

Abstract
Background:
Population based cancer registry is inevitable to measure the indicators of cancer. This retrospective study was conducted to perform the age specific incidence and age standardized rate of cancer by sex, age and sites in Nepal, 2012.
Materials and Methods:
The data collected by hospital based National cancer registry programme of Nepal were used to calculate the age specific incidence of five major cancers by sex and sites. The age standardized rate of ten major cancers, both in males and females of 2012 was also performed.
Results:
The 70-74 years age group had the highest incidence rate (188.08) for men while for women the age group of 65-69 years had the highest incidence (140.61) per 100,000. For male, lung cancer had the highest incidence rate (4.45) whereas bladder had the lowest rate (0.98). Similarly for female, Cervix Uteri cancer had the highest incidence rate (5.35) whereas stomach had the lowest (1.06).
Conclusion:
This study presented that cancer was increased with age both in males and females. The leading cancer in males was bronchus and lung while in females it was cervix uteri. .
Keywords: Cancer; , age specific; , incidence; , Nepal.
Introduction
The profound effect of cancer was alike in both highly developed and less developing countries worldwide. The key factors behind the increase in cancer occurrence were growth and aging of the population, which also incorporated increasing prevalence of established risk factors such as smoking, overweight, physical inactivity, and in association with changing reproductive patterns of urbanization and economic prosperity. According to the estimation of GLOBOCAN, almost 14.1 million new cancer cases and 8.2 million deaths occurred in 2012 globally. The data showed that approximately 57% of cases and 65% of cancer deaths around the globe had accounted [1]. Lung, prostate, colorectal, stomach and liver cancer were the most common cancer among men diagnosed in 2012 while for female breast, colorectal, lung, cervix and stomach were the most common. In Asia, Africa and Central South America, more than 60% of the world’s total new cases of cancer occurred annually. After 20 years, the incidence of cancer was expected to increase by about 70% [2].
The infrastructure of health facilities was very poor in Nepal though the government had announced that health care to be a fundamental right for everyone. The government in Nepal had given the lowest priority for the management of cancer [3]. The number of reports and hospital based studies that had been published very few in Nepal. The only preliminary data on cancer incidence were found from teaching hospital, some cancer hospitals and some general hospitals in different parts of the country. These reports generated valuable information even though they did not provide the national figures. With the help of the World Health Organization (WHO), a new network for cancer registration of cancer data was set up in Nepal in 2005. In the advancement of epidemiological studies of Cancer in Nepal, this registry system brought a new step which made it possible to collect at least some basic cancer data to publish hospital based reports [3].
The goal of this study is to describe the distribution of cancer (age specific incidence and age standardized rate) by age, site and sex in order to provide evidence for the stakeholders to formulate the policy and plan for the prevention and control of cancer. Though few studies was conducted by using the national cancer registry data which only presented the cancer numbers by age [4, 5]. The total crude incidence rate for five major types of cancers for men and women were also different in our study because we had used the 2011 census population of five regions of Nepal to calculate the 2012 population by using the population growth rate of Nepal. The previous study had used the projected population for the denominator to calculate the crude incidence [4]. In 2012, 7212 new cancer cases were registered in seven hospital based cancer registries throughout the Nepal. The number of cancer cases for men was 3291 (45.6%), while for women it was 3921 (54.4%). Among the total cases, 3307 new cancer cases were reported by BP Koirala Memorial Cancer Hospital, Chitwan which was 45.9% of the total cancer cases in 2012. In the same way the Bhaktapur Cancer Hospital reported 1513 (21.0%), Bir Hospital, Kathmandu 950 (13.2%), TU Teaching Hospital Kathmandu 625 (8.7%), BP Koirala Institute of Health Sciences, Dharan 545 (7.6%), Manipal Teaching Hospital, Pokhara 203(2.8%), Kanti Children´s Hospital, Kathmandu 69 (1.0%) [6].
Methodology
The population growth rate from 2001 to 2011 published in population monograph of Nepal volume 1 and the Census population of 2011 was used to predict the 2012 population of Nepal [7]. We had used world standard population in five years interval to adjust the age. World population was taken from Cancer Registration: Principles and methods [8].
