

Abstract
Objective:
To describe detailed MRI results from 2 head-to-head phase III trials, Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis Study I (CARE-MS I; NCT00530348) and Study II (CARE-MS II; NCT00548405), of alemtuzumab vs subcutaneous interferon β-1a (SC IFN-β-1a) in patients with active relapsing-remitting multiple sclerosis (RRMS).
Methods:
The impact of alemtuzumab 12 mg vs SC IFN-β-1a 44 μg on MRI measures was evaluated in patients with RRMS who were treatment-naive (CARE-MS I) or who had an inadequate response, defined as at least one relapse, to prior therapy (CARE-MS II).
Results:
Both treatments prevented T2-hyperintense lesion volume increases from baseline. Alemtuzumab was more effective than SC IFN-β-1a on most lesion-based endpoints in both studies (p < 0.05), including decreased risk of new/enlarging T2 lesions over 2 years and gadolinium-enhancing lesions at year 2. Reduced risk of new T1 lesions (p < 0.0001) and gadolinium-enhancing lesion conversion to T1-hypointense black holes (p = 0.0078) were observed with alemtuzumab vs SC IFN-β-1a in CARE-MS II. Alemtuzumab slowed brain volume loss over 2 years in CARE-MS I (p < 0.0001) and II (p = 0.012) vs SC IFN-β-1a.
Conclusions:
Alemtuzumab demonstrated greater efficacy than SC IFN-β-1a on MRI endpoints in active RRMS. The superiority of alemtuzumab was more prominent during the second year of both studies. These findings complement the superior clinical efficacy of alemtuzumab over SC IFN-β-1a in RRMS.
ClinicalTrials.gov identifier:
NCT00530348 and NCT00548405.
Classification of evidence:
The results reported here provide Class I evidence that, for patients with active RRMS, alemtuzumab is superior to SC IFN-β-1a on multiple MRI endpoints.
MRI plays a central role in the diagnosis and management of multiple sclerosis (MS)1,2 and provides mechanistic insights into the clinical efficacy of disease-modifying therapies. Meta-analyses show a correlation between the effects of pharmacotherapies on MRI, relapse rate,3,4 and disability.5 Accordingly, MRI assessments are commonly included as efficacy endpoints in MS clinical trials.6 MRI of MS patients visualizes inflammatory brain white matter lesions7 and resulting tissue injury/edema8 and enables indirect detection of the tissue damage and diffuse degenerative processes that contribute to progressive brain atrophy.8
Alemtuzumab (LEMTRADA; Sanofi Genzyme, Cambridge, MA), a humanized anti-CD52 monoclonal antibody approved in many countries for the treatment of active relapsing-remitting MS (RRMS),9–11 was evaluated in 2 phase III trials in active RRMS (Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis Study I [CARE-MS I], treatment-naive patients; and Study II [CARE-MS II], patients with an inadequate response, defined as one or more relapse, to prior therapy). The most common adverse events with alemtuzumab were mild to moderate infusion-associated reactions. Other adverse events included infections and autoimmune disorders.12,13
Despite subcutaneous interferon β-1a (SC IFN-β-1a; Rebif; EMD Serono Inc, Rockland, MA) suppressing focal inflammatory activity on MRI by ≈80%,14 superior benefit was observed in both CARE-MS studies for alemtuzumab compared with SC IFN-β-1a regarding the percentage of patients free of MRI disease activity and reduction in brain volume loss. Here, we report additional MRI outcomes for these 2 trials, including analyses of lesion numbers, risk of new lesions, and brain atrophy by year.
METHODS
Standard protocol approvals, registrations, and patient consents.
The CARE-MS I (ClinicalTrials.gov number NCT00530348) and CARE-MS II (ClinicalTrials.gov number NCT00548405) trials were carried out in accordance with the International Conference on Harmonization Good Clinical Practice guidelines, applicable domestic and international regulations, including US 21 Code of Federal Regulations part 312 (Investigational New Drug Application) and parts 50 and 56 (concerning informed consent and institutional review board regulations), and clinical research guidelines established by the principles defined in the World Medical Association’s Declaration of Helsinki and its amendments. Accordingly, approval was received from an ethical standards committee in human experimentation, and all patients gave written informed consent before participating in the studies.
Study design.
Trial designs, published in detail elsewhere,12,13 are summarized briefly here. The CARE-MS program consisted of 2 phase III, randomized, 2-year, rater-blinded, active-controlled, head-to-head trials of alemtuzumab vs SC IFN-β-1a in patients with RRMS who were treatment-naive (CARE-MS I) or had an inadequate response (one or more relapse after ≥6 months of treatment) to prior therapy (CARE-MS II).12,13 Patients were randomized 2:1 to receive alemtuzumab 12 mg/d IV on 5 consecutive days at baseline and on 3 consecutive days 12 months later or SC IFN-β-1a 44 μg 3 times weekly. Coprimary endpoints were relapse rate and time to 6-month sustained accumulation of disability. In CARE-MS II, IFN-β-1a–neutralizing antibodies were assayed at baseline and 24 months with a cytopathic effect inhibition assay (BioMonitor, Copenhagen, Denmark).
