

Abstract
Background:
Diabetes is a leading cause of cardiovascular disease (CVD). Moreover, CVD accounts for primary cause of death among diabetic patients. Physicians, especially in the primary care setting, have effective role in the management of cardiovascular risk factors. Therefore, we aimed to compare the prevalence of modifiable cardiovascular risk factors in Type 2 diabetic patients attending to an urban health center as a primary care center with Institute of Endocrinology and Metabolism Diabetes Clinic (IEMDC) as a tertiary center.
Methods:
This cross-sectional study was performed on 200 adult diabetic patients attending urban health center (Abouzar Health Center) and 201 diabetic patients in a tertiary center. The patients’ cardiovascular risk factors including lipid profile, systolic and diastolic blood pressure (BP), and smoking history were recorded. The number of patients who did not achieve the target according to the American Diabetes Association guidelines was determined and compared.
Results:
The patients in urban health center were older than those who attending IEMDC (P = 0.004). The duration of diabetes was longer among urban center patients (P < 0.001). Comparison of cardiovascular risk factors between two groups of patients showed a significant number of patients with poor-controlled low-density lipoprotein (75% vs. 44.7%) and triglyceride (74% vs. 51.7%) in patients attending primary center (P < 0.001). However, the prevalence of high diastolic BP (60.6% vs. 44.5%) was significantly higher in patients attending IEMDC (P = 0.001). There was no significant difference between the two centers’ findings in glycosylated hemoglobin level, high-density lipoprotein level, and systolic BP.
Conclusions:
Both centers have failure in target achievement in some risk factors; however, the inability of the primary care center in controlling hyperlipidemia in comparison with the tertiary center is a serious warning to provide training about managing dyslipidemia in these centers.
Keywords: Cardiovascular risk factors, primary care setting, tertiary care setting, Type 2 diabetes
INTRODUCTION
Type 2 diabetes is increasing dramatically around the world, including in Iran. The major burden of disease in our country is noncommunicable diseases.[1,2] Cardiovascular disease (CVD) is a common medical complication of diabetes.[3] The diabetic patients are at risk of developing macrovascular diseases, particularly CVD.[4] CVD is responsible for 75%–80% of mortality in diabetic patients.[5,6] The well-known risk factors for developing CVD are dyslipidemia, high blood pressure (BP), smoking, obesity, diabetes, impaired glucose tolerance, and positive family history of CVD.[7] Although diabetes alone is a major risk factor for CVD, people with diabetes, particularly Type 2 diabetes, often have hypertension and dyslipidemia, which intensify the risk of developing CVD.[8] It has been shown that improvement in controlling major risk factors coexisting with diabetes has significant benefits for reducing cardiovascular events.[9] The optimal control of hypertension in people with diabetes can reduce macro- and micro-vascular complications.[10] There is evidence that appropriate management of hyperlipidemia in a diabetic patient is even more effective than in normal populat[11] Large-scale studies show that the use of aspirin, antihypertensive agents, and statins has a great impact on preventing cardiovascular events up to 75%.[12,13] The aim of diabetes care is achieving a good quality of life and health status such as nondiabetic people.[14,15] Given that more than 70% of diabetic patients receive routine care at a primary health center, these clinics have a key role in taking care of patients with diabetes.[16]
This study aimed to compare cardiovascular risk factors and glycemic control in a sample of diabetic patients from the primary care center (Abouzar Clinic [AC], Tehran, Iran) who were treated by general practitioners (GPs) with those of patients from the tertiary center (Institute of Endocrinology and Metabolism Diabetes Clinic [IEMDC], Tehran, Iran) who were treated by endocrinologists.