Study Design and the Participants
This is a hospital based retrospective study and the number of cases was 7212 in 2012.
Data Collection
This study has retrieved the data from seven hospital-based-cancer registry (B P Koirala Memorial Cancer hospital, Bhaktapur cancer hospital, Bir hospital, TU teaching hospital, Kanti children hospital, BP Koirala institute of health science and Manitpal teaching hospital) in 2012 in Nepal.
Inclusion criteria
All total cases with known age, sex and sites were included in the study.
Exclusion criteria
All double/multiple entry cases were excluded [6].
Explanatory variable
Age and gender were the explanatory variables.
Outcome Variable
Cancer incidence rate by sex and sites were the outcome variable.
Ethical Committee approval
Permission has taken prior to the study from the B.P.Koirala Memorial Cancer Hospital, Nepal.
Data management and statistical analysis:
Cancer cases were categorized as per international classification of disease for oncology (ICD-10) published by the international agency for research on cancer/ world health organization (IARC/WHO). The age specific incidence (ASI per 100,000) was calculated by age, sex, and sites. Age Standardized Rate (ASR) of top ten major cancer sites in both sexes were also performed. For statistical analysis, SPSS (version 23.0) and Microsoft Excel 2010 were used.
Results
Cancer was increased by age (Table 1). From the 45-49 age groups in male, the cancer incidence increased rapidly. The 70-74 age groups had highest cancer incidence (188.08) for men. For female, the cancer incidence increased rapidly from the 30-34 age groups. The age group of 65-69 years had the highest incidence (140.61) for female.
Table 1.
Age specific incidence (ASI) of cancer per 100,000 in both sex in Nepal, 2012
| Age group | Male Population | Male ASI | Female Population | Female ASI | Both sex ASI |
|---|---|---|---|---|---|
| 00-04 | 1332893.63 | 3.38 | 1270235.82 | 2.44 | 2.92 |
| 05-09 | 1657607.30 | 4.65 | 1591052.38 | 1.95 | 3.32 |
| 10-14 | 1788542.12 | 3.47 | 1734111.01 | 3.69 | 3.58 |
| 15-19 | 1462795.54 | 6.22 | 1655478.91 | 3.99 | 5.03 |
| 20-24 | 1058334.91 | 7.46 | 1332113.12 | 6.91 | 7.15 |
| 25-29 | 930230.70 | 10.54 | 1177674.60 | 9.85 | 10.15 |
| 30-34 | 781524.89 | 14.46 | 977694.85 | 14.93 | 14.72 |
| 35-39 | 750811.11 | 14.65 | 875629.55 | 31.75 | 23.86 |
| 40-44 | 669055.19 | 24.06 | 735249.27 | 54.68 | 40.09 |
| 45-49 | 583049.37 | 36.70 | 605754.14 | 76.43 | 56.95 |
| 50-54 | 512654.68 | 61.05 | 505884.03 | 99.03 | 79.92 |
| 55-59 | 418238.16 | 83.68 | 410478.91 | 111.09 | 97.26 |
| 60-64 | 373363.35 | 119.99 | 393558.72 | 104.94 | 112.27 |
| 65-69 | 281569.29 | 145.97 | 280216.69 | 140.61 | 143.29 |
| 70-74 | 202038.95 | 188.08 | 198243.07 | 121.06 | 154.89 |
| 75+ | 221615.06 | 152.97 | 231768.27 | 98.37 | 125.06 |
| Total | 13024324.25 | 25.27 | 13975143.34 | 28.06 | 26.71 |
When comparing male and female, it was seen that the cancer incidence increased earlier for female than for male. From the 0-4 to 25-29 age group, Cancer incidence in male was higher than for female. From the 30-34 to 55-59 age group female had a higher cancer incidence than male. From the 60-64 age groups, male had a higher incidence than female.
