

Abstract
Background
Chinese herbal medicine has been used to treat hypertension in China and East Asia since centuries. In this study, we conduct an overview of systematic reviews of Chinese herbal medicine in the treatment of primary hypertension to 1) summarize the conclusions of these reviews, 2) evaluate the methodological quality of these reviews, and 3) rate the confidence in the effect on each outcome.
Methods
We comprehensively searched six databases to retrieve systematic reviews of Chinese herbal medicine for primary hypertension from inception to December 31, 2015. We used AMSTAR to evaluate the methodological quality of included reviews, and we classified the quality of evidence for each outcome in included reviews using the GRADE approach.
Results
A total of 12 systematic reviews with 31 outcomes were included, among which 11 systematic reviews focus on the therapeutic effect of Chinese herbal medicine combined with conventional medicine or simple Chinese herbal medicine versus simple conventional medicine. Among the 11 items of AMSTAR, the lowest quality was “providing a priori design” item, none review conformed to this item, the next was “stating the conflict of interest” item, only three reviews conformed to this item. Five reviews scored less than seven in AMSTAR, which means that the overall methodological quality was fairly poor. For GRADE, of the 31 outcomes, the quality of evidence was high in none (0 %), moderate in three (10 %), low in 19 (61 %), and very low in nine (29 %). Of the five downgrading factors, risk of bias (100 %) was the most common downgrading factor in the included reviews, followed by imprecision (42 %), inconsistency (39 %), publication bias (39 %), and indirectness (0 %).
Conclusions
The methodological quality of systematic reviews about Chinese herbal medicine for primary hypertension is fairly poor, and the quality of evidence level is low. Physicians should be cautious when applying the interventions in these reviews for primary hypertension patients in clinical practice.
Electronic supplementary material
The online version of this article (doi:10.1186/s13643-016-0353-y) contains supplementary material, which is available to authorized users.
Keywords: Chinese herbal medicine, Primary hypertension, Overview, GRADE, Quality of evidence, Methodological quality
Background
Primary hypertension is associated with structural changes of the heart and blood vessels, which may lead to cardiovascular morbidity (i.e., cardiovascular disease, stroke, peripheral vascular disease, renal disease, and Alzheimer’s) and mortality. However, the pathogenesis of primary hypertension remains unclear at present [1]. Primary hypertension is typically defined as having a systolic blood pressure (SBP) ≥140 mmHg and a diastolic blood pressure (DBP) ≥90 mmHg [2, 3]. Globally, approximately one billion people are affected by primary hypertension [2], and seven million deaths per year may be related to primary hypertension [4]. In addition, for every 20 mmHg increase in SBP and 10 mmHg increase in DBP (through the range from 115/75 to 185/115 mmHg) among people aged 40 to 70 years, the risk of cardiovascular disease (CVD) morbidity doubles [2].
The current practice focuses on achieving a target blood pressure level less than 140/90, which is believed to be helpful in reducing the risk of stroke and myocardial infarction and improving quality of life. However, while hypertension contributes to adverse cardiovascular outcomes, lowering blood pressure to below this arbitrary value has not been convincingly shown to reduce cardiovascular morbidity and mortality [5]. This finding highlights the importance of finding safe and effective treatments to prevent hypertension-related mortality and morbidity.
The ultimate aim of treating hypertension is to reduce morbidity and mortality with minimum adverse effects. Diuretics, beta-blockers, calcium-channel blockers, and angiotensin-converting enzyme (ACE) inhibitors are commonly used as antihypertensive drugs [6–8]. Although many different antihypertensive drugs are available, the BP levels of approximately two thirds of the patients under treatment have not reached the target level [3, 9]. Even if blood pressure has been controlled within a normal range, patients may still have high cardiovascular morbidity and mortality rates [10].
Chinese herbal medicine has been used to treat hypertension in China and East Asia since centuries. It usually applies a combination of several (often more than 10) herbs that make up a formula under the guidance of traditional theory. Understanding the effect of Chinese herbal medicine on blood pressure could be valuable for the management of high blood pressure. Currently, there are several systematic reviews published regarding the effect of Chinese herbal medicine on primary hypertension, which indicated that Chinese herbal medicines (e.g., the liuwei dihuang pill and tianma gouteng yin) were effective and safe for primary hypertension when compared with conventional treatments (e.g., diuretics, beta-blockers, calcium-channel blockers, and ACE inhibitors) [11–13], but the quality of evidence were unclear. In order to establish the efficacy and safety of Chinese herbal medicine for treating primary hypertension, an overview is needed to (1) summarize the conclusions of these reviews, (2) evaluate the methodological quality of these reviews, and (3) rate the confidence in the effect on each outcome.
Methods
Search strategy
Systematic searches of the following electronic databases were conducted: PubMed (1950 to December 2015), Chinese Biomedical database (1980 to December 2015), China Knowledge Resource Integrated Database (1980 to December 2015), and Wanfang database (1998 to December 2015), Search strategies for PubMed, EMBASE, and Chinese Biomedical database consisted of relevant MeSH terms, which were adapted for the respective databases and are available on request. Text word “Chinese herbal medicine”, “traditional Chinese medicine” and “alternative medicine” were used to search target reviews. Only English and Chinese papers were included. An additional file shows more search strategy detail (see Additional file 1).
