

Abstract
The Medio-Dorsal Nuclei (MDN) including the thalamic magnocellular and parvocellular thalamic regions has been implicated in verbal memory function. In a 77 year old lady, with a prior history of a clinically silent infarct of the left MDN, we observed the acute onset of spontaneous confabulations when an isolated new infarct occurred in the right MDN. The patient and five age-matched healthy subjects underwent Magnetic Resonance Imaging (MRI) and Diffusion Tensor Imaging (DTI). The thalamic lesions were localized by overlapping Morel Thalamic Atlas with structural MRI data. DTI was used to assess: i) white matter alterations (Fractional Anisotropy, FA) within fibers connecting the ischemic areas to cortex; ii) the micro-structural damage (Mean Diffusivity) within the thalamic sub-regions defined by their structural connectivity to the Anterior Cingulate Cortex (ACC) and to the temporal lobes. These target regions were chosen because their damage is considered associated with the appearance of confabulations. Thalamic lesions were localized within the parvocellular regions of the right and left MDNs. The structural connectivity study showed that the fiber tracts, connecting the bilaterally damaged thalamic regions with the frontal cortex, corresponded to the anterior thalamic radiations (ATR). FA within these tracts was significantly lower in the patient as compared to controls. Mean diffusivity within the MDNs projecting to Broadman area (BA) 24, BA25 and BA32 of ACC was significantly higher in the patient than in control group. Mean diffusivity values within the MDN projecting to temporal lobes in contrast were not different between patient and controls. Our findings suggest the involvement of bilateral MDNs projections to ACC in the genesis of confabulations and help provide clarity to the longstanding debate on the origin of confabulations.
Abbreviations: ACoA, Anterior communicating artery; ACC, Anterior Cingulate Cortex; AN, Anterior thalamic nuclei; ATR, Anterior thalamic radiations; BA, Broadman area; BEDPOSTX, Bayesian Estimation of Diffusion Parameters obtained using Sampling; BET, Brain Extraction Tool; CSF, cerebrospinal fluid; DTI, Diffusion Tensor Imaging; DWI-SE, Diffusion Weighted Image Spin-Echo; FA, Fractional Anisotropy; FAST, FMRIB's Automated Segmentation Tool; FIRST, FMRIB's Integrated Registration and Segmentation Tool; FNIRT, FMRIB's Non-Linear Registration Tools; FLIRT, FMRIB's Linear Image Registration Tool; KS, Korsakoff Syndrome; MDN, Medio-dorsal thalamic nuclei; MNI, Montreal Neurological Institute (MNI); MRI, Magnetic Resonance Imaging; SUSAN, Smallest Univalue Segment Assimilating Nucleus; TE, Echo time; TR, Repetition time; W TFE, Weighted Turbo Field-Echo W TFE
Keywords: Confabulation, Amnesia, Medio-dorsal thalamic region
Highlights
-
•
Isolated and symmetric lacunar lesions were located in the medio-dorsal thalamus.
-
•
DTI shows disconnections between medio-dorsal thalamus and anterior cingulate cortex.
-
•
Medio-dorsal thalamus may have a role in the genesis of confabulations.
1. Introduction
Confabulations are defined as “falsification of memory occurring in clear consciousness in association with an organically derived amnesia” (Berlyne, 1972). Confabulations are classified as spontaneous (i.e. spontaneous outpouring of erroneous memories which can be sustained, wide-ranging, grandiose) or provoked (i.e. by questions probing memory) (Berlyne, 1972). The narrative of confabulation varies with the environment context (spontaneous) or probing (provoked) and this is in contrast with delusions which are characterized by consistent narratives, which do not vary through time, and have recognizable patterns or themes e.g. persecutory, jealous, guilt, of reference, as reported in 5th edition of Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013). It is not clear whether the two types of confabulations represent different disorders (Van der Horst, 1932, Kopelman, 1987) or different degrees of a condition which in the presence of concurrent amnesia starts with the appearance of provoked (“moderate”) confabulations and progresses to spontaneous (“severe”) production of false memories (Kapur and Coughlan, 1980, DeLuca and Cicerone, 1991, Della Barba, 1993, Fischer et al., 1995).
Patients who confabulate spontaneously act upon memories that are obviously false or provide false information without intending to lie, and are unaware of these falsehoods.
Confabulations may be present in several different conditions, including ruptured aneurysms of the anterior communicating artery, subaracnoid haemorrage, encephalitis, Alzheimer' disease (AD) and traumatic brain injury. Spontaneous confabulations were originally described in Korsakoff Syndrome (KS) following Wernicke encephalopathy. KS is typically due to thiamine deficiency, and is clinically characterized by anterograde amnesia although confabulations may or may not be a feature (Markowitsch, 2000). Pathologically, KS is characterized by variable lesions of mammillary bodies, of anterior (AN) or medio-dorsal thalamic nuclei (MDN) and of mammillo-thalamic projections (Gold and Squire, 2006, Harding et al., 2000, Mair et al., 1979, Mayes et al., 1988).
From an imaging perspective, patients with KS have been shown to have hyperintensities in diencephalic, mesencephalic (Cerase et al., 2011), hypothalamic (Ptak et al., 2001), encephalic (Kopelman et al., 2009, Victor et al., 1971) and cerebellar (Laureno, 2012) structures.
Nevertheless, the clinic-pathological origin of confabulations in KS are still a subject of debate. Historically the amnesia associated with KS was reported not to correlate with the severity of spontaneous confabulations (Benson, 1994, Mercer et al., 1977), and the onset of confabulation was attributed to the disconnection of one of the relays of Papez circuit, with the debate first focusing on lesions of the mammillary bodies and fornices (Dusoir et al., 1990, Mair et al., 1979, Victor et al., 1971), independently of thalamic lesions. Subsequently the possible role of the AN and, in particular, the impact of damage to mammillo-thalamic tracts which carry projections from the mammillary bodies to the AN (Aggleton and Brown, 1999, Clarke et al., 1994, Harding et al., 2000, Carlesimo et al., 2011, Danet et al., 2015, Ghika-Schmid and Bogousslavsky, 2000) was highlighted. Other authors have further implicated the medial structures of the thalamus as the MDN (Aggleton and Brown, 1999, Cipolotti et al., 2008, Graff-Radford et al., 1990, Markowitsch, 1983, Van der Werf et al., 2000) in the aetiology of confabulations whilst others have suggested that confabulations, in KS, do not occur without thalamic lesions of anterior, or of medial or medio-dorsal nuclei (Brion et al., 1983, Mair et al., 1979).
Isolated lesions may provide clarity on these debates on the origin of confabulations but the majority of studies focusing on diencephalic amnesia due to vascular lesions, have not reported on these. Limited studies have suggested that confabulations occur after AN or MDN lesions (Markowitsch et al., 1993, Schnider et al., 1996a), but in other studies, patients with similar lesions of the MDN and posterior thalamic nuclei lesions did not express any confabulations (Karnath et al., 2001, Muller et al., 1999).
Florid confabulations have also been described in patients who survived ruptures of anterior communicating artery (ACoA), and these have been identified as patients with ACoA amnesic confabulatory syndrome. Notably however confabulations can occur in these cases in the absence of thalamic lesions (Damasio et al., 1985, DeLuca and Cicerone, 1991; DeLuca, 1993, Schnider et al., 1996a, Ptak and Schnider, 1999) and instead have been suggested to arise as a result of cortical lesions of orbitofrontal areas and Anterior Cingulate Cortex (ACC), which are not affected in KS.