Figure 1: Age specific Incidence (ASI) rate of cancer for both sex in Nepal, 2012
Figure 1:
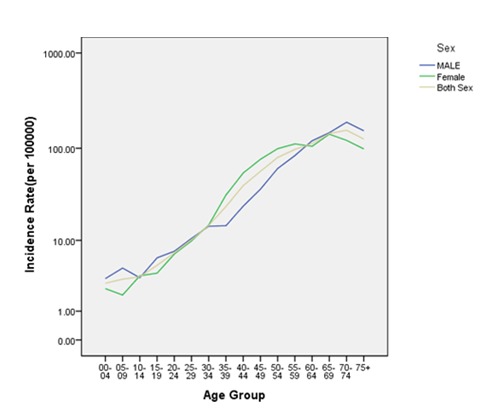
Age specific Incidence (ASI) rate of cancer for both sex in Nepal, 2012
Figure 2: Age specific incidence of five major cancers in males per 100,000 in Nepal, 2012
Figure 2:
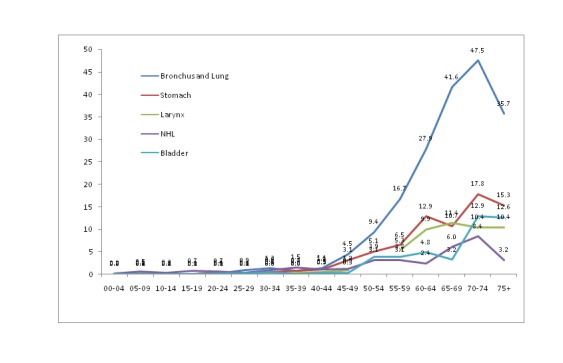
Age specific incidence of five major cancers in males per 100,000 in Nepal, 2012
Lung cancer had the highest incidence (4.45) whereas bladder had the lowest incidence (0.98) per 100,000 in males (Table 2). All cancers had the highest incidence at the age of 70-74. It also demonstrated that cancer was increased with age in males. Table 3 illustrated that the cervix uteri cancer had the highest incidence (5.35) whereas stomach cancer had the lowest incidence (1.06) per 100,000 in females. From the 30-34 age groups the cancer incidence was increased up-to the 55-59 age groups. Cervix Uteri, breast, bronchus and lung and stomach cancers had the highest incidence at the age of 65-69. However, the highest incidence in the ovary was found at the age of 50-54. From the 60-64 age groups, the cancer incidence had a decreasing trend.
Table 2.
Age specific incidence of five major cancers per 100,000 in males in Nepal, 2012
| Age group | Bronchus and Lung | Stomach | Larynx | NHL | Bladder |
|---|---|---|---|---|---|
| 00-04 | 0.00 | 0.00 | 0.00 | 0.15 | 0.00 |
| 05-09 | 0.18 | 0.06 | 0.12 | 0.54 | 0.00 |
| 10-14 | 0.06 | 0.00 | 0.00 | 0.34 | 0.00 |
| 15-19 | 0.07 | 0.00 | 0.07 | 0.68 | 0.00 |
| 20-24 | 0.09 | 0.38 | 0.00 | 0.66 | 0.09 |
| 25-29 | 0.86 | 0.11 | 0.00 | 0.32 | 0.11 |
| 30-34 | 1.28 | 0.38 | 0.00 | 0.90 | 0.51 |
| 35-39 | 0.80 | 0.67 | 0.27 | 1.47 | 0.00 |
| 40-44 | 1.35 | 1.05 | 0.45 | 1.05 | 0.30 |
| 45-49 | 4.46 | 3.09 | 0.86 | 1.20 | 0.34 |
| 50-54 | 9.36 | 5.07 | 4.29 | 3.12 | 3.90 |
| 55-59 | 16.74 | 6.46 | 5.26 | 3.11 | 3.83 |
| 60-64 | 27.85 | 12.86 | 9.91 | 2.41 | 4.82 |
| 65-69 | 41.55 | 10.65 | 11.36 | 6.04 | 3.20 |
| 70-74 | 47.52 | 17.82 | 10.39 | 8.41 | 12.87 |
| 75+ | 35.65 | 15.34 | 10.38 | 3.16 | 12.63 |
| Total | 4.45 | 1.84 | 1.31 | 1.14 | 0.98 |
| NHL:Non Hodgkins Lymphoma | |||||
Table 3.
