

Abstract
Context/objective
To describe the technique and clinical results of percutaneous atlantoaxial anterior transarticular fixation combined with limited exposure posterior C1/2 arthrodesis in patients with a high-riding vertebral artery.
Design setting
Zhejiang Spine Center, China.
Participants
Five patients with a high-riding vertebral artery and an upper cervical fracture.
Interventions
Percutaneous atlantoaxial anterior transarticular screw fixation combined with limited exposure posterior C1/2 wire fusion.
Outcome measures
Computed tomography scans were used to assess the high-riding vertebral artery and feasibility of anterior transarticular screw fixation preoperatively. A Philadelphia collar was used to immobilize the neck postoperatively. Anteroposterior (open-mouth) and lateral views were obtained at pre/postoperation and at the follow-up.
Results
The operation was performed successfully on all of the patients, and no intraoperative operation-related complications such as nerve injury, vertebral artery, and soft tissue complications occurred. The mean follow-up period was 33.8 months (range: 24 to 58 months). No screw breakage, loosening, pullout, or cutout was observed. Bone union was achieved in all patients at the last follow-up.
Conclusions
Our small case series results suggested that percutaneous anterior transarticular screw fixation combined with mini-open posterior C1/2 wire fusion is a technically minimally invasive, safe, feasible, and useful method to treat patients with a high-riding vertebral artery.
Keywords: Percutaneous, Minimally invasive, Anterior transarticular screw fixation, High-riding vertebral artery, Gallie fusion
Introduction
The atlantoaxial instability caused by trauma or congenital malformation usually requires C1/2 arthrodesis. Posterior transarticular screw fixation with wiring techniques or laminar clamps are widely used by surgeons and considered as the golden standard for C1/2 fusion.1–3 However, the complicated structures of the atlantoaxial complex deem surgery for this region as high risk. Elgafy et al.4 have reported that approximately 10–23% of patients who require atlantoaxial arthrodesis have anatomic variations of the vertebral artery on at least one side and are not suitable for posterior transarticular screw fixation. The rate reported by Lau et al.5 is approximately 40%.
The anatomic feasibility of atlantoaxial anterior transarticular screw fixation has been reported by Lu et al.,6 and a biomechanical study of this technique has shown that it can achieve comparable biomechanical stability as posterior transarticular screw fixation.7 The method of inserting the anterior transarticular screw percutaneously has the advantages of being a minimally invasive procedure and having decreased blood loss, lessened postoperative pain, and an accelerated recovery time. The drawback of anterior transarticular screw fixation is that it cannot provide a sufficient bone bed for a bone graft.8
For five patients with a high-riding vertebral artery, to avoid injuring the vertebral artery and to decrease the trauma as much as possible, we performed percutaneous atlantoaxial anterior transarticular screw fixation combined with mini-open posterior C1/2 wire fusion.
Methods and materials
Between March 2007 and October 2010, five patients with a high-riding vertebral artery were treated by percutaneous atlantoaxial anterior transarticular screw fixation combined with limited exposure posterior C1/2 wire fusion in our department. Three of them were men and two were women, with an average age of 61.4 years old (range: 47–72 years old). Three patients had a Jefferson fracture with a rupture of the transverse ligament, one patient had a Jefferson fracture with a type II odontoid fracture, and one patient had an atlantoaxial dislocation. Computed tomography (CT) scans were used to assess the high-riding vertebral artery and the feasibility of anterior transarticular screw fixation preoperatively. Anteroposterior (open-mouth) and lateral views were also obtained preoperatively. The clinical data are shown in Table 1.
Table 1.