With the present report we describe the occurrence of spontaneous confabulations following bilateral isolated ischemic lesions of MDN, mainly involving the parvocellular nuclei.
The patient described in the present report qualified as a ‘spontaneous confabulator’ based on the criterion proposed by Berlyne in 1972 in that the patient acted upon her self-generated confabulations.
We also combined structural MRI and DTI to assess the possible microstructural damage of thalamic regions projecting to the ACC to further understand the anatomical impact of the lesions in our patient and their relation to the confabulations.
Finally, we compared lesions observed in five previously described cases of thalamic confabulations, with lesions observed in the present case.
2. Materials and methods
2.1. Case description
At the time of admission and appearance of confabulations, the patient was a 77 year old lady, married for 56 years, mother of two daughters and grandmother of four grandchildren. She was moderately obese (BMI = 31.2) and she had an eight-year history of type 2 Diabetes in the context of a Metabolic Syndrome, which was treated with 500 mg metphormine b.i.d., three years history of hypertension treated with candesartan, 16–32 mg day, and hypercholesterolemia, treated with rosuvastatine 20 mg day. Her family history was unremarkable, and a detailed post-hoc collateral history obtained from her General Practitioner and family members confirmed absence of any psychiatric history preceding the events leading to admission to the hospital.
Two years before her most recent infarct, she had been admitted to our hospital because of an acute sensation of lightheadedness and confusion, with lethargy, which had lasted for 2 h and which had occurred 26 h before hospital admission. She was completely asymptomatic when admitted on ward, and the event was interpreted as Transient Ischemic event, but a CT scan performed two days after this first event, showed an isolated hypodensity in the left MDN (Fig. 1A).
Figure 1.

CT scan performed after the two admissions. Panel A shows CT scan performed two days after the left ischemic lacune appearance. Panels B and C show CT scans performed 3 and 6 days after the right MDN lacune appearance, two years after the left lacune.
The primary presentation leading to the new and most recent admission, according to her family members, was that of confusion and disorientation. The first CT scan performed 8 h after the onset of symptoms, at arrival to the hospital, showed only a residual hypodensity of the left MDN.
On the following day disorientation was still present, and bedside neuropsychiatric examination revealed anterograde amnesia and a retrograde amnesia for the three days preceding admission.
However, the symptom of major concern for the family was that the patient had bizarre thought content, the most consistent being that she was in the hospital because of pregnancy and was close to partum. When involved in spontaneous conversation with neurologists, she could not be averted from the topic of the imminent delivery, and her confabulations were detailed and florid; when asked about the role of attending nurses she explained that they were midwives, and when in the presence of her husband, she jocularly identified him as the “culprit” of her hospital admission.
Further attempts, by the examiners, to involve the patient in conversation, always resulted in florid confabulations, about different issues (e.g. professional activities of her relatives, housework, culinary ability etc.). Objectively, the bedside Cookie Theft picture test (Goldglass and Kaplan, 1983) was described with florid confabulations about events preceding the activities represented in the picture.
A CT scan performed two days after onset of confabulations showed the appearance of right MDN hypodensity (Fig. 1A–B). Subsequent CT-angiography, extracranial and intracranial artery ultra-sound scan and echocardiography were normal. Two EEGs, performed during the hospital stay were normal. The patient underwent MRI at day 7 after the onset of confabulations and confirmed the presence of bilateral ischemic thalamic lesions (Fig. 2).
Figure 2.

MRI scan performed after second admission. Figure show MRI performed 8 days after the right MDN lacune appearance.
Our clinical interpretation was that the observed bilateral MDN lesions were due to lacunae in the territory of the polar pre-mammillary thalamic or tubero-thalamic arteries, rather than to cardiac emboli.
The patient underwent lumbar puncture to exclude the presence of cerebrospinal fluid marker of AD. CSF AD profile was defined as follows: beta amyloid level < 800 pg/mL, total tau > 300 pg/mL, and phosporylated-tau protein > 60 pg/mL (Parnetti et al., 2008). CSF protein levels were normal: 42-amino-acid isoform of amyloid-β1-42 (Aβ42) was 971 pg/mL (normal values > 800 pg/mL), total tau 165 pg/mL (normal values < 300 pg/mL), phosphorylated tau (P-tau) 25 pg/mL (normal values < 60 pg/mL).
The patient was discharged three days after the acute onset of confabulations. A detailed neuropsychological evaluation was performed 8 days after the onset of confabulations. The patient's engagement with the neuropsychological assessments was good. The evaluation demonstrated that the patient was remarkably impaired in tests assessing declarative episodic memory for verbal material and she also showed abnormal scores of episodic memory tests based on visuospatial material. On tests assessing executive functions the patient scored poorly and confabulated as shown by specific neuropsychological battery results (Table 1).
Table 1.
Patient's neuropsychological assessment.
| Domain/test | Raw scores | Stanine (StN) or *corrected scores | Cut-off scores | %ile or %ile range |
|---|---|---|---|---|
| General Cognition | ||||
| MMSE | 23 | *22.3 | 24 | |
| Raven (coloured matrices) | 18 | StN = 2 | 17–28 | |
| Memory | ||||
| Rey verbal learning | ||||
| Immediate | 20 | StN = 1 | 6–17 | |
| Delayed | 1 | StN = 0 | < 5 | |
| Words paired associate learning | 2 | StN = 0 | < 5 | |
| Short story | ||||
| Immediate and delayed | 3 | StN = 0 | < 5 | |
| Supra-span spatial learning | 1 | StN = 0 | < 5 | |
| Attention/WM | ||||
| Digit span forward | 4 | StN = 2 | 17–28 | |
| Corsi | 3 | StN = 1 | 6–17 | |
| TMTA | 121 | StN = 1 | 6–17 | |
| TMTB | 289 | StN = 0 | < 5 | |
| Visual search | 34 | StN = 2 | 17–28 | |
| Executive Functions | ||||
| FAB | 11/18 | 13.4 | ||
| WCST (% perseverative errors) | 53 | 6 | ||
| WCST (% errors) | 74 | 4 | ||
| Verbal fluency (semantic) | 8 | StN = 2 | 17–28 | |
| Neuropsychiatric inventory | 32 | |||
| Confabulation battery | Correct/total resp. | Confabul./total resp. | ||
| Personal semantic memory | 12/20 | 6/20 | ||
| Episodic memory | 8/15 | 7/15 | ||
| Time and place orientation | 6/10 | 2/10 | ||
| General semantic memory | 8/15 | 0/15 | ||
Bold type: relevant findings. Cut-off scores are only reported when applicable.
StN: stanine scores, this is a method of scaling test scores on a nine-point standard scale with a mean of five and a standard deviation of two. It is the Standard Method for rating neuropsychological test scores on the Italian Population. StN = 0 is outside normative limits, StN = 1indicates lower limit of control population. %ile indicates conversion from the stanine scale into percentile based on the normative data. FAB: Frontal assessment battery; WCST: Wisconsin Card Sorting Test; TMTA: trail making test part A; TMTB trail making test part B. In bold the impaired performance.