METHODS
This descriptive cross-sectional study was performed in AC, Tehran, Iran, as the urban primary health care center [district health center, Figure 1] and in the IEMDC, Tehran, Iran [teaching hospital, Figure 1], a teaching center, as the tertiary center (health services organization in Iran is shown in Figure 1). These two centers are located in areas with the same socioeconomic status. A total of 401 patients were included by convenience sampling. According to the inclusion criteria, 201 cases were from AC and 200 cases from IEMDC chosen consecutively. Inclusion criteria were predefined as follows: Adult cases (age more than 18 years) with Type 2 diabetes. The definition of diabetes was based on the American Diabetes Association (ADA) criteria 2013.[17] The participant characteristics including age, sex, economic situation, education, and duration of diabetes were collected. The patients’ cardiovascular risk factors including lipid profile, systolic and diastolic BP, body mass index (BMI), smoking history, and glycosylated hemoglobin (HbA1c) were also recorded. Reports of diabetes complications including microalbuminuria, macroalbuminuria, retinopathy, cerebrovascular diseases, and peripheral neuropathy were retrieved from medical records. For more accuracy, all variables were obtained from the mean value of the last three measurements. The target cutoff values for control of all risk factors were defined according to the ADA 2013.[17] Based on these definitions, BP ≤140/80, low-density lipoprotein (LDL) ≤100, triglyceride (TG) ≤150, HbA1c ≤7.0, high-density lipoprotein (HDL) ≥40 in male, and HDL ≥50 in female cases were considered as desirable targets.
Figure 1.
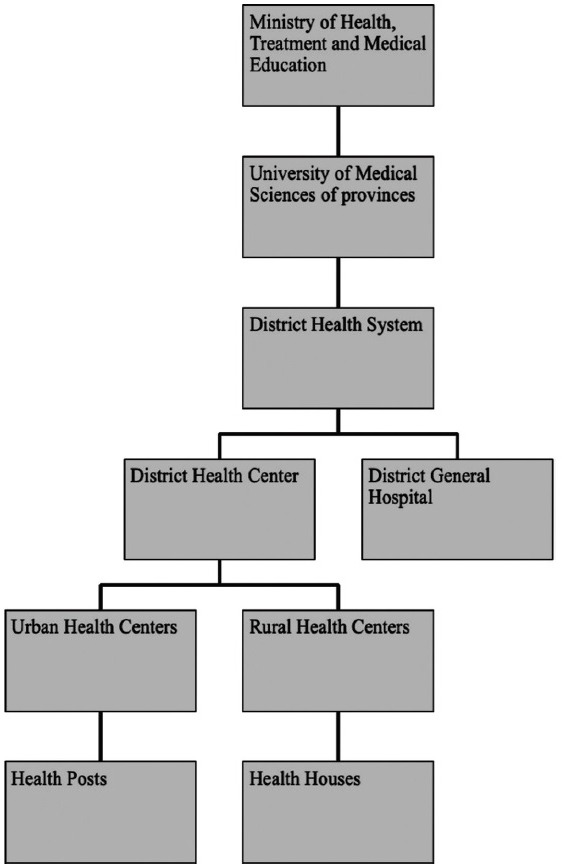
Health system network in Iran
This study was approved by the Ethics Committee of Institute of Endocrinology and Metabolism, Iran University of Medical Sciences, and in accordance with the Helsinki Declaration of 1975, as revised in 2008.
Statistical analysis
Statistical analysis was performed using SPSS for Windows (Version 18.0. Chicago: SPSS Inc.). Data of continues variables are shown in mean ± standard deviations, and categorical variables are expressed as frequency (percent).
Normality of data was checked using Kolmogorov–Smirnov test, and nonnormal variables were compared using Mann–Whitney U-test. For analysis of normal variables, equality of variances was assessed using Levene's test, and Student's t-test and Chi-square test were used to compare continuous and categorical variable, respectively. P < 0.05 was considered statistically significant in this work.
RESULTS
A total of 401 adult patients with Type 2 diabetes were included as follows: 200 (49.9%) patients received care at the AC as a primary care center and 201 (50.1%) at IEMDC as a tertiary center. Table 1 shows clinical characteristics that included demographic and laboratory findings in two groups of patients. Only 22.7% of patients (23% in AC and 22.4% in IEMDC) had normal BMI. There was a significant difference between cases attending tertiary center and primary center with respect to mean value of the duration of diabetes, diastolic BP, TG, and LDL. Furthermore, statin therapy is significantly more frequent in the tertiary center.
Table 1.
