

Abstract
[Purpose] Clarification of the differences in the compression volume of the lungs by the heart (CVLH) between postures may facilitate the selection of optimal postures in respiratory care. Determining CVLH in the supine, semi-prone (Sim’s position), and side-lying positions was the aim of this study. [Subjects and Methods] Eight healthy volunteers (six males, two females; mean age, 29.0 ± 9.2 years) were enrolled in the study. Measurements were performed in the supine, right and left semi-prone, and right and left side-lying positions. semi-prone position was inclined 45° ventrally from the side-lying position. A 1.5-T system with a fast advanced spin-echo sequence in the coronal plane was used for magnetic resonance imaging. [Results] CVLH and heart compression ratio were significantly lower in the semi-prone position on both sides than the other positions. The heart was displaced ventrally when semi-prone and a larger area of the heart leaned on the ventral chest wall, localizing compression to part of the ventral region of the dependent lung. [Conclusion] The region of lungs compressed by the heart is reduced in the semi-prone position due to ventral displacement of the heart. These results suggest that maintaining expansion of the dependent lung is easier in the semi-prone position.
Key words: Semi-prone, Lung volume, Compression by heart
INTRODUCTION
In respiratory care, the position of the patient is changed to improve ventilation-perfusion, increase lung volume, and facilitate mucociliary clearance1). The shape of the mediastinal organs, such as the heart, and the spatial positional relationships between the lungs and other contents of the mediastinum are affected by changes in position2). The gradient in regional lung volume is explained by the gradient in pleural pressure. Regional differences in pleural pressure are attributed to three factors: the weight of the lungs, differences between the shape of the lung tissue and surrounding pleural space, and compression of the lungs by both the heart3) and abdominal pressure4). The gradient of pleural pressure is increased by the heart’s compression of the lung. Transpulmonary pressure at the compression site is thus about 3 cmH2O lower than at other areas of the lungs, and lung expansion is reduced5).
It has been suggested by Albert and Hubmayr that the relative compression volume of the lungs by the heart (CVLH) was smaller in the prone position than in the supine position6). This has been considered one of the factors contributing to improved ventilation of the dorsal lung when placing a patient with acute respiratory distress syndrome into a prone position. However, CVLH has not been clarified for the side-lying position (SL) or semi-prone position (Sim’s position: SP). Clarification of the differences in CVLH between these postures may thus facilitate the selection of optimal postures in respiratory care.
The purpose of this study was to determine CVLH in the supine position, SP, and SL.
SUBJECTS AND METHODS
Eight healthy volunteers (six males, two females; mean age, 29.0 ± 9.2 years; mean height, 166.4 ± 9.3 cm; mean body weight, 59.3 ± 8.8 kg) were enrolled in the study. No subjects had any history of pulmonary or cardiovascular disease. Prior to participation in the study, written informed consent was obtained from all subjects and the study was approved by the Ethics Committee of Ibaraki Prefectural University of Health Sciences (Number: 441).
Measurements were performed in the supine position, right and left SL, and right and left SP. The SP was inclined 45° ventrally from the SL. Magnetic resonance imaging (MRI) was performed using a 1.5-T system (Excelart Vantage 1.5 T; Toshiba Medical Systems, Otawara, Japan). MRI was performed using the fast advanced spin-echo method in the coronal plane, covering the entire thoracic cavity. Scan parameters were as follows: repetition time, 191 ms; echo time, 4.8 ms; number of signal averages, 1; and slice thickness, 10 mm. MRI scanning for 30 s produced 17 slices. Subjects assumed each position and were instructed to hold their breath for 30 s at end-tidal expiratory lung volume.
Using ImageJ software (Rasband, W.S., ImageJ, U.S. National Institutes of Health, Bethesda, MA, http://imagej.nih.gov/ij/, 1997–2014), images from the MRI were analyzed. As an indicator of compression of the lungs by the heart, CVLH and the heart compression ratio (HC ratio) were calculated.