Clinical data of the five patients in this study
| Case | Age (yrs) | Sex | Clinical diagnosis | Follow-up (months) |
|---|---|---|---|---|
| 1 | 47 | M | Jefferson fracture, rupture of transverse ligament | 24 |
| 2 | 68 | F | Jefferson fracture, rupture of transverse ligament | 36 |
| 3 | 64 | M | Jefferson fracture, rupture of transverse ligament | 58 |
| 4 | 72 | M | Jefferson fracture, type II odontoid fracture | 24 |
| 5 | 56 | F | Atlantoaxial dislocation | 27 |
Operative technique
The patient underwent fiber-optic nasotracheal intubation and was positioned in the supine position on a radiolucent table, the head and neck were stabilized, and traction of approximately 3 kg was applied to Gardner-Wells calipers. A radiolucent dental pad was placed inside the mouth, high-resolution anteroposterior open-mouth and lateral views were obtained, and the procedure of percutaneous atlantoaxial anterior transarticular screw fixation was performed according to the methods reported previously by Li et al.9: an initial 5–10-mm incision was made anteriorly at approximately the level of the C4–5 disc space, and blunt artery forceps or finger tip dissection was carried out to the anterior border of the spinal column using the Smith-Robinson approach. A guide tube with a 1.2-mm inner diameter was inserted and reached the anterior border of C2. To insert the left screw, the tip of the guide tube was situated at the anterior border of C2 at approximately 5–10 mm left of the mid-line under the anteroposterior (AP) image. Next, a 1.2-mm-diameter K-wire with inserted inside the guide tube and aimed towards the center of the lateral mass at an angle of 20° to 30° to the mid-line on the anteroposterior view and 20° to 28° to the vertical line on the lateral view with a driller. After this, a protective tube (7.0 mm outer diameter and 6.0 mm inner diameter) was advanced, and the guide tube was subsequently removed. A recess for the screw was fashioned, a 3.5-mm or 4.0-mm cannulated screw was inserted over the K-wire, and the K-wire was removed if the screw was well positioned. A similar procedure was then repeated on the opposite side. Closure of the wound was done after checking for hemostasis (Figs. 1A–D).
Figure 1.
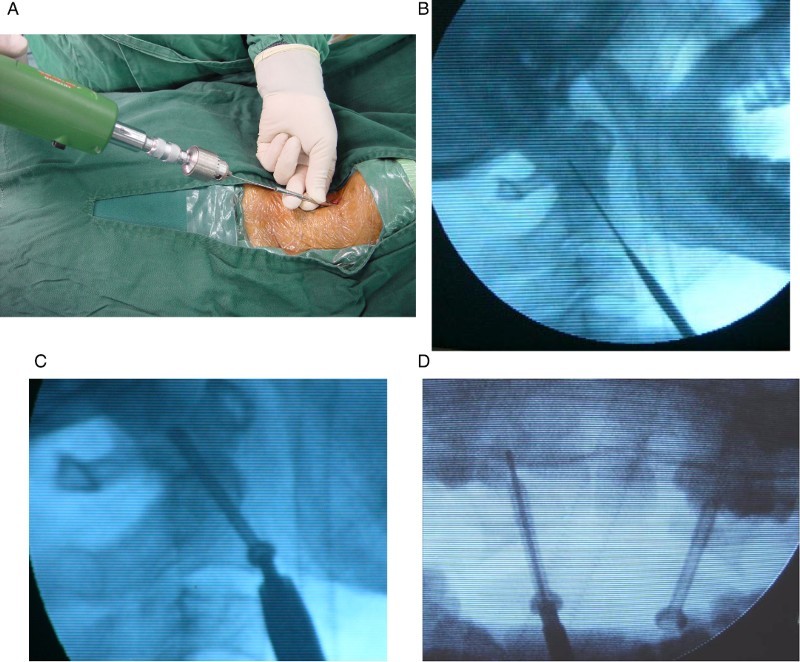
Photographs showing the percutaneous atlantoaxial anterior transarticular screw fixation procedure. A, B: A 1.2-mm Kirschner wire with a sharp tip was inserted inside the guide tube, which was aimed toward the center of the lateral mass. C, D: Two 3.5-mm cannulated screws were inserted over the K-wire, inside of the protective tube.
Next, the patient was positioned in the prone position. An initial midline skin incision of approximately 4 cm was made at the level of the C1/2 segment. The neck muscles were dissected, and the bony structure of C1/2 was exposed and decorticated. Gallie fusion was performed, and cancellous bone harvested from the iliac crest was grafted around C1/2. Closure of the wound was done after checking for hemostasis. A Philadelphia collar was used to immobilize the neck for 12 weeks postoperatively. Anteroposterior (open-mouth) and lateral views were obtained at postoperation and follow-up.
