

Abstract
Aims:
Bronchial asthma constitutes important problem worldwide. This chronic lung disease has detrimental effect in the oral cavity like reduction of salivary secretion, change in salivary composition and pH.
Materials and Methods:
This study was conducted to compare the prevalence of dental caries in asthmatic children and healthy children, and also to evaluate the correlation between the Streptococcus mutans, Lactobacillus and dental caries in both the groups.
Results:
In this study, the mean decayed, missing, filled teeth score of children in the study group was (4.53 ± 3.38) higher than the control group (1.51 ± 1.58) (P < 0.01). The S. mutans count of the study group was (59574.47 ± 28510.67) higher than the control group (19777.78 ± 17899.83) P < 0.01. The Lactobacillus count in study group was (43553.19 ± 58776.96) higher than the control group (8843.84 ± 7982.72) P < 0.01. Subjects using inhaled corticosteroids were more prone to develop dental caries than the control group with odds ratio = 6.26 and 95% confidence interval.
Conclusions:
The dental caries prevalence increases with the usage of β2 agonist and corticosteroid inhalers for the treatment of asthma. Thus in asthmatic children, increase in caries prevalence might be due to the drug treatment and not due to the disease by itself. It can be concluded that asthmatic children have a higher prevalence of dental caries than healthy children. Hence, special oral health care is needed for asthmatic children.
KEY WORDS: Anti-asthmatic drugs, dental caries, Lactobacillus, Streptococcus
Chronic lung diseases especially bronchial asthma constitute important problem worldwide. It is estimated that around 300 million people in the world currently have asthma. With projected increase in population, it is estimated that there may be an additional 100 million persons with asthma by 2015.[1,2] Systemic diseases like bronchial asthma have a detrimental effect in the oral cavity like reduction of salivary secretion, change in salivary composition and pH.
The negative effects induced by dental caries include pain, dysfunction, poor appearance, and speech development problems.[3] Inhaled β2 agonists provide a favorable environment for the growth and multiplication of microorganisms causing dental caries (Streptococcus mutans and Lactobacilli) by decreasing salivary secretion.[4,5] Children who receive β2-agonists have a higher prevalence of dental caries and it increases with the severity of bronchial asthma when compared with healthy controls.[4,5] Various studies have demonstrated conflicting results in the association between asthma and dental caries. Some researchers found no association between dental caries and childhood asthma; whereas some found no association between asthma and increase in caries over time.[6] Ryberg et al. found a positive link between increased incidence of dental caries and regular use of inhaled ß2-agonists for the treatment of asthma. It has been suggested that asthmatics have altered salivary composition and flow rates due to the presence of auto-antibodies to ß2-agonists adrenergic receptors.[7,8,9] This study was conducted to compare asthmatic children and healthy controls with respect to the prevalence of dental caries. In addition, we examined the relationship between the presence of S. mutans, Lactobacillus and occurrence of dental caries in both groups.
Materials and Methods
The present case-control study was conducted in the Department of Paedodontics and Preventive Dentistry, Sree Mookambika Institute of Dental Sciences in association with Sree Mookambika Institute of Medical Sciences, India. Permission to conduct the study was obtained from the Institutional Human Ethical Committee. Fifty-five children aged 6–14 years using a daily combination of inhaled β2 agonist and corticosteroid medication only, for at least 2 years were included as cases in the study. The same number of age-matched healthy controls was also studied. Subjects on antibiotics and orthodontic treatment (fixed/removable) were excluded from the study.
Procedure
Oral examinations were carried out according to the WHO guidelines (WHO, 1997).[10] The investigation was carried out in the morning, between 8 and 11 o’clock. The examinations were performed in a dental chair, under good light using a plane mouth mirror and an explorer.
Assessment of dental caries status
This was recorded using decayed, missing, filled teeth (DMFT) index (Henry Klein, Carrole E Palmer and Knutson JW, 1938) and deft index (Grubbel, 1944). Both cases and controls were examined and screened for DMFT and deft indices, respectively.
Collection of saliva
Un-stimulated whole salivary samples were collected in sterile vials 2 h after any oral or visual exposure to food stuffs. All the salivary samples were collected between 8 and 11 am to avoid any variation in the concentration of the saliva due to circadian rhythm. The study population was asked to pool the saliva in the floor of their oral cavity and spit into a sterile vial immediately.[11] Saliva samples were vortexed and serially diluted in 10-fold steps in 0.05N saline.