Age specific incidence of five major cancers per 100,000 in females in Nepal, 2012
| Age group | Cervix Uteri | Breast | Bronchus and Lung | Ovary | Stomach |
|---|---|---|---|---|---|
| 00-04 | 0.16 | 0.00 | 0.00 | 0.00 | 0.00 |
| 05-09 | 0.06 | 0.06 | 0.00 | 0.06 | 0.00 |
| 10-14 | 0.06 | 0.17 | 0.00 | 0.06 | 0.00 |
| 15-19 | 0.18 | 0.18 | 0.06 | 0.79 | 0.00 |
| 20-24 | 0.08 | 0.53 | 0.23 | 0.98 | 0.15 |
| 25-29 | 0.59 | 1.87 | 0.59 | 0.76 | 0.25 |
| 30-34 | 2.35 | 2.56 | 0.20 | 0.92 | 0.72 |
| 35-39 | 5.25 | 8.57 | 0.57 | 2.28 | 1.03 |
| 40-44 | 11.56 | 15.37 | 1.36 | 3.26 | 2.86 |
| 45-49 | 17.66 | 18.65 | 4.13 | 4.95 | 2.31 |
| 50-54 | 24.12 | 16.21 | 9.49 | 8.10 | 3.36 |
| 55-59 | 26.80 | 17.78 | 11.94 | 5.36 | 5.36 |
| 60-64 | 21.60 | 11.43 | 16.52 | 5.34 | 3.56 |
| 65-69 | 27.12 | 12.49 | 28.91 | 6.42 | 8.21 |
| 70-74 | 20.68 | 12.11 | 28.75 | 5.55 | 5.04 |
| 75+ | 15.96 | 8.63 | 19.42 | 2.16 | 2.59 |
| Total | 5.35 | 4.59 | 2.85 | 1.70 | 1.06 |
Figure 3: Age specific incidence of five major cancers in females per 100,000 in Nepal, 2012
Figure 3:
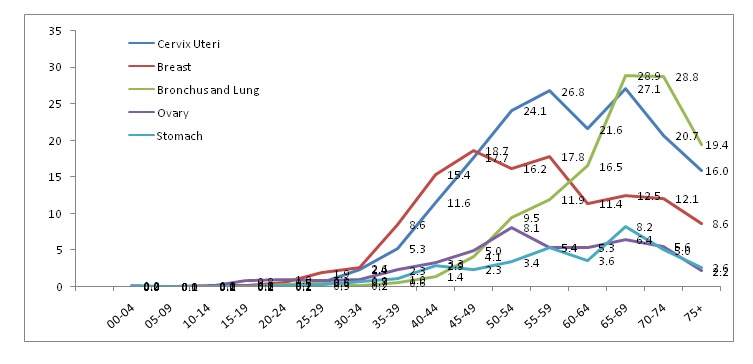
Age specific incidence of five major cancers in females per 100,000 in Nepal, 2012
In males, bronchus and lung cancer had the highest ASR (5.74) while in females the cervix uteri had the highest ASR (7.00) per 100,000 (Table 4).
Table 4.
Age Standardized Rate (ASR) of 10 major cancer sites per 100,000 in males and females in Nepal, 2012
| Male | Female | ||
|---|---|---|---|
| Cancer sites | ASR | Cancer sites | ASR |
| Bronchus and Lung | 5.74 | Cervix Uteri | 7.00 |
| Stomach | 2.36 | Breast | 5.70 |
| Larynx | 1.69 | Bronchus and Lung | 3.89 |
| NHL | 1.29 | Ovary | 2.09 |
| Bladder | 1.23 | Stomach | 1.37 |
| Other and unspecified | 1.21 | Gall bladder | 1.37 |
| Brain | 0.84 | Thyroid | 1.01 |
| Rectum | 0.95 | Other and ill defined sites | 0.76 |
| Other and ill defined sites | 0.88 | Brain | 0.64 |
| Connective Subcutaneous and other soft tissue | 0.73 | Rectum | 0.67 |
| NHL:Non Hodgkins Lymphoma | |||
Discussion
Due to the non-existence of a population based national cancer registry system in Nepal, the exact figures were not clear in terms of cancer epidemiology. Even well-known Comprehensive monograph, Cancer in five continents published by the International Agency for Research on Cancer (WHO), cancer incidence in Nepal was not reported due to data unavailability.