Selection of reviews
We included systematic reviews that met the following criteria: (1) evaluated the effects of Chinese herbal medicine on primary hypertension compared with conventional drugs; (2) provided a clearly defined clinical question, inclusion and exclusion criteria, and searching strategies; and (3) summarized the results for at least one desired outcome. Systematic reviews that had insufficient information for data extraction, translations, and duplicates were excluded.
Data extraction
Two reviewers (ZXK and FMX) independently extracted information from the included studies using a standard form. We used original study reports only if specific data were missing. We extracted the following information:
Basic information including publication year, retrieval strategy, inclusion criteria, quality assessment methods, and conclusions
Number of included studies and participants
Drug used, dose, and formulation (if formulation was available)
Outcomes (including desirable outcomes and adverse events)
Assessment of methodological quality and quality of evidence
Methodological quality
We used the assessing the methodological quality of systematic reviews (AMSTAR) [14] scale to assess the methodological quality of the included reviews. Each review was assessed by two researchers (ZXK and FMX) independently, and any disagreements were resolved by a third author (LYD). For each item, a judgment of “yes” or “no” was assigned according to judgment criteria of AMSTAR. An additional file provides the criterion to score methodological quality of systematic reviews (see Additional file 2). The number of “yes” will be counted as the total score of AMSTAR, which can reflect the overall methodological quality of reviews. If the total score is less than seven, which indicates the overall methodological quality of review is poor. The assessment process was based on the following 11 items:
Was a priori design provided?
Was there duplicate study selection and data extraction?
Was a comprehensive literature search performed?
Were published and unpublished studies included irrespective of language of publication?
Was a list of studies (included and excluded) provided?
Were the characteristics of the included studies provided?
Was the scientific quality of the included studies assessed and documented?
Was the scientific quality of the included studies used appropriately in formulating conclusions?
Were the methods used to combine the findings of studies appropriate?
Was the likelihood of publication bias assessed?
Was a conflict of interest stated?
Quality of evidence
The quality of evidence reflects the extent to which confidence in an estimate of the effect is adequate to support a particular recommendation [15]. The quality of evidence for each outcome was rated following the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Handbook [15] by two reviewers (ZXK and FMX) independently, and disagreements were resolved by a third reviewer (LYD). GRADE classified the quality of evidence into four levels: high, moderate, low, and very low (Table 1) [15]. The rating process was based on the following five downgrading factors.
-
i)
Risk of bias was assessed on the basis of the methodological quality of RCTs included in the systematic reviews and considered allocation concealment, blinding, incomplete outcome data, selective reporting, and other factors [16, 17]. In this review, we rated the factor relied on the risk of bias assessments by the authors of the included reviews.
-
ii)
Inconsistency (i.e., heterogeneity) was assessed according to the outcomes of the χ 2 test and I 2 statistic reported in the systematic reviews. If I 2 was >50 %, P < 0.05, and the heterogeneity could not be explained by conducting subgroup analysis or meta-regression, the quality of evidence was downgraded [18].
-
iii)
Indirectness was defined as having an indirect comparison in one of the following four aspects: population, intervention, comparator, and outcome (PICO). These four aspects were judged depending on the target PICO of interest [19].
-
iv)
Imprecision was assessed in different ways for different types of data. For dichotomous outcomes, the quality of evidence was downgraded if either of the following two conditions were true [20]: (1) the total number of events was less than 300, or (2) the 95 % confidence interval (CI) of pooled risk ratio/odds ratio included both 1 and either 0.75 or 1.25. For continuous outcomes, the reasons for downgrading were (1) total population size less than 400, or (2) the 95 % CI of pooled mean difference/weighted mean difference included 0 and either −0.5 or 0.5.
-
v)
Publication bias was assessed through funnel plots and Egger’s test. A two-tailed P value of <0.05 was considered to indicate publication bias. When there are only few studies included in the systematic review, the publication bias is challenging to interpret by funnel plots or statistical tests. Under these circumstances, we assessed publication bias based on the search methodology, databases searched, whether filters had been used, and inclusion of unpublished studies and gray literature (conference abstracts, protocols, and books) [21].
Table 1.
Definition of the four levels of evidence by GRADE [15]
| Quality level | Definition |
|---|---|
| High | We are very confident that the true effect lies close to that of the estimate of the effect |
| Moderate | We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different |
| Low | Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect |
| Very low | We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect |
For each downgrade factor, a judgment of “no”, “serious” (downgrade by one level), or “very serious” (downgrade by two levels) was assigned. At the very beginning, the quality of evidence of all outcomes were classified as “high” by default; after rating, each outcome received a quality level of high, moderate, low, or very low.
Data analysis
A narrative description of the included reviews was undertaken. We have tabulated review-level summaries for all the outcomes listed above from each of the included reviews. Where outcomes were meta-analyzed within a review, we extracted and reported pooled effect sizes. Where no quantitative pooling of effect sizes was reported, or where outcomes were reported descriptively by single studies, we reported these results using a standardized language indicating direction of effect and statistical significance. For continuous outcomes, we summarized data using the weighted mean difference (WMD) with 95 % confidence interval (CI) as reported in the included reviews. For dichotomous outcomes, we presented the risk ratio (RR) or odds ratio (OR) and 95 % CI as appropriate.
