug 15;106(4):581–586. doi: 10.1016/j.amjcard.2010.03.073. [DOI] [PubMed] [Google Scholar]
- 8.Nelwan S.P., Kors J.A., Meij S.H., van Bemmel J.H., Simoons M.L. Reconstruction of the 12-lead electrocardiogram from reduced lead sets. J Electrocardiol. 2004 Jan;37(1):11–18. doi: 10.1016/j.jelectrocard.2003.10.004. [DOI] [PubMed] [Google Scholar]
- 9.Nelwan S.P., Crater S.W., Green C.L., Johanson P., van Dam T.B., Meij S.H. Assessment of derived 12-lead electrocardiograms using general and patient-specific reconstruction strategies at rest and during transient myocardial ischemia. Am J Cardiol. 2004 Dec 15;94(12):1529–1533. doi: 10.1016/j.amjcard.2004.08.031. [DOI] [PubMed] [Google Scholar]
- 10.Dower G.E., Yakush A., Nazzal S.B., Jutzy R.E., Ruiz C.E. Deriving the 12-lead electrocardiogram from four (EASI) electrodes. J Electrocardiol. 1988;21(suppl):S182–S187. doi: 10.1016/0022-0736(88)90090-8. [DOI] [PubMed] [Google Scholar]
- 11.Frank E. An accurate, clinically practical system for spatial vectorcardiography. Circulation. 1956;13:737–749. doi: 10.1161/01.cir.13.5.737. [DOI] [PubMed] [Google Scholar]
- 12.Feild D.Q., Feldman C.L., Horacek B.M. Improved EASI coefficients: their derivation, values and performance. J Electrocardiol. 2002;35(suppl.):23–33. doi: 10.1054/jelc.2002.37151. [DOI] [PubMed] [Google Scholar]
- 13.Welinder A., Sornmo L., Feild D.Q., Feldman C.L., Pettersson J., Wagner G.S. Comparison of signal quality between EASI and Mason-Likar 12-lead electrocardiograms during physical activity. Am J Crit Care. 2004 May;13(3):228–234. [PubMed] [Google Scholar]
- 14.Drew B.J., Pelter M.M., Adams M.G., Wung S.F., Chou T.M., Wolfe C.L. 12-lead ST-segment monitoring vs single-lead maximum ST-segment monitoring for detecting ongoing ischemia in patients with unstable coronary syndromes. Am J Crit Care. 1998;7:355–363. [PubMed] [Google Scholar]
- 15.Lewis T. Clinical electrocardiography. fifth ed. Shaw and Sons; London, UK: 1931. Auricular fibrillation. [Google Scholar]
- 16.Bakker A.L., Nijkerk G., Groenemeijer B.E., Waalewijn R.A., Koomen E.M., Braam R.L. The Lewis lead:making recognition of P waves easy during wide QRS complextachycardia. Circulation. 2009;119:e592–e593. doi: 10.1161/CIRCULATIONAHA.109.852053. [DOI] [PubMed] [Google Scholar]
- 17.Huemer M., Meloh H., Attanasio P., Wutzler A., Parwani A.S., Matsuda H. The Lewis lead for detection of ventriculoatrial conduction type. Clin Cardiol. 2016 Feb;39(2):126–131. doi: 10.1002/clc.22505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fontaine G., Guiraudon G., Frank R., Vede K., Grosgogeat Y., Cabrol C. Stimulation studies and epicardial mapping in ventricular tachycardia: study of mechanisms and selection for surgery. In: Kulbertus H.E., editor. Re-entrant arrhythmias: mechanisms and treatment. University Park Press; Baltimore: 1977. pp. 334–350. [Google Scholar]
- 19.Gottschalk B., Gysel M., Barbosa-Barros R., De Sousa Rocha R.P., Pérez-Riera A.R., Zhang L. The use of fontaine leads in the diagnosis of arrhythmogenic right ventricular dysplasia. Ann Noninvasive Electrocardiol. 2014 May;19(3):279–284. doi: 10.1111/anec.12153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wang J., Yang B., Chen H., Ju W., Chen K., Zhang F. Epsilon waves detected by various electrocardiographic recording methods: in patients with arrhythmogenic right ventricular cardiomyopathy. Tex Heart Inst J. 2010;37(4):405–411. [PMC free article] [PubMed] [Google Scholar]
- 21.Sivaraman J., Uma G., Venkatesan S., Umapathy M., Dhandapani V.E. Normal limits of ECG measurements related to atrial activity using a modified limb lead system. Anatol J Cardiol. 2015 Jan;15(1):2–6. doi: 10.5152/akd.2014.5155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jayaraman S., Gandhi U., Sangareddi V., Mangalanathan U., Shanmugam R.M. Unmasking of atrial repolarization waves using a simple modified limb lead system. Anatol J Cardiol. 2015 Aug;15(8):605–610. doi: 10.5152/akd.2014.5695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Katheria A., Rich W., Finer N. Electrocardiogram provides a continuous heart rate faster than oximetry during neonatal resuscitation. Pediatrics. 2012 Nov;130(5):e1177–e1181. doi: 10.1542/peds.2012-0784. [DOI] [PubMed] [Google Scholar]