

Abstract
Background
The number of obese children in the US remains high, which is problematic due to the mental, physical, and academic effects of obesity on child health. Data indicate that school-age children, particularly underserved children, experience unhealthy gains in BMI at a rate nearly twice as fast during the summer months. Few efforts have been directed at implementing evidence-based programming to prevent excess weight gain during the summer recess.
Methods
Camp NERF is an 8-week, multi-component (nutrition, physical activity, and mental health), theory-based program for underserved school-age children in grades Kindergarten - 5th coupled with the USDA Summer Food Service Program. Twelve eligible elementary school sites will be randomized to one of the three programming groups: 1) Active Control (non-nutrition, physical activity, or mental health); 2) Standard Care (nutrition and physical activity); or 3) Enhanced Care (nutrition, physical activity, and mental health) programming. Anthropometric, behavioral, and psychosocial data will be collected from child-caregiver dyads pre- and post-intervention. Site-specific characteristics and process evaluation measures will also be collected.
Discussion
This is the first, evidence-based intervention to address the issue of weight gain during the summer months among underserved, school-aged children. Results from this study will provide researchers, practitioners, and public health professionals with insight on evidence-based programming to aid in childhood obesity prevention during this particular window of risk.
Trial Registration
Keywords: Nutrition, Physical activity, Elementary children, Behavioral intervention, Childhood obesity prevention
Background
While recent reports indicate a plateau in the rate of childhood obesity in the United States, the number of obese children remains high [1]. In 2011–2012, obesity affected 17 % of US youth, with 31.8 % being classified as overweight or obese [1]. Significant differences in prevalence of obesity exist between racial, ethnic and age groups. Non-Hispanic black and Hispanic youth are significantly more affected by obesity than their non-Hispanic White and non-Hispanic Asian peers [1]. Additionally, there appears to be a developmental trajectory in prevalence of obesity as 8 % of 2- to 5-year olds, 17.7 % of 6- to 11-year olds, and 20.5 % of 12- to 19-year olds were classified as obese in 2011–2012 [1]. So while it appears that the rise in obesity has tapered off, the prevalence of overweight and obesity among US youth remains concerning due to its devastating consequences, which affect the physical and mental health of children, as well as their academic success [2, 3].
Emerging research has begun to point to particular windows of risk for child weight gain. Troubling data indicate that school-age children experience unhealthy gains in BMI at a rate nearly twice as fast during the summer months when school is out of session compared to the school year [4–10]. African American and Hispanic, minority groups and economically disadvantaged children, subpopulations already at increased risk for obesity, as well as girls, may be particularly vulnerable to unhealthy weight gain during these non-academic months [1]. Limited knowledge of the external factors that lead to altered diet and physical activity during the summer time is available to adequately explain the unfavorable weight gain occurring in many children during this window of risk [11].
The rise and current status of obesity in the US has occurred at such a rapid rate that it cannot solely be attributed to biological changes [12]. While obesity rates have been rising over the past several decades, the US food environment has also been changing drastically, providing convenient access to an abundance of inexpensive, highly palatable, energy-dense foods [13]. Thus, the current prevalence of childhood obesity and demonstrated increase in obesity during the summer months could be a response to children’s increased exposure to the food environment [13], which they have less frequent access to during the school year, and lack of structured physical activity. Schools play a critical role in promoting healthy diet and physical activity behaviors during the academic year [14]. During the summer months, however, children lose access to this structured environment (e.g., provision of healthy snacks and meals; opportunity for structured and unstructured physical activity; nutrition, physical activity, and health related policies and programs).
The United States Department of Agriculture (USDA) aims to provide access to healthy, nutritious meals to children during the summer months through the USDA Summer Food Service Program (SFSP) [15]. Unfortunately, attendance at USDA SFSP sites, especially open sites, and amount of meals served tends to be low. According to the Food Research Action Center, only 15.8 % of free or reduced-cost school lunch participants received lunch in the summer of 2015 nationally [16]. In Ohio, only 10.8 % of free or reduced-cost school lunch participants participated in the SFSP [17]. Several stakeholders have hypothesized that these low numbers are due to a lack of structured programming at the sites to attract children. Few efforts have been directed at designing evidence-based nutrition and physical activity programs to equip underserved children with the necessary knowledge, skills, and other resources to prevent excess weight gain during the summer recess.