Results
A total of 2260 records yielded from electronic databases. After removing duplicates, 1477 studies were screened by the titles or abstracts and 422 studies were assessed through the full texts. Finally, 12 systematic reviews about Chinese herbal medicine for primary hypertension were included in this overview [11–13, 22–30] (Fig. 1).
Fig. 1.

Flow diagram showing the search process and study selection
Description of the included reviews
Among the 12 included reviews, all the reviews were published in Chinese, the publication time ranged from 2006 to 2014, and 83 % [11–13, 22–26, 29, 30] were published in the recent 5 years. Four reviews [11, 12, 22, 23] reported the age of the patients, and one [23] reported the follow-up time. Only one review compared Chinese herbal medicine with conventional drugs [13]; the others compared Chinese herbal medicine combined with conventional drugs against single conventional drugs. Nine reviews [13, 22–28, 30] adopted the Jadad scale, and three [21, 23, 24] used risk of bias tools [31] to assess the methodological quality of RCTs included in the review. Table 2 shows the characteristics of included systematic reviews.
Table 2.
Characteristics of the included systematic reviews
| Researchers and publication time | Types of included studies | Number of studies (total sample) | Age | Interventions | Follow-up time | Evaluation criteria of methodology | Conclusions | |
|---|---|---|---|---|---|---|---|---|
| Treatment group | Control group | |||||||
| Chen 2014 [11] | RCT | 12 (1001) | 39–80 | Banxia baizhu tianma tang + conventional medicine | Conventional medicine | – | Jadad | As compared with conventional medicine banxia baizhu tianma tang combined with it can improve the clinical curative effect in treating high blood pressure |
| Wang 2012 [12] | RCT | 11 (981) | 36–86 | Danshen injection + control group | Hemostatic agents、dehydrator, regulation of blood pressure, brain cell protective agent | 6 months | Jadad | Danshen injection has a certain treatment effect in treating hypertensive cerebral hemorrhage, and the earlier the better |
| Guo 2013 [13] | RCT | 14 (1364) | – | Liuwei dihuang pill + conventional medicine | Conventional medicine | – | Jadad | The whole therapy effect of liuwei dihuang pill combined with conventional medicine is better than that of single conventional medicine, and so do the SBP and DBP |
| Zhou 2012 [22] | RCT | 8 (554) | – | Tianma gouteng yin + captopril | Captopril | – | Jadad | Compared with single captopril, the clinical efficacy of tianma gouteng yin combined with captopril is more better, which can improve symptoms with better blood pressure effect |
| Dong 2011 [23] | RCT | 6 (543) | – | Tianma gouteng yin + captopril | Captopril | – | Jadad | Tianma gouteng yin may obtain better treatment result and more security than enalapril in treatment of essential hypertension |
| Ren 2006 [24] | RCT | 11 (1010) | – | TCM combination therapy including Chinese herb medicine, Chinese patent medicines, acupuncture, etc.) + conventional medicine | Conventional medicine | – | Jadad | Traditional Chinese medicine may have similar effect with conventional medicine in primary hypertension therapy |
| Dai 2010 [25] | RCT | 9 (655) | – | Therapied by Chinese herb medicine or combined with conventional medicine | Conventional medicine | – | Jadad | Traditional Chinese medicine can reduce the SBP and DBP effectively, improve efficiency, integrated Chinese and Western treatment is more better |
| Du 2014 [26] | RCT | 10 (1777) | – | Yangxue qingnao granules + conventional medicine | Conventional medicine | – | Risk of bias | Yangxue qingnao granules can significantly improve headache, dizziness, insomnia symptoms of high blood pressure |
| Li 2012 [27] | RCT | 17 (1323) | – | TCM combination therapy including Chinese herb medicine compound, Chinese patent medicines, acupuncture, etc.) + conventional medicine | Conventional medicine | – | Jadad | Traditional Chinese medicine has a certain effect in treatment of elderly hypertension patients and reduced pulse pressure with symptoms reduced |
| Xiong 2012 [28] | RCT | 16 (1424) | 19–78 | Banxia baizhu tianma tang + blood pressure drugs | Blood pressure drugs or placebo | – | Risk of bias | Banxia baizhu tianma tang has better antihypertensive effect |
| Wang 2013 [29] | RCT | 22 (1808) | 30–74 | Tianma gouteng yin + blood pressure drugs | Blood pressure drugs | – | Risk of bias | The efficacy and safety evidence of tianma gouteng yin, as an adjunct of blood pressure medicine, needs further study |
| Wu 2013 [30] | RCT | 9 (784) | – | Tianma gouteng yin | Conventional medicine | – | Jadad | Tianma gouteng yin can effectively lower the SBP and DBP |
“–”means do not report related information
Methodological quality of the included reviews
AMSTAR scale was used to evaluate the methodological quality of the included reviews. All of the included reviews were not registered [11–13, 22–30] in advance. Five reviews [24, 25, 27, 28, 30] did not provide the search strategies, which could not respect the process of the literature selection and data extraction. Five reviews [23–27] did not search gray literature, two reviews [27, 29] did not provide information of the included and excluded articles, and six reviews [24–27, 29, 30] did not provide the basic information of the included articles. Additionally, one review [30] did not appropriately explain the findings of studies, four reviews [11–13, 28, 30] did not assess for publication bias, and nine studies [22–30] did not state the conflicts of interest. Table 3 shows the methodological quality of the included studies.
Table 3.