Confabulations continued after discharge from the hospital: themes of pregnancy and partum subsided 2 weeks after her return at home, but were substituted by further confabulations related to daily life issues, family relationships, economic matters, and her husband's job and these confabulations were sustained even 5 years after the right MDN infarct. For example, when asked about her husband, who was 85 years old by then and had been retired for 20 years, she would explain that he was out to work detailing cores and activities. No evidence was ever reported of delusional ideation, e.g. persecutory, jealousy, guilt, grandiose, religious, somatic, ideas of reference (Fernandez et al., 2008), nor of hallucinations in any sensory modality. Because of amnesia, confabulations and apathy, the latter being the main concern of the patient's caregivers during follow-up, and lack of other neurological explanations, our clinical opinion was that the symptoms were consistent with anterior (Ghika-Schmid and Bogousslavsky, 2000) or combined polar and paramedian (Perren et al., 2005) thalamic infarction.
Deficits in neuropsychological test scores remained consistent during follow up. Supplementary Table 1 shows the results of an assessment performed two years after Right MDN lesion, supporting the argument that there was no progressive neurodegenerative process.
2.2. Neuropsychological assessment
The Neuropsychological assessment consisted of tests standardized on the Italian population, investigating the following cognitive domains (Table 1 and Supplementary Table 1): general cognition [Mini Mental Examination (Folstein et al., 1975); Raven Coloured Progressive Matrices (Basso et al., 1987)], executive functions [Frontal Assessment Battery (Appollonio et al., 2005); Wisconsin Card Sorting Test (Heaton, 1981); Verbal Fluency (Spinnler and Tognoni, 1987)], short and long term memory [Rey Verbal Learning (Carlesimo et al., 1996); Words Paired Associate Learning and Short Story (Novelli et al., 1986); Supra-Span Spatial Learning, Spinnler and Tognoni, 1987)], working memory and attention [Trail Making Test (Giovagnoli et al., 1996); Digit Span and Corsi Test (Orsini et al., 1987); Visual Search (Spinnler and Tognoni, 1987)]. Visuospatial skills were investigated, by means of visual attention and visual memory tests. A detailed evaluation of language was not assessed because the patient did not show any symptoms (such as anomia or paraphasia) at bedside test. In addition we also investigated the presence of neuropsychiatric symptoms (the NPI; Cummings et al., 1994) as well the tendency to confabulate by means of a structured questionnaire (Della Barba, 1993). This last is a pool of 95 questions involving the retrieval of various kinds of information such as personal, general and linguistic semantic memory, episodic memory and orientation. We used 4 out of the 6 original sets for a total of 60 questions. We did not administer the two sets of “I don't know” questions, i.e. questions constructed so that the appropriate response is likely to be “I don't know” by a normal subject. Responses were classified as correct, wrong or confabulatory. No standard scores are available for the battery, however the number of confabulatory responses for each set can definitely provide a picture of the confabulatory behavior.
2.3. MR protocol
The first MR data were collected 7 days after the acute onset of the symptoms. A second recording was performed 3 months later. All MR data were collected with a Philips Achieva 3 T scanner (Philips Medical System, Best, the Netherlands) equipped with 8-channel receiver coil. After scout and reference sequences, a 3-dimensional T1-Weighted Turbo Field-Echo (3D T1-W TFE, TR/TE = 11/5 ms, slice thickness of 0.8 mm, FOV = 256 × 192 × 170 mm) and Diffusion Weighted Image Spin-Echo (DWI-SE; TR/TE = 3691/67 ms, 15 diffusion-sensitive gradient directions) sequences were performed.
Five age-matched healthy women were used as controls.
2.4. MR data analysis
MR data were processed by using Functional MRI of the Brain (FMRIB) Software Library (FSL version 4.1 (http://www.fmrib.ox.ac.uk/fsl; (Smith et al., 2004) and TrackVis (http://trackvis.org).
2.4.1. Preprocessing
Noise reduction on T1 images was performed using Smallest Univalue Segment Assimilating Nucleus (SUSAN) algorithm on structural images. Eddy-currents correction was performed on diffusion images. For structural and DWI images, brain and skull extraction was carried out using Brain Extraction Tool (BET).
2.4.2. Localization of thalamic lesions
The T1 structural image of the patient was co-registered in common space on the non-linear MNI152 template with 1 × 1 × 1 mm resolution, by means of affine transformations based on 12 degrees of freedom (three translations, three rotations, three scalings and three skews) using FMRIB's Linear Image Registration Tool (FLIRT). Working on MNI space, a Morel three-dimensional atlas of the human thalamus (Morel et al., 1997, Krauth et al., 2010) was overlapped on the patient T1 image in order to localize the thalamic bilateral lesions.
2.4.3. Thalamic parcellation and micro-structural assessment
Segmentation of thalami was performed by processing T1-W structural images with FMRIB's Integrated Registration and Segmentation Tool (FIRST) (Patenaude et al., 2011).
Mean diffusivity was assessed because it is an index for both grey and white matter damage and high values of mean diffusivity are related to membrane density reduction and cell loss of both neurons and glia (Canu et al., 2010, Delli Pizzi et al., 2014, Delli Pizzi et al., 2015).
For each participant, mean diffusivity maps were obtained from a tensor-model fit in FSL (FDT, FMRIB's Diffusion Toolbox). Next, mean diffusivity maps were registered to MNI standard space using FMRIB's Non-Linear Registration Tools (FNIRT).
By using the methods described by Behrens et al. (2003), the MRI and DWI data of control subjects were combined to parcellate MDN (defined by MNI Morel Atlas) according to their cortical structural connectivity with BA24, BA25 and BA32. These data were merged for constructing a MDN structural connectivity atlas. The binarized MDN obtained from the MNI Morel Atlas was used as “seed” structure. The binarized Harvard Oxford Cortical Atlas (provided by FSL) was then used to “target” cortical regions. Thalamic CDR projecting to temporal cortex was obtained from Oxford thalamic connectivity atlas (provided by FSL). All masks were in Montreal Neurological Institute (MNI) space (1 × 1 × 1 mm). After Bayesian Estimation of Diffusion Parameters obtained using Sampling Techniques (BEDPOSTX), the DTI maps were registered to MNI standard space using: 1. FLIRT to register each subject's b0 image to its native structural image, and 2. FMRIB's Non-Linear Registration Tools (FNIRT) to register the structural and diffusion images to MNI space (1 × 1 × 1 mm). All masks were then propagated onto each individual's DTI scalar maps using the inverse of the above transformations. To exclude thalamic voxels that contained cerebrospinal fluid (CSF), the b0 images were segmented using FMRIB's Automated Segmentation Tool (FAST) and CSF binarized to be used as exclusion mask. Next, probabilistic tracking was performed by PROBTRACKX tool. “Find the biggest” command line was used to obtain an atlas defining the MDN subdivision on basis of its connection with ACC (Fig. 3). Finally, the mean diffusivity values were calculated in each connectivity-defined sub-region (CDR).
Figure 3.

Structural connectivity-based subdivision of medio-dorsal thalamic regions (MDNs) obtained from control subjects. Voxels are classified and coloured according to the highest probability of connection to a specific cortical region. Red = connectivity-defined sub-region (CDR) that projects from MDN thalamus to BA25; dark Blue = CDR that projects from thalamus to BA32; green = CDR that projects from MDN to BA24; yellow = CDR that projects from thalamus to temporal lobe. R = right; L = left. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
2.4.4. Tractography and structural connectivity assessment
For each participant, fractional anisotropy (FA) maps were obtained from a tensor-model fit in FSL (FDT, FMRIB's Diffusion Toolbox). TrackVis (http://trackvis.org) was used for visualization purpose and to perform tractography. Specifically, by using the subject's b0 image as reference, two spheres (radius = 3 mm) were placed on the right and left thalamic lesions, as “seed regions”. Structural connectivity along the resulting tracts of interest was assessed by FA.