Camp Nutrition Education Recreation and Fitness (NERF) is a multi-component, evidence-based nutrition, physical activity, and mental health intervention that is coupled with USDA SFSP open sites in Columbus, Ohio. To our knowledge, this is the first multi-component, evidence-based intervention to address the disproportionate childhood weight gain in underserved children during the summer months. The long-term goal is to develop and implement effective theory-based community nutrition and physical activity interventions for childhood obesity prevention, particularly in underserved minority children, aimed at empowering children to make healthy dietary and physical activity choices and achieve a healthy weight and, ultimately, overall optimal health and wellness. The primary aims of this research project are to:
- Evaluate the efficacy of Camp NERF to improve child nutrition, physical activity, mental health, and anthropometric outcomes.
- Hypothesis 1.1: Diet quality, physical activity and sedentary time, positive and negative affect, BMI z-scores, and waist circumference (WC) z-scores will improve more from baseline to post-intervention among children participating at the Enhanced Care sites compared to Standard Care and Active Control sites.
- Evaluate the efficacy of Camp NERF to improve caregiver self-efficacy for establishing healthy family nutrition and physical activity practices, amount of physical activity, and BMI.
- Hypothesis 2.1: Caregiver self-efficacy scores for establishing healthy family nutrition and physical activity practices, physical activity score, and BMI will improve more from baseline to post-intervention among families participating at the Enhanced Care sites compared to the Standard Care and Active Control sites.
- Evaluate the efficacy of Camp NERF to improve youth mentor nutrition, physical activity, and anthropometric outcomes.
- Hypothesis 3.1: Diet quality, physical activity and sedentary time, positive and negative affect, BMI z-scores, and waist circumference (WC) z-scores will improve among youth mentors from baseline to post-intervention.
Methods
Camp NERF theoretical framework
Commonalities among the relatively few successful community-based childhood obesity prevention efforts include: theoretical framework to the intervention, multi-component strategies, direct or indirect engagement of caregivers, and specific behavioral targets [18]. It has become widely accepted that use of a theoretical framework in the design of behavior change interventions is an essential ingredient for achieving positive outcomes. The Camp NERF intervention is guided by the social ecological model (SEM) and social cognitive theory (SCT) [19–21].
According to the socio-ecological framework, there is a complex interplay of factors at multiple levels of influence that determine a child’s weight status, health, and wellness [22]. A child’s risk for obesity is influenced by personal factors, such as genetics and diet and physical activity behaviors. These personal factors are, in turn, influenced by multiple external layers of influence including caregiver/family practices and behaviors, environmental settings (home, school, community), various organizational sectors (education, government, public health, leisure, recreation), and social norms and values (societal rules that guide attitudes, beliefs, and behaviors, peer influence). The socio-ecological framework provides a theory-based approach to investigating the problem of childhood obesity and an understanding of the deep complexity of the etiology of this disease. It also serves as a useful tool in the design of theory-based behavior change interventions – and underlines the necessity in conducting cross-disciplinary research to effectively diminish the problem of childhood obesity.
The SCT broadly used among community nutrition researchers, proposes that behavior change results from a reciprocal relationship between personal and external factors [20]. An individual needs the personal resources to enact the desired behavior, which includes: knowledge and skills (ability to perform desired behavior); cognitive behavior techniques (goal-setting, problem solving, coping strategies); and self-efficacy (confidence in one’s ability to enact the behavior). Regarding cognitive behavioral techniques, self-control is achieved via goal-setting. When goals are not achieved, alternative skills, such as problem solving and coping strategies can be employed to attain initial goals or set new, more achievable goals [20]. Also worth noting, children and adolescents who develop proficiency in general cognitive behavior techniques experience a sense of personal empowerment. In turn, this alleviates the mental health symptoms associated with overweight and obesity (poor self-concept and symptoms of anxiety and depression), leading to subsequent diet and physical activity related behavior change [23]. Cognitive behavior techniques are either vastly underdeveloped or missing from the curriculum of most childhood obesity prevention interventions [24, 25]. The Camp NERF intervention utilizes two evidence-based curricula that incorporate cognitive behavioral techniques - Coordinated Approaches to Child Health (CATCH) [26] and Creating Opportunities for Personal Empowerment (COPE) [27]. Additionally, goal-setting opportunities strategies are integrated into the Camp NERF curriculum and achievement of goals are tracked with goal-setting necklaces.
Under the SCT, environmental or external factors also play a part in determining behavior. With regards to child diet and physical activity behaviors, examples include: role modeling (caregivers, teachers, peers), availability of healthy meals and snacks, opportunity for indoor or outdoor physical activity and structure provided by daily routines [22]. Due to the complexity of behavior origination and change, the most efficacious interventions have been multi-component in design and included either direct or indirect caregiver engagement. As the nutritional gatekeepers of the household, caregivers play a major role in shaping the eating behaviors of their children and thus must be included as an intervention target [28]. Caregivers help children establish and reinforce target behaviors by role modeling intake of healthy foods, setting expectations for healthy food intake, and making healthy foods available [29]. The same principle holds true for physical activity related behaviors – that is, caregivers heavily influence their child(ren)’s engagement in physical activity and exercise, as well as sedentary and screen time [30]. Thus, caregivers must be involved either directly or indirectly in behavioral interventions directed at the child. The food and physical activity environments, caregivers, and peers are all targets of the Camp NERF intervention.