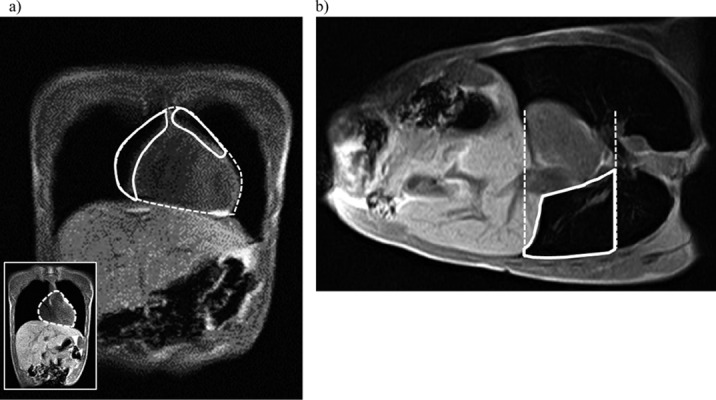
In the supine position, an image was selected that reflected the largest heart area. The heart border was then checked visually and the outline of the heart was traced. This tracing of the heart was superimposed over all underlying images. Lung areas that overlapped with this superimposed heart were considered to represent areas of lung compressed by the heart (Fig. 1a). The sum of these overlapping lung areas was taken as the CVLH.
Fig. 1.
MRI image analysis using Image J
a) In the supine position, an image that reflects the largest heart was selected (lower left). The heart border was checked visually and the outline of the heart was traced (dashed line). This tracing of the heart was superimposed over all underlying images. Lung areas that overlapped with this superimposed heart (solid line) were considered to represent the area of lung compressed by the heart. The sum of these overlapping lung areas was taken as the compression volume of the lung by the heart (CVLH). b) In the side -lying position, a vertical line was drawn from the upper and lower edges of the heart (dash lines). The dependent lung area between the two vertical lines (solid line) was defined as the area of lung compressed by the heart. The sum of these compressed lung areas on all images was then used as the CVLH.
In the SL, vertical lines were drawn from the upper and lower edges of the heart. The dependent lung area between the two vertical lines was defined as the area of lung compressed by the heart (Fig. 1b). The sum of these compressed lung areas on all images was then used as the CVLH. Unlike in the SL, the lower part of the lung in the SP is not compressed in coronal slices. A 3-dimensional image was therefore created from the coronal slices using ImageJ software. Vertical images in the SP, as a position inclined 45° ventrally, were created from the 3-dimensional image, and then CVLH was calculated in the same way as with the SL.
The HC ratio was calculated by dividing CVLH by total lung volume. To determine the lung area of each slice, the lung border was checked visually and the outline of the lung was traced. The total lung volume was calculated as the sum of lung areas from the 17 slices.
For statistical analysis, position differences were first tested using one-way analysis of variance, followed by the Student-Newman-Keuls test to determine differences between each level of significance (IBM SPSS 20). For statistical processing, a risk function value of <5% was fixed as the level of significance.
RESULTS
The CVLH and HC ratios in each of the five positions are summarized in Table 1. CVLH was significantly lower in the right and left SP than in the other three positions. CVLH was significantly lower in the left SL than in the supine position or right SL (Table 1). The HC ratio was significantly lower in the right and left SP than in the other three positions. The HC ratio was significantly lower in left SL than in the supine position or right SL. The HC ratio was significantly higher in right SL than in the supine position (Table 1).
Table 1. CVLH and HC ratio in the five positions.