Major Cancers in Male in Nepal, 2012
Lung:
This study found that the Bronchus and lung cancer had the highest incidence (4.45) which was almost three times greater than the second most common cancer stomach in males. The third most common cancer was larynx followed by the NHL. Among five cancer sites, bladder had the lowest incidence rate (0.98). Out of 7212 cases of Nepal in 2012, 17.6% were the lung cancer [4]. Comparison with the previous studies done in Nepal also presented that lung followed by oral cavity; larynx and stomach were the most common types of cancers in male. There were 14.6% lung cancers in men while for female the corresponding percentage was 10.8 out of 4397 cases [5]. Similarly, another study also demonstrated that Lung cancer was the leading cancer followed by larynx, stomach and tongue for male [9]. However, a hospital based retrospective study in Manipal teaching hospital indicated that head and Neck were the most common types of cancers and lung was the second most common cancer for male [10]. Some cases of lung cancer were also observed at lower ages in our study; it could be because of genetic links [11]. In 2012, approximately 1.8 million new lung cancer cases were found, accounting for almost 13% of all cancers diagnosed. As lung cancer was the most commonly diagnosed cancer, it was the major cause of death among males in 2012. The highest lung cancer incidence rates among men were found in Europe, Eastern Asia, and Northern America, and the lowest rates were in sub-Saharan Africa. This study had further reported that the age standardized rate (ASR) of lung cancer per 100,000 in males was 30.00 in less developed areas [1].
Stomach:
In our study, the second most common cancer was stomach (1.84 crude incidences) for male. One previous conducted in Nepal had reported that (7.3%) were stomach cancer out of 7212 cases [4]. Similarly, another former study performed that (7.5%) stomach cancers in male, while the corresponding percentage of females was (4.1%) out of 4397 cases [5]. Some cases of stomach cancer were also found in early ages in our study; it might be because of hereditary [12]. Approximately 951,600 new stomach cancers and 723,100 deaths occurred in 2012. Men were almost two times higher as compared to women in stomach cancer and vary widely worldwide. Overall, incidence rates were highest in Eastern Asia particularly in Korea, Mongolia, Japan, and China, Central and Eastern Europe, and South America whereas the lowest incidence rates were found in most parts of Africa and Northern America. This study had also performed that the age standardized rate (ASR) of stomach cancer per 100,000 in males was 30.00 in less developed areas [1].
Larynx:
This study revealed that larynx was the third most common cancer (1.31 crude incidence) for male. The seven hospital based cancer registry report of Nepal stated that (5.2%) were the larynx cases [4]. Similarly, another previous study conducted in Nepal reported that 3.7% larynx cancers in, male, while the corresponding percentage of females was 1.3% out of 4397 cases [5]. In head and neck region, Laryngeal malignancy was considered as the second most common malignancy worldwide. There were a variety of malignant tumors arising in the larynx. Squamous cell carcinoma was the commonest and accounts for more than 90% of all malignancies. The incidence of laryngeal malignancy was increasing in the developing countries probably due to increased use of alcohol and smoking [13]. In developing countries, Carcinoma of larynx had been reported as the most common primary head and neck cancer), whereas it was the second most common head and neck cancer worldwide [14]. A study by Torre et al (2015) revealed that the age standardized rate (ASR) of larynx cancer per 100,000 in males was 3.5 in less developed areas [1].