Anti-microbial assessment of Streptococcus mutans and Lactobacilli
Aliquots of 100 µl of the appropriate dilutions were cultured into mitis salivarius bacitracin (MSB) agar for the selective isolation and enumeration of S. mutans. The MSB agar plates were incubated anaerobically for 48 h at 37°C.[12] The isolation and enumeration of Lactobacilli was achieved by inoculating the diluted saliva sample (100 µL) onto Rogosa Lactobacillus selection Agar plate and incubating at 37°C for 96 h. Thereafter, the typical colony morphology counts and CFUs were recorded. Lactobacilli and S. mutans were identified and recorded.[13]
Statistical analysis
Data were entered into Microsoft Excel/2000 and later exported to SIGMAPLOT (Systat version 12). Descriptive statistics (mean, standard deviation) were calculated. Independent samples t-test was used to test statistical significance at the 5% level. Odds ratio was calculated to measure the association between exposure and outcome.
Results
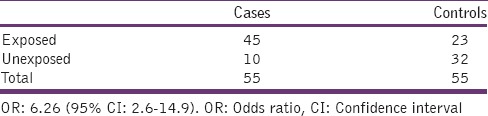
There was a statistically significant difference in the mean DMFT scores of cases (subjects with bronchial asthma) and controls (healthy subjects) (P < 0.001) [Table 1] with a higher value for cases. The mean S. mutans count of cases was significantly higher (P < 0.001) than controls [Table 2]. Similarly, the mean Lactobacillus count of cases were significantly higher (P < 0.001) than controls [Table 3]. Subjects using inhaled corticosteroids were 6.26 times (95% confidence interval 2.6–14.9) more likely to develop dental caries than those who did not [Table 4].
Table 1.
Comparison of mean decayed, missing, filled teeth score of asthmatic group and control group
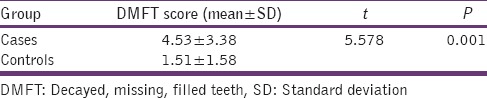
Table 2.
Comparison of mean Streptococcus mutans count in asthmatic and control group

Table 3.
Comparison of mean Lactobacillus count in asthmatic and control group

Table 4.
Odds ratio
Discussion
Oral health-care workers should be adept at recognizing the signs and symptoms of asthma as the prevalence of bronchial asthma is increasing.[14] Bronchial asthma is characterized by decreased β adrenergic reactivity combined with an increased sensitivity to α-adrenergic and cholinergic agonists. The presence of specific autoantibodies to the β2-adrenergic receptor in atopic subjects has been suggested as evidence of autonomic dysfunction.[15,16,17] The various salivary proteins include enzymes, immunoglobulins (IgA, IgG, IgM), mucous, glycoproteins (mucins), albumin (trace), certain polypeptides, and other antibacterial factors of importance in oral health.[18,19] Statherins and proline-rich proteins promote mineralization of enamel by keeping saliva supersaturated with calcium phosphate salts. Metred dose inhalers (MDIs) have a relatively low pH 5.5 and also contain cariogenic sweeteners as carriers. The cariogenic insult is enhanced by frequent, long-term use and faulty use of MDIs.[20,21] β2 agonists and corticosteroids cause a substantial fall in oral pH[22] and a decrease in salivary flow rate.[23] Salivary glands may contain target systems for many drugs like beta-receptors drugs. Salbutamol causes bronchodilation, leading to the production of saliva that is high in protein concentration, but low in volume. Simultaneously, it decreases the amount of reabsorbed water into the salivary ducts.[18,19] One of the main reasons for an increased prevalence of caries in asthmatic children could be the reduced salivary flow coupled with increased levels of Mutans streptococci and Lactobacillus in saliva.[24,25] The decrease in pH of saliva and plaque in asthmatics might be caused by the drug and not the disease.[26] It has been shown that a large proportion of inhaled drug may be retained in the oropharynx. The amount of retained drug could range from 60% (dry powder inhaler with extension tube) to 80% (metered dose inhaler). In addition, some dry powder inhalers contain sugar so that the patient can better tolerate the taste of the drug. Frequent oral inhalation of sugar combined with a decrease in salivary flow rate and a decrease in pH of saliva might contribute to increase in caries.[22]
In this study, the mean DMFT score of cases (4.53 ± 3.38) was higher than controls (1.51 ± 1.58). The S. mutans count of cases (59574.47 ± 28510.67) was higher than controls (19777.78 ± 17899.83). Similarly, the Lactobacillus count in cases (43553.19 ± 58776.96) was higher than controls (8843.84 ± 7982.72). Similar findings have been reported by various investigators.[7,8,25,27,28]
Recently, Shulman et al.[6] questioned the association between caries and asthma, but a direct comparison of that study and the present one is not feasible due to differences in study design.