AMSTAR for methodological quality of included systematic reviews
| Included studies | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Item 10 | Item 11 | Total score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chen 2014 [11] | N | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | 9 |
| Wang 2012 [12] | N | Y | Y | N | Y | Y | Y | Y | Y | Y | N | 8 |
| Guo 2013 [13] | N | N | Y | N | Y | N | Y | Y | Y | Y | N | 6 |
| Zhou 2012 [22] | N | N | Y | N | Y | N | Y | Y | Y | Y | N | 6 |
| Dong 2011 [23] | N | Y | Y | N | Y | N | Y | Y | Y | Y | N | 7 |
| Ren 2006 [24] | N | N | N | N | N | N | Y | Y | Y | Y | N | 4 |
| Dai 2010 [25] | N | N | Y | Y | Y | Y | Y | Y | Y | N | N | 7 |
| Du 2014 [26] | N | Y | N | Y | N | N | Y | Y | Y | Y | N | 6 |
| Li 2012 [27] | N | N | N | Y | Y | N | Y | N | Y | Y | N | 5 |
| Xiong 2012 [28] | N | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 9 |
| Wang 2013 [29] | N | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 9 |
| Wu 2013 [30] | N | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | 9 |
Y means adequate; N means inadequate. Item 1. Was an a priori design provided? Item 2. Was there duplicate study selection and data extraction? Item 3. Was a comprehensive literature search performed? Item 4. Were published and unpublished studies included irrespective of language of publication? Item 5. Was a list of studies (included and excluded) provided? Item 6. Were the characteristics of the included studies provided? Item 7. Was the scientific quality of the included studies assessed and documented? Item 8. Was the scientific quality of the included studies used appropriately in formulating conclusions? Item 9. Were the methods used to combine the findings of studies appropriate? Item 10. Was the likelihood of publication bias assessed? Item 11. Was a conflict of interest stated?
Effect of interventions
Antihypertensive effect
Seven reviews [11, 13, 22–24, 27, 30] analyzed the antihypertensive effect of Chinese herbal medicines on treating primary hypertension; among which five reviews [22, 24–26, 30] indicated that Chinese herbal medicine combined with the conventional medicine is better than the single conventional medicine, and the difference was statistically significant (P < 0.05). The combination of Chinese herbal medicines and conventional medicine including banxia baishu tianma tang plus conventional medicine [11] (OR = 1.19 [1.12, 1.26], moderate quality of evidence), liuwei dihuang pill plus conventional medicine [13] (OR = 1.16 [1.11, 1.21], moderate quality of evidence), tianma goutengyin plus captopril [23] (OR = 4.69 [2.58, 8.53], low quality of evidence), and acupuncture plus conventional medicine [27] (OR = 2.63 [1.99, 3.47], low quality of evidence). See Fig. 2 for more information.
Fig. 2.
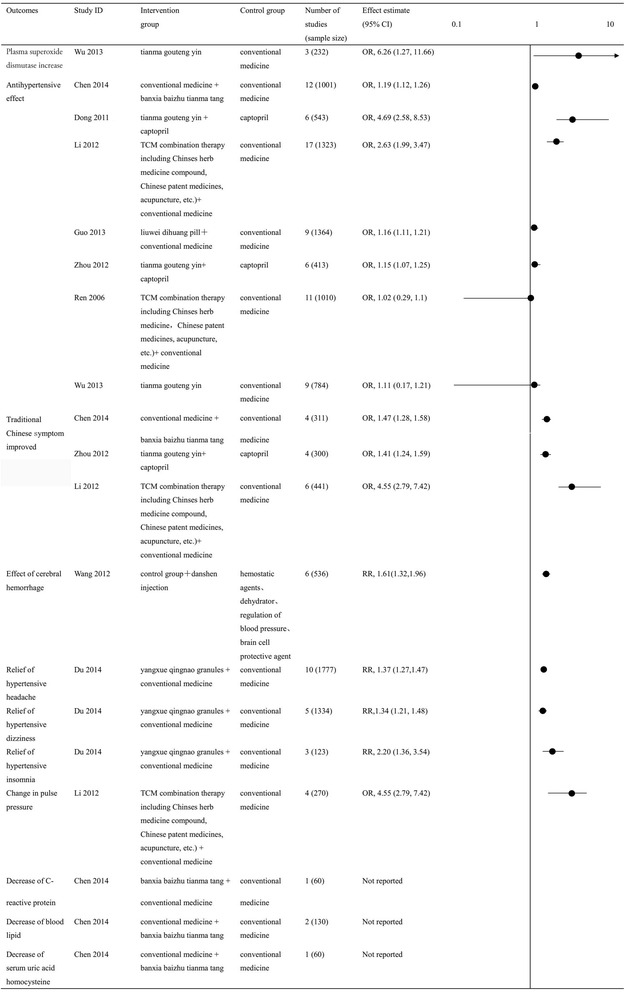
Summary of findings for dichotomous outcomes
Decreasing SBP and DBP effect
Three reviews [25, 28, 29] analyzed the changes of SBP and DBP levels in patients using Chinese herbal medicines to treat primary hypertension. All the three reviews showed that traditional Chinese medicine combined with conventional medicine were more efficient than single conventional medicine on the effect of SBP. The combination of Chinese herbal medicines and conventional medicine can decease SBP including Chinses herb medicine plus conventional medicine [25] (WMD = −4.15 [−7.70, −0.61], low quality of evidence), banxia baizhu tianma tang plus blood pressure drugs [28] (WMD = −12.3 [−13.52, −10.54], low quality of evidence), and tianma goutengyin plus blood pressure drugs [29] (WMD = −4.33 [−8.44, −0.22], low quality of evidence). However, only one review [28] showed a beneficial result for DBP [WMD, −7.98 (−8.85, −7.12), low quality of evidence] (Fig. 3).