Non Hodgkins Lymphoma (NHL):
This study presented that the NHL was the fourth most common cancer (1.14 crude incidence) for male. Out of 7212 cases in Nepal, 4.5% were the NHL [4]. Similarly, finding from multi institution, hospital based cancer incidence showed that 4.6% NHL cancers cases for male while the corresponding percentage for female was 2.3% out of 4397 cases [5]. Data revealed that in 2012, 385,700 new cases of non-Hodgkin lymphoma (NHL) and 199,700 deaths were estimated. The highest incidence rates of NHL was found in more developed areas such as Western and Northern Europe as well as Australia while as Asia and Eastern Europe had the lowest incidence rates. With the exception of some Sub-Saharan areas, in general, Africa had the lowest incidence rate. This study had also presented that the age standardized rate (ASR) of NHL per 100,000 in males was 4.3 in less developed areas [1].
Major Cancers for Female in Nepal, 2012
Cervix cancer
This study found that the Cervix uteri cancer had the highest crude incidence (5.35) which was almost two times greater than the third most common cancer bronchus and lung (2.85) for female .The second most common cancer was breast (4.59) which was almost three times greater than ovary cancer (1.70). The stomach cancer had the lowest incidence (1.06) per 100,000 in females. A recent study had found that out of 7212 cases in Nepal, 19.1% were the cervix uteri [4]. Similarly, another study presented that 21.4% of cervix uteri cancers out of 4397 cases for female [5]. Some studies in Nepal had also indicated that Cervix, breast and lung cancer were the common cancers for female [5, 10]. However, one study conducted in Manipal teaching hospital in Nepal showed that lung cancer was the major cancer for female followed by cervix, breast, stomach and ovary [9]. In 2012, 527,600 new cervical cases and 265,700 deaths were estimated worldwide. Cervical cancer was the second most frequently diagnosed cancer and the third major cause of cancer death among women in less developed countries. The incidence of these cases was found to be highest in sub-Saharan African, Latin America and the Caribbean, and Melanesia whereas the lowest incidence occurred in Western Asia, Australia/New Zealand, and Northern American. Tentatively 90% accounted for cervical cancer deaths in developing countries around the globe: 60,100 deaths in Africa, 144,400 in Asia and 28,600 in Latin America and the Caribbean. As India was the second largest populous country in the world, it alone accounted for 25% of cervical deaths (67,500). Cervical cancer was the leading cause of deaths among women in Eastern, Middle, and Southern Africa including Melanesia. This study had also illustrated that the age standardized rate (ASR) of cervix uteri per 100,000 in females was 15.7 in less developed areas [1].
Breast cancer:
In this study, breast cancer was the second most common cancer for female. The highest incidence rate of breast cancer was in the age of 45-49 (18.65) followed by the 55-59 years group (17.78). A previous study revealed that out of 7212 cases, 16.3% were breast cancers in Nepal [4]. Similarly, another study reported that 15.7% female breast cancer out of 4397 cases [5]. Although breast cancer was the most frequently diagnosed cancer, it was the prime cause of death among the females in worldwide. In 2012, tentatively 1.7 million cases and 521,900 deaths occurred because of cancer. Among women, breast cancer alone was responsible for 25% of all cancer cases and 15% of all cancer deaths. The figure was deadly in more advanced countries comprising about one –half of all breast cancer cases and 38% of deaths. The rates were higher in North America, Australia/New Zealand, and Northern and Western Europe as compared to most of Africa and Asian and intermediate in Central and Eastern Europe. This study had also showed that the age standardized rate (ASR) of breast cancer per 100,000 in females was 31.3 in less developed areas [1].
Lung cancer:
In our study, bronchus and lung cancer was the third most common cancer (2.85 crude incidence) for female. The highest incidence was in the age group 65-69 years (28.91) followed by 70-74 years (28.75). A recent study had found that out of 7212 cases in Nepal, 10.2% were the lung cancer [4]. Similarly, another study reported that 10.8% lung cancer cases for female out of 4397 [5].Lung cancer was also found to be the leading cause of cancer death among women in more developed countries, and the second most common cause of cancer death in less developed countries. In case of women, the highest –lung cancer occurred in Northern and Western Europe, Northern America, Eastern Asia, and Australia/New Zealand. This study had also demonstrated that the age standardized rate (ASR) of lung cancer per 100,000 in females was 11.1 in less developed areas [1].