2.5. Comparison with previous cases
A complete literature search (PubMed search: thalamus and confabulations), and careful reading of case descriptions, allowed the identification of five previous cases, presenting with unequivocally described confabulations and isolated thalamic lesions documented by MRI figures. One further case, of bilateral combined thalamic lesions with confabulations, did not have any MRI data (Perren et al., 2005). The five cases were reported by Markowitsch et al. (1993), Schnider et al. (1996a), Nys et al. (2004), Yoneoka et al. (2004), and one was a case out of 12 of the Ghika-Schmid and Bogousslavsky (2000) series. None of these studies performed the thalamus parcellation based on structural connectivity, neither did they identify the lesion sites by coregistering with a thalamic atlas (e.g. Morel) on their structural MRI data. Indeed, the identification of the lesion location was carried out by visual comparison with atlases or by redrawing the lesions on anatomical templates developed by the authors within their respective research centers (Ghika Schmidt and Bougousslavski, 2000). In order to compare the different findings we manually reported the thalamic lesions described by the different authors on an MNI template of one of the planes showing lesions in our patient. As MRI raw data from the different studies were not available, we are well aware that our drawings of lesions described by other authors represent an approximation, yet the figure renders a concise idea of sidedness and anteromedial location of thalamic lesions.
2.6. Statistical analysis
Confidence interval (mean ± 3 SD) was estimated on FA and mean diffusivity values obtained from the control groups. Patient FA values were standardized (z-scores) and z scores ≥ 3 were considered as a substantial change in FA and mean diffusivity.
3. Results
Visual inspection of patients' MRI images showed symmetrical lacunar thalamic infarctions (Fig. 2A–F). The thalamic lesions were localized within the parvocellular MDN of the right and left thalami (Fig. 4). No additional brain abnormalities were detected on T2-weighted and FLAIR scans. None of the healthy controls had any MRI-detectable abnormality.
Figure 4.

Location of right and left thalamic lesion on mediodorsal nuclei, according with the Morel Atlas. The red and orange boundaries delimit respectively the magnocellular and parvocellular portions of the thalami. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
The comparison between our patient and controls showed bilaterally increased mean diffusivity values in thalamic CDR, evidencing reduced integrity of medio-dorsal thalamic regions projecting to BA25, BA24 and BA32 areas (Table 2). No difference was observed for the mean diffusivity within the MDN projecting to temporal lobes.
Table 2.
Mean diffusivity values within the right and left thalamic regions projecting to anterior cingulate cortex (including BA24, BA25 and BA32 areas) and to temporal cortex.
| Controls | Patient | Lower CI | Upper CI | |
|---|---|---|---|---|
| BA24-R | 0.000760 ± 0.000081 | 0.000834 | 0.000719 | 0.000800 |
| BA24-L | 0.000757 ± 0.000030 | 0.000925 | 0.000696 | 0.000818 |
| BA25-R | 0.000816 ± 0.000061 | 0.001129 | 0.000690 | 0.000942 |
| BA25-L | 0.000787 ± 0.000056 | 0.000911 | 0.000671 | 0.000903 |
| BA32-R | 0.000781 ± 0.000016 | 0.000820 | 0.000736 | 0.000814 |
| BA32-L | 0.000761 ± 0.000031 | 0.000771 | 0.000698 | 0.000824 |
| Temporal-R | 0.000799 ± 0.00016 | 0.000805 | 0.000776 | 0.000823 |
| Temporal-L | 0.000785 ± 0.00026 | 0.000801 | 0.000788 | 0.000827 |
Mean diffusivity values are expressed as mean ± standard deviation (SD); CI = Confidence Interval (mean ± 3 SD). Significant results are reported in bold.
The tractography showed that fibers, which started from thalamic regions involved by ischemic lesions and project to the frontal cortex, were accurately matched with right and left anterior thalamic radiations (ATR) (Fig. 5). The FA within these tracts was significantly lower in the patient as compared to controls (Table 3).
Figure 5.

Tractography results. Left panel: the right and left anterior thalamic radiations (ATRs) projecting from the “seed region” (thalamic lesions) to prefrontal cortex. Right panel: box plot reporting the distribution of the FA values for the right and left ATRs in the patient (red line in the plot) and controls. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Table 3.
Fractional anisotropy (FA) values within the right and left anterior thalamic radiations in patient and controls.
| FA |
||
|---|---|---|
| Right ATR | Left ATR | |
| Controls | 0.43 ± 0.02 | 0.43 ± 0.02 |
| Patient | 0.37 | 0.36 |
| Upper CI | 0.46 | 0.43 |
| Lower CI | 0.39 | 0.38 |
FA values are expressed as mean ± standard deviation (SD); CI = Confidence Interval (mean ± 3 SD). Significant results are reported in bold.
Volumetric measures of the thalami showed no significant differences between the patient and the controls subjects.
4. Discussion
The case report described in our paper demonstrates that confabulations can occur as a result of isolated bilateral and symmetric ischemic lesions of the MDN, particularly the parvocellular nuclei. The identification of thalamic nuclei was carefully obtained by matching with Morel's Atlas and by thalamic parcellation. This evidence provides a clinical answer to the vexed question about the origin of confabulations. In KS the variability and extent of observed lesions in previous studies has made it difficult to delineate precisely which anatomical structures account for confabulations (Victor et al., 1971). In contrast, in our reported case we observed that isolated ischemic lesions of MDN were characterized by florid confabulations, which accompanied anterograde amnesia.
In our patient, MDN lesions were particularly symmetric and anatomically discrete, involving only limited parts of thalami, unlike lesions observed in KS and in other neurodegenerative disorders.
The MDN lesions occurred in different times in our patient, but the onset of confabulations only manifested when the second lacunar stroke of the right MDN occurred.
In Fig. 6 we present a reconstruction, in comparison with lesions observed in our patient, of sites and extent of lesions reported in the four previous single case studies, where spontaneous confabulations were unequivocally described (Markowitsch et al., 1993, Schnider et al., 1996b, Nys et al., 2004, Yoneoka et al., 2004) and in the patient R2 of the case series by Ghika-Schmid and Bogousslavsky (2000), who was the only one presenting with confabulations out of twelve patients. As explained in methods, our reconstruction is based on MRI figures reported in the original studies, while, in our case, the identification of nuclei is based on connectivity parcellation and atlas matching. In the quoted studies, excluding the study by Markowitsch (1983), the involved thalamic nuclei are indicated as anterior or anteromedial. In the case of patient R2, by Ghika-Schmid and Bogousslavsky (2000), thalamic lesions involved only the right AN and MDN. In the case reported by Nys et al. (2004), thalamic lesions were in the right anteromedial thalamic nuclei, but further bilateral thalamic lesions involved also the MDN. In the case reported by Yoneoka et al. (2004), the left AN were instead involved, but bilateral lesions also encompassed the mammillo-thalamic tracts. The extent and locations of the infarcts described in Markowitsch's patient are strikingly similar to those reported in our study, and in the case by Schnider et al. (1996b), like in the case by Ghika-Schmid and Bogousslavsky (2000), only the right AN were affected by ischemia, but the capsular genu and white matter (where ATRs are located, Fig. 5) were also affected.
