

SUMMARY
PCSK9 is a proprotein convertase which is involved in the degradation of low-density lipoprotein (LDL) receptors in the liver.
Mutations in the PCSK9 gene cause familial hypercholesterolaemia in a subset of patients by reducing the number of LDL receptors on the surface of hepatocytes. This decreases their ability to clear LDL cholesterol from plasma.
Conversely, other PCSK9 mutations result in unusually low concentrations of plasma LDL cholesterol and a reduced risk of atherosclerotic disease.
Blocking the activity of PCSK9 with monoclonal antibodies reduces the degradation of LDL receptors and increases the clearance of LDL cholesterol.
An injection of PCSK9-specific antibody suppresses LDL-cholesterol concentrations for several weeks.
Introduction
The 1985 Nobel Prize for Physiology or Medicine was awarded to Michael Brown and Joseph Goldstein for their research into the link between cholesterol metabolism and coronary artery disease.1 This research increased our understanding of the pathophysiology of disorders such as familial hypercholesterolaemia, and paved the way for important therapies like statins (HMG-CoA reductase inhibitors). They found that the low-density lipoprotein (LDL) receptor, expressed primarily in the liver, was responsible for clearing LDL particles from plasma.
Statins decrease the intracellular concentration of cholesterol in the liver. This increases the expression of LDL receptors and more LDL cholesterol is removed from the circulation (Fig. 1).
Fig. 1.
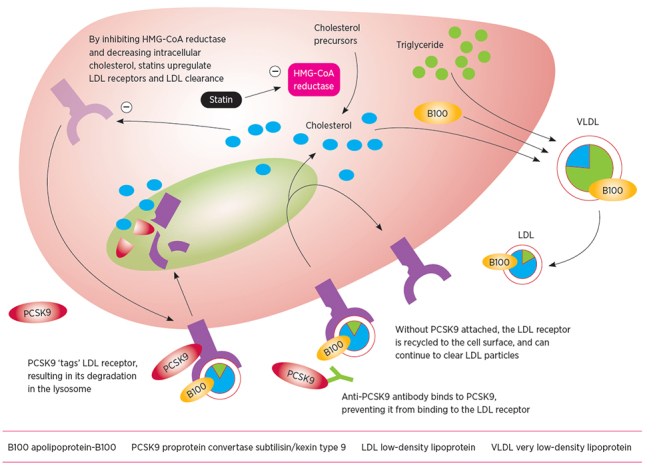
- Mechanism of action of statins and anti-PCSK9 monoclonal antibodies
Proprotein convertases
Proprotein convertases are a family of enzymes involved in converting precursors of secretory proteins, such as hormones, enzymes and receptors, into bioactive molecules at their intended target tissue. These enzymes are part of regulatory pathways that help the body to maintain homeostasis.
PCSK9
PCSK9 (proprotein convertase subtilisin/kexin type 9) was first described in 2003 (Fig. 2).2 In its active form, PCSK9 regulates cell surface receptors, in particular the LDL receptor. The enzyme encoded by the PCSK9 gene is primarily expressed in the liver.
Fig. 2.
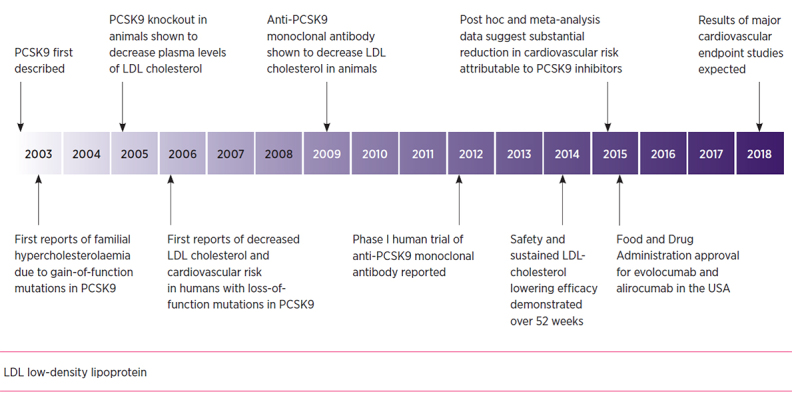
- Timeline of developments in the history of PCSK9
Most cases of familial hypercholesterolaemia are due to mutations resulting in defective LDL receptors, with others caused by defects in the ligand for the LDL receptor, apolipoprotein-B100. Inherited ‘gain-of-function’ mutations in the PCSK9 gene have recently also been found to cause familial hypercholesterolaemia. This is characterised by very high plasma concentrations of LDL cholesterol and associated with premature atherosclerotic cardiovascular disease.3 Conversely, ‘loss-of-function’ PCSK9 mutations result in unusually low concentrations of plasma LDL cholesterol. People with these mutations have a markedly reduced lifetime risk of atherosclerotic cardiovascular disease.4
PCSK9 circulates in three main forms:
mature, monomeric protein, which circulates exclusively in an LDL-bound form
multimeric, self-associated form, which probably has increased activity
furin-cleaved, inactive fragment.