Cancer and Age in Nepal
Due to not enough publication about the cancer incidence (Crude and ASR) in Nepal, we had compared our result with numbers of cancer cases by age. It was also reported that age is a major determinant of cancer incidence. The incidence of cancer increased dramatically with age [2].Our study found that early and old age of male had a higher incidence than female. However, middle age female had a higher incidence than male. One study performed in Nepal assessed that the age group 55-65 years accounted for about 29.0% of the total cancer cases while the 45-55 years constitute 23.7%. The incidence of cancer was found to be less in children below 15 years of age at 1.9% [15]. Another research conducted in Nepal also illustrated that 37.5% of cancers in male occurred between the ages of 61 to 70 years while for female the corresponding percentage was 28.6% [9].The research performed in Multi-institution hospital, Nepal presented that cancer cases increased by age. The number of cancer cases was highest in the age of 60-64 for male while for female the number was highest in the age of 45-49 [5]. Likewise, another study demonstrated that the most prevalent age group of female was 50-54 years (12.8%), while in male it was 60-64 years (13.6%) [4]. Our study showed that the cancer incidence was high (188.08) at the age of 70-74 for male while for female the incidence was 140.61 at the age of 65-69. Research had shown that breast cancer was the second most common malignancy among women in Nepal. The age group 40-50 years had a higher number of cancer cases than other age groups [16].Our study showed that the age groups with the highest incidence of breast cancer were 40-44 to 55-59. Gynecological cancers were most common in ages between 40 and 60 years with a mean age of 45 years [17]. The maximum frequency (33%) of cases was found in the age group 40 to 49 years [18]. A retrospective study conducted in the Manipal Teaching Hospital, Nepal stated that in total 944 cancer cases, the common age group was between 50-70 years [10]. Our study showed that the cancer incidence rate was also higher in the age groups of 45-49 and 65-69 for female.
Conclusion
Both males and females are highly contracted by the preventable cancer in Nepal. Our finding showed that cancer increases with age, both in males and females. The most common cancers in males were bronchus and lung, stomach and larynx while in females the cervix uteri, breast and bronchus and lung were the most common cancer in 2012.
Limitation of the Study
As this is a hospital based study, the findings of population based cancer registry of other countries cannot be used to compare the incidence of Nepal.
Future Scope of the Study
This study could be useful in cancer epidemiology and cancer statistics to formulate the policy and plan for the prevention and control of cancer in Nepal.
Already known on this topic
A couple of studies had been conducted to show the burden of cancer in Nepal. The previous study had presented only the number of cancer cases by sex and sites.
What this study adds
This study is different from the previous studies in Nepal because it has clearly presented the cancer incidence by age, sex and sites. Furthermore, this study has also performed the age standardized rate of ten major cancers both in males and females.
References
- 1. Brechin S, Bigrigg A., et al. Male and female sterilisation. Current Obstetrics & Gynaecology. 2006; 16:39-46. http://dx.doi.org/10.1016/j.curobgyn.2005.11.002 [Google Scholar]
- 2. WHO Cancer Fact sheet No.297: World Health Organization (February 2015). [Cited 2016 January 10]. Available from: http://www.who.int/mediacentre/factsheets/fs297/en/