Figure 6.
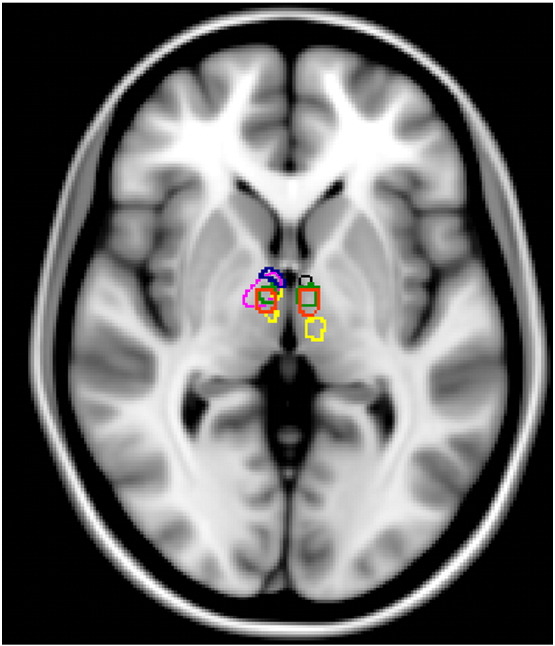
Comparison of the lesions observed in present case with lesions of confabulating patients described in five previous studies. Image shows the sites and extent of the lesions of the previous studies reporting the emergence of spontaneous confabulations in comparison with the lesions observed in our patient (delimited with orange boundaries). The lesions reported in Schnider et al. (1996b), Markowitsch et al. (1993), Nys et al. (2004), Ghika-Schmid and Bogousslavsky (2000) and Yoneoka et al. (2004) were highlighted with blue, green, yellow, fuchsia and black boundaries, respectively. All lesions boundaries were manually drawn on the basis of the figures reported in the original studies. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)
Therefore, our comparison of the few reported cases of ischemic thalamic confabulations, suggests that, in order to induce confabulations, anterior and MDN lesions should involve the right thalamus [as evident in the second ischemic lesion observed in our patient, or in the patient described by Schnider et al. (1996b), and in the case of patient R2 by Ghika-Schmid and Bogousslavsky (2000)] or should involve bilateral thalamic areas [our case, Markowitsch et al. (1993), Nys et al. (2004), Yoneoka et al. (2004)]. We therefore suggest that any lesion of right or left anteromedial thalamus disinhibits the production of narrative confabulations, but bilateral involvement of the Papez circuit (in any site of the circuit) is needed in order to provide the severity of the background amnesia, which will, in turn, drive the richness of the confabulatory narrative.
The novelty of our study, is that by combining MRI and DTI techniques, not used in prior studies, we could also demonstrate microstructural damage of the MDN, which connects thalamus with the frontal cortex and the ACC.
We focused our attention to projections of MDN to ACC and medial frontal cortex given that the only other clinical condition where confabulations occur, as a result of spatially restricted lesions, is the AcoA syndrome, where orbitofrontal (OF) and ACC are variably disrupted by aneurismal ruptures (Turner et al., 2008), and because a previous Single Photon Emission CT study in a patient with KS (Benson et al., 1996) showed hypoperfusion in ACC.
In our patient, we found WM alterations within the anterior thalamic radiations and micro-structural damage within MDN projecting to BA24, BA25 and BA32. Conversely, we also observed that thalamic projections to the temporal lobe were preserved bilaterally. Therefore, we suggest that these projections do not play a significant role in the aetiology of confabulations. Whereas temporal lobes are known to have connections with anterior thalamic nuclei via the Papez circuit (Jankowski et al., 2013) and sparse connections of the perirhinal cortex are known to reach the MDN (Mitchell and Charbotky, 2013), the largest bundle of fibers (the temporo-pulvinar bundle) reaches the posterior thalamic nuclei (pulvinar) (Zhang et al., 2010, Klein et al., 2010, Aggleton and Brown, 2006), which was not damaged in our patient.
A previous hypothesis on the mechanism of confabulations in patients with ACoA syndrome suggests that lesions of orbitofrontal areas and ACC induce confabulations by altering reality monitoring and representation of ongoing reality (Schnider et al., 1996a, Schnider et al., 1996b, Schnider, 2001, Schnider, 2003, Schnider et al., 2005), or by causing a dysfunction in strategic memory retrieval (Moscovitch, 1989, Moscovitch and Melo, 1997).
As an alternative explanation, we suggest that the ACC could modulate, by inhibition, the activity of posterior cingulate cortex, which is the main hub of the Default Mode Network (DMN). Lesions of MDN, by altering glutamatergic facilitatory projections to ACC, could downregulate ACC and disinhibit the DMN, whose role is thought to consist mainly in the introduction of self-referential narrative into experience (Gusnard and Raichle, 2001, Catani et al., 2013). The ensuing disinhibition of the DMN could explain the florid narratives occurring in confabulations. This hypothesis is speculative, however, and will need further experimental assessments to determine its veracity: fMRI studies should assess, in confabulating patients, whether DMN is disinhibited, like in frontotemporal lobar degeneration (Zhou et al., 2010), Lewy body dementia and Parkinson's Disease with Dementia patients with delusions and hallucinations (Franciotti et al., 2013, Franciotti et al., 2015, Galvin et al., 2011, Kenny et al., 2012, Peraza et al., 2014, Shine et al., 2015), or inhibited, like in AD patients (Greicius et al., 2004).
The following are the supplementary data related to this article.
Supplementary Table 1.
Acknowledgments
Funding: This work was supported by the Italian Ministry of Health [grant no. GR-2010-2313418].
