

Abstract
Balaghat district in Central India is characterized by perennial malaria transmission. In this study, we have estimated malaria parasite rates by microscopic examination of blood smears by conducting active (ACD) and passive surveillance (PCD) in the villages of Baihar community health center (CHC) during January 2012–December 2012. Comparison of the results of two methods revealed that ACD (active case detection) in villages provides relatively large numbers of malaria positive cases (1408/3601) as compared to PCD (passive case detection) at CHC (139/2743) (OR 12.03, 95% CI, 9.97–14.57, p < 0.0001). Similarly, large numbers of Plasmodium falciparum cases (1194) were found (SFR, 33.2%) in villages, while only 98 P. falciparum cases (SFR, 3.6%) were found at CHC (OR 13.39, 95% CI, 10.80–16.73, p < 0.0001). Likewise, Plasmodium vivax were 211 (SVR, 5.9%) in villages by ACD (OR 4.1, 95% CI, 2.91–5.9, p < 0.0001), while only 41 P. vivax (SVR, 1.5%) were found at CHC. In this cross-sectional study, we discussed the potential role of ACD in strengthening of surveillance for high coverage. For malaria elimination initiative, a surveillance system must be more sensitive than PCD along with effective tools for vector control to target high-risk population who are not visiting the health facility and seed transmission to the surrounding population. The study highlights the substantial difference in the malaria positivity rate by two methods in difficult and hard-to-reach areas and recommendations are made to understand how best to deploy ACD methods in the pursuit of malaria elimination.
Keywords: Active surveillance, Passive surveillance, Malaria, Plasmodium falciparum, Plasmodium vivax, Central India, Tribal, Microscopic examination
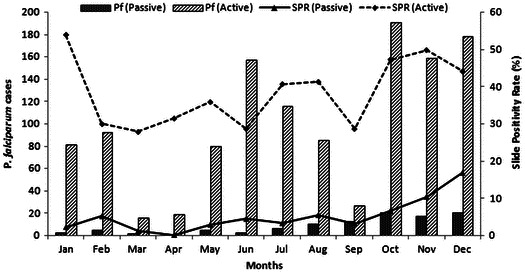
Graphical abstract showing the month wise active and passive malaria prevalence.
Introduction
Malaria is a major health problem in tribal areas of the India. A recent study indicated that 8% of India’s population residing in tribal areas contributes to 46% of total malaria, 70% of Plasmodium falciparum and 47% of malarial deaths in the country.1 Another study revealed that tribal households had 1.4 times more chances of malaria when compared to other social groups and backward class households living in the same area and exposed to similar malarious conditions.2 Parasite rates are important indicators of disease burden3 and malaria risk is not equally distributed within a population, and variation in the risk of malaria within a population is poorly understood particularly in tribal areas of India.4,5
Balaghat district (longitude 80°15′E, latitude 21°84′N) in Central India is highly malarious with perennial transmission of malaria in a forested region where both P. falciparum and Plasmodium vivax are prevalent, and P. malariae also found6,7 (Fig. 1). An epidemiological study on the dynamics of forest malaria in Balaghat revealed that there are two highly efficient vectors i.e. Anopheles culicifacies and Anopheles fluviatilis and both are involved in perennial transmission of malaria,7 though the area is under two rounds of indoor residual spray (IRS) with synthetic pyrethroids. Understanding the multifaceted determinants of malaria transmission is important in areas of perennial malaria transmission. Most malaria control programs have passive surveillance systems to identify, treat, and report individuals who present themselves to health facilities.8 It is known that passive surveillance grossly underestimated the malaria prevalence as only those patients receive treatment when they seek medical care, thus it would have a limited impact on malaria transmission. On the contrary, active surveillance which involves screening of population by visiting door to door, targeting of all subjects with fever or history of fever is suitable for difficult and hard-to-reach areas in an attempt to increase access to care in underserved areas.8,9 This study was undertaken to understand the epidemiology and pattern of malaria in an endemic area by PCD in comparison with ACD carried out in the same area.
Figure 1.

Map of India showing state of Madhya Pradesh; district Balaghat and study villages in Baihar community health center.