In sum, due to the inherent complexity of behavior, use of theoretical frameworks, such as the SEM and SCT, are absolutely critical in the design and conduct of behavioral interventions. Please refer to Fig. 1 for the Camp NERF theoretical framework.
Fig. 1.
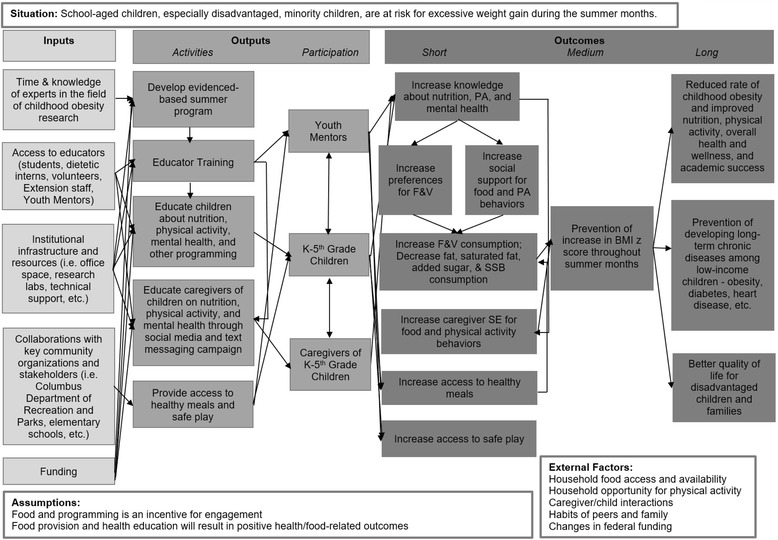
Camp NERF 2015 Theoretical Framework
Research design
Camp NERF is an 8-week pre-test, post-test group site-randomized controlled trial. It is a multi-component nutrition, physical activity, and mental health education intervention coupled with the USDA SFSP, specifically open sites located at public elementary schools. Through daily access to healthy foods, safe play and structured physical activity, along with engagement in an evidence-based health behavior educational curriculum, Camp NERF is designed specifically to prevent unintended, unhealthy weight gain during the summer months in underserved school-aged children. Potential sites were identified by a community partner whose responsibility it is to support SFSP sites in Franklin County, OH, and were considered eligible if they were: 1) an elementary school; 2) a USDA SFSP open site; and 3) lacking structured programming. Twelve sites were identified as meeting these inclusion criteria and will be randomized to one of three treatment or programming groups: 1) Enhanced Care (nutrition, physical activity, and mental health programming); 2) Standard Care (nutrition and physical activity programming); and 3) Active Control (non-nutrition, physical activity, and mental 4H programming). Figure 2 provides an overview of the three treatments for Camp NERF.
Fig. 2.
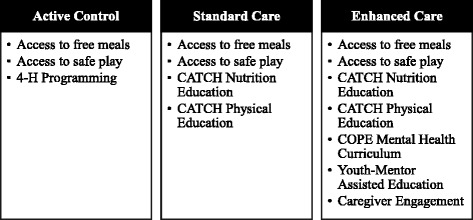
Overview of the Camp NERF Treatments
Power was calculated using change in BMI z-score as the outcome of interest. Based on the results from previous pilot test [31, 32], we assume that between-subject variation is normally distributed with a standard deviation of 1.03 and that between-site variation (nested within treatment group) is negligible. Under these assumptions, recruiting 20 subjects per site (planning for 20 % attrition) provides approximately 70 % power to detect a difference of 0.5 points in change in BMI between the treatment group and either of the two control groups using a one-sided test at alpha = 0.05. The model used is described further in the Data Analysis section.
USDA SFSP open feeding sites operate 5 days a week from mid-June through the beginning of August. Their hours of operation will be approximately 9:00 AM – 3:00 PM, although these times vary slightly by site. Camp NERF program (Enhanced Care, Standard Care, or Active Control) will occur 2 days per week for approximately 4 hours each day. This is expected to equate to 64 h of direct exposure per child, a sufficient dose for eliciting behavior change in the targeted outcomes [33–42]. Table 1 provides an overview of a sample day at an Enhance Care site.
Table 1.