Study outcomes.
This analysis aimed to determine whether superior outcomes (clinical and top-line MRI) observed with alemtuzumab vs SC IFN-β-1a in the CARE-MS studies were also observed for secondary and tertiary MRI measures from these studies. The results reported here provide Class I evidence that, for patients with active RRMS, alemtuzumab is superior to SC IFN-β-1a on multiple MRI endpoints. The results represent Class I evidence because of several elements of the study design. Randomization was stratified by clinical site. Furthermore, masked raters were used for study assessments related to key efficacy endpoints.
MRI protocol.
MRI scans were obtained at baseline and annually. CARE-MS II patients had at least a 30-day washout from prior IFN-β or glatiramer acetate before baseline MRI. Baseline and posttreatment scans were analyzed at NeuroRx Research (Montreal, QC, Canada; lesion analyses) and the Cleveland Clinic MS MRI Analysis Center (Cleveland, OH; brain parenchymal fraction [BPF]) by experts masked to treatment-group assignment.
T1-weighted pre– and post–gadolinium contrast, T2-weighted and proton density (dual-echo) precontrast, fluid-attenuated inversion recovery precontrast, and 3-dimensional gradient-echo, postcontrast MRI sequences were performed before methylprednisolone administration. These data enabled comprehensive analyses of T2, T1, and gadolinium-enhancing lesions and brain atrophy.
Percentage change in T2 lesion volume was a secondary endpoint. Tertiary MRI endpoints included new/enlarging T2, new T1 and gadolinium-enhancing lesion counts, percentage change in T1 lesion volume, proportion of patients free from MRI disease activity (absence of new gadolinium-enhancing and new/enlarging T2 lesions), percentage of gadolinium-enhancing lesions evolving to chronic T1 lesions (black holes), and brain atrophy.
T2-weighted lesions were segmented15 and manually corrected as necessary. T1 lesions were segmented within T2-weighted lesions with the use of a threshold of 85% of the intensity of surrounding normal-appearing white matter. Regions of acute T1 hypointensity associated with gadolinium enhancement were not counted in the analysis. New lesion counts were made relative to the prior visit and added over time intervals as appropriate. Brain volume loss was measured with the BPF metric, calculated from proton density/T2-weighted dual-echo images with brain segmentation software developed at the Cleveland Clinic.16
Statistical analysis.
Percentage changes from baseline to year 2, years 1 to 2, and baseline to year 1 in T2 and T1 lesion volume and BPF were analyzed with the ranked analysis of covariance with adjustment for baseline value and geographic region.
Lesion counts were analyzed through negative binomial regression with robust standard error estimation and adjustment for baseline count and geographic region. Gadolinium-enhancing, T1, and T2 lesion activity, defined as any new lesion first appearing at the specified time point, was analyzed with logistic regression.
Odds of MRI disease activity at any postbaseline visit were analyzed through logistic regression with adjustment for baseline gadolinium-enhancing lesion count and geographic region.
Odds of gadolinium-enhancing lesions evolving to black holes were analyzed with a marginal logistic model fit through generalized estimating equations with a compound symmetric working correlation matrix, robust variance estimation, and adjustment for geographic region. Reported p values are nominal and not adjusted for multiple comparisons.
RESULTS
Patients.
The studies included 1,248 patients with RRMS. In total, 386 treatment-naive (CARE-MS I) patients were randomized to alemtuzumab (376 were treated) and 195 to SC IFN-β-1a (187 treated). Among patients with inadequate response to prior therapy (CARE-MS II), 436 were randomized to alemtuzumab (426 treated) and 231 to SC IFN-β-1a (202 treated).12,13
Baseline demographic and disease characteristics were consistent with active RRMS and similar between treatment arms (table 1). CARE-MS II patients had longer disease duration (per protocol, up to 10 years vs 5 years in CARE-MS I) and higher baseline Expanded Disability Status Scale scores (per protocol, up to 5.0 vs 3.0 in CARE-MS I). The average duration of prior disease-modifying therapy for CARE-MS II patients was 35 months.
Table 1.
Baseline demographic and disease characteristics

Scans analyzed.