Material and methods
This cross-sectional study was undertaken in forest villages of Baihar community health center (CHC), Balaghat district, for one year (January 2012–December 2012). These villages are located at a distance of 5–35 km from the CHC and public transport facility is not available. The inhabitants of the Baihar CHC are mainly Baiga, particularly vulnerable tribes, who are less educated and less wealthy compared to the general population and have immense faith in sorcery and witchcraft. People are reluctant to go to a health facility and prefer to approach their spiritual leader for treatment. The details of the study area have been published elsewhere.7 Their houses are poorly constructed, scattered in fields and the forest on undulating terrain. The local economy is forest based. Most of the inhabitants of the villages work as laborers in forest nurseries, road construction, and other casual jobs. P. falciparum was a dominant parasite species throughout the year. Spleen rate was 43.8% in young children (2–9 years). Two efficient vector species, i.e. A. culicifacies and A. fluviatilis, were involved in malaria transmission during most part of the year i.e. 10 months.7 The study area is under two rounds of IRS with synthetic pyrethroid (First round in May–June and second round in August–September). Seasons are defined as a spring (February–March), summer (April–June), monsoon (July–September), post-monsoon (October–November) and winter (December–January).
A malaria clinic was established at Baihar CHC by National Institute for Research in Tribal Health (NIRTH). All the symptomatic patients from 30 study villages (Population 20,000) who visited CHC with fever, body ache and other symptoms were screened for malaria parasites (PCD). A finger-prick blood sample was obtained from all symptomatic individuals under sterile conditions using disposable equipment. Thick and thin blood smears were prepared, stained with JSB stain,10 and examined under the microscope on the spot at CHC. A report of the result and treatment was given to all individuals prior to their departure from the clinic. In the same 30 villages, ACD was undertaken by a trained field team of NIRTH comprising a medical officer, one technician and two field assistants and a driver. The community was informed of active surveillance through community leaders. The active surveillance was carried out once a month by visiting door to door, and started at 8 AM after taking written informed consent.
A finger-prick blood sample was obtained from all individuals who participated in the ACD program. The field assistants assist in the preparation of blood smears and staining the slides which were also brought to CHC for processing. The results of the blood smears were made available the next day along with treatment.
The technician examined 100 fields in thick smears before declaring it negative. For quality control, 100% of positive smears and 10% of negative smears were re-examined by a second expert who was unaware of previous results. All P. falciparum cases were given ACT (artesunate + SP) and primaquine (PQ) and all P. vivax cases were given CQ and PQ as per national guidelines.11 Pregnant women and infants were not given primaquine.
The data were double-key entered in MS Access 2003 (Microsoft Corporation, Redmond, Washington, USA) based data entry screen. Data analysis was done using SPSS 17 for Windows (SPSS Inc. Chicago, IL). Age was recoded as a categorical variable (<1, >1–4, >4–8, >8–14 and >14 and above) before analysis. Gametocyte carriers were recorded only for P. falciparum.
The slide positivity rate (SPR) is the proportion of examined thick films was found positive for malaria parasite and the related slide falciparum rate (SFR) and slide vivax rate (SVR) were calculated. The P. falciparum percentage was defined as the number of blood smears found positive for P. falciparum in all blood smears positive for malaria. The study is approved by the Institutional Ethics Committee.
Results
Comparison of the results by two methods revealed that ACD in villages provides relatively large numbers of positive cases (1408/3601) as compared to PCD at CHC (139/2743) (OR 12.03, 95% CI, 9.97–14.57, p < 0.0001). Similarly, large numbers of P. falciparum cases (1194) were found (SFR, 33.2%) in villages, while only 98 P. falciparum cases (SFR, 3.6%) were found at CHC (OR 13.39, 95% CI, 10.80–16.73, p < 0.0001). Gametocytes were recorded in 12% patients in ACD as against 4% in PCD. Similarly, P. vivax were 211 (SVR, 5.9%) in villages by ACD (OR 4.1, 95% CI, 2.91–5.9, p < 0.0001), while only 41 P. vivax (SVR, 1.5%) were found at CHC.
Age-group wise stratification revealed (Table 1) that highest SPR was found in young children of 1–4 years when compared to adults by both ACD (OR 3.6, 95% CI, 2.7–4.7, p < 0.0001) and PCD (OR 2.2, 95% CI, 1.3–3.9, p < 0.005). ACD revealed that gametocytes were highest in young children aged 1–4 years (OR 1.9, 95% CI, 1.0–3.7) followed by relatively older children aged 4–8 years (OR 1.9, 95% CI, 1.1–3.3) and infants less than 1 year (OR 1.6, 95% CI, 0.6–4.1) when compared to adults. By PCD, very few gametocytes were found; hence, no trend was observed.