| Supine | Rt SL | Lt SL | Rt SP | Lt SP | |
|---|---|---|---|---|---|
| CVLH (cm3) | 304.0 ± 66.4 | 363.9 ± 97.3 | 218.8 ± 53.3*†† | 102.7 ± 34.4**††## | 90.9 ± 71.6**††## |
| HC ratio (%) | 10.1 ± 2.6 | 12.2 ± 2.0* | 7.4 ± 1.0**†† | 2.1 ± 1.1**††## | 1.4 ± 1.2**††## |
N=8. Values are given as mean ± SE. *p<0.05 vs. supine; **p<0.01 vs. supine; ††p<0.01 vs. Rt SL; ##p<0.05 vs. Lt SL. Lt: left; Rt: right; SL: side lying; SP: semi-prone; CVLH: compression volume of the lungs by the heart; HC ratio: heart compression ratio
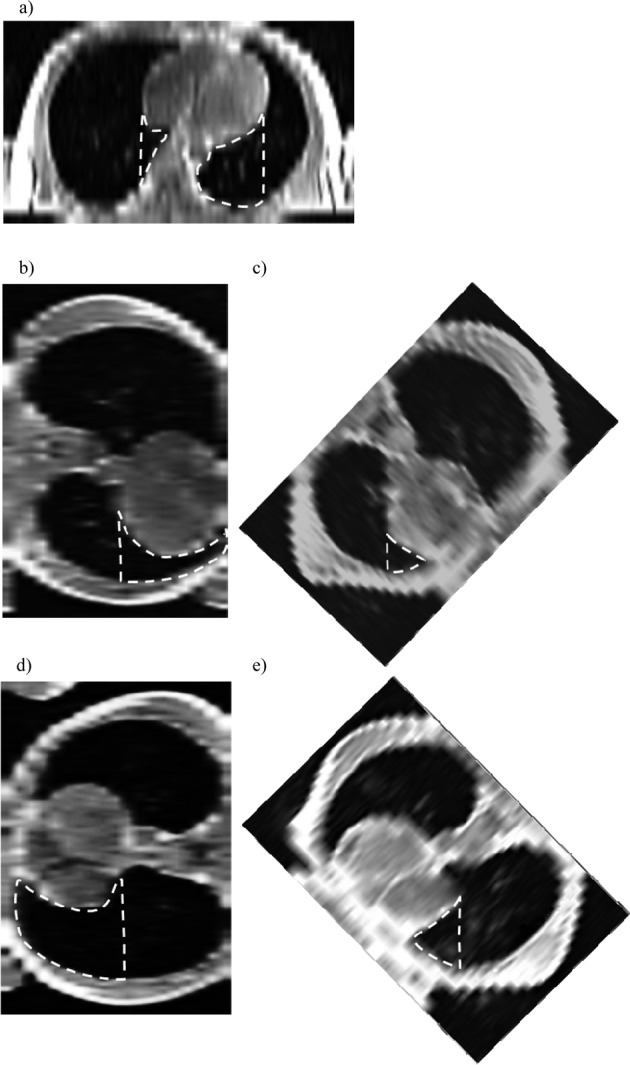
Figure 2 shows the region compressed by the heart in the horizontal plane with the largest heart shadow. The region compressed by the heart was mainly the dorsomedial region of the left lung in the supine position, and the ventral region of the dependent lung in the SL. In all subjects, displacement of the heart downward was greater in the left SL than right SL. The heart was displaced ventrally by gravity in the SP and a larger area of the heart leaned on the ventral chest wall. The region compressed by the heart in the SP was thus localized to part of the ventral region of the dependent lung (Fig. 2).
Fig 2.
The region compressed by the heart in the horizontal plane
a) supine; b) left side lying; c) left semi-prone; d) right side lying; e) right semi-prone. Dashed line encloses the region compressed by the heart.
DISCUSSION
The present results showed that the CVLH and HC ratio were significantly lower in the SP than supine position or SL. This finding is likely attributable to the same mechanisms by which the volume of lung compression by the heart is reduced when prone. Ball et al. suggested that prone positioning produced a ventral shift of the heart and great vessels, leading to a much larger area of the heart coming into contact with the anterior chest wall2). Spatial displacement of the heart in the thoracic cavity is a factor contributing to the lower area of compression by the heart when prone7). The SP also produced a ventral shift of the heart due to gravity and the heart leaned on the ventral chest wall. The region of lung compressed by the heart was thus considered to be reduced in the SP because of the ventral displacement of the heart. On the other hand, part of the heart is against the spine and a substantial part lies against the lungs when supine. The dorsal inside region of the left lung was therefore compressed by the heart in the supine position. In addition, the SL produced a downward shift of the heart. As a result, the heart did not lie against the chest wall as in the SP. The area of lung compressed by the heart is therefore larger in the SL than the SP.