In CARE-MS I, depending on the MRI metric, analyzable scans were available for 98.4% to 98.8% of patients at baseline, 96.4% to 97.0% at year 1, and 93.3% to 96.6% at year 2. Values for CARE-MS II were as follows: 98.2% to 99.2% at baseline, 95.7% to 97.0% at year 1, and 91.7% to 96.6% at year 2. In cases with missing data, the main reason for not performing the scan was withdrawal from the study (2.3% in CARE-MS I and 4.0% in CARE-MS II).
Inflammatory lesion activity.
The risk of developing new/enlarging T2 lesions was significantly lower with alemtuzumab vs SC IFN-β-1a over the 2-year study period and in year 2 for CARE-MS I patients (risk reduction 34%, odds ratio 0.66, 95% confidence interval [CI] 0.45–0.97; and risk reduction 57%, odds ratio 0.43, 95% CI 0.29–0.64, respectively, both p < 0.05, figure 1A and table e-1 at neurology.org) and for CARE-MS II patients (risk reduction 62%, odds ratio 0.38, 95% CI 0.26–0.55; and risk reduction 73%, odds ratio 0.27, 95% CI 0.19–0.39, both p < 0.0001, figure 2A and table e-1). Risk of T2 lesions also decreased significantly in year 1 in CARE-MS II patients (risk reduction 53%, odds ratio 0.47, 95% CI 0.33–0.68, p < 0.0001).
Figure 1. Percentage of CARE-MS I patients free from lesion activity and overall MRI disease activity.

Percentage of patients free from (A) new/enlarging T2-hyperintense lesions, (B) gadolinium (Gd)-enhancing lesions, and (C) new T1-hypointense lesions and (D) free from MRI disease activity. Freedom from MRI disease activity defined as the absence of new Gd-enhancing lesions and new/enlarging T2-hyperintense lesions. CARE-MS = Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis; CI = confidence interval; NS = no significant difference; SC IFN-β-1a = subcutaneous interferon β-1a. *p < 0.05; **p ≤ 0.0001.
Figure 2. Percentage of CARE-MS II patients free from lesion activity and overall MRI disease activity.

Percentage of patients free from (A) new/enlarging T2-hyperintense lesions, (B) gadolinium (Gd)-enhancing lesions, and (C) new T1-hypointense lesions and (D) free from MRI disease activity. Freedom from MRI disease activity defined as the absence of new Gd-enhancing lesions and new/enlarging T2-hyperintense lesions. CARE-MS = Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis; CI = confidence interval; SC IFN-β-1a = subcutaneous interferon β-1a. *p < 0.05; **p ≤ 0.0001.
Alemtuzumab was also superior to SC IFN-β-1a with respect to the cumulative number of new/enlarging T2 lesions. In CARE-MS I patients, the mean number of T2 lesions significantly decreased with alemtuzumab vs SC IFN-β-1a over the 2-year study period (mean count 2.3 [SD 6.1] vs 3.2 [SD 5.3]) and in year 2 (0.7 [SD 2.6] vs 1.6 [SD 3.8], both p < 0.05). Among CARE-MS II patients, significant reductions were also observed with alemtuzumab over the 2-year period (3.6 [SD 11.8] vs 8.4 [SD 17.5], p < 0.0001), in year 1 (2.2 [SD 7.6] vs 4.3 [SD 9.8], p < 0.05), and in year 2 (1.4 [SD 5.8] vs 4.1 [SD 9.1], p < 0.0001).
Both treatments were effective in reducing the formation of gadolinium-enhancing lesions (figures 1B and 2B) compared with baseline (table 1). At year 2, the risk of gadolinium-enhancing lesions was significantly reduced with alemtuzumab vs SC IFN-β-1a for both CARE-MS I and CARE-MS II (risk reduction 70%, odds ratio 0.30, 95% CI 0.17–0.53; and risk reduction 69%, odds ratio 0.31, 95% CI 0.19–0.51, both p < 0.0001), as was the mean number of gadolinium-enhancing lesions (mean count 0.2 [SD 0.8] vs 0.3 [SD 1.0] and 0.3 [SD 1.5] vs 1.1 [SD 4.1], respectively, both p < 0.05). At year 1, significantly more alemtuzumab-treated than SC IFN-β-1a–treated patients were free from gadolinium-enhancing lesions in CARE-MS II (85.9% vs 76.8%, p = 0.0036, figure 2B).
Further subgroup analyses of CARE-MS II patients showed that the reduced risk of T2 lesions and gadolinium-enhancing lesions with alemtuzumab vs SC IFN-β-1a was statistically significant regardless of prior SC IFN-β-1a treatment or the presence/absence of baseline IFN-β-1a–neutralizing antibodies (figures e-1 and e-2).
T2-hyperintense lesion volume.