Some PCSK9 mutations result in changes to the self-association or furin-mediated cleavage of PCSK9. These mutations lead to gain or loss of function.5
PCSK9 is cleared from the circulation by the LDL receptor. It is then cleaved inside hepatocytes (Fig. 1).
Role of PCSK9
PCSK9 regulates the degradation of the LDL receptor in response to cholesterol concentrations within the cell (Fig. 1). PCSK9 binds to an extracellular part of the LDL receptor. Apolipoprotein-B100, the structural protein of LDL and ligand for the LDL receptor, binds to a different site on the LDL receptor.
After the LDL receptor is internalised into the hepatocyte, it is trafficked to a lysosome, where it can be either degraded or recycled back to the surface of the hepatocyte. PCSK9 prevents the LDL receptor from forming a closed conformation, making the receptor susceptible to enzymatic degradation.6 LDL receptors without PCSK9 bound to them are therefore more likely to be recycled to the cell surface.
Although animal models suggest that PCSK9 has other roles in cholesterol metabolism aside from the regulation of LDL-receptor recycling, this has not been borne out in the clinical setting in humans. In LDL-receptor knockout mice, LDL-cholesterol concentrations are increased by PCSK9 administration or overexpression, despite the absence of LDL receptors as a clearance pathway.7,8 However, this finding is inconsistent with that in humans with LDL-receptor-negative familial hypercholesterolaemia, in whom blocking the action of PCSK9 does not decrease plasma concentrations of LDL cholesterol.9
Animal studies have suggested roles for PCSK9 in non-hepatic tissue. These include intestinal and adipocyte lipid metabolism, development of atherosclerotic plaques and inflammation, apoptotic cell death, and regulation of blood pressure and glycaemia.5 Clinically significant roles of PCSK9 other than in cholesterol metabolism have not been identified or emerged in the form of unexpected adverse effects despite thousands of patients being treated with anti-PCSK9 antibodies.
PCSK9 inhibition
Inhibiting PCSK9 means that more LDL receptors will be recycled to the surface of the cell. This should increase the clearance of LDL cholesterol from the circulation.
Various approaches to the pharmacological inhibition of PCSK9 have been investigated. Molecules that prevent the formation of PCSK9 include antisense oligonucleotides and small interfering RNAs. Molecules that bind to mature PCSK9, preventing it from interacting with LDL receptors, include the small adnectin polypeptides and monoclonal antibodies.5
The anti-PCSK9 monoclonal antibodies are of most therapeutic interest and are currently in phase III trials. Details of their binding sites have not been fully disclosed, but earlier monoclonal antibodies are known to bind at or near PCSK9's binding site for the LDL receptor. In pre-clinical studies this sterically inhibits the interaction of PCSK9 with the LDL receptor.10 Blocking the binding of PCSK9 to the LDL receptor reduces the degradation of the receptor. This markedly increases the clearance of LDL and substantially lowers plasma LDL cholesterol, as well as apolipoprotein-B100 (Fig. 1).
Consistent with the long plasma half-life of monoclonal antibodies, a single dose of an anti- PCSK9 antibody can suppress the plasma LDL-cholesterol concentration for several weeks. Repeated injections cause a sustained reduction of about 50–70% from baseline, as monotherapy or when added to a statin.11-13
Lipoprotein(a)
PCSK9 inhibition also decreases the plasma concentrations of lipoprotein(a) (Lp(a)) by around 20–30%.11,13 This particle is similar in size and cholesterol content to LDL. Unlike LDL, its apolipoprotein-B100 moiety is covalently linked to apolipoprotein(a), a potentially prothrombotic apolipoprotein with sequence similarity to plasminogen. Genetic and epidemiological studies suggest a causal association between Lp(a) and the risk of atherosclerotic cardiovascular disease.14
How PCSK9 inhibitors lower Lp(a) concentrations is unknown and warrants further research. Lp(a) is not currently understood to be cleared by the LDL receptor, and statins, which upregulate the LDL receptor, do not substantially lower plasma concentrations of Lp(a). However, recent in vitro studies have suggested that the LDL receptor may indeed have a role in Lp(a) clearance.15
Conclusion
The story of PCSK9 since its discovery just over a decade ago is an important case study in translating research into practice. PCSK9-inhibiting therapies have efficacy in lowering LDL cholesterol which could decrease the risk of atherosclerotic cardiovascular disease, particularly in high-risk patients. They could reduce the need for radical therapies such as lipoprotein apheresis in patients with severe heterozygous familial hypercholesterolaemia, and homozygous familial hypercholesterolaemia with residual LDL-receptor function.
Footnotes
Gerald Watts has received honoraria for advisory boards and research grants from Sanofi and Amgen.