Fig. 3.

Summary of findings for continuous outcomes
Traditional Chinese symptom improvement
Three reviews [11, 22, 27] analyzed the traditional Chinese symptom improvement. All reviews showed that banxia baizhu tianma tang (OR = 1.47 [1.28, 1.58], low quality of evidence), tianma gouteng yin (OR = 1.41 [1.24, 1.59], low quality of evidence), and acupuncture (OR = 4.55 [2.79, 7.42], low quality of evidence), combined with conventional medicine were better than single conventional medicine for traditional Chinese symptom improvement; all differences were statistically significant (P < 0.05) (Fig. 2).
Adverse events
Five reviews [11, 12, 22, 23, 28] evaluated adverse events associated with Chinese herbal medicine combined with conventional medicine, including headaches, swelling, heart palpitations, and lethargy. Two reviews [23, 28] reported that Chinese herbal medicine (tianma gouteng yin and banxia baizhu tianma tang) combined with conventional medicine for the treatment of primary hypertension was safe, without any adverse reactions noted.
Summary of other findings
One review [26] indicated that yangxue qingnao granules combined with conventional medicine had a better effect on hypertensive headache (RR = 1.37 [1.27, 1.47]), hypertensive dizziness (RR = 1.34 [1.21, 1.48]), and hypertensive insomnia (RR = 2.20 [1.36, 3.54]) than conventional medicine. Another review [11] compared banxia baizhu tianma tang plus conventional medicine with conventional medicine alone; however, they did not report the effects on C-reactive protein, blood lipid, serum uric acid, or homocysteine levels. This indicates that a selective reporting bias existed in this review.
Summary of quality of evidence
A total of 31 outcomes were measured by the 12 included reviews [11–13, 22–30]. Among these outcomes, the quality of evidence was high in none (0 %), moderate in three (10 %), low in 19 (61 %), and very low in nine (29 %). Of the five downgrading factors, the risk of bias (n = 31, 100 %) was the most common downgrading factor in the included reviews, followed by imprecision (n = 13, 42 %), inconsistency (n = 12, 39 %), publication bias (n = 12, 39 %), and indirectness (n = 0, 0 %). According to GRADE, the risk of bias is defined as a defect in random sequence generation, allocation concealment, blinding, incomplete outcome data, selective reporting, and other bias. Among these, random sequence generation was the most important factor contributing to the overall poor quality for these reviews. Table 4 shows the quality of evidence of the included reviews.
Table 4.
GRADE for quality of evidence profile
| Study ID | Outcomes (number of studies) | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Quality of evidence |
|---|---|---|---|---|---|---|---|
| Chen 2014 [11] | Overall antihypertensive effect (12) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low |
| Traditional Chinese symptom improved (4) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| Decrease of C-reactive protein (1) | Seriousa | No serious | No serious | Seriousd | Strongly suspectedb | Very low | |
| Decrease of blood lipid (2) | Seriousa | Seriousc | No serious | Seriousd | Undetected | Very low | |
| Decrease of serum uric acid homocysteine (2) | Seriousa | No serious | No serious | Seriousd | Strongly suspectede | Very low | |
| Adverse events (1) | Seriousa | No serious | No serious | Seriousd | Strongly suspectede | Very low | |
| Wang 2012 [12] | Effect of cerebral hemorrhage (6) | Seriousa | No serious | No serious | No serious | Undetected | Moderate |
| Nervous function defect of cerebral infarction score (8) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| Adverse events (5) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| Guo 2013 [13] | Overall antihypertensive effect (9) | Seriousa | No serious | No serious | No serious | Undetected | Moderate |
| Zhou 2012 [22] | Overall antihypertensive effect (6) | Seriousa | No serious | No serious | No serious | Undetected | Moderate |
| Traditional Chinese symptom improved (4) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| safety (5) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| Dong 2011 [23] | Overall antihypertensive effect (6) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low |
| safety (2) | Seriousa | No serious | No serious | Seriousd | Strongly suspectede | Very low | |
| Ren 2006 [24] | Overall antihypertensive effect (11) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low |
| Dai 2010 [25] | Decrease of systolic blood pressure (9) | Seriousa | No serious | No serious | Seriousd | Undetected | Low |
| Decrease of diastolic blood pressure (9) | Seriousa | No serious | No serious | Seriousd | Undetected | Low | |
| Du 2014 [26] | Relief of hypertensive headache (10) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low |
| Relief of hypertensive dizziness (5) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low | |
| Relief of hypertensive insomnia (3) | Seriousa | No serious | No serious | Seriousd | Strongly suspectedb | Very low | |
| Li 2012 [27] | Overall antihypertensive effect (17) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low |
| Traditional Chinese symptom improved (6) | Seriousa | No serious | No serious | No serious | Strongly suspectedb | Low | |
| Changes of pulse pressure (4) | Seriousa | Seriousc | No serious | Seriousd | Undetected | Very low | |
| Xiong 2012 [28] | Decrease of systolic blood pressure (3) | Seriousa | Seriousc | No serious | Seriousd | Undetected | Very low |
| Decrease of diastolic blood pressure (3) | Seriousa | Seriousc | No serious | Seriousd | Undetected | Very low | |
| Adverse events (4) | Seriousa | No serious | No serious | Seriousd | Undetected | Low | |
| Wang 2013 [29] | Decrease of systolic blood pressure (3) | Seriousa | Seriousc | No serious | No serious | Undetected | Low |
| Decrease of diastolic blood pressure (3) | Seriousa | Seriousc | No serious | No serious | Undetected | Low | |
| Wu 2013 [30] | Plasma superoxide dismutase increase (3) | Seriousa | No serious | No serious | Seriousd | Undetected | Low |