Both treatments led to initial reductions from baseline in median T2 lesion volumes (figure 3, A and B). The largest reductions were seen in CARE-MS I during year 1, after initiation of alemtuzumab or SC IFN-β-1a treatment (figure 3A). This effect was significantly greater for alemtuzumab vs SC IFN-β-1a in year 2 (p = 0.0364), reflecting a further reduction in mean (−0.9%) and median (−1.8%, figure 3A) T2 lesion volumes in alemtuzumab-treated patients compared with SC IFN-β-1a–treated patients, in whom mean T2 lesion volume increased (3.0%) and median T2 lesion volume was unchanged. In CARE-MS II, T2 lesion volume changed minimally over the 2-year study in all patients; however, a significant between-treatment difference in favor of alemtuzumab was observed in year 2 (p = 0.0261, figure 3B).
Figure 3. Median percentage change in T2-hyperintense and T1-hypointense lesion volume in CARE-MS I and CARE-MS II.

Median percentage change from baseline in T2-hyperintense lesion volume in (A) CARE-MS I and (B) CARE-MS II. Median percentage change from baseline in T1-hypointense lesion volume in (C) CARE-MS I and (D) CARE-MS II. CARE-MS = Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis; NS = no significant difference; SC IFN-β-1a = subcutaneous interferon β-1a. *p < 0.05.
New T1-hypointense lesions.
The risk of developing new T1-hypointense lesions was significantly lower with alemtuzumab compared with SC IFN-β-1a in year 1 (51% reduction, odds ratio 0.49, 95% CI 0.32–0.74), in year 2 (79% reduction, odds ratio 0.21, 95% CI 0.13–0.36), and over the 2-year study period (63% reduction, odds ratio 0.37, 95% CI 0.25–0.55, all p < 0.001, figure 2C) for CARE-MS II patients and in year 2 for CARE-MS I patients (67% reduction, odds ratio 0.33, 95% CI 0.19–0.58, p = 0.0001, figure 1C). A significantly greater reduction in T1 lesion volume was observed with alemtuzumab vs SC IFN-β-1a in year 1 and over the 2-year study period in CARE-MS I (both p < 0.05, figure 3C). In year 2, an increase in T1 lesion volume was observed in year 2 with SC IFN-β-1a but not with alemtuzumab (p < 0.05). In CARE-MS II, T1 lesion volume increased in year 1 with SC IFN-β-1a but not with alemtuzumab (p < 0.05, figure 3D).
Conversion to black holes.
Gadolinium-enhancing lesions that formed in year 1 were significantly less likely to evolve into chronic black holes by year 2 in alemtuzumab-treated patients in CARE-MS II compared with those receiving SC IFN-β-1a (67% risk reduction, p = 0.0078). No significant reduction in black hole conversion in year 2 was observed in alemtuzumab-treated patients compared with SC IFN-β-1a–treated patients in CARE-MS I (45%, p = 0.1389). No difference was seen for lesions measured at year 1 that formed before treatment and were enhancing at baseline.
Brain parenchymal fraction.
Alemtuzumab significantly reduced brain volume loss compared with SC IFN-β-1a in CARE-MS I patients (figure 4A) during year 1 (−0.59% vs −0.94%, p < 0.0001) and year 2 (−0.25% vs −0.50%, p = 0.0052) and over the 2-year study period (−0.87% vs −1.49%, p < 0.0001). CARE-MS II patients similarly had less brain volume loss during year 1 (−0.47% vs −0.54%) and year 2 (−0.22% vs −0.35%) after alemtuzumab (figure 4B), although the reduction was statistically significant only over the 2-year study period (−0.62% vs −0.81%, p = 0.012).
Figure 4. Median percentage change in brain parenchymal fraction in (A) CARE-MS I and (B) CARE-MS II.