Table 1.
Age-group wise malaria prevalence in Baihar clinic and villages of Baihar CHC, district Balaghat
| Survey type | Age group | BSE | Pos | Pf | Pv | Pfg | SPR | SFR | SVR | Pf (%) | Pv (%) | Pfg (%) | OR malaria (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Passive | ≤1 year | 17 | 1 | 1 | 0 | 0 | 5.9 | 5.9 | 0.0 | 100.0 | 0.0 | 0.0 | 1.4 (0.2−10.4) |
| >1–4 years | 174 | 16 | 8 | 8 | 1 | 9.2 | 4.6 | 4.6 | 50.0 | 50.0 | 12.5 | 2.2 (1.3–3.9)* | |
| >4–8 years | 250 | 16 | 14 | 2 | 1 | 6.4 | 5.6 | 0.8 | 87.5 | 12.5 | 7.1 | 1.5 (0.9–2.6) | |
| >8–14 years | 344 | 20 | 15 | 5 | 0 | 5.8 | 4.4 | 1.5 | 75.0 | 25.0 | 0.0 | 1.3 (0.8–2.2) | |
| >14 years | 1958 | 86 | 60 | 26 | 2 | 4.4 | 3.1 | 1.3 | 69.8 | 30.2 | 3.3 | Ref.[1] | |
| Total | 2743 | 139 | 98 | 41 | 4 | 5.1 | 3.6 | 1.5 | 70.5 | 29.5 | 4.1 | ||
| Active | ≤1 year | 148 | 70 | 52 | 18 | 7 | 47.3 | 35.1 | 12.2 | 74.3 | 25.7 | 13.5 | 2.7 (1.9–3.9)** |
| >1–4 years | 310 | 168 | 128 | 39 | 20 | 54.2 | 41.3 | 12.6 | 76.2 | 23.2 | 15.6 | 3.6 (2.7–4.7)** | |
| >4–8 years | 648 | 307 | 262 | 44 | 40 | 47.4 | 40.4 | 6.8 | 85.3 | 14.3 | 15.3 | 2.7 (2.2–3.4)** | |
| >8–14 years | 1484 | 611 | 514 | 97 | 58 | 41.2 | 34.6 | 6.5 | 84.1 | 15.9 | 11.3 | 2.1 (1.8–2.5)** | |
| >14 years | 1011 | 252 | 238 | 13 | 21 | 24.9 | 23.5 | 1.3 | 94.4 | 5.2 | 8.8 | Ref.[1] | |
| Total | 3601 | 1408# | 1194 | 211 | 146 | 39.1 | 33.2 | 5.9 | 84.8 | 15.0 | 12.2 |
Passive collection: patients visited the hospital clinic; active fever surveillance: door–to-door visits for surveillance of fever cases in villages.
BSE: blood slide examination; Pos: positive for malaria; Pf: Plasmodium falciparum; Pv: Plasmodium vivax; Pfg: Plasmodium falciparum gametocyte; SPR: slide positivity rate; SFR: slide falciparum rate; SVR: slide vivax rate.
p < 0.005.
p < 0.0001.
Three cases were P. malariae.
Season wise analysis revealed that the SPR was highest in winter and lowest in spring (OR 4.0, 95% CI, 1.5–10.8, p < 0.005) by PCD (Table 2), while highest SPR was observed in the post-monsoon and lowest in spring season by ACD (OR 2.2, 95% CI, 1.8–2.9, p < 0.0001). Gametocytes were significantly more in post-monsoon season as compared to other seasons. (χ2 = 39.18, p < 0.0001).
Table 2.