- 3. Subedi KS, Sharma P. Cancer treatment in Nepal: A historical background, development of treatment facilities, epidemiology and challenges for prevention and control of cancer. Austral-Asian Journal of Cancer 2012; 11 : 205 - 12. file:///C:/Users/gtl530/Downloads/Cancer%20Treatment%20in%20Nepal-%20A%20Historical%20Background,%20Development%20of%20Treatment%20Facilities,%20Epidemiology%20and%20Challenges%20for%20Prevention%20and%20Control%20of%20Cancer..pdf [Google Scholar]
- 4. Pun CB, Pradhananga KK, Siwakoti B, et al. Malignant Neoplasm Burden in Nepal-Data from the seven major cancer service hospitals for 2012. Asian Pac J Cancer Prev 2015; 16 (18): 8659 - 63. http://dx.doi.org/10.7314/APJCP.2015.16.18.8659 PMid: [DOI] [PubMed] [Google Scholar]
- 5. Pradhananga KK, Baral M, Shrestha BM. Multi-institution hospital-based cancer incidence data for Nepal: an initial report. Asian Pac J Cancer Prev 2009; 10 : 259 - 62. http://www.apocpcontrol.org/paper_file/issue_abs/Volume10_No2/259c_Kishore.pdf PMid: [PubMed] [Google Scholar]
- 6. National Cancer Registry Programme Report of Hospital Based National Cancer Registry 2012. B.P. Koirala Memorial Cancer Hospital cancer prevention, control and research department.. [Google Scholar]
- 7. Population Monograph of Nepal. Population Dynamics, Government of Nepal, National Planning Commission Secretariat, Central Bureau of Statistics 2014. ; I; http://un.org.np/sites/default/files/Population%20Monograph%202014%20Volume%201.pdf [Google Scholar]
- 8. Jensen OM, Parkin DM, Maclennan , Muir CS, et al. Cancer Registration: Principles and Methods, IARC scientific publication 1991; No. 95 https://www.iarc.fr/en/publications/pdfs-online/epi/sp95/SP95.pdf [Google Scholar]
- 9. Binu VS, Chandrashekhar TS, Subba SH, et al. Cancer pattern in western Nepal: A hospital based retrospective study Asian Pac J Cancer Prev 2007; 8 : 183 - 86. http://www.apocpcontrol.org/paper_file/issue_abs/Volume8_No2/183_Binu_4.pdf PMid: [PubMed] [Google Scholar]
- 10. CR Bhatt, K Sharan, J Ninan, et al. Cancer Treatment by Radiotherapy in Western Nepal: A hospital based study. Asian Pac J Cancer Prev 2009; 10 : 205 - 08. http://www.apocpcontrol.org/paper_file/issue_abs/Volume10_No2/205c%20Bhatt%20.pdf PMid: [PubMed] [Google Scholar]
- 11.Lung cancer (small cell). What is small cell lung cancer? [Cited 2016 June 10]. Available from: http://www.cancer.org/acs/groups/cid/documents/webcontent/003116-pdf.pdf.
- 12.Stomach cancer. What is stomach cancer? . [Cited 2016 June 10]. Available from: http://www.cancer.org/acs/groups/cid/documents/webcontent/003141-pdf.pdf.
- 13. Koirala K. Epidemiological study of laryngeal caricinoma in western Nepal. Asian Pac J Cancer Prev 2015; 16 : 6541 - 44. http://www.apocpcontrol.org/paper_file/issue_abs/Volume16_No15/6541-6544%206.20%20Krishna%20Koirala.pdf http://dx.doi.org/10.7314/APJCP.2015.16.15.6541 PMid: [DOI] [PubMed] [Google Scholar]
- 14. Chu EA, Young JK. Laryngeal cancer: diagnosis and preoperative work-up. Otolaryngo Clin N Am 2008; 41 : 673 - 95. http://dx.doi.org/10.1016/j.otc.2008.01.016 PMid: [DOI] [PubMed] [Google Scholar]
- 15. Mishra SR, Neupane D, Bhandari PM, Khanal V, Kallestrup P. Burgeoning burden of non-communicable diseases in Nepal: a scoping review. Globalisation and Health 2015; 10 : 1 - 10. http://dx.doi.org/10.1186/s12992-015-0119-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Singh YP, Sayami Y. Management of Breast Cancer in Nepal. J Nepal Med Assoc 2009; 48 : 252 - 57. PMid: [PubMed] [Google Scholar]
- 17. Dhakal HP, Pradhan M. Histological pattern of Gynecological cancers: J Nepal Med Assoc 2009; 48 : 301 - 05. http://www.ncbi.nlm.nih.gov/pubmed/21105554 PMid: [PubMed] [Google Scholar]
- 18. Jha AK, Jha J, Bista R, et al. A scenario of cervical carinoma in a cancer hospital: J Nepal Med Assoc. 2009; 48 : 199 - 202. http://www.ncbi.nlm.nih.gov/pubmed/20795457 PMid: [PubMed] [Google Scholar]