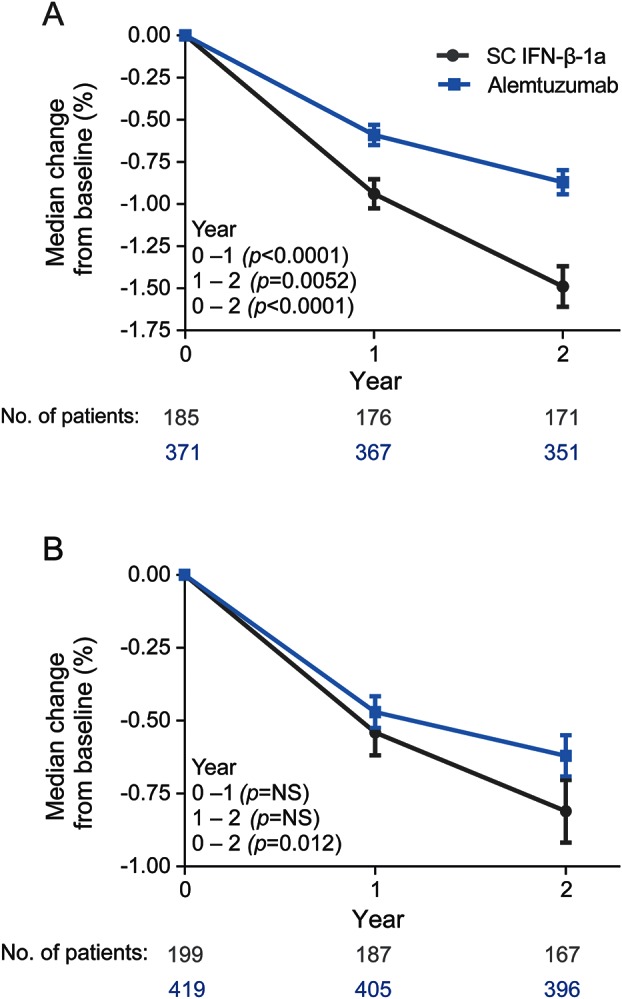
Data are shown as medians with standard error bars; p values are for the comparison of alemtuzumab with SC IFN-β-1a over the time period shown. CARE-MS = Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis; NS = no significant difference; SC IFN-β-1a = subcutaneous interferon β-1a.
Freedom from MRI disease activity.
Alemtuzumab significantly increased the percentage of treatment-naive patients free from MRI disease activity vs SC IFN-β-1a during year 2 (p < 0.0001) and over the entire course of CARE-MS I (p = 0.0388, figure 1D). In CARE-MS II, alemtuzumab significantly increased the percentage of MRI disease activity–free patients vs SC IFN-β-1a during year 1 (p = 0.0001), during year 2 (p < 0.0001), and over the 2-year study period (p < 0.0001, figure 2D).
DISCUSSION
The CARE-MS I and II studies in patients with active RRMS who were treatment-naive or who had an inadequate response to prior therapy, respectively, met the clinical efficacy objective of demonstrating a statistically significant treatment effect of alemtuzumab compared with the active comparator SC IFN-β-1a for at least one coprimary efficacy endpoint (annualized relapse rate or 6-month sustained accumulation of disability), as previously reported.12,13 We report here that the treatment effects of alemtuzumab also surpassed the well-established benefits of SC IFN-β-1a on many MRI endpoints, providing complementary evidence for the observed clinical efficacy of alemtuzumab in patients with RRMS.
Marked benefits of alemtuzumab beyond those of SC IFN-β-1a during the first year of study were observed in one or both of the CARE-MS studies for many MRI outcomes. After 2 years, the benefits of alemtuzumab vs SC IFN-β-1a were even more apparent, with significantly better outcomes emerging both in treatment-naive patients and in those with an inadequate response to prior therapy for all MRI markers of focal inflammatory disease, including T2-hyperintense lesion volume, cumulative number and overall risk of developing new/enlarging T2- and gadolinium-enhancing lesions, risk of developing new T1 lesions, and percentage of patients free from MRI disease activity. Because alemtuzumab-treated patients received a second course at the beginning of the second year of the study (corresponding to a full course of therapy for the treatment of active RRMS), the second alemtuzumab course appears to have contributed to the overall degree of efficacy seen at 2 years and beyond in these and previous studies17,18 and may further increase the effect on core disease mechanisms and hence longer-term clinical outcome.
T2-hyperintense lesion volume is an MRI marker of MS disease burden. In the absence of effective MS therapy, the volume of T2 lesions typically increases over time. For example, in the pivotal trial of SC IFN-β-1a, the placebo group had a 10% increase in T2 lesion volume over 2 years, and the efficacy of SC IFN-β-1a was demonstrated by an ≈4% reduction in lesion volume.14 T2 lesion volume changes may be less easily interpreted in an active comparator trial. In a 1-year study of fingolimod (1.25 or 0.5 mg daily) vs intramuscular IFN-β-1a, changes in T2 lesion volume did not differ significantly between treatment groups19 even though both therapies have shown efficacy on this measure in placebo-controlled trials.20,21 Similarly, in the CARE-MS studies, there was no difference between treatments in T2 lesion volume change over 2 years (a secondary endpoint), but the initial reductions in T2 lesion volume with either treatment compared to baseline represent a positive outcome that likely reflects the effectiveness of both alemtuzumab and SC IFN-β-1a. Finally, although the year 1 T2 volume results were dominated by resolution of preexisting T2 lesions, a significant difference between treatments emerged in year 2 in both studies, again suggesting potential benefit of the second alemtuzumab treatment course and resulting in durable effectiveness of alemtuzumab compared with SC IFN-β-1a in preventing new lesion formation.