Results
The operation was performed successfully on all patients. The procedure of percutaneous atlantoaxial anterior transarticular screw fixation had a blood loss of less than 10 mL, which could be considered as negligible, while the blood loss of the posterior mini-open Gallie fusion procedure was less than 100 mL. No intraoperative operation-related complications such as nerve injury, vertebral artery, and soft tissue complications occurred. The mean follow-up period was 33.8 months (range: 24 to 58 months). No screw breakage, loosening, pullout, or cutout was observed. Bone union was achieved in all patients, and the rotation was reduced to approximately 50° at the last follow-up.
Case presentation
A 68-year-old woman complained of pain in her upper neck and numbness of both upper limbs after a fall accident. Preoperative CT showed a Jefferson fracture and a rupture of her transverse ligament (Figs. 2A and B). Due to her high-riding vertebral artery, we felt posterior transarticular screw fixation was unsuitable for her, so we performed percutaneous atlantoaxial anterior transarticular screw fixation and mini-open posterior C1/2 wire fusion on her (Figs. 2C–E). No screw breakage, loosening, pullout, or cutout was observed on anteroposterior and lateral views (Figs. 2F and 2G) at the last follow-up, and the numbness of her upper limbs had disappeared.
Figure 2.
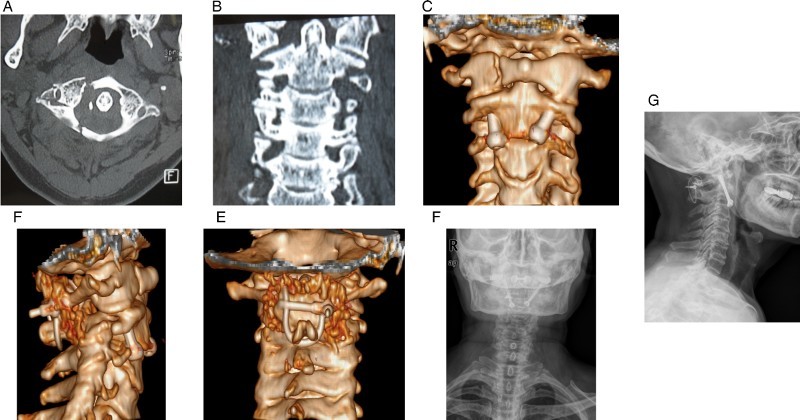
A, B: Preoperative CT showing a Jefferson fracture and a rupture of the transverse ligament of one patient. C–E: The postoperative CT 3D reconstruction by atlantoaxial anterior transarticular screw fixation and C1/2 wire fusion. F, G: The anteroposterior and lateral views at the last follow-up. Bone union was achieved; no screw breakage, loosening, pullout, or cutout was observed.
Discussion
There are many techniques reported to treat atlantoaxial instability, including Brooks fusion, Gallie fusion, and the interlaminar clamp,10,11 Magerl, and Harms techniques.12,13 The Magerl technique provides a better biomechanical property than posterior wiring.14–16 The combination of posterior transarticular screw fixation and the posterior one-point technique (Gallie or Brooks technique or Halifax clamps) as well as three-point fixation are widely used by surgeons. The three-point fixation can provide a high degree of stiffness in all ranges of motion,17 and it provides good clinical results.18 The posterior transarticular screw fixation technique was modified by McGuire and Harkey,19 and this three-point technique can also be performed as a minimally invasive method using a percutaneous transarticular screw and mini-open wire fusion.20,21 These modified methods have the advantages of having a smaller skin incision, less blood loss, and reduced muscular dissection.22 However, all of these techniques have a higher risk of vertebral artery injury,4,5 and many clinical studies have reported this complication.23–25 In fact, the vertebral artery injury may be catastrophic.26
To avoid the drawbacks of the Magerl technique, Harms et al.13 have designed the technique of “posterior C1–C2 polyaxial screw and rod fixation.” The Harms technique has a lower risk of vertebral artery injury than the Magerl technique. However, the Harms technique has some disadvantages, such as a longer duration of surgery, a longer hospital stay, more blood loss, and higher instrumentation costs27 than the Magerl technique. Moreover, it has been reported that some patients complain of complications related to postoperative C2 neuralgia.28
Additionally, approximately 8.5% of patients with small C2 pedicles were not suitable for the Harms technique.27 The rich venous plexus at the position of the C1 screw entry point would cause venous bleeding during the procedure with a wide exposure. Lu et al. have described the anatomic feasibility of atlantoaxial anterior transarticular screw fixation.6 Aided with instruments designed by one author (YLC), it is easy to insert the anterior transarticular screws percutaneously, which is technically feasible, safe, useful, and minimally invasive,9 with a skin incision of only approximately 10 mm. At the same time, the posterior skin wound of approximately 4 cm in length is enough for the Gallie wire, which is less than the skin wound resulting from the Harms technique. The tissue trauma and the length of the skin incision were the same as those reported by El Saghir et al.20 Therefore, similar to Elsaghir et al., we call the posterior approach as a “mini-open approach technique”.