Demographic characteristics and cardiovascular risk factors in both studied groups
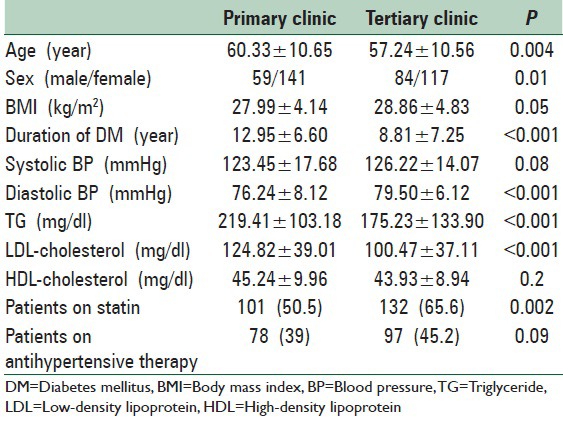
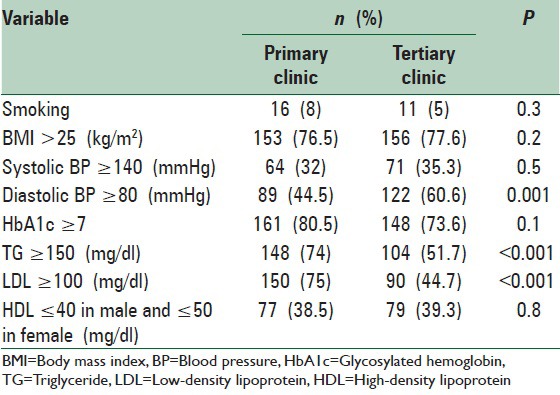
Table 2 compares the percentage of patients who reached to optimal control of cardiovascular risk factors according to the ADA goals at both centers.
Table 2.
Comparison of risk factors controlling between two studied groups
Diabetes management was not different between two groups. Whereas insulin use was more common in the tertiary center, this difference was not statistically significant [Figure 2].
Figure 2.
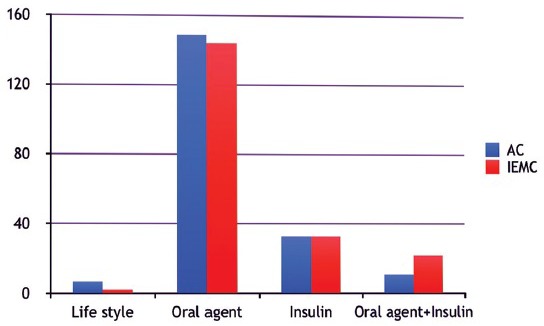
The methods of treatment for hyperglycemia in both groups
Other health-care measurements included dilated eye examination, albuminuria, and assess the presence of coronary artery disease. Twenty-three percent of patients (24.5% and 21.8% in AC and IEMDC, respectively, P = 0.2) did not have an eye examination. Diabetic retinopathy was found in 19.5% of patients (16% in AC and 22.8% in IEMDC, respectively, P = 0.1). The prevalence of proliferative diabetic retinopathy was 7.5% in the study population (6% in AC and 9% in IEMDC), and nonproliferative diabetic retinopathy was detected in 12% of them (10% and 14% in AC and IEMDC, respectively).
Nephropathy was not assessed in 15.4% of all patients (20% at AC vs. 11% at IEMDC). The prevalence of albuminuria was 37% in AC and 26.3% in IEMDC (P = 0.002). In AC, 32.5% of patients had microalbuminuria and 4.5% had macroalbuminuria in contrast to IEMDC, which 22.8% of participants had microalbuminuria and 3.5% of them had macroalbuminuria.
History of coronary artery disease was not available in 13.2% of patients. Ischemic heart disease was reported in 14.5% of cases (7% vs. 21.8% in AC vs. IEMDC, respectively, P < 0.001).