Season wise malaria prevalence in Baihar clinic and villages of Baihar CHC, district Balaghat
| Survey Type | Season | BSE | Pos | Pf | Pv | Pfg | SPR | SFR | SVR | Pf (%) | Pv (%) | Pfg (%) | OR Malaria (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Passive | Spring (February–March) | 170 | 5 | 5 | 0 | 1 | 2.9 | 2.9 | 0.0 | 100.0 | 0.0 | 20.0 | Ref.[1] |
| Summer (April–June) | 515 | 16 | 6 | 10 | 1 | 3.1 | 1.2 | 1.9 | 37.5 | 62.5 | 16.7 | 1.1 (0.4–2.9) | |
| Monsoon (July–September) | 1212 | 46 | 28 | 18 | 1 | 3.8 | 2.3 | 1.5 | 60.9 | 39.1 | 3.6 | 1.3 (0.5–3.3) | |
| Post Monsoon (October–November) | 624 | 48 | 37 | 11 | 1 | 7.7 | 5.9 | 1.8 | 77.1 | 22.9 | 2.7 | 2.8 (1.1–7.0) | |
| Winter (December–January) | 222 | 24 | 22 | 2 | 0 | 10.8 | 9.9 | 0.9 | 91.7 | 8.3 | 0.0 | 4.0 (1.5–10.8)* | |
| Total | 2743 | 139 | 98 | 41 | 4 | 5.1 | 3.6 | 1.5 | 70.5 | 29.5 | 4.1 | ||
| Active | Spring (February–March) | 406 | 120 | 107 | 13 | 0 | 29.6 | 26.4 | 3.2 | 89.2 | 10.8 | 0.0 | Ref.[1] |
| Summer (Apriil–June) | 1003 | 313 | 254 | 56 | 30 | 31.2 | 25.3 | 5.6 | 81.2 | 17.9 | 11.8 | 1.1 (0.8–1.4) | |
| Monsoon (July–September) | 752 | 289 | 226 | 63 | 20 | 38.4 | 30.1 | 8.4 | 78.2 | 21.8 | 8.8 | 1.4 (1.2–1.9)** | |
| Post Monsoon (October–November) | 799 | 386 | 348 | 38 | 65 | 48.3 | 43.6 | 4.8 | 90.2 | 9.8 | 18.7 | 2.2 (1.8–2.9)* | |
| Winter (December–January) | 641 | 300 | 259 | 41 | 31 | 46.8 | 40.4 | 6.4 | 86.3 | 13.7 | 12.0 | 2.1 (1.6–2.7)* | |
| Total | 3601 | 1408# | 1194 | 211 | 146 | 39.1 | 33.2 | 5.9 | 84.8 | 15.0 | 12.2 |
Passive collection: patients visited the hospital clinic; active Fever Surveillance: door-to-door visits for surveillance of fever cases in villages.
BSE: blood slide examination; Pos: positive for malaria; Pf: Plasmodium falciparum; Pv: Plasmodium vivax; Pfg: Plasmodium falciparum gametocyte; SPR: slide positivity rate; SFR: slide falciparum rate; SVR: slide vivax rate.
p < 0.005.
p < 0.0001.
Three cases were P. malariae.
Table 3 showed village wise malaria positivity by ACD. Though all the villages are highly malarious but village-to-village variations are common. Average SPR of 30 villages was 38.8 (95%CI 35.2–42.4) and ranged from 17.9 to 62.2%; similarly, average SFR was 32.95 (95%CI 29.5–36.4) and ranged from 13.7 to 57.5%. The average proportion of P. vivax was 14.8 (95%CI 11.8–17.9) and P. falciparum was 84.8 (95% CI 81.6–88.0).
Table 3.