| Overall antihypertensive effect (9) | Seriousa | Seriousc | No serious | No serious | Undetected | Low |
aUnclear random sequence generation, allocation concealment blinding not done in all studies
bStatistical test for publication bias was underpowered
c I 2 >50 %
dInsufficient sample size and wide confidence interval
eIncomplete retrieval for unpublished studies and gray literature
Discussion
Although the systematic review is one of the most important research methods and provides the strongest level of evidence in evidence-based medicine [32], only those reviews with qualified methodologies and a high quality of evidence can provide comprehensive and reliable evidence to decisionmakers [33]; otherwise, review findings are likely to mislead decisionmakers. An overview of systematic reviews is a comprehensive evaluation method, which summarizes the findings, detects the methodological quality, and grades the evidence quality of all systematic reviews on one disease. In this overview, almost 60 % of the systematic reviews were found to have a good methodology quality (AMSTAR score ≥7). A summary of the findings of these reviews showed that Chinese herbal medicine combined with conventional medicine in the treatment of primary hypertension has better efficacy and safety than treatment with a single conventional medicine. This finding might reflect that Chinese herbal medicine combined with conventional medicine can improve the clinical symptoms and delay disease progression in patients with primary hypertension. Additionally, Chinese herbal medicine combined with conventional medicine offers the potential to reduce side effects and medical costs when compared with single conventional medicine.
However, we found that 90 % of the outcomes were of low or very low quality of evidence when using the GRADE criteria to evaluate the systematic reviews, indicating that the true effect might be substantially different from the effect estimated in these reviews. Of the five downgrading factors, the risk of bias was the most common factor downgrading the level of evidence. All of the outcomes from the 12 reviews were downgraded for this factor, and failure of random sequence generation was the most important factor contributing to the overall poor risk of bias scores. This indicates that rigorous training on conducting Chinese herbal medicine trials for investigators is warranted. Imprecision was downgraded most often due to insufficient sample size, while inconsistency was downgraded due to unreasonable inclusion criteria and large I 2 squared values. Finally, downgrading of evidence for publication bias was most commonly due to not reviewing gray literature and presenting underpowered statistical tests.
Most of the outcomes in the systematic reviews of Chinese herbal medicine for primary hypertension were surrogate outcomes, such as blood pressure and nervous function defect score. These outcomes do not reflect all effects of the complex pathological process associated with primary hypertension [33] or substitute for the measurement of end-outcomes such as mortality, end-organ damage, stroke, coronary artery disease, and renal failure. Sometimes, advantages might outweigh the disadvantages when we use surrogate outcomes to measure the effectiveness of an intervention. For example, clofibrate, a fibrate lipid-lowering drug for ischemic heart disease patients, could reduce the risk of ischemic heart disease in patients by 20 %, but the all-cause mortality increased to 44 % [34]. Therefore, future studies assessing the use of Chinese herbal medicine in treatment of primary hypertension need to be conducted with a focus on end outcomes.
This overview has several strengths: we used a structured and explicit approach, a comprehensive search strategy, and eligibility criteria designed to identify systematic reviews about the use of Chinese herbal medicine for the treatment of primary hypertension. We also created strict quality assessment criteria to evaluate the methodological quality and the quality of evidence for each review, which increases the validity and reliability of the findings. We used the GRADE system, a previously validated scientific approach, to rate the quality of the evidence. This overview, however, also has some limitations: we excluded systematic reviews that had insufficient information for extracting data, which might introduce selection bias. Publication bias was also sometimes challenging to assess with funnel plots and Egger’s test. For instance, although the formal statistical tests showed no significant publication bias, these tests might have been severely underpowered given the small number of original studies in the systematic reviews. Some systematic reviews using the fixed effect model resulted in a large I 2 values (more than 50 %), which were incorrect. Finally, some of the reviews’ authors might desire to compare Chinese herbal medicine versus drugs, and some of the authors were Chinese medical workers, so it is possibility exist interpretation bias in some reviews.
Conclusions
Physicians should be cautious when applying the interventions in these reviews for primary hypertension patients in clinical practice. Our overview suggests that the methodological quality and quality of evidence in Chinese herbal medicine for primary hypertension is fairly poor. More efforts must be made to improve the quality of RCTs about Chinese herbal medicine. First, clinical trials about Chinese herbal medicine should be designed in high methodological quality, registered on the Chinese Clinical Trial Register (ChiCTR) platform [35], and reported following CONSORT checklist [36, 37] to minimize bias. Second, systematic reviews about Chinese herbal medicine should be conducted following the Cochrane Handbook for Systematic Reviews [31] to improve the methodological quality and report the systematic reviews according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement; Third, Chinese GRADE Center should make a further effort to spread the GRADE system and train guideline developers on how to make recommendations based on low and very low quality evidence [38].