DISCUSSION
In this study, it was noted that patients who were managed in AC had longer durations of diabetes and were older than those cases in the tertiary centers. Controlling HbA1c in both centers had been the weakest among cardiovascular risk factors. In agreement with our results, another study from Iran found that 75% of their cases had HbA1c higher than the target.[18] The second most common risk factor was high LDL, which was significantly higher than the target in patients at the AC. This finding was also reported by other studies;[19] however, the result of this study was better than the reports of NHANES III, that 15.4% had LDL values less than 100 mg/dl.[20] The patients of the AC used less statins than the patients of the IEMDC. This finding suggests that most of the GPs are unfamiliar with statin therapy. Both centers’ plans are efficient in managing hypertension; however, the primary center is more successful than tertiary center in achieving diastolic BP goal. The reason behind this finding can be due to the fact that patient referred to the tertiary centers has more advanced disease. In addition, the longer interval between visits in the tertiary center may be the other explanation of this finding. This is in agreement with other studies,[21,22] while they have reported more success in controlling hypertension in their cases. It is noteworthy that the optimal cutoff point for control of hypertension in the current study was lower than the same study (140/80 vs. 140/90).[23] The prevalence of overweight and obesity was not significantly different between the two centers, and only about one-quarter of patients had normal weight. This finding was consistent with other studies.[24] The prevalence of low HDL-cholesterol levels was similar among participant in both primary and tertiary centers. Indeed, this condition was less common in the current study as compared to most studies.[19,20] However, there are other important determinants of HDL-cholesterol level, such as sex, genetic background, smoking, nutritional status, medication, and physical activity.[25] The other two reasons for our finding could be that: (a) most participants in our study were female, and (b) the number of cases who smoked was very low. Less than 10% of patients in this study were smokers, whereas smoking was a highly frequent factor in other studies.[21,26] Overall, although target achievement was low at both centers, the frequency of patients admitted to the primary health center who had achieved guideline goals did not differ significantly with those of the tertiary center, with the exception of the lipid control. This result suggests that the educational programs on controlling cardiovascular risk factors in diabetic patients for GPs in the primary health centers could improve the implementation of guidelines and outcomes. One limitation of the current study is that information about the levels of education and income as probable important factors was not available.
CONCLUSIONS
Since most patients with diabetes take the services in the primary health-care center, it is important to improve diabetes care in these sites. It is recommended that continuous systematic training programs on the international guidelines and targets of risk factor control be offered to GPs because they are the first to encounter the patient and can play an important role in patient health management. In addition, although both centers have a failure in target achievement in some risk factors, the inability of primary care center in controlling hyperlipidemia in comparison with the tertiary center is a serious warning to improve GPs knowledge about lipid guideline.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Haghdoost AA, Rezazadeh-Kermani M, Sadghirad B, Baradaran HR. Prevalence of type 2 diabetes in the Islamic Republic of Iran: Systematic review and meta-analysis. East Mediterr Health J. 2009;15:591–9. [PubMed] [Google Scholar]
- 2.Herman WH, Zimmet P. Type 2 diabetes: An epidemic requiring global attention and urgent action. Diabetes Care. 2012;35:943–4. doi: 10.2337/dc12-0298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tranche S, Galgo A, Mundet X, Sánchez-Zamorano MA. Karen AP Study Investigators. Cardiovascular risk factors in type 2 diabetic patients: Multifactorial intervention in primary care. Kidney Int Suppl. 2005;93:S55–62. doi: 10.1111/j.1523-1755.2005.09313.x. [DOI] [PubMed] [Google Scholar]
- 4.Henry RR. Przeventing cardiovascular complications of type 2 diabetes: Focus on lipid management. Clin Diabetes. 2001;19:113–20. [Google Scholar]
- 5.Grundy SM, Benjamin IJ, Burke GL, Chait A, Eckel RH, Howard BV, et al. Diabetes and cardiovascular disease: A statement for healthcare professionals from the American Heart Association. Circulation. 1999;100:1134–46. doi: 10.1161/01.cir.100.10.1134. [DOI] [PubMed] [Google Scholar]
- 6.Laakso M. Epidemiology of diabetic dyslipidemia. Diabetes Rev. 1995;3:408–22. [Google Scholar]
- 7.Aggarwal A, Aggarwal S, Sarkar PG, Sharma V. Predisposing factors to premature coronary artery disease in young (Age [Less-Than or Equal To] 45 years) smokers: A single center retrospective case control study from India. J Cardiovasc Thorac Res. 2014;6:15–9. doi: 10.5681/jcvtr.2014.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.American Diabetes Association. (8) Cardiovascular disease and risk management. Diabetes Care. 2015;38(Suppl):S49–57. doi: 10.2337/dc15-S011. [DOI] [PubMed] [Google Scholar]
- 9.Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med. 2008;358:580–91. doi: 10.1056/NEJMoa0706245. [DOI] [PubMed] [Google Scholar]
- 10.Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352:837–53. [PubMed] [Google Scholar]
- 11.Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: Results of AFCAPS/TexCAPS.Air force/texas coronary atherosclerosis prevention study. JAMA. 1998;279:1615–22. doi: 10.1001/jama.279.20.1615. [DOI] [PubMed] [Google Scholar]
- 12.Stratton IM, Cull CA, Adler AI, Matthews DR, Neil HA, Holman RR. Additive effects of glycaemia and blood pressure exposure on risk of complications in type 2 diabetes: A prospective observational study (UKPDS 75) Diabetologia. 2006;49:1761–9. doi: 10.1007/s00125-006-0297-1. [DOI] [PubMed] [Google Scholar]
- 13.Yusuf S. Two decades of progress in preventing vascular disease. Lancet. 2002;360:2–3. doi: 10.1016/S0140-6736(02)09358-3. [DOI] [PubMed] [Google Scholar]
- 14.Diabetes UK. Recommendations for the Provision of Services in Primary Care for People with Diabetes. 2005. [Last accessed on 2015 Apr 22]. Available from: https://www.diabetes.org.uk/Documents/Professionals/primary_recs.pdf .