Village wise (active case detection) showing malaria positive P. falciparum and P. vivax
| Village Code | BSE | Pos | Pf | Pv | SPR | SFR | SVR | Pf (%) | Pv (%) |
|---|---|---|---|---|---|---|---|---|---|
| AA | 95 | 17 | 13 | 4 | 17.9 | 13.7 | 4.2 | 76.5 | 23.5 |
| AB | 115 | 55 | 53 | 2 | 47.8 | 46.1 | 1.7 | 96.4 | 3.6 |
| AC | 117 | 46 | 38 | 8 | 39.3 | 32.5 | 6.8 | 82.6 | 17.4 |
| AD | 80 | 28 | 22 | 6 | 35.0 | 27.5 | 7.5 | 78.6 | 21.4 |
| AE | 91 | 21 | 19 | 2 | 23.1 | 20.9 | 2.2 | 90.5 | 9.5 |
| AF | 84 | 40 | 22 | 17 | 47.6 | 26.2 | 20.2 | 55.0 | 42.5 |
| AG | 166 | 65 | 54 | 11 | 39.2 | 32.5 | 6.6 | 83.1 | 16.9 |
| AH | 175 | 80 | 69 | 11 | 45.7 | 39.4 | 6.3 | 86.3 | 13.8 |
| AI | 118 | 51 | 45 | 6 | 43.2 | 38.1 | 5.1 | 88.2 | 11.8 |
| AJ | 74 | 26 | 25 | 1 | 35.1 | 33.8 | 1.4 | 96.2 | 3.8 |
| AK | 114 | 44 | 37 | 7 | 38.6 | 32.5 | 6.1 | 84.1 | 15.9 |
| AL | 149 | 85 | 71 | 14 | 57.0 | 47.7 | 9.4 | 83.5 | 16.5 |
| AM | 181 | 64 | 49 | 15 | 35.4 | 27.1 | 8.3 | 76.6 | 23.4 |
| AN | 121 | 38 | 32 | 6 | 31.4 | 26.4 | 5.0 | 84.2 | 15.8 |
| AO | 128 | 47 | 41 | 6 | 36.7 | 32.0 | 4.7 | 87.2 | 12.8 |
| AP | 196 | 87 | 74 | 13 | 44.4 | 37.8 | 6.6 | 85.1 | 14.9 |
| AQ | 204 | 59 | 52 | 7 | 28.9 | 25.5 | 3.4 | 88.1 | 11.9 |
| AR | 116 | 40 | 29 | 11 | 34.5 | 25.0 | 9.5 | 72.5 | 27.5 |
| AS | 118 | 54 | 41 | 12 | 45.8 | 34.7 | 10.2 | 75.9 | 22.2 |
| AT | 75 | 28 | 27 | 1 | 37.3 | 36.0 | 1.3 | 96.4 | 3.6 |
| AU | 91 | 35 | 30 | 5 | 38.5 | 33.0 | 5.5 | 85.7 | 14.3 |
| AV | 128 | 66 | 53 | 13 | 51.6 | 41.4 | 10.2 | 80.3 | 19.7 |
| AW | 127 | 79 | 73 | 6 | 62.2 | 57.5 | 4.7 | 92.4 | 7.6 |
| AX | 80 | 26 | 21 | 4 | 32.5 | 26.3 | 5.0 | 80.8 | 15.4 |
| AY | 93 | 42 | 39 | 3 | 45.2 | 41.9 | 3.2 | 92.9 | 7.1 |
| AZ | 92 | 34 | 29 | 5 | 37.0 | 31.5 | 5.4 | 85.3 | 14.7 |
| BA | 140 | 41 | 35 | 6 | 29.3 | 25.0 | 4.3 | 85.4 | 14.6 |
| BB | 114 | 44 | 39 | 5 | 38.6 | 34.2 | 4.4 | 88.6 | 11.4 |
| BC | 137 | 30 | 27 | 3 | 21.9 | 19.7 | 2.2 | 90.0 | 10.0 |
| BD | 82 | 36 | 35 | 1 | 43.9 | 42.7 | 1.2 | 97.2 | 2.8 |
BSE: blood slide examination; Pos: positive for malaria; Pf: Plasmodium falciparum; Pv: Plasmodium vivax; Pfg: Plasmodium falciparum gametocyte; SPR: slide positivity rate; SFR: slide falciparum rate; SVR: slide vivax rate.
Discussion
Malaria is a major challenge in the forested tribal belt where no public transport system is available and health infrastructure is poor.7,12 With a year-round presence in some parts of the country, it exacts an unacceptable toll on the health of the people of all ages.13 Moreover, population movement in and out of the forest was common and there was no mechanism in place to check these movements.14 Extending effective and appropriate care in such sparsely populated areas is difficult due to lack of resources.15 Recently, India launched the national malaria elimination program to eliminate malaria from India in a phase wise manner by 2030.
