

Abstract
Duplication cysts occur because of congenital aberration during gut development. They are commonly diagnosed during infancy and rarely during adulthood. We present an adult male who presented to surgical emergency with acute intestinal obstruction. Intraoperatively, this patient was found to have a non-communicating duplication cyst of ileum causing proximal obstruction. The involved segment of the small bowel was resected and a divided loop ileostomy was created.
Background
Duplication cysts may be present from the oesophagus to the anal canal. The reported incidence of an enteric duplication cyst is 1 in 4500 autopsies. Small intestine is the commonest site (44%) of enteric duplication, ileum being the commonest segment.1 2 Duplication cysts of small intestine rarely present as acute abdomen. They are diagnosed most commonly during the infancy but rarely during adulthood. These usually present as mass, pressure effect on adjacent organs, volvulus and obstruction in children. The cysts may be either communicating or non-communicating. The asymptomatic cysts may be complicated by fistulisation, bleeding or even malignant degeneration.3 We present a rare case of ileal non-communicating duplication cyst presenting as acute obstruction in an adult male. The unique entity in adults with this presentation is rarely reported in literature.
Case presentation
A 20-year-old male patient presented to surgical emergency with a history of absolute constipation for 3 days. It was associated with three episodes of bilious vomiting. There was no history of such symptoms. On examination, the patient had tachycardia 112/min, blood pressure of 100/70 mm Hg and dehydration. His abdomen was distended, but no guarding/rigidity. Visible intestinal peristalsis could be appreciated clinically. His hernial orifices were normal and rectum was empty on examination.
Investigations
Abdominal X-ray (figure 1) showed multiple air fluid levels with distended small bowel loops and no colonic air. Ultrasound scan of the abdomen revealed no mass lesion and feature of small bowel obstruction. Contrast-enhanced CT scan was deferred as the patient was in frank obstruction and there was significant risk of aspiration while administering oral contrast.
Figure 1.

Abdominal X-ray showing dilated small bowel loops.
Differential diagnosis
Tuberculosis of small bowel (common in Indian patients)
Hernia (internal)
Adhesions
Meckel's diverticulum with band causing obstruction
Malignancy
Treatment
A nasogastric tube was inserted and 1000 mL of the bilious fluid was drained. The patient was resuscitated and prepared for surgery. A trial of non-operative management was deferred as the patient was in frank obstruction with visible intestinal peristalsis. Intraoperatively, the small bowel was distended and there was a cyst in the small bowel mesentery with a band. The band along with cyst was causing stricture and ileal obstruction. The segmental resection of the ileum was performed with the cyst and bowel exteriorised as stoma due to proximal an oedematous and distended bowel (figure 2). On histopathological examination the cyst wall contained epithelial lining of small bowel with sub mucosa, muscularis mucosa and serosa. There was mild submucosal oedema; focally there was ulceration and transmural necrosis with inflammation extending into the serosa causing serositis. A similar morphology was seen in the Ileal segment (figure 3).
Figure 2.
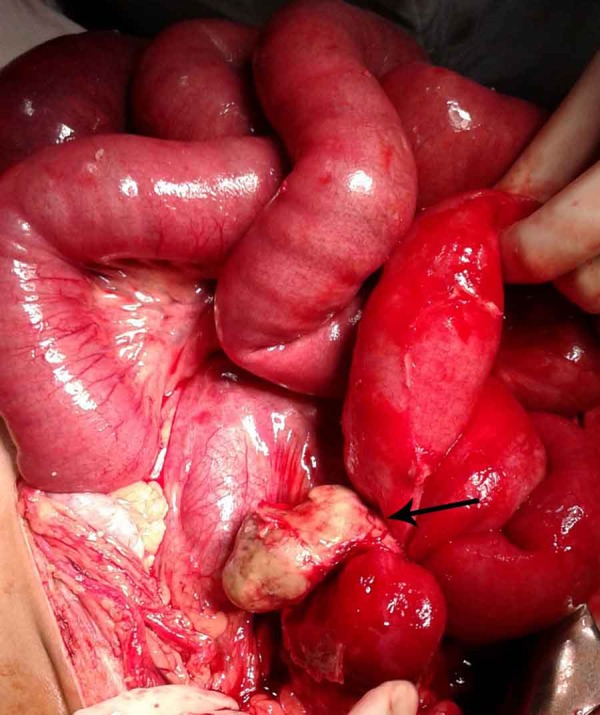
Intraoperative photograph showing the cyst (arrow) with proximal obstruction.
Figure 3.
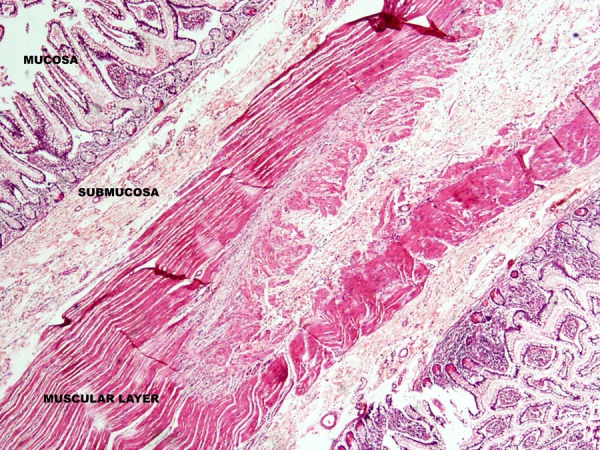
Photomicrograph of the cyst showing all the layers of the small bowel.