The superiority of alemtuzumab vs SC IFN-β-1a in suppressing new MS lesion formation was also apparent in the reduced risk of developing T2- and gadolinium-enhancing brain lesions in both CARE-MS studies. Furthermore, subgroup analyses of CARE-MS II patients showed that the reduction in risk of T2- and gadolinium-enhancing lesions with alemtuzumab vs SC IFN-β-1a was observed regardless of prior SC IFN-β-1a use or baseline IFN-β-1a–neutralizing antibody status.
In both CARE-MS studies, alemtuzumab had a beneficial impact on MRI outcomes that have been linked to disability progression. Brain volume loss begins early in MS; such loss is considered to reflect tissue destruction and has been shown to correlate with disability progression.5,10,16,22,23 Alemtuzumab significantly reduced brain volume loss compared with SC IFN-β-1a, and over the 2 years of study, there was a continued deceleration of volume loss in both patient populations. Moreover, it is possible that the observed results underestimate the treatment effect of alemtuzumab on this measure. Some of the apparent brain volume loss may actually reflect a therapeutic decrease in inflammation and edema, an effect called pseudo-atrophy.16 The greater apparent brain volume loss in CARE-MS I than in CARE-MS II supports this interpretation because treatment-naive patients would be expected to have more preexisting inflammation and edema than patients who had received prior disease-modifying therapies. Alemtuzumab also had a beneficial impact on other MRI outcomes that have been linked to neurologic impairment and accumulation of disability.24,25 Active inflammatory lesions that previously showed gadolinium enhancement may evolve into chronic T1-hypointense lesions, called black holes, representing foci of permanently reduced axonal density.25 In CARE-MS II, alemtuzumab-treated patients were more likely than SC IFN-β-1a–treated patients to have no new T1 lesions, and alemtuzumab significantly reduced the percentage of gadolinium-enhancing lesions converting to black holes vs SC IFN-β-1a during year 2. Therefore, imaging outcomes from both studies suggest that alemtuzumab has a more beneficial effect than SC IFN-β-1a on the chronic neurodegenerative processes associated with MS and support the observation in patients who had an inadequate response to prior therapy that alemtuzumab can slow the accumulation of disability more effectively than SC IFN-β-1a.26
We report here that, in both CARE-MS studies, the treatment effects of alemtuzumab surpassed the well-established benefits of the active comparator SC IFN-β-1a on a range of MRI endpoints linked to both the focal inflammatory disease associated with MS and chronic neurodegenerative processes associated with the accumulation of disability. The MRI findings reported here therefore provide complementary evidence for the observed clinical efficacy of alemtuzumab vs SC IFN-β-1a in patients with RRMS.
Supplementary Material
ACKNOWLEDGMENT
Prof. Christian Confavreux (in memoriam) and Dr. Edward Fox were members of the CARE-MS steering committee and contributed to study design but did not participate in manuscript development. Critical review of the manuscript was provided by Aji Nair, PhD, who was employed at Sanofi Genzyme during the development of the manuscript, and Stanley Krolczyk, DO, formerly of the University of South Florida and currently an employee of Sanofi Genzyme. Statistical analysis and critical review of the manuscript were provided by Amy Cinar, who was employed at Sanofi Genzyme during the development of the manuscript.
GLOSSARY
- BPF
brain parenchymal fraction
- CARE-MS
Comparison of Alemtuzumab and Rebif Efficacy in Multiple Sclerosis
- CI
confidence interval
- IFN-β-1a
interferon β-1a
- MS
multiple sclerosis
- RRMS
relapsing-remitting multiple sclerosis
Footnotes
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
D.L.A., J.A.C., A.J.C., H.-P.H., E.H., K.W.S., D.H.M., and D.A.S.C. contributed to study design, data collection, and writing and critical review of the manuscript and approved the final submission draft. E.F., V.V.B., G.G., M.S., and M.A.P. contributed to data collection and writing and critical review of the manuscript and approved the final submission draft. H.L.W. contributed to study design and writing and critical review of the manuscript and approved the final submission draft. D.L.A. also oversaw all MRI analyses with the exception of BPF analyses, which were supervised by E.F. S.L.L. led the statistical support, contributed to the writing and critical review of the manuscript, and approved the final submission draft. D.R.T. provided editorial and medical writing support (assistance in drafting the manuscript, technical editing, copyediting, and responding to reviewers’ comments).
STUDY FUNDING
Dr. Havrdova was supported by the Czech Ministry of Education, PRVOUK-P26/LF1/4. The CARE-MS studies were funded by Sanofi Genzyme and Bayer HealthCare Pharmaceuticals.