Acknowledgements
We thank Siqi Fu, Wei Deng, Nan Yang, Rongrong Cui, Peiyu Zhang, and Rui Li (Mikevier PharmaScience Co. Ltd) for extracting data and rating quality of evidence. Enping Yang, Zhi Yi (Mikevier PharmaScience Co. Ltd), and Janne Estill (Institute of Social and Preventive Medicine, University of Bern, Switzerland) for providing assistance with editing the final manuscript.
Funding
This study was supported by the National Nature Science Foundation of China (No. 81160478).
Authors’ contributions
ZXK, LYD, and FMX contributed to the concept and design of the study and data analysis. LK, CKB, and LYQ collected the data and revised the article. SSB, SP, and LB contributed to the draft and critical revision of the article. All authors contributed to the interpretation of study data and critically reviewed and approved the manuscript before submission.
Competing interests
The authors declare that they have no competing interests.
Abbreviations
- ACE
Angiotensin-converting enzyme
- AMSTAR
Assessing the Methodological Quality of Systematic Reviews
- CBM
Chinese Biomedical database
- ChiCTR
Chinese Clinical Trial Register
- CI
Confidence interval
- CNKI
China Knowledge Resource Integrated Database
- CVD
Cardiovascular disease
- DBP
Diastolic blood pressure
- GRADE
Grading of Recommendations, Assessment, Development, and Evaluation
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
Randomized controlled trials
- SBP
Systolic blood pressure
Additional files
Search strategy. The process of how to search PubMed, EMBASE, Cochrane library, CBM, CNKI, and Wang fang database was given in this file. (PDF 180 KB)
Judgment criteria of AMSTAR. This file provided a criterion of how to score the methodological quality of systematic reviews. (PDF 165 KB)
Contributor Information
Zhao Xinke, Email: zxkd412@163.com.
Li Yingdong, Email: lydj412@163.com.
Feng Mingxia, Email: fmx0706@126.com.
Liu Kai, Email: liukai_2006@126.com.
Chen Kaibing, Email: 422375418@qq.com.
Lu Yuqing, Email: luyuqinmq@126.com.
Sun Shaobo, Email: sunmorning.sun@foxmail.com.
Song Peng, Email: songp06@163.com.
Liu Bin, Email: 1055352783@qq.com.
References
- 1.Marushco YV, Zlobynets AS. Clinical features and optimization of the treatment of children with combination gastroduodenal pathology and primary hypertension. Lik Sprava. 2015;(1-2):132-4. [PubMed]
- 2.Daskalopoulou SS, Rabi DM, Zarnke KB, Dasgupta K, Nerenberg K, et al. The 2015 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2015;31(5):549–68. doi: 10.1016/j.cjca.2015.02.016. [DOI] [PubMed] [Google Scholar]
- 3.Chobanian AV, Bakris GL, Black HR, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8) JAMA. 2014;311(5):507–20. doi: 10.1001/jama.2013.284427. [DOI] [PubMed] [Google Scholar]
- 4.World Health Organization. International Society of Hypertension Writing Group 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J Hypertens. 2003;21:1983–92. doi: 10.1097/00004872-200311000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Go AS, Bauman MA, Coleman King SM, Fonarow GC, Lawrence W, et al. An effective approach to high blood pressure control: a science advisory from the American Heart Association, the American College of Cardiology, and the Centers for Disease Control and Prevention. J Am Coll Cardiol. 2014;63(12):1230–8. doi: 10.1016/j.jacc.2013.11.007. [DOI] [PubMed] [Google Scholar]
- 6.Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the american society of hypertension and the international society of hypertension. J Clin Hypertens (Greenwich) 2014;16(1):14–26. doi: 10.1111/jch.12237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.ESH/ESC Task Force for the Management of Arterial Hypertension 2013 ESH/ESC Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) J Hypertens. 2013;31(10):1925–38. doi: 10.1097/HJH.0b013e328364ca4c. [DOI] [PubMed] [Google Scholar]
- 8.Sheridan S. Primary prevention: hypertension. Clinical Evidence (http://clinicalevidence.bmj.com/). BMJ, (Assessed 18 Oct 2015). [PubMed]
- 9.Odusola AO, Stronks K, Hendriks ME, Schultsz C, Akande T. Enablers and barriers for implementing high-quality hypertension care in a rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers. Glob Health Action. 2016;9:29041. doi: 10.3402/gha.v9.29041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.World Health Organization. Prevention of cardiovascular disease: guidelines for assessment and management of total cardiovascular risk. Geneva: WHO; 2007.
- 11.Xinyu C, Linglong Y, Zixuan L, et al. Meta-analysis of Banxia Baizhu Tianma decoction in treatment of primary hypertension. Liaoning J Tradit Chin Med. 2014;41(02):196–9. [Google Scholar]
- 12.Qiong W. Salvia Injection for hypertensive hemorrhage: a meta-analysis[D]. Hangzhou: Zhe Jiang University; 2012. [Article in Chinese].