In this study, the preoperative CT scans showed that all of the patients studied had anatomic variations of the high-riding vertebral artery, and posterior transarticular screws were evaluated as being difficult to apply and having a higher risk of vertebral artery injury. Therefore, we first performed the atlantoaxial anterior transarticular screw technique on these five patients with a high-riding vertebral artery in the supine position. None of them had complications of vertebral artery injury. Each patient was positioned in the supine position when he or she was first sent into the operation room and for anesthesia. After anesthesia, the atlantoaxial joint was still unstable, the head and neck of the patient were still stabilized, and traction was obtained with Gardner-Wells calipers. If the posterior Magerl or Harms technique were to be performed, the position of the patient would need to be changed at this time. However, percutaneous anterior transarticular screw fixation was performed first, we did not need to change the position of the patient at this time. After anterior transarticular screw fixation was completed, the C1 and C2 vertebrae were stabilized immediately by bilateral anterior transarticular screws. Therefore, it was safer to change the position of the patient at this time. Only one position change of the patient was required with our technique, which is the same as the single posterior position operation of the Harms or Magerl technique.
Moreover, the screw was inserted percutaneously and the technique of percutaneous anterior transarticular screw fixation had the advantages of being safe for the vertebral artery and having less blood loss, less muscular trauma, a smaller skin incision, and a quicker patient recovery time. The disadvantage of this technique was that it could not provide a sufficient bone bed for a graft.8 Therefore, to reach enough fusion, we inserted a mini open Gallie wire posteriorly. We believe that the indications for this technique are the same as those for posterior transarticular screw fixation (the Magerl technique) and the Harms technique. In addition, we recommend applying our technique for patients who are deemed as having anatomic variations such as a high-riding vertebral artery or when posterior transarticular screw fixation is thought to be difficult. We suggest that preoperative CT scans are obtained so that the risk of vertebral artery injury can be evaluated preoperatively.
The limitations of this technique9 are that it is not recommended for some physical characteristics such as considerable cervical kyphosis or concomitant thoracic kyphosis, which may interfere with the fixation of the screws.
Although our technique cannot replace the Magerl and Harms techniques, we suggest that our technique could be an alternative choice for surgeons.
Conclusion
Percutaneous atlantoaxial anterior transarticular screw fixation combined with mini-open posterior C1/2 wire fusion was suitable to patients with a high-riding vertebral artery, and it has the advantages of being safe for the vertebral artery and having less blood loss, less muscular trauma, a smaller skin incision, and a quicker patient recovery time. Therefore, it could be an alternative choice instead of the Magerl and Harms techniques for surgeons.
Disclaimer statements
Contributors Conceiving and designing the study: AMW, XYW, YLC. Obtaining funding and/or ethics approval: AMW, XYW, YLC. Collecting the data: AMW, ZF, HZX. Analysing the data: FZ, XLZ. Interpreting the data: AMW, XYW, HZX. Writing the article in whole or in part: AMW, XYW. Revising the article: all authors.
Funding This work is supported by National Natural Science Foundation of China (81372014, 81371988), Natural Science Foundation of Zhejiang Province for Distinguished Young Scholars (R12H060002), Qianjiang Talents Project of Technology Office of Zhejiang Province (2010R10075). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflicts of interest The authors declare that they have no conflict of interest.
Ethics approval This paper has received ethical approval from the Institutional Review Board of Second Affiliated Hospital of Wenzhou Medical University.