Outcome and follow-up
Postoperatively the patient did well and discharged on fifth postoperative day. Thereafter the patient was readmitted and reversal of stoma was performed after 3 months of index surgery.
Discussion
Duplication cysts are a rare cause of intestinal obstruction in adults. They can occur from the foregut to hindgut. These cysts occur in the small bowel most of the times, ileum being the most common site.1 2 These congenital malformations are diagnosed in first 2 years of life in more than 80% of children,4 5 presentation during adulthood is rare (5–6%).4 They may present as asymptomatic mass, obstruction, perforation, intussusception, volvulus or pressure symptoms on adjacent organs.3
Two types of duplication cysts have been described in the literature. Non-communicating or cystic duplications are more common (82%). Communicating or tubular cyst are rare.4 6 Our patient had a non-communicating cyst causing proximal obstruction.
Ileal duplication cysts with obstruction have been rarely reported in adults.7 The diagnostic modalities may be less informative. Ultrasound scan is the preferred modality as it shows the double wall sign. CT/MRI scan can demonstrate the mass but this differential will be considered rarely in adults.5 8 Recently reports of the diagnosis of cysts with endoscopic ultrasound has been published.9 On histological examination the inner wall is lined with columnar epithelium but other types of epithelial lining have also been reported.4 6 Malignant degeneration of the neglected cyst have also been reported. Ileal duplications most commonly turn malignant and present as an advanced stage of cancer.10 11
As the cyst shares its blood supply with the bowel segment, the resection of cysts mandates the resection of the bowel along with the involved mesentery. However, there has been a report of isolated cyst excision in which it was supplied with a separate vascular pedicle.12 13 Primary anastomosis of the resected bowel is the preferred management but in this present case the proximal bowel was grossly distended, oedematous so a stoma was considered safe by the operating surgeons.
Learning points.
Although rare, duplication cysts of bowel can present as acute obstruction in adults.
High index of suspicion is required in countries like India where other causes of ileal obstruction (ie, tuberculosis) are more common.
It should be considered as a differential diagnosis for a young adult presenting with acute intestinal obstruction.
Resection of the cyst along with the involved segment of the bowel offers definitive treatment.
Footnotes
Contributors: AG, KC and BD were involved in writing, editing and gave approval of the manuscript. LK edited and approved the manuscript. LK is the guarantor.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Kim YJ, Kim YK, Jeong YJ et al. Ileal duplication cyst: Y-configuration on in vivo sonography. J Pediatr Surg 2009;44:1462–4. [DOI] [PubMed] [Google Scholar]
- 2.Cheng G, Soboleski D, Daneman A et al. Sonographic pitfalls in the diagnosis of enteric duplication cysts. Am J Roent 2005;184:521–5. [DOI] [PubMed] [Google Scholar]
- 3.Kim SK, Lim LM, Lee SJ et al. Completely isolated enteric duplication cyst: case report. Abdom Imaging 2003;28:12–14. [DOI] [PubMed] [Google Scholar]
- 4.Frering V, Velecela E, Fouque P et al. Upper digestive duplications in adults. Ann Chir 1995;49:928–35. [PubMed] [Google Scholar]
- 5.Fiorani C, Scaramuzzo R, Lazzaro A et al. Intestinal duplication in adulthood: a rare entity, difficult to diagnose. World J Gastrointest Surg 2011;3:128–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abubakar AM, Troebs RB. Gastrointestinal duplications. In: Ameh EA, Bickler SW, Lakhoo K et al., eds Paediatric surgery: a comprehensive text for Africa. Seattle, WA, USA: Global HELP organization; 2011:397–400. [Google Scholar]
- 7.Barbosa L, Soares C, Póvoa AA et al. Ileal duplication: an unusual cause of intestinal obstruction in adult life. BMJ Case Rep 2015;2015:pii: bcr2014206638 doi:10.1136/bcr-2014-206638 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shah A, Du J, Sun Y et al. Dynamic change of intestinal duplication in an adult patient: a case report and literature review. Case Report Med 2012;2012:297585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.R′ıos SS, Noia JL, Nallib IA et al. Adult gastric duplication cyst: diagnosis by endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) . Rev Esp Enferm Dig 2008;100:586–90. [DOI] [PubMed] [Google Scholar]
- 10.Blank G, Königsrainer A, Sipos B et al. Adenocarcinoma arising in a cystic duplication of the small bowel: case report and review of literature. World J Surg Oncol 2012;10:55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beltrán MA, Barría C, Contreras MA et al. Adenocarcinoma and intestinal duplication of the ileum. Report of one case. Rev Med Chil 2009;137:1341–5. [PubMed] [Google Scholar]
- 12.Sinha A, Ojha S, Sarin YK. Completely isolated, noncontiguous duplication cyst. Eur J Pediatr Surg 2006;16:127–9. [DOI] [PubMed] [Google Scholar]
- 13.Srivastava P, Gangopadhyay AN, Kumar V et al. Noncommunicating isolated enteric duplication cyst in childhood. J Pediatr Surg 2009;44: 9–10. [DOI] [PubMed] [Google Scholar]