The PCD only detects symptomatic patients and overlook individuals who are not seeking treatment. Identifying hyperendemic communities within endemic areas constitutes an important challenge for malaria control and elimination as this population contributes disproportionately to malaria transmission. By treating these individuals, not only the community would be protected, but has also resulted in substantial reduction in transmission intensity. Targeting these high-risk populations prevents the spread of malaria more widely as was done in Brazil.16 Otherwise, the population who is not visiting health facilities, seed transmission in the surrounding population in receptive areas, thus creating new foci. The greatest risk of malaria among children of 1–4 years of age observed in this study was comparable to an earlier finding from this area7 and nearby tribal areas.17 Gametocytes were present in 12% of the subjects by ACD and highest during post-monsoon months which is the main transmission season. The prevalence of gametocytes is commonly used as a parameter of malaria transmission.18
Strengthening of surveillance to achieve high coverage is a priority and an alternative to ACD which would overcome the shortcomings of missed cases, who cannot seek treatment, is a mass screening of the population in high-risk areas which can be best performed through screen and treat campaign. However, in inaccessible forested areas, screen and treat campaign can be practically possible using rapid diagnostic tests (RDTs) by visiting house to house and testing consenting people and dispensing anti-malarials for malaria parasites.19,20 However, low parasite density could be a major limitation for wide-scale testing by RDTs.21−23 Moreover, the operational feasibility and acceptability of malaria workers administering RDTs and ACTs within the community in remote areas needs careful evaluation. Furthermore, these communities should be screened at times when people are at home i.e. early morning or late evening. All missed cases should be covered by another visit in the same area to enhance the coverage. Demographic characteristics of these missed people will provide important information of people at high risk and they would not be missed. Many of them might be infected who can amplify transmission by transmitting the malaria parasites to a large number of mosquitoes.24 Studies conducted earlier showed that in hard-to-reach areas, community-wide coverage with the IRS or insecticide-treated bed nets (ITNs) is difficult to achieve in a field situation.7 Moreover, a high coverage with ITNs may not be a guarantee for a sustained decline of malaria as it is linked with lack of proper use and mosquito biting behavior.25 These intervention tools bring a substantial reduction in malaria transmission but have limitation for malaria elimination.26,27
This cross-sectional study for the first time in our knowledge has estimated the malaria positivity by ACD v. PCD methods in the same area and has shed light on the substantial difference in the malaria positivity rate by two methods. A reliance on PCD will miss many infections thereby preventing access to diagnosis and treatment among populations at higher risk of malaria. More research on the operational feasibility of ACD and mass screening need to be explored to enable the development of evidence-based strategies for malaria prevention and elimination in inaccessible areas. Such an approach warrants investigation in the context of impact on malaria control and financial implication.
This study has some limitations. The two methods (ACD v. PCD) are actually not comparable as people visiting CHC are screened for malaria irrespective of fever or history of fever. On the contrary, in villages, only fever or cases with history of fever were screened for malaria once in a month. Moreover, our surveillance was confined to a small rural population. This probably explains why we found 39% malaria positivity in villages as against 5% at the CHC. Even though ACT is in the place as a first-line treatment, it is in short supply and there is no drug resistance against ACT.7 Access to treatment is also an important indicator of the success of the malaria control in that interventions need to reach remote communities at increased risk of malaria. The minimum distance of a village from CHC is 5 km in this study while traditional healers hail from the same community, live among them, and are always available, which is another reason for their preference of the community.28−30
How active surveillance will be deployed to pursue malaria elimination is a challenge. A malaria eradication research agenda consultative group suggested that any parasitaemia, whether high or low density, has the potential for malaria transmission and therefore is a threat to malaria elimination efforts.31 Active surveillance played a major role in interrupting malaria transmission in Sri Lanka.32 This study suggests that ACD tailored to the local epidemiological setting should be considered as a potential tool complementary to other antimalarial measures to achieve and maintain malaria control and thereby its elimination. This is further supported by the fact that malaria surveillance systems are estimated to detect only 14% of all malaria cases worldwide.33 Strong malaria surveillance system is fundamental to both program design and implementation.
Ethical approval
The study protocol was approved by the institutional review board of the National Institute for research in Tribal Health (NIRTH), Jabalpur, Madhya Pradesh.
Funding
This study received financial support from the Indian Council of Medical Research (ICMR), New Delhi.
Acknowledgements
We thank all the study participants and their relatives for providing the informed consent. We thank all the project staff at the Community Health Centre, Baihar, Balaghat, for their help and support. Thanks are also due to Dr. Ravendra Sharma, Scientist D, NIRTH for help in statistical analysis.