- 13.Yixin G, Xinlin C, Zhenwen Q, et al. Meta-analysis and systematic reviews of Liuweidihuang Pills combined with Western medicine on hypertension. J Emerg Tradit Chin Med. 2013;22(02):189–91. [Google Scholar]
- 14.Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. doi: 10.1186/1471-2288-7-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Schünemann H, Brożek J, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendation. [Updated October 2013]. The GRADE Working Group; 2013. Available from www.gradeworkinggroup.org.
- 16.GRADE Working Group Grading quality of evidence and strength of recommendations. BMJ. 2004;328(7454):1490. doi: 10.1136/bmj.328.7454.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zhou W, GE L, XU J, Shi XT, Liang L, An N, et al. Quality evaluation on the systematic reviews/meta-analyses related to interventions published in the Chinese journal of evidence-based medicine. Chin J Evid-based Med. 2013;13(4):482–8. [Google Scholar]
- 18.Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidence--inconsistency. J Clin Epidemiol. 2011;64(12):1294–302. doi: 10.1016/j.jclinepi.2011.03.017. [DOI] [PubMed] [Google Scholar]
- 19.Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence—indirectness. J Clin Epidemiol. 2011;64(12):1303–10. doi: 10.1016/j.jclinepi.2011.04.014. [DOI] [PubMed] [Google Scholar]
- 20.Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence—imprecision. J Clin Epidemiol. 2011;64(12):1283–93. doi: 10.1016/j.jclinepi.2011.01.012. [DOI] [PubMed] [Google Scholar]
- 21.Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines: 5. Rating the quality of evidence—publication bias. J Clin Epidemiol. 2011;64(12):1277–82. doi: 10.1016/j.jclinepi.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 22.Qainyi Z, Kaiqi M, Yixin G, et al. Therapeutic effect of Tianma Gouteng decoction combined with captopril in treatment of primary hypertension: a systematic review and meta-analysis. J Anhui Univ Chin Med. 2013;32(04):12–7. [Google Scholar]
- 23.Daxing D, Songlin Y, Nan Y, et al. Therapeutic effect of Tianma Gouteng decoction combined with enalapril in treatment of primary hypertension: a systematic review and meta-analysis. J Emerg Tradit Chin Med. 2011;20(05):762–4. [Google Scholar]
- 24.Yi R, Aihua O, Xiaozhong L. Traditional Chinese medicine for treatment of primary hypertension: a meta-analysis of randomized controlled trials. Shaanxi J Tradit Chin Med. 2006;27(07):794–6. [Google Scholar]
- 25.Juan D. Systematic review of traditional Chinese medicine for treatment of primary hypertension. J China Tradit Chin Med Inf. 2010;02(36):22–4. [Google Scholar]
- 26.Hao D, Xiaohua D. Efficacy of Yangxue Qingnao granule in treatment of associated symptoms of hypertension: a meta-analysis. J Anhui Univ Chin Med. 2014;33(1):8–11. [Google Scholar]
- 27.Dongna L, Chuanhua Y. Effects of Chinese medicine on elderly isolated systolic hypertension: a meta-analysis. Liaoning J Tradit Chin Med. 2012;39(05):812–5. [Google Scholar]
- 28.Xiong X, Yang X, Liu W, et al. Banxia Baizhu Tianma decoction for essential hypertension: a systematic review of randomized controlled trials. Evid Based Complement Alternat Med. 2012;2012:271462. doi: 10.1155/2012/271462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wang J, Feng B, Yang X, Liu W, et al. Tianma gouteng yin as adjunctive treatment for essential hypertension: systematic review of randomized controlled trials. Evid Based Complement Alternat Med. 2013;2013:706125. doi: 10.1155/2013/706125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wu X, Jiang X. Systematic review and meta analysis of randomized controlled trials on Tianmagouteng decoction in treatment of primary hypertension with liver Yang hyperactivity syndrome. J Tradit Chin Med. 2013;33(1):15–8. doi: 10.1016/S0254-6272(13)60094-1. [DOI] [PubMed] [Google Scholar]
- 31.Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration; 2011. Available from http://handbook.cochrane.org/.
- 32.Lunny C, Brennan SE, McDonald S, McKenzie JE. Evidence map of studies evaluating methods for conducting, interpreting and reporting overviews of systematic reviews of interventions: rationale and design. Syst Rev. 2016;5(1):4. doi: 10.1186/s13643-015-0178-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Xinfeng G, Quan Z, Shilong L. Thinking on surrogate outcomes, intermediary outcomes and their application in TCM clinical efficacy evaluation. Chin J Integr Tradit Wes Med. 2005;25(7):585–90. [PubMed] [Google Scholar]
- 34.Oliver MF, Heady JA, Morris JN, et al. For the Committee of Principal Investigators. WHO cooperative trial of primary prevention of ischemic heart disease with clofibrate to lower serum cholesterol: final mortality follow-up. Lancet. 1984;2:600–4. [PubMed] [Google Scholar]
- 35.Chinese Clinical Trial Register. http://www.chictr.org.cn (Accessed 22 Dec 2015).
- 36.Schulz KF, Altman DG, Moher D, CONSORT Group CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi: 10.1136/bmj.c332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869. doi: 10.1136/bmj.c869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Thornton J, Alderson P, Tan T, et al. Introducing GRADE across the NICE clinical guideline program. J Clin Epidemiol. 2013;66:124e31. doi: 10.1016/j.jclinepi.2011.12.007. [DOI] [PubMed] [Google Scholar]