DISCLOSURE
D. Arnold reports having served on advisory boards for, received speaker honoraria from, served as a consultant to, or received research support from Acorda, Bayer, Biogen, Eli Lilly, EMD Serono, Genentech, GlaxoSmithKline, Medimmune, Merck Serono, NeuroRx Research, Novartis, Opexa Therapeutics, Receptos, Roche, Sanofi, Sanofi Genzyme, Teva, the Canadian Institutes of Health Research, and the Multiple Sclerosis Society of Canada, and holds stock in NeuroRx Research. E. Fisher has received consulting fees from Biogen, Novartis, and Sanofi Genzyme and research funding from the National Institutes of Health, Biogen, and Sanofi Genzyme. E. Fisher is now an employee of Biogen. V. Brinar reports no disclosures relevant to the manuscript. J. Cohen reports personal compensation for serving as a consultant or speaker from Biogen, Elan, Novartis, Teva, and Vaccinex and research support paid to his institution from Biogen, Consortium of MS Centers, US Department of Defense, NIH, National MS Society, Novartis, Receptos, Synthon, Sanofi Genzyme, and Teva. A. Coles reports receiving consulting fees, lecture fees, and institutional grant support from Sanofi Genzyme. G. Giovannoni reports receiving personal compensation for participating on advisory boards in relation to clinical trial design, trial steering committees, and data and safety monitoring committees from Bayer HealthCare Pharmaceuticals, Biogen, Canbex, Eisai, Elan, Fiveprime, Genentech, GlaxoSmithKline, Ironwood, Merck Serono, Novartis, Pfizer, Roche, Sanofi Genzyme, Synthon BV, Teva, UCB Pharma, and Vertex Pharmaceuticals. H. Hartung reports receiving the approval of the Rector of HHU fees for consulting, lectures, and activities in steering committees of the following companies: Bayer HealthCare Pharmaceuticals, Biogen, BioMS, Merck Serono, Novartis, Sanofi Genzyme, and Teva. E. Havrdova reports receiving honoraria and grant support from Bayer HealthCare Pharmaceuticals, Biogen, Genentech, GlaxoSmithKline, Merck Serono, Octapharma, Pfizer, Roche, Sanofi, Sanofi Genzyme, and Teva. K. Selmaj reports receiving consulting fees from Novartis, Biogen, Roche, and Sanofi Genzyme; lecture fees from Novartis, Merck Serono, Biogen, and Bayer HealthCare Pharmaceuticals; and financial compensation, including travel, from Sanofi Genzyme for scientific presentations. M. Stojanovic reports no disclosures relevant to the manuscript. H. Weiner reports receiving consulting/honoraria from Biogen, EMD Serono, Teva, Novartis, Nasvax, GlaxoSmithKline, and Sanofi Genzyme, and research support from EMD Serono and GlaxoSmithKline. S. Lake and D. Margolin report receiving personal compensation as employees of Sanofi Genzyme. D. Thomas reports receiving personal compensation as an employee of Evidence Scientific Solutions. M. Panzara reports receiving personal compensation as an employee of Sanofi Genzyme during study conduct and analysis and during preparation of the manuscript. A. Compston reports receiving consulting fees and grant support from Sanofi Genzyme and lecture fees from Bayer Schering Pharma on behalf of the University of Cambridge; and personal remuneration for lecture fees from Sanofi Genzyme. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Arnold DL. The place of MRI in monitoring the individual MS patient. J Neurol Sci 2007;259:123–127. [DOI] [PubMed] [Google Scholar]
- 2.Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol 2011;69:292–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sormani MP, Bonzano L, Roccatagliata L, Cutter GR, Mancardi GL, Bruzzi P. Magnetic resonance imaging as a potential surrogate for relapses in multiple sclerosis: a meta-analytic approach. Ann Neurol 2009;65:268–275. [DOI] [PubMed] [Google Scholar]
- 4.Sormani MP, Bonzano L, Roccatagliata L, De Stefano N. Magnetic resonance imaging as surrogate for clinical endpoints in multiple sclerosis: data on novel oral drugs. Mult Scler 2011;17:630–633. [DOI] [PubMed] [Google Scholar]
- 5.Sormani MP, Arnold DL, De Stefano N. Treatment effect on brain atrophy correlates with treatment effect on disability in multiple sclerosis. Ann Neurol 2014;75:43–49. [DOI] [PubMed] [Google Scholar]