References
- Aggleton J.P., Brown M.W. Episodic memory, amnesia, and the hippocampal-anterior thalamic axis. Behav. Brain Sci. 1999;22:425–444. discussion 444-489. [PubMed] [Google Scholar]
- Aggleton J.P., Brown M.W. Interleaving brain systems for episodic and recognition memory. Trends Cogn. Sci. 2006;10:455–463. doi: 10.1016/j.tics.2006.08.003. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association . American Psychiatric Association; 2013. Diagnostic and Statistical Manual of Mental Disorders. [Google Scholar]
- Appollonio I., Leone M., Isella V., Piamarta F., Consoli T., Villa M.L., Forapani E., Russo A., Nichelli P. The frontal assessment battery (FAB): normative values in an Italian population sample. Neurol. Sci. 2005;26:108–116. doi: 10.1007/s10072-005-0443-4. [DOI] [PubMed] [Google Scholar]
- Basso A., Capitani E., Laiacona M. Raven's coloured progressive matrices: normative values on 305 adult normal controls. Funct. Neurol. 1987;2:189–194. [PubMed] [Google Scholar]
- Behrens T.E., Johansen-Berg H., Woolrich M.W., Smith S.M., Wheeler-Kingshott C.A., Boulby P.A., Barker G.J., Sillery E.L., Sheehan K., Ciccarelli O., Thompson A.J., Brady J.M., Matthews P.M. Non-invasive mapping of connections between human thalamus and cortex using diffusion imaging. Nat. Neurosci. 2003;6:750–757. doi: 10.1038/nn1075. [DOI] [PubMed] [Google Scholar]
- Benson D.F. New York Oxford University press; 1994. The Neurology of Thinking. [Google Scholar]
- Benson D.F., Djenderedjan A., Miller B.L., Pachana N.A., Chang L., Itti L., Eng G.E., Mena I. Neural basis of confabulation. Neurology. 1996;46:1239–1243. doi: 10.1212/wnl.46.5.1239. [DOI] [PubMed] [Google Scholar]
- Berlyne N. Confabulation. Br. J. Psychiatry. 1972;120:31–39. doi: 10.1192/bjp.120.554.31. [DOI] [PubMed] [Google Scholar]
- Brion S., Mikol J., Plas J. Memoire et specialization fonctionelle hemispherique. Rapport anatomoclinique. Rev. Neurol. 1983;139:39–43. [PubMed] [Google Scholar]
- Canu E., McLaren D.G., Fitzgerald M.E., Bendlin B.B., Zoccatelli G., Alessandrini F., Pizzini F.B., Ricciardi G.K., Beltramello A., Johnson S.C., Frisoni G.B. Microstructural diffusion changes are independent of macrostructural volume loss in moderate to severe Alzheimer's disease. J. Alzheimers Dis. 2010;19:963–976. doi: 10.3233/JAD-2010-1295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlesimo G.A., Caltagirone C., Gainotti G., the Group for the Standardization of the Mental Deterioration Battery, editors. The mental deterioration battery: normative data, diagnostic reliability and qualitative analyses of cognitive impairmentEur Neurol. 1996;36:378–384. doi: 10.1159/000117297. [DOI] [PubMed] [Google Scholar]
- Carlesimo G.A., Lombardi M.G., Caltagirone C. Vascular thalamic amnesia: a reappraisal. Neuropsychologia. 2011;49:777–789. doi: 10.1016/j.neuropsychologia.2011.01.026. [DOI] [PubMed] [Google Scholar]
- Catani M., Dell'Acqua F., Thiebaut de Schotten M. A revised limbic system model for memory, emotion and behavior. Neurosci. Biobehav. Rev. 2013;37:1724–1737. doi: 10.1016/j.neubiorev.2013.07.001. [DOI] [PubMed] [Google Scholar]
- Cerase A., Rubenni E., Rufa A., Vallone I., Galluzzi P., Coratti G., Franchi F., Giannini F., Venturi C. CT and MRI findings of Wernicke's encephalopathy. Radiol. Med. 2011;16:319–333. doi: 10.1007/s11547-011-0618-x. [DOI] [PubMed] [Google Scholar]
- Cipolotti L., Husain M., Crinion J., Bird C.M., Khan S.S., Losseff N., Howard R.S., Leff A.P. The role of the thalamus in amnesia: a tractography, high-resolution MRI and neuropsychological study. Neuropsychologia. 2008;46:2745–2758. doi: 10.1016/j.neuropsychologia.2008.05.009. [DOI] [PubMed] [Google Scholar]
- Clarke S., Assal G., Bogousslavsky J., Regli F., Townsend D.W., Leenders K.L., Blecic S. Pure amnesia after unilateral left polar thalamic infarct: topographic and sequential neuropsychological and metabolic (PET) correlations. J. Neurol. Neurosurg. Psychiatry. 1994;57:27–34. doi: 10.1136/jnnp.57.1.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings J.L., Mega M., Gray K., Rosenberg-Thompson S., Carusi D.A., Gornbein J. The neuropsychiatric inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44:2308–2314. doi: 10.1212/wnl.44.12.2308. [DOI] [PubMed] [Google Scholar]
- Damasio A.R., Graff-Radford N.R., Eslinger P.J., Damasio H., Kassell N. Amnesia following basal forebrain lesions. Arch. Neurol. 1985;42:263–271. doi: 10.1001/archneur.1985.04060030081013. [DOI] [PubMed] [Google Scholar]
- Danet L., Barbeau E.J., Eustache P., Planton M., Raposo N., Sibon I., Albucher J.F., Bonneville F., Peran P., Pariente J. Thalamic amnesia after infarct: the role of the mammillothalamic tract and mediodorsal nucleus. Neurology. 2015;85:2107–2115. doi: 10.1212/WNL.0000000000002226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Della Barba G. Different patterns of confabulations. Cortex. 1993;29:567–581. doi: 10.1016/s0010-9452(13)80281-x. [DOI] [PubMed] [Google Scholar]
- Delli Pizzi S., Maruotti V., Taylor J.P., Franciotti R., Caulo M., Tartaro A., Thomas A., Onofrj M., Bonanni L. Relevance of subcortical visual pathways disruption to visual symptoms in dementia with Lewy bodies. Cortex. 2014;59:12–21. doi: 10.1016/j.cortex.2014.07.003. [DOI] [PubMed] [Google Scholar]
- Delli Pizzi S., Franciotti R., Taylor J.P., Thomas A., Tartaro A., Onofrj M., Bonanni L. Thalamic involvement in fluctuating cognition in dementia with Lewy bodies: magnetic resonance evidences. Cereb. Cortex. 2015;25:3682–3689. doi: 10.1093/cercor/bhu220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeLuca J. Predicting neurobehavioral patterns following anterior communicating artery aneurysm. Cortex. 1993;29:639–647. doi: 10.1016/s0010-9452(13)80287-0. [DOI] [PubMed] [Google Scholar]
- DeLuca J., Cicerone K.D. Confabulation following aneurysm of the anterior communicating artery. Cortex. 1991;27:417–423. doi: 10.1016/s0010-9452(13)80036-6. [DOI] [PubMed] [Google Scholar]
- Dusoir H., Kapur N., Byrnes D.P., McKinstry S., Hoare R.D. The role of diencephalic pathology in human memory disorder. Evidence from a penetrating paranasal brain injury. Brain. 1990;113:1695–1706. doi: 10.1093/brain/113.6.1695. [DOI] [PubMed] [Google Scholar]
- Fernandez H.H., Aarsland D., Fénelon G., Friedman J.H., Marsh L., Tröster A.I., Poewe W., Rascol O., Sampaio C., Stebbins G.T., Goetz C.G. Scales to assess psychosis in Parkinson's disease: critique and recommendations. Mov. Disord. 2008;23:484–500. doi: 10.1002/mds.21875. [DOI] [PubMed] [Google Scholar]
- Fischer R.S., Alexander M.P., D'Esposito M., Otto R. Neuro-psychological and neuroanatomical correlates of confabulation. J. Clin. Exp. Neuropsychol. 1995;17:20–28. doi: 10.1080/13803399508406577. [DOI] [PubMed] [Google Scholar]