- 15.Vasan RS, Sullivan LM, Wilson PW, Sempos CT, Sundström J, Kannel WB, et al. Relative importance of borderline and elevated levels of coronary heart disease risk factors. Ann Intern Med. 2005;142:393–402. doi: 10.7326/0003-4819-142-6-200503150-00005. [DOI] [PubMed] [Google Scholar]
- 16.Harris MI. Medical care for patients with diabetes. Epidemiologic aspects. Ann Intern Med. 1996;124(1 Pt 2):117–22. doi: 10.7326/0003-4819-124-1_part_2-199601011-00007. [DOI] [PubMed] [Google Scholar]
- 17.American Diabetes Association. Standards of medical care in diabetes-2013. Diabetes Care. 2013;36(Suppl 1):S11–66. doi: 10.2337/dc13-S011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bonakdaran S, Ebrahimzadeh S, Noghabi SH. Cardiovascular disease and risk factors in patients with type 2 diabetes mellitus in Mashhad, Islamic Republic of Iran. East Mediterr Health J. 2011;17:640–6. [PubMed] [Google Scholar]
- 19.Berthold H, Gouni-Berthold I, Bestehorn K, Bohm M, Krone W. Cardiovascular risk factors in patients with type 2 diabetes in Germany. Dtsch Arztebl Koln. 2007;104:731. [Google Scholar]
- 20.Harris MI. Health care and health status and outcomes for patients with type 2 diabetes. Diabetes Care. 2000;23:754–8. doi: 10.2337/diacare.23.6.754. [DOI] [PubMed] [Google Scholar]
- 21.Akbar DH, Ahmed MM, Algamdi AA. Cardiovascular risk factors in Saudi Arabian and non-Saudi Arabian diabetic patients in Saudi Arabia. East Mediterr Health J. 2003;9:884–92. [PubMed] [Google Scholar]
- 22.Carolino ID, Molena-Fernandes CA, Tasca RS, Marcon SS, Cuman RK. Risk factors in patients with type 2 diabetes mellitus. Rev Lat Am Enfermagem. 2008;16:238–44. doi: 10.1590/s0104-11692008000200011. [DOI] [PubMed] [Google Scholar]
- 23.Patnaik L, Pattnaik S, Ghosh T, Sahoo A K, Sahu T. Coronary heart disease risk factors among diabetic patients attending a tertiary care hospital-a cross sectional study. Internet J Epidemiol. 2013;11:1. [Google Scholar]
- 24.Teimouri A, Iraj B, Amini M, Hovsepian S. The effect of quality of care on cardiovascular risk factors in newly diagnosed diabetic patients. Int J Prev Med. 2014;5:1432–8. [PMC free article] [PubMed] [Google Scholar]
- 25.Ellison RC, Zhang Y, Qureshi MM, Knox S, Arnett DK, Province MA. Investigators of the NHLBI Family Heart Study. Lifestyle determinants of high-density lipoprotein cholesterol: The National Heart, Lung, and Blood Institute Family Heart Study. Am Heart J. 2004;147:529–35. doi: 10.1016/j.ahj.2003.10.033. [DOI] [PubMed] [Google Scholar]
- 26.McFarlane SI, Jacober SJ, Winer N, Kaur J, Castro JP, Wui MA, et al. Control of cardiovascular risk factors in patients with diabetes and hypertension at urban academic medical centers. Diabetes Care. 2002;25:718–23. doi: 10.2337/diacare.25.4.718. [DOI] [PubMed] [Google Scholar]