References
- 1.Sharma RK, Thakor HG, Saha KB, Sonal GS, Dhariwal AC, Singh N. Malaria situation in India with special reference to tribal areas. Indian J Med Res. 2015;141(5):537–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sharma RK, Singh MP, Saha KB, Bharti PK, Jain V, Singh PP, et al. Socio-economic & household risk factors of malaria in tribal areas of Madhya Pradesh, Central India. Indian J Med Res. 2015;141(5):567–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hay SI, Snow RW. The malaria atlas project: developing global maps of malaria risk. PLoS Med. 2006;3(12):e473. 10.1371/journal.pmed.0030473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Singh N, Shukla MM, Dash AP. Control of malaria in Central India (Madhya Pradesh) hope or hype. Trans R Soc Trop Med Hyg. 2009;103(2):209–10. 10.1016/j.trstmh.2008.09.017 [DOI] [PubMed] [Google Scholar]
- 5.Singh N. A new global malaria eradication strategy: implications for malaria research from an Indian perspective. Trans R Soc Trop Med Hyg. 2009;103(12):1202–3. 10.1016/j.trstmh.2009.04.023 [DOI] [PubMed] [Google Scholar]
- 6.Bharti PK, Chand SK, Singh MP, Mishra S, Shukla MM, Singh R, et al. Emergence of a new focus of Plasmodium malariae in forest villages of district Balaghat, Central India: implications for the diagnosis of malaria and its control. Trop Med Int Health. 2013;18(1):12–17. 10.1111/tmi.12005 [DOI] [PubMed] [Google Scholar]
- 7.Singh N, Chand SK, Bharti PK, Singh MP, Chand G, Mishra AK, et al. Dynamics of forest malaria transmission in Balaghat District, Madhya Pradesh, India. PLoS ONE. 2013;8(9):e73730 10.1371/journal.pone.0073730 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sturrock HJ, Hsiang MS, Cohen JM, Smith DL, Greenhouse B, Bousema T, et al. Targeting asymptomatic malaria infections: active surveillance in control and elimination. PLoS Med. 2013;10(6):e1001467 10.1371/journal.pmed.1001467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Singh N, Shukla MM, Chand G, Bharti PK, Singh MP, Shukla MK, et al. Epidemic of Plasmodium falciparum malaria in Central India, an area where chloroquine has been replaced by artemisinin-based combination therapy. Trans R Soc Trop Med Hyg. 2011;105(3):133–9. 10.1016/j.trstmh.2010.11.002 [DOI] [PubMed] [Google Scholar]
- 10.Singh J, Bhattacharji LM. Rapidstaining of malarial parasites by a water soluble stain. Ind Med Gaz. 1944;79:102–4. [PMC free article] [PubMed] [Google Scholar]
- 11.National Vector Borne Disease Control Programme National drug policy. 2010. [cited 2016 Mar 15]; Available from: http://www.nvbdcp.gov.in/Doc/drug-policy-2010.pdf
- 12.Singh N, Mishra AK, Shukla MM, Chand SK. Forest malaria in Chhindwara, Madhya Pradesh (Central India) – a case study in an ethnic tribal community. Am J Trop Med Hyg. 2003;68(5):602–7. [DOI] [PubMed] [Google Scholar]
- 13.Pradhan A, Anasuya A, Pradhan MM, Ak K, Kar P, Sahoo KC et al. Trends in Malaria in Odisha, India–an analysis of the 2003–2013 time-series data from the national vector borne disease control program. PLoS ONE. 2016. Feb 11;11(2):e0149126. doi: 10.1371/journal.pone.0149126 10.1371/journal.pone.0149126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Singh N, Singh OP, Sharma VP. Dynamics of malaria transmission in forested and deforested region of Mandla district, Central India, Madhya Pradesh. J Am Mosq Control Assoc. 1996;12(2):225–34. [PubMed] [Google Scholar]
- 15.Singh N, Dash AP, Krongthong T. Fighting malaria in Madhya Pradesh (Central India): are we loosing the battle? Malar J. 2009;8(1):93. doi: 10.1186/1475-2875-8-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wesolowski A, Eagle N, Tatem AJ, Smith DL, Noor AM, Snow RW, et al. Quantifying the impact of human mobility on malaria. Science. 2012;338:267–70. 10.1126/science.1223467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chand G, Chaudhary NK, Soan V, Kaushal LS, Sharma RK, Singh N. Transmission dynamics & epidemiology of malaria in two tribal districts in Madhya Pradesh, India. Indian J Med Res. 2015;141(5):556–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bousema JT, Gouagna LC, Drakeley CJ, Meutstege AM, Okech BA, Akim IN, et al. Plasmodium falciparum gametocyte carriage in asymptomatic children in western Kenya. Malar J. 2004;3(18). doi: 10.1186/1475-2875-3-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yekutiel P. Problems of epidemiology in malaria eradication. Bull World Health Organ. 1960;22(6):669–83. [PMC free article] [PubMed] [Google Scholar]