- Folstein N.F., Folstein S.E., McHugh P.R. Mini-mental state: a practical method for grading the cognitive state of patients for clinician. J. Psychiatry Res. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Franciotti R., Falasca N.W., Bonanni L., Anzellotti F., Maruotti V., Comani S., Thomas A., Tartaro A., Taylor J.P., Onofrj M. Default network is not hypoactive in dementia with fluctuating cognition: an Alzheimer disease/dementia with Lewy bodies comparison. Neurobiol. Aging. 2013;34:1148–1158. doi: 10.1016/j.neurobiolaging.2012.09.015. [DOI] [PubMed] [Google Scholar]
- Franciotti R., Delli Pizzi S., Perfetti B., Tartaro A., Bonanni L., Thomas A., Weis L., Biundo R., Antonini A., Onofrj M. Default mode network links to visual hallucinations: a comparison between Parkinson's disease and multiple system atrophy. Mov. Disord. 2015;30:1237–1247. doi: 10.1002/mds.26285. [DOI] [PubMed] [Google Scholar]
- Galvin J.E., Price J.L., Yan Z., Morris J.C., Sheline Y.I. Resting bold fMRI differentiates dementia with Lewy bodies vs Alzheimer disease. Neurology. 2011;76:1797–1803. doi: 10.1212/WNL.0b013e31821ccc83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ghika-Schmid F., Bogousslavsky J. The acute behavioral syndrome of anterior thalamic infarction: a prospective study of 12 cases. Ann. Neurol. 2000;48:220–227. [PubMed] [Google Scholar]
- Giovagnoli A.R., Del Pesce M., Mascheroni S., Simoncelli M., Laiacona M., Capitani E. Trail making test: normative values from 287 normal adult controls. Ital. J. Neurol. Sci. 1996;17:305–309. doi: 10.1007/BF01997792. [DOI] [PubMed] [Google Scholar]
- Gold J.J., Squire L.R. The anatomy of amnesia: neurohistological analysis of three new cases. Learn. Mem. 2006;13:699–710. doi: 10.1101/lm.357406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldglass H., Kaplan E. Boston Diagnostic Aphasia Examination; 1983. The Assessment of Aphasia and Related Disorders. [Google Scholar]
- Graff-Radford N.R., Tranel D., Van Hoesen G.W., Brandt J.P. Diencephalic amnesia. Brain. 1990;113:1–25. doi: 10.1093/brain/113.1.1. [DOI] [PubMed] [Google Scholar]
- Greicius M.D., Srivastava G., Reiss A.L., Menon V. Default-mode network activity distinguishes Alzheimer's disease from healthy aging: evidence from functional MRI. Proc. Natl. Acad. Sci. U. S. A. 2004;101:4637–4642. doi: 10.1073/pnas.0308627101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gusnard D.A., Raichle M.E. Searching for a baseline: functional imaging and the resting human brain. Nat. Rev. Neurosci. 2001;2:685–694. doi: 10.1038/35094500. [DOI] [PubMed] [Google Scholar]
- Harding A., Halliday G., Caine D., Kril J. Degeneration of anterior thalamic nuclei differentiates alcoholics with amnesia. Brain. 2000;123:141–154. doi: 10.1093/brain/123.1.141. [DOI] [PubMed] [Google Scholar]
- Heaton R.K. 4th ed. Psycho-logical Assessment Resources; Odessa, FL: 1981. Wisconsin Card Sorting Test Manual. [Google Scholar]
- Jankowski M., Ronqvist K., Tasnov M., Vann S., Wright N., Erichsen J., Aggleton J., O’Mara S. The anterior thalamus provides a subcortical circuit supporting memory and spatial navigation. Front. Syst. Neurosci. 2013;7:45. doi: 10.3389/fnsys.2013.00045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kapur N., Coughlan A.K. Confabulation and frontal lobe dysfunction. J. Neurol. Neurosurg. Psychiatry. 1980;43:461–463. doi: 10.1136/jnnp.43.5.461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karnath H.O., Ferber S., Himmlebach M. Spatial awareness is a function of the temporal not the posterior parietal lobe. Nature. 2001;411:950–953. doi: 10.1038/35082075. [DOI] [PubMed] [Google Scholar]
- Kenny E.R., Blamire A.M., Firbank M.J., O'Brien J.T. Functional connectivity in cortical regions in dementia with Lewy bodies and Alzheimer's disease. Brain. 2012;135:569–581. doi: 10.1093/brain/awr327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein J., Rushworth M., Beherens T., Mackay C., Crespigny A., D'Arceuil H., Johansen-Berg H. Topography of connections between human prefrontal cortex and mediodorsal thalamus studied with diffusion tractography. Neuroimage. 2010;51:555–564. doi: 10.1016/j.neuroimage.2010.02.062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopelman M.D. Two types of confabulation. J. Neurol. Neurosurg. Psychiatry. 1987;50:1482–1487. doi: 10.1136/jnnp.50.11.1482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopelman M.D., Bright P., Fulker H., Hinton N., Morrison A., Verfaellie M. Remote semantic memory in patients with Korsakoff's syndrome and herpes encephalitis. Neuropsychology. 2009;23:144–157. doi: 10.1037/a0014447. [DOI] [PubMed] [Google Scholar]
- Krauth A., Blanc R., Poveda A., Jeanmonod D., Morel A., Székely G. A mean three-dimensional atlas of the human thalamus: generation from multiple histological data. Neuroimage. 2010;49:2053–2062. doi: 10.1016/j.neuroimage.2009.10.042. [DOI] [PubMed] [Google Scholar]
- Laureno R. Nutritional cerebellar degeneration, with comments on its relationship to Wernicke disease and alcoholism. Handb. Clin. Neurol. 2012;103:175–187. doi: 10.1016/B978-0-444-51892-7.00010-3. [DOI] [PubMed] [Google Scholar]
- Mair W.G., Warrington E.K., Weiskrantz L. Memory disorder in Korsakoff's psychosis: a neuropathological and neuropsychological investigation of two cases. Brain. 1979;102:749–783. doi: 10.1093/brain/102.4.749. [DOI] [PubMed] [Google Scholar]
- Markowitsch H.J. Diencephalic amnesia: a reorientation towards tracts? Biobehav. Rev. 1983;7:35–43. [Google Scholar]
- Markowitsch H.J. Memory and amnesia. In: Mesulam M.M., editor. Principles of Cognitive and Behavioral Neurology. Oxford Univ Press; New York: 2000. pp. 257–293. [Google Scholar]
- Markowitsch H.J., Cramon D.Y., Schuri U. Mnestic performance profile of a bilateral diencephalic infarct patient with preserved intelligence and severe amnestic disturbance. J. Clin. Exp. Neuropsychol. 1993;15:627–657. doi: 10.1080/01688639308402586. [DOI] [PubMed] [Google Scholar]
- Mayes A.R., Meudell P.R., Mann D., Pickering A. Location of lesions in Korsakoff's syndrome: neuropsychological and neuropathological data on two patients. Cortex. 1988;24:367–383. doi: 10.1016/s0010-9452(88)80001-7. [DOI] [PubMed] [Google Scholar]
- Mercer B., Wapner W., Gardner H., Benson D.F. A study of confabulation. Arch. Neurol. 1977;34:429–433. doi: 10.1001/archneur.1977.00500190063009. [DOI] [PubMed] [Google Scholar]