REFERENCES
- 1.Brown MS, Goldstein JL. A receptor-mediated pathway for cholesterol homeostasis. Science 1986;232:34-47. 10.1126/science.3513311 [DOI] [PubMed] [Google Scholar]
- 2.Seidah NG, Benjannet S, Wickham L, Marcinkiewicz J, Jasmin SB, Stifani S, et al. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiation. Proc Natl Acad Sci USA 2003;100:928-33. 10.1073/pnas.0335507100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abifadel M, Varret M, Rabès JP, Allard D, Ouguerram K, Devillers M, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet 2003;34:154-6. 10.1038/ng1161 [DOI] [PubMed] [Google Scholar]
- 4.Cohen JC, Boerwinkle E, Mosley TH, Jr, Hobbs HH. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med 2006;354:1264-72. 10.1056/NEJMoa054013 [DOI] [PubMed] [Google Scholar]
- 5.Page MM, Stefanutti C, Sniderman A, Watts GF. Recent advances in the understanding and care of familial hypercholesterolaemia: significance of the biology and therapeutic regulation of proprotein convertase subtilisin/ kexin type 9. Clin Sci (Lond) 2015;129:63-79. 10.1042/CS20140755 [DOI] [PubMed] [Google Scholar]
- 6.Leren TP. Sorting an LDL receptor with bound PCSK9 to intracellular degradation. Atherosclerosis 2014;237:76-81. 10.1016/j.atherosclerosis.2014.08.038 [DOI] [PubMed] [Google Scholar]
- 7.Tavori H, Fan D, Blakemore JL, Yancey PG, Ding L, Linton MF, et al. Serum proprotein convertase subtilisin/kexin type 9 and cell surface low-density lipoprotein receptor: evidence for a reciprocal regulation. Circulation 2013;127:2403-13. 10.1161/CIRCULATIONAHA.113.001592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sun H, Samarghandi A, Zhang N, Yao Z, Xiong M, Teng BB. Proprotein convertase subtilisin/kexin type 9 interacts with apolipoprotein B and prevents its intracellular degradation, irrespective of the low-density lipoprotein receptor. Arterioscler Thromb Vasc Biol 2012;32:1585-95. 10.1161/ATVBAHA.112.250043 [DOI] [PubMed] [Google Scholar]
- 9.Stein EA, Honarpour N, Wasserman SM, Xu F, Scott R, Raal FJ. Effect of the proprotein convertase subtilisin/kexin 9 monoclonal antibody, AMG 145, in homozygous familial hypercholesterolemia. Circulation 2013;128:2113-20. 10.1161/CIRCULATIONAHA.113.004678 [DOI] [PubMed] [Google Scholar]
- 10.Chan JC, Piper DE, Cao Q, Liu D, King C, Wang W, et al. A proprotein convertase subtilisin/kexin type 9 neutralizing antibody reduces serum cholesterol in mice and nonhuman primates. Proc Natl Acad Sci USA 2009;106:9820-5. 10.1073/pnas.0903849106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Robinson JG, Farnier M, Krempf M, Bergeron J, Luc G, Averna M, et al. ODYSSEY LONG TERM Investigators . Efficacy and safety of alirocumab in reducing lipids and cardiovascular events. N Engl J Med 2015;372:1489-99. 10.1056/NEJMoa1501031 [DOI] [PubMed] [Google Scholar]
- 12.Ballantyne CM, Neutel J, Cropp A, Duggan W, Wang E, Plowchalk D, et al. Efficacy and safety of bococizumab (RN316/PF-04950615), a monoclonal antibody against proprotein convertase subtilisin/kexin type 9 in statin-treated hypercholesterolemic subjects: results from a randomized, placebo-controlled, dose-ranging study (NCT: 01592240). J Am Coll Cardiol 2014;63 Suppl:A1374 10.1016/S0735-1097(14)61374-7 [DOI] [Google Scholar]
- 13.Raal FJ, Giugliano RP, Sabatine MS, Koren MJ, Langslet G, Bays H, et al. Reduction in lipoprotein(a) with PCSK9 monoclonal antibody evolocumab (AMG 145): a pooled analysis of more than 1,300 patients in 4 phase II trials. J Am Coll Cardiol 2014;63:1278-88. 10.1016/j.jacc.2014.01.006 [DOI] [PubMed] [Google Scholar]
- 14.Koschinsky M, Boffa M. Lipoprotein(a) as a therapeutic target in cardiovascular disease. Expert Opin Ther Targets 2014;18:747-57. 10.1517/14728222.2014.920326 [DOI] [PubMed] [Google Scholar]
- 15.Romagnuolo R, Scipione CA, Boffa MB, Marcovina SM, Seidah NG, Koschinsky ML. Lipoprotein(a) catabolism is regulated by proprotein convertase subtilisin/kexin type 9 through the low density lipoprotein receptor. J Biol Chem 2015;290:11649-62. 10.1074/jbc.M114.611988 [DOI] [PMC free article] [PubMed] [Google Scholar]