Effects of compression of the dependent lung by the heart have been inferred from several studies comparing supine and prone positions. Those studies suggested that the gravitational gradients in ventilation, regional Va/Q ratio7), pleural pressure5), and transpulmonary pressure8) were less when prone compared with when supine. This implies that, in the prone posture, alveolar size is more uniform and thus so is the distribution of local lung compliance, resulting in more uniform ventilation. This represents a factor in the ventilatory improvement of the dorsal lung region in the prone position and is generally considered to be an effect of lung compression by the heart9).
Albert and Hubmayr recorded that relative CVLH was 1–4% when prone6). In the present study, the HC ratio was 2.1 ± 1.1% in the right SP and 1.4 ± 1.2% in the left SP. Lung compression by the heart in the SP is therefore as low as when prone. These results suggest that ventilation of the dorsal lung region in the SP may be improved by the same mechanisms that are in effect when prone.
The SL is often used for the purpose of expanding and improving ventilation in the nondependent lung. However, compliance is lower in the SL than when sitting, supine, or prone4), and easy expansion of the dependent lung is not achieved in this position. In particular, expansion of the ventral dependent lung is limited in the SL10). One factor is the compression of the dependent lung by the downward displacement of the heart in the SL4). In the present study, the HC ratio was higher in the right SL than in any other position. Although CVLH and the HC ratio in the left SL were less than in the right SL, the heart was greatly displaced onto the dependent lung. These results suggest that maintaining expansion of the dependent lung is easier in the SP than the SL.
The present study has one primary limitation. The transpulmonary pressures for the regions of lung compressed by the heart were not measured. Differences in compression pressure strength to the lung under the heart between each posture are thus unknown. This issue requires examination in the future.
REFERENCES
- 1.Ota H, Kawai H, Sato M, et al. : Effect of early mobilization on discharge disposition of mechanically ventilated patients. J Phys Ther Sci, 2015, 27: 859–864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ball WS, Wicks JD, Mettler FA, Jr: Prone-supine change in organ position: CT demonstration. AJR Am J Roentgenol, 1980, 135: 815–820. [DOI] [PubMed] [Google Scholar]
- 3.Milic-Emili J: Ventilation distribution. In: Hamid Q, Shannon J, Martin J, (eds.), Physiologic Basis of Respiratory Disease, 1st ed. Hamilton: BC Decker, 2005, pp 133–141. [Google Scholar]
- 4.Washko GR, O’Donnell CR, Loring SH: Volume-related and volume-independent effects of posture on esophageal and transpulmonary pressures in healthy subjects. J Appl Physiol 1985, 2006, 100: 753–758. [DOI] [PubMed] [Google Scholar]
- 5.Hyatt RE, Bar-Yishay E, Abel MD: Influence of the heart on the vertical gradient of transpulmonary pressure in dogs. J Appl Physiol 1985, 1985, 58: 52–57. [DOI] [PubMed] [Google Scholar]
- 6.Albert RK, Hubmayr RD: The prone position eliminates compression of the lungs by the heart. Am J Respir Crit Care Med, 2000, 161: 1660–1665. [DOI] [PubMed] [Google Scholar]
- 7.Henderson AC, Sá RC, Theilmann RJ, et al. : The gravitational distribution of ventilation-perfusion ratio is more uniform in prone than supine posture in the normal human lung. J Appl Physiol 1985, 2013, 115: 313–324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tawhai MH, Nash MP, Lin CL, et al. : Supine and prone differences in regional lung density and pleural pressure gradients in the human lung with constant shape. J Appl Physiol 1985, 2009, 107: 912–920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Prisk GK, Yamada K, Henderson AC, et al. : Pulmonary perfusion in the prone and supine postures in the normal human lung. J Appl Physiol 1985, 2007, 103: 883–894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mase K, Tagami M, Imura S, et al. : Regional lung volume differences between the side-lying and semi-prone positions. J Phys Ther Sci, 2016, 28: 1020–1025. [DOI] [PMC free article] [PubMed] [Google Scholar]