- Mitchell A., Charbotky S. What does the mediodorsal thalamus do? Front. Syst. Neurosci. 2013;7:37. doi: 10.3389/fnsys.2013.00037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morel A., Magnin M., Jeanmonod D. Multiarchitectonic and stereotactic atlas of the human thalamus. J. Comp. Neurol. 1997;387:588–630. doi: 10.1002/(sici)1096-9861(19971103)387:4<588::aid-cne8>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- Moscovitch M. Confabulation and the frontal system: strategic versus associative retrival in neuropsychological theories of memory. In: Roediger H.L.I., Craik F.I.M., editors. Varieties of Memories and Consciousness. Essays in in the Honour of Endel Tulving. Lawrence Erlbaum Associates; Hillsdale NJ: 1989. pp. 133–160. [Google Scholar]
- Moscovitch M., Melo B. Strategic retrieval and the frontal lobes: evidence from confabulation and amnesia. Neuropsychologia. 1997;35:1017–1034. doi: 10.1016/s0028-3932(97)00028-6. [DOI] [PubMed] [Google Scholar]
- Muller A., Baumgartner R.W., Rohrebach C., Regard M. Persistent Kluver-Bucy syndrome after bilateral thalamic infarction. Neurology. 1999;41:450–452. [PubMed] [Google Scholar]
- Novelli G., Papagno C., Capitani E., Laiacona M. Tre test clinici di ricerca e produzione lessicale. Taratura su sogetti normali. Arch. Psicol. Neurol. Psichiatr. 1986 [Google Scholar]
- Nys G.M., van Zandvoort M.J., Roks G., Kappelle L.J., de Kort P.L., de Haan E.H. The role of executive functioning in spontaneous confabulation. Cogn. Behav. Neurol. 2004;17:213–218. [PubMed] [Google Scholar]
- Orsini A., Grossi D., Capitani E., Laiacona M., Papagno C., Vallar G. Verbal and spatial immediate memory span: normative data from 1355 adults and 1112 children. Ital. J. Neurol. Sci. 1987;8:539–548. doi: 10.1007/BF02333660. [DOI] [PubMed] [Google Scholar]
- Parnetti L., Tiraboschi P., Lanari A., Peducci M., Padiglioni C., D'Amore C., Pierguidi L., Tambasco N., Rossi A., Calabresi P. Cerebrospinal fluid biomarkers in Parkinson's disease with dementia and dementia with Lewy bodies. Biol. Psychiatry. 2008;64:850–855. doi: 10.1016/j.biopsych.2008.02.016. [DOI] [PubMed] [Google Scholar]
- Patenaude B., Smith S.M., Kennedy D.N., Jenkinson M. A Bayesian model of shape and appearance for sub-cortical. Brain. 2011;56:907–922. doi: 10.1016/j.neuroimage.2011.02.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peraza L.R., Kaiser M., Firbank M., Graziadio S., Bonanni L., Onofrj M., Colloby S.J., Blamire A., O'Brien J., Taylor J.P. fMRI resting state networks and their association with cognitive fluctuations in dementia with Lewy bodies. Neuroimage Clin. 2014;4:558–565. doi: 10.1016/j.nicl.2014.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perren F., Clarke S., Bogousslavsky J. The syndrome of combined polar and paramedian thalamic infarction. Arch. Neurol. 2005;62:1212–1216. doi: 10.1001/archneur.62.8.1212. [DOI] [PubMed] [Google Scholar]
- Ptak R., Schnider A. Confabulations after orbitofrontal damage: the role of temporal context confusion and self monitoring. Neurocase. 1999;5:243–250. [Google Scholar]
- Ptak R., Birtoli B., Imboden H., Hauser C., Weis J., Schnider A. Hypothalamic amnesia with spontaneous confabulations: a clinicopathologic study. Neurology. 2001;56:1597–1600. doi: 10.1212/wnl.56.11.1597. [DOI] [PubMed] [Google Scholar]
- Schnider A. Spontaneous confabulation, reality monitoring, and the limbic system—a review. Brain Res. Brain Res. Rev. 2001;36:150–160. doi: 10.1016/s0165-0173(01)00090-x. [DOI] [PubMed] [Google Scholar]
- Schnider A. Spontaneous confabulation and the adaptation of thought to ongoing reality. Nat. Rev. Neurosci. 2003;4:662–671. doi: 10.1038/nrn1179. [DOI] [PubMed] [Google Scholar]
- Schnider A., von Däniken C., Gutbrod K. The mechanisms of spontaneous and provoked confabulations. Brain. 1996;119:1365–1375. doi: 10.1093/brain/119.4.1365. [DOI] [PubMed] [Google Scholar]
- Schnider A., Gutbrod K., Hess C.W., Schroth G. Memory without context: amnesia with confabulations after infarction of the right capsular genu. J. Neurol. Neurosurg. Psychiatry. 1996;61:186–193. doi: 10.1136/jnnp.61.2.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnider A., Bonvallat J., Emond H., Leemann B. Reality confusion in spontaneous confabulation. Neurology. 2005;65:1117–1119. doi: 10.1212/01.wnl.0000178900.37611.8d. [DOI] [PubMed] [Google Scholar]
- Shine J.M., Muller A.J., O′Callaghan C., Hornberger M., Halliday G.M., Lewis S.J.G. Abnormal connectivity between the default mode and the visual system underlies the manifestation of visual hallucinations in Parkinson's disease: a task-based fMRI study. NPJ Park. Dis. 2015:5003. doi: 10.1038/npjparkd.2015.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith S.M., Jenkinson M., Woolrich M.W., Beckmann C.F., Behrens T.E., Johansen-Berg H., Bannister P.R., De Luca M., Drobnjak I., Flitney D.E., Niazy R.K., Saunders J., Vickers J., Zhang Y., De Stefano N., Brady J.M., Matthews P.M. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23:S208–S219. doi: 10.1016/j.neuroimage.2004.07.051. [DOI] [PubMed] [Google Scholar]
- Spinnler, H., Tognoni, G. Gruppo Iitaliano per lo studio neuropsicologico dell'invecchiamento. Standardizzazione e Taratura Italiana di test neuropsicologici. Masson Italia Periodici, 7 198. 1987 [PubMed]
- Turner M., Cipolotti L., Yousri T.A., Shallice T. Confabulations: damage to a specific inferior-medial prefrontal system. Cortex. 2008;44:637–648. doi: 10.1016/j.cortex.2007.01.002. [DOI] [PubMed] [Google Scholar]
- Van der Horst L. Uber die Psychologie des Korsakowsyndroms. Monatsschr. Psychiatr. Neurol. 1932;83:65–84. [Google Scholar]
- Van der Werf Y.D., Witter M.P., Uylings H.B., Jolles J. Neuropsychology of infarctions in the thalamus: a review. Neuropsychologia. 2000;38:613–627. doi: 10.1016/s0028-3932(99)00104-9. [DOI] [PubMed] [Google Scholar]
- Victor M., Adamds R.D., Collins G.H. The Wernicke Korsakoff syndrome. In: Vinken P.J., Bruyn G.W., editors. Handbook of Clinical Neurology. Blackwell Scientific; Oxford: 1971. pp. 243–270. [Google Scholar]
- Yoneoka Y., Takeda N., Inoue A., Ibuchi Y., Kumagai T., Sugai T., Takeda K., Ueda K. Acute Korsakoff syndrome following mammillothalamic tract infarction. AJNR Am. J. Neuroradiol. 2004;25:964–968. [PMC free article] [PubMed] [Google Scholar]
- Zhang D., Snyder A.Z., Shimony J.S., Fox M.D., Raichle M.E. Noninvasive functional and structural connectivity mapping of the human thalamocortical system. Cereb. Cortex. 2010;20:1187–1194. doi: 10.1093/cercor/bhp182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou J., Greicius M.D., Gennatas E.D., Growdon M.E., Jang J.Y., Rabinovici G.D., Kramer J.H., Weiner M., Miller B.L., Seeley W.W. Divergent network connectivity changes in behavioural variant frontotemporal dementia and Alzheimer's disease. Brain. 2010;133:1352–1367. doi: 10.1093/brain/awq075. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1.