- 6.Barkhof F, Simon JH, Fazekas F, et al. MRI monitoring of immunomodulation in relapse-onset multiple sclerosis trials. Nat Rev Neurol 2011;8:13–21. [DOI] [PubMed] [Google Scholar]
- 7.Giovannoni G, Silver NC, Good CD, Miller DH, Thompson EJ. Immunological time-course of gadolinium-enhancing MRI lesions in patients with multiple sclerosis. Eur Neurol 2000;44:222–228. [DOI] [PubMed] [Google Scholar]
- 8.Filippi M, Rocca MA, Barkhof F, et al. Association between pathological and MRI findings in multiple sclerosis. Lancet Neurol 2012;11:349–360. [DOI] [PubMed] [Google Scholar]
- 9.Fox EJ. Alemtuzumab in the treatment of relapsing-remitting multiple sclerosis. Expert Rev Neurother 2010;10:1789–1797. [DOI] [PubMed] [Google Scholar]
- 10.Jones JL, Anderson JM, Phuah CL, et al. Improvement in disability after alemtuzumab treatment of multiple sclerosis is associated with neuroprotective autoimmunity. Brain 2010;133:2232–2247. [DOI] [PubMed] [Google Scholar]
- 11.Cox AL, Thompson SA, Jones JL, et al. Lymphocyte homeostasis following therapeutic lymphocyte depletion in multiple sclerosis. Eur J Immunol 2005;35:3332–3342. [DOI] [PubMed] [Google Scholar]
- 12.Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial. Lancet 2012;380:1819–1828. [DOI] [PubMed] [Google Scholar]
- 13.Coles AJ, Twyman CL, Arnold DL, et al. Alemtuzumab for patients with relapsing multiple sclerosis after disease-modifying therapy: a randomised controlled phase 3 trial. Lancet 2012;380:1829–1839. [DOI] [PubMed] [Google Scholar]
- 14.Li DK, Paty DW. Magnetic resonance imaging results of the PRISMS trial: a randomized, double-blind, placebo-controlled study of interferon-beta1a in relapsing-remitting multiple sclerosis: Prevention of Relapses and Disability by Interferon-beta1a Subcutaneously in Multiple Sclerosis. Ann Neurol 1999;46:197–206. [DOI] [PubMed] [Google Scholar]
- 15.Francis SJ. Automatic Lesion Identification in MRI of Multiple Sclerosis Patients [Masters in Science thesis]. Montreal: McGill University; 2004. [Google Scholar]
- 16.Rudick RA, Fisher E, Lee JC, Simon J, Jacobs L. Use of the brain parenchymal fraction to measure whole brain atrophy in relapsing-remitting MS: Multiple Sclerosis Collaborative Research Group. Neurology 1999;53:1698–1704. [DOI] [PubMed] [Google Scholar]
- 17.CAMMS223 Trial Investigators, Coles AJ, Compston DA, et al. Alemtuzumab vs. interferon beta-1a in early multiple sclerosis. N Engl J Med 2008;359:1786–1801. [DOI] [PubMed] [Google Scholar]
- 18.Coles AJ, Fox E, Vladic A, et al. Alemtuzumab more effective than interferon beta-1a at 5-year follow-up of CAMMS223 clinical trial. Neurology 2012;78:1069–1078. [DOI] [PubMed] [Google Scholar]
- 19.Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med 2010;362:402–415. [DOI] [PubMed] [Google Scholar]
- 20.Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis: the Multiple Sclerosis Collaborative Research Group (MSCRG). Ann Neurol 1996;39:285–294. [DOI] [PubMed] [Google Scholar]
- 21.Kappos L, Radue EW, O’Connor P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med 2010;362:387–401. [DOI] [PubMed] [Google Scholar]
- 22.Sormani MP, Bonzano L, Roccatagliata L, Mancardi GL, Uccelli A, Bruzzi P. Surrogate endpoints for EDSS worsening in multiple sclerosis: a meta-analytic approach. Neurology 2010;75:302–309. [DOI] [PubMed] [Google Scholar]
- 23.Popescu V, Agosta F, Hulst HE, et al. Brain atrophy and lesion load predict long term disability in multiple sclerosis. J Neurol Neurosurg Psychiatry 2013;84:1082–1091. [DOI] [PubMed] [Google Scholar]
- 24.van Waesberghe JH, Kamphorst W, De Groot CJ, et al. Axonal loss in multiple sclerosis lesions: magnetic resonance imaging insights into substrates of disability. Ann Neurol 1999;46:747–754. [DOI] [PubMed] [Google Scholar]
- 25.Truyen L, van Waesberghe JH, van Walderveen MA, et al. Accumulation of hypointense lesions (“black holes”) on T1 spin-echo MRI correlates with disease progression in multiple sclerosis. Neurology 1996;47:1469–1476. [DOI] [PubMed] [Google Scholar]
- 26.Arnold DL, Cohen JA, Coles AJ, et al. Effect of Alemtuzumab versus Rebif on Brain MRI Measurements: Results of CARE-MS II. Presented at 29th Congress of the European Committee for Research and Treatment in Multiple Sclerosis (ECTRIMS); 2012; Lyon, France; P877.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.