Although this study did not include the analysis of saliva flow and certain chemical components, it demonstrated a clear association between beta-agonists, salivary changes and dental caries among children. The results of our study support the hypothesis that asthmatic children undergoing treatment with short-acting ß2-agonists may have an increased risk of caries.
Conclusions
This study showed that subjects using daily inhaled corticosteroids for more than 2 years were 6 times more likely to develop dental caries than the control group. The bacteria counts in the saliva of asthmatic children were significantly higher than the control group. These results may be attributed to high xerostomia, low pH drugs with cariogenic sweeteners. Our results suggest inhaled ß2-agonists and corticosteroids could be factors influencing caries development.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Olar M, Luca R, Marica C. Carious experience in children suffering from bronchial asthma. Int J Med Dent. 2012;2:21–6. [Google Scholar]
- 2.Report of the Global Alliance Against Chronic Respiratory Diseases, 5th General Meeting, Toronto, Canada. 2010 Jun 1-2; [Google Scholar]
- 3.Vázquez EM, Vázquez F, Barrientos MC, Córdova JA, Lin D, Beltrán FJ, et al. Association between asthma and dental caries in the primary dentition of Mexican children. World J Pediatr. 2011;7:344–9. doi: 10.1007/s12519-011-0300-x. [DOI] [PubMed] [Google Scholar]
- 4.Shulman JD, Taylor SE, Nunn ME. The association between asthma and dental caries in children and adolescents: A population-based case-control study. Caries Res. 2001;35:240–6. doi: 10.1159/000047464. [DOI] [PubMed] [Google Scholar]
- 5.Wogelius P, Poulsen S, Sørensen HT. Use of asthma-drugs and risk of dental caries among 5 to 7 year old Danish children: A cohort study. Community Dent Health. 2004;21:207–11. [PubMed] [Google Scholar]
- 6.Mazzoleni S, Stellini E, Cavaleri E, Angelova Volponi A, Ferro R, Fochesato Colombani S. Dental caries in children with asthma undergoing treatment with short-acting beta2-agonists. Eur J Paediatr Dent. 2008;9:132–8. [PubMed] [Google Scholar]
- 7.Ryberg M, Möller C, Ericson T. Effect of beta 2-adrenoceptor agonists on saliva proteins and dental caries in asthmatic children. J Dent Res. 1987;66:1404–6. doi: 10.1177/00220345870660082401. [DOI] [PubMed] [Google Scholar]
- 8.Ryberg M, Möller C, Ericson T. Saliva composition in asthmatic patients after treatment with two dose levels of a beta 2-adrenoceptor agonist. Arch Oral Biol. 1990;35:945–8. doi: 10.1016/0003-9969(90)90013-z. [DOI] [PubMed] [Google Scholar]
- 9.Ryberg M, Möller C, Ericson T. Saliva composition and caries development in asthmatic patients treated with beta 2-adrenoceptor agonists: A 4-year follow-up study. Scand J Dent Res. 1991;99:212–8. doi: 10.1111/j.1600-0722.1991.tb01887.x. [DOI] [PubMed] [Google Scholar]
- 10.World Health Organization. Oral Health Survey Basic Method. 4th ed. Geneva: World Health Organization; 1997. [Google Scholar]
- 11.Shifa S, Muthu MS, Amarlal D, Rathna Prabhu V. Quantitative assessment of IgA levels in the unstimulated whole saliva of caries-free and caries-active children. J Indian Soc Pedod Prev Dent. 2008;26:158–61. doi: 10.4103/0970-4388.44031. [DOI] [PubMed] [Google Scholar]
- 12.Gamboa F, Estupinan M, Galindo A. Presence of Streptococcus mutans in saliva and its relationship with dental caries; Antimicrobial susceptibility of the isolates. Universitas Scientiarum. 2004;9:23–7. [Google Scholar]