References
- 1.Dickman CA, Sonntag VK. Posterior C1-C2 transarticular screw fixation for atlantoaxial arthrodesis. Neurosurgery 1998;43(2):275–80; discussion 280–1. doi: 10.1097/00006123-199808000-00056 [DOI] [PubMed] [Google Scholar]
- 2.Fuji T, Oda T, Kato Y, Fujita S, Tanaka M. Accuracy of atlantoaxial transarticular screw insertion. Spine (Phila Pa 1976) 2000;25(14):1760–4. doi: 10.1097/00007632-200007150-00004 [DOI] [PubMed] [Google Scholar]
- 3.Weidner A, Wahler M, Chiu ST, Ullrich CG. Modification of C1-C2 transarticular screw fixation by image-guided surgery. Spine (Phila Pa 1976) 2000;25(20):2668–73; discussion 2674. doi: 10.1097/00007632-200010150-00020 [DOI] [PubMed] [Google Scholar]
- 4.Elgafy H, Potluri T, Goel VK, Foster S, Faizan A, Kulkarni N. Biomechanical analysis comparing three C1-C2 transarticular screw salvaging fixation techniques. Spine (Phila Pa 1976) 2010;35(4):378–85. doi: 10.1097/BRS.0b013e3181bc9cb5 [DOI] [PubMed] [Google Scholar]
- 5.Lau SW, Sun LK, Lai R, Luk MS, Ng YS, Wong NM, et al. Study of the anatomical variations of vertebral artery in C2 vertebra with magnetic resonance imaging and its application in the C1-C2 transarticular screw fixation. Spine (Phila Pa 1976) 2010;35(11):1136–43. [DOI] [PubMed] [Google Scholar]
- 6.Lu J, Ebraheim NA, Yang H, Heck BE, Yeasting RA. Anatomic considerations of anterior transarticular screw fixation for atlantoaxial instability. Spine (Phila Pa 1976) 1998;23(11):1229–35; discussion 1236. doi: 10.1097/00007632-199806010-00011 [DOI] [PubMed] [Google Scholar]
- 7.Sen MK, Steffen T, Beckman L, Tsantrizos A, Reindl R, Aebi M. Atlantoaxial fusion using anterior transarticular screw fixation of C1-C2: technical innovation and biomechanical study. Eur Spine J 2005;14(5):512–8. doi: 10.1007/s00586-004-0823-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Xu H, Chi YL, Wang XY, Dou HC, Wang S, Huang YX, et al. Comparison of the anatomic risk for vertebral artery injury associated with percutaneous atlantoaxial anterior and posterior transarticular screws. Spine J 2012;12(8):656–62. doi: 10.1016/j.spinee.2012.05.010 [DOI] [PubMed] [Google Scholar]
- 9.Li WL, Chi YL, Xu HZ, Wang XY, Lin Y, Huang QS, et al. Percutaneous anterior transarticular screw fixation for atlantoaxial instability: a case series. J Bone Joint Surg Br 2010;92(4):545–9. doi: 10.1302/0301-620X.92B4.22790 [DOI] [PubMed] [Google Scholar]
- 10.Brooks AL, Jenkins EB. Atlanto-axial arthrodesis by the wedge compression method. J Bone Joint Surg Am 1978;60(3):279–84. [PubMed] [Google Scholar]
- 11.Holness RO, Huestis WS, Howes WJ, Langille RA. Posterior stabilization with an interlaminar clamp in cervical injuries: technical note and review of the long term experience with the method. Neurosurgery 1984;14(3):318–22. doi: 10.1227/00006123-198403000-00010 [DOI] [PubMed] [Google Scholar]
- 12.Magerl F, Seemann P. Stable posterior fusion at the atlas and axis by transarticular screw fixation. In: Kehr P, Weidner A, editors. Cervical Spine. Vienna, Austria: Spinger-Verlag; 1987. p. 322–327. [Google Scholar]
- 13.Harms J, Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine (Phila Pa 1976) 2001;26(22):2467–71. doi: 10.1097/00007632-200111150-00014 [DOI] [PubMed] [Google Scholar]
- 14.Grob D, Crisco JJ 3rd, Panjabi MM, Wang P, Dvorak J. Biomechanical evaluation of four different posterior atlantoaxial fixation techniques. Spine (Phila Pa 1976) 1992;17(5):480–90. doi: 10.1097/00007632-199205000-00003 [DOI] [PubMed] [Google Scholar]