- 20.Macauley C. Aggressive active case detection: a malaria control strategy based on the Brazilian model. Soc Sci Med. 2005;60(3):563–73. 10.1016/j.socscimed.2004.05.025 [DOI] [PubMed] [Google Scholar]
- 21.Bridges DJ, Winters AM, Hamer DH. Malaria elimination: surveillance and response. Pathog Global Health. 2012;106(4):224–31. 10.1179/2047773212Y.0000000035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McMorrow ML, Aidoo M, Kachur SP. Malaria rapid diagnostic tests in elimination settings–can they find the last parasite? Clin Microbiol Infect. 2011;17(11):1624–31. 10.1111/j.1469-0691.2011.03639.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Singh N, Shukla MM, Shukla MK, Mehra RK, Sharma S, Bharti PK, et al. Field and laboratory comparative evaluation of rapid malaria diagnostic tests versus traditional and molecular techniques in India. Malar J. 2010;9:191. doi: 10.1186/1475-2875-9-191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Smith DL, McKenzie FE, Snow RW, Hay SI. Revisiting the basic reproductive number for malaria and its implications for malaria control. PLoS Biol. 2007;5(3):e42 10.1371/journal.pbio.0050042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Pulford J, Hetzel MW, Bryant M, Siba PM, Mueller I. Reported reasons for not using a mosquito net when one is available: a review of the published literature. Malar J. 2011;10:83. doi: 10.1186/1475-2875-10-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fegan GW, Noor AM, Akhwale WS, Cousens S, Snow RW. Effect of expanded insecticide-treated bednet coverage on child survival in rural Kenya: a longitudinal study. Lancet. 2007;370(9592):1035–9. 10.1016/S0140-6736(07)61477-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bhattarai A, Ali AS, Kachur SP, Mårtensson A, Abbas AK, Khatib R, et al. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PLoS Med. 2007;4(11):e309 10.1371/journal.pmed.0040309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Singh N, Singh MP, Saxena A, Sharma VP, Kalra NL. Knowledge, attitude, beliefs and practices (KABP) study related to malaria intervention strategies in ethnic tribals of Mandla (Madhya Pradesh). Curr Sci. 1998;75(12):1386–1390. [Google Scholar]
- 29.Sundararajan R, Kalkonde Y, Gokhale C, Greenough PG, Bang A. Barriers to malaria control among marginalized tribal communities: a qualitative study. PLoS ONE. 2013;8(12):e81966. doi: 10.1371/journal.pone.0081966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Vijayakumar KN, Gunasekaran K, Sahu SS, Jambulingam P. Knowledge, attitude and practice on malaria: a study in a tribal belt of Orissa state, India with reference to use of long lasting treated mosquito nets. Acta Trop. 2009. Nov;112(2):137–42. doi: 10.1016/j.actatropica.2009.07.011. [DOI] [PubMed] [Google Scholar]
- 31.The Malera Consultative Group on Diagnoses and Diagnostics A research agenda for malaria eradication: diagnoses and diagnostics. PLoS Med. 2011;8(1):e1000396. doi: 10.1371/journal.pmed.1000396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wickremasinghe R, Fernando SD, Thillekaratne J, Wijeyaratne PM, Wickremasinghe AR. Importance of active case detection in a malaria elimination programme. Malar J. 2014. May;13(1):186 10.1186/1475-2875-13-186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.World Health Organization (WHO) World Malaria Report. 2013. Available from: http://www.who.int/malaria/publications/world_malaria_report_2013/wmr2013_no_profiles.pdf?ua=1