- 13.Hegde PP, Ashok Kumar BR, Ankola VA. Dental caries experience and salivary levels of Streptococcus mutans and lactobacilli in 13-15 years old children of Belgaum city, Karnataka. J Indian Soc Pedod Prev Dent. 2005;23:23–6. doi: 10.4103/0970-4388.16022. [DOI] [PubMed] [Google Scholar]
- 14.Steinbacher DM, Glick M. The dental patient with asthma.An update and oral health considerations. J Am Dent Assoc. 2001;132:1229–39. doi: 10.14219/jada.archive.2001.0365. [DOI] [PubMed] [Google Scholar]
- 15.Szentivanyi A. The radioligand binding approach in the study of lymphocytic adrenoceptors and the constitutional basis of atopy. J Allergy Clin Immunol. 1980;65:5–11. doi: 10.1016/0091-6749(80)90170-0. [DOI] [PubMed] [Google Scholar]
- 16.Venter JC, Fraser CM, Harrison LC. Autoantibodies to beta 2-adrenergic receptors: A possible cause of adrenergic hyporesponsiveness in allergic rhinitis and asthma. Science. 1980;207:1361–3. doi: 10.1126/science.6153472. [DOI] [PubMed] [Google Scholar]
- 17.Venter JC, Fraser CM, Harrison LC, Kaliner M. Autoantibodies to β 2-adrenergic receptors correlate with autonomic nervous system abnormalities. Fed Proc. 1981;40:355. [Google Scholar]
- 18.Al-Sandook TA, Al-Mashhadane FA, Taqa A. Salivary protein components and oral health in patients undergoing therapy with beta adrenegic agonist and antagonist. Al Rafidain Dent J. 2008;8:219–24. [Google Scholar]
- 19.Thomas MS, Parolia A, Kundabala M, Vikram M. Asthma and oral health: A review. Aust Dent J. 2010;55:128–33. doi: 10.1111/j.1834-7819.2010.01226.x. [DOI] [PubMed] [Google Scholar]
- 20.Milano M, Lee JY, Donovan K, Chen JW. A cross-sectional study of medication-related factors and caries experience in asthmatic children. Pediatr Dent. 2006;28:415–9. [PubMed] [Google Scholar]
- 21.Maupomé G, Shulman JD, Medina-Solis CE, Ladeinde O. Is there a relationship between asthma and dental caries.: A critical review of the literature? J Am Dent Assoc. 2010;141:1061–74. doi: 10.14219/jada.archive.2010.0335. [DOI] [PubMed] [Google Scholar]
- 22.Kargul B, Tanboga I, Ergeneli S, Karakoc F, Dagli E. Inhaler medicament effects on saliva and plaque pH in asthmatic children. J Clin Pediatr Dent. 1998;22:137–40. [PubMed] [Google Scholar]
- 23.Jain M, Mathur A, Sawla L, Nihlani T, Gupta S, Prabu D, et al. Prevalence of dental erosion among asthmatic patients in India. Rev ClíPesqui Odontol. 2009;5:247–54. [Google Scholar]
- 24.Sivasithamparam K, Young WG, Jirattanasopa V, Priest J, Khan F, Harbrow D, et al. Dental erosion in asthma: A case-control study from south east Queensland. Aust Dent J. 2002;47:298–303. doi: 10.1111/j.1834-7819.2002.tb00541.x. [DOI] [PubMed] [Google Scholar]
- 25.Stensson M, Wendt LK, Koch G, Oldaeus G, Birkhed D. Oral health in preschool children with asthma. Int J Paediatr Dent. 2008;18:243–50. doi: 10.1111/j.1365-263X.2008.00921.x. [DOI] [PubMed] [Google Scholar]
- 26.Conolly ME, Greenacre JK. The lymphocyte beta-adrenoceptor in normal subjects and patients with bronchial asthma: The effect of different forms of treatment on receptor function. J Clin Invest. 1976;58:1307–16. doi: 10.1172/JCI108586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McDerra EJ, Pollard MA, Curzon ME. The dental status of asthmatic British school children. Pediatr Dent. 1998;20:281–7. [PubMed] [Google Scholar]
- 28.Shashikiran ND, Reddy VV, Raju PK. Effect of antiasthmatic medication on dental disease: Dental caries and periodontal disease. J Indian Soc Pedod Prev Dent. 2007;25:65–8. doi: 10.4103/0970-4388.33450. [DOI] [PubMed] [Google Scholar]