- 15.Melcher RP, Puttlitz CM, Kleinstueck FS, Lotz JC, Harms J, Bradford DS. Biomechanical testing of posterior atlantoaxial fixation techniques. Spine (Phila Pa 1976) 2002;27(22):2435–40. doi: 10.1097/00007632-200211150-00004 [DOI] [PubMed] [Google Scholar]
- 16.Smith MD, Kotzar G, Yoo J, Bohlman H. A biomechanical analysis of atlantoaxial stabilization methods using a bovine model. C1/C2 fixation analysis. Clin Orthop Relat Res 1993;(290):285–95. [PubMed] [Google Scholar]
- 17.Henriques T, Cunningham BW, Olerud C, Shimamoto N, Lee GA, Larsson S, et al. Biomechanical comparison of five different atlantoaxial posterior fixation techniques. Spine (Phila Pa 1976) 2000;25(22):2877–83. doi: 10.1097/00007632-200011150-00007 [DOI] [PubMed] [Google Scholar]
- 18.Grob D, Jeanneret B, Aebi M, Markwalder TM. Atlanto-axial fusion with transarticular screw fixation. J Bone Joint Surg Br 1991;73(6):972–6. [DOI] [PubMed] [Google Scholar]
- 19.McGuire RA Jr., Harkey HL. Modification of technique and results of atlantoaxial transfacet stabilization. Orthopedics 1995;18(10):1029–32. [DOI] [PubMed] [Google Scholar]
- 20.ElSaghir H, Boehm H, Greiner-Perth R. Mini-open approach combined with percutaneous transarticular screw fixation for C1-C2 fusion. Neurosurg Rev 2005;28(1):59–63. [DOI] [PubMed] [Google Scholar]
- 21.Kaminski A, Gstrein A, Kalicke T, Muhr G, Muller EJ. Mini-open percutaneous transarticular screw fixation for acute and late atlantoaxial instability. Acta Orthop Belg 2008;74(1):102–8. [PubMed] [Google Scholar]
- 22.Schmidt R, Richter M, Gleichsner F, Geiger P, Puhl W, Cakir B. Posterior atlantoaxial three-point fixation: comparison of intraoperative performance between open and percutaneous techniques. Arch Orthop Trauma Surg 2006;126(3):150–6. doi: 10.1007/s00402-005-0046-9 [DOI] [PubMed] [Google Scholar]
- 23.Goel A, Gupta S. Vertebral artery injury with transarticular screws. J Neurosurg 1999;90(2):376–7. [DOI] [PubMed] [Google Scholar]
- 24.Farey ID, Nadkarni S, Smith N. Modified Gallie technique versus transarticular screw fixation in C1-C2 fusion. Clin Orthop Relat Res 1999;(359):126–35. doi: 10.1097/00003086-199902000-00013 [DOI] [PubMed] [Google Scholar]
- 25.Elliott RE, Tanweer O, Boah A, Morsi A, Tracy BA, Frempong-Boadu A, et al. Comparison of screw malposition and vertebral artery injury of C2 pedicle and transarticular screws: meta-analysis and review of the literature. J Spinal Disord Tech 2014;27(6):305–15. doi: 10.1097/BSD.0b013e31825d5daa [DOI] [PubMed] [Google Scholar]
- 26.Neo M, Fujibayashi S, Miyata M, Takemoto M, Nakamura T. Vertebral artery injury during cervical spine surgery: a survey of more than 5600 operations. Spine (Phila Pa 1976) 2008;33(7):779–85. doi: 10.1097/BRS.0b013e31816957a7 [DOI] [PubMed] [Google Scholar]
- 27.Vergara P, Bal JS, Hickman Casey AT, Crockard HA, Choi D. C1-C2 posterior fixation: are 4 screws better than 2? Neurosurgery 2012;71(1 Suppl Operative):86–95. doi: 10.1227/NEU.0b013e31825356f5 [DOI] [PubMed] [Google Scholar]
- 28.Gautschi OP, Payer M, Corniola MV, Smoll NR, Schaller K, Tessitore E. Clinically relevant complications related to posterior atlanto-axial fixation in atlanto-axial instability and their management. Clin Neurol Neurosurg 2014;123:131–5. doi: 10.1016/j.clineuro.2014.05.020 [DOI] [PubMed] [Google Scholar]