Camp NERF daily curricula delivery schedule at enhanced care sites
| Time | Grades K-2 | Time | Grades 3–5 |
|---|---|---|---|
| 8:30 AM | Arrival; Engage with participants before and during breakfast | 8:30 AM | Arrival; Engage with participants before during breakfast |
| 10:00 AM | Nutrition Education | 10:00 AM | Physical Education |
| 10:00 AM | Discussion | 10:00 AM | Warm-up |
| 10:10 AM | Learning Activity | 10:05 AM | Go Fitness |
| 10:25 AM | Physical Activity | 10:20 AM | Go Activity |
| 10:40 AM | Cool-down | ||
| 10:45 AM | Mental Health | 10:45 AM | Mental Health |
| 11:15 AM | Physical Education | 11:15 AM | Nutrition Education |
| 11:15 AM | Warm-up | 11:15 AM | Discussion |
| 11:20 AM | Go Fitness | 11:25 AM | Learning Activity |
| 11:35 AM | Go Activity | 11:40 AM | Physical Activity |
| 11:55 AM | Cool-down | ||
| 12:00 PM | Lunch; Lunchtime Engagement and Trivia | 12:00 PM | Lunch; Lunchtime Engagement and Trivia |
Participants and recruitment
The target population for Camp NERF is underserved minority children entering kindergarten through fifth grade and their adult caregiver from urban neighborhoods in Columbus, Ohio. Participants will be recruited through a variety of methods including, but not limited to, school announcements, emails, flyers, phone calls, and neighborhood canvassing. Prior to enrollment in the study, a consent form, parental permission form, and assent form will be completed by the caregiver and child, respectively.
Also, data will be collected from high school students who will serve as Youth Mentors for the child participants at the Camp NERF Enhanced Care sites. The Youth Mentors will be recruited through a collaborating partner, the Godman Guild Association that provides internships to high-school aged students during the summer months through Temporary Assistance for Needy Families (TANF) funding. Prior to study enrollment, a parental permission form and assent form will be completed by the caregiver and Youth Mentor, respectively, for those under the age of 18. Youth Mentors 18 years of age or older will complete consent forms prior to enrollment in the study. Individuals who are not interested in enrolling in the study will still be able to participate as Camp NERF Youth Mentors.
Data collection
Data collection training
Data collectors will consist of undergraduate and graduate students from nutrition, public health or other related fields, as well as registered dietitian nutritionists. All data collectors will undergo an 8-hour data collection training, which will include didactic sessions followed by role-playing to practice techniques and become familiar with the instruments. At the end of the 8-week intervention prior to post-test data collection, data collectors will complete a 2-hour review training to reacquaint themselves with the instruments and learn additional post-test data collection feedback surveys.
Impact measures
Child-caregiver dyads and youth mentors will be interviewed at baseline and post-intervention using the Camp NERF Child Assessment Form, Camp NERF Adult Assessment Form, and Camp NERF Youth Mentor Assessment Form, respectively. Each assessment form consists of validated nutrition, physical activity, and mental health questionnaires. Three (2 weekdays and 1 weekend day) 24-hour dietary recalls will be conducted for both the children and youth mentors. Heights, weights, blood pressure, and waist circumference measurements will be taken for the children and youth mentors. Caregivers will self-report height and weight. Table 2 provides the Camp NERF Evaluation Chart and outlines all validated surveys and outcomes measured for participants.
Table 2.
Camp NERF evaluation chart for children, caregivers, and youth mentors
| Outcomes | Goal | Measure | b0 | T1 |
|---|---|---|---|---|
| Child Outcomes | ||||
| Nutrition | ||||
| Food Attitudes and Preferences | Increase preference for fruits and vegetables | Fruit and Vegetable Preferences Domel 1993 85 |
X | X |
| Dietary Intake | Increase quality of diet (increase fruit and vegetable intake (quantity and variety), decrease intake of foods high in solid fats and added sugars; decrease sugar-sweetened beverages) | Caregiver-assisted 24-hour diet recall Burrows et al 2010 86 Baxter et al 2003 87 Baxter et al 2009 88 |
X | X |
| Physical Activity | ||||
| Physical activity level and sedentary time | Increase estimated active time and decrease estimated time in sedentary behavior | 3rd-5th: SPAN questionnaire Hoelscher et al 2010 89 |
X | X |
| Mental Health | ||||
| Self-concept | Increase positive affect | PANAS Survey Laurent et al 1999 90 |
X | X |
| Decrease negative affect | ||||
| Retain positive changes in self-concept | ||||
| Social Support | ||||
| Social Support for Food and Physical Activity Habits | Increase social support for food and physical activity habits | Social Support Scale for Food and Physical Activity Habits | X | X |
| Gadhoke 2015 91 | ||||
| Social Support for Healthy and Unhealthy Eating | Increase social support for healthy eating and decrease social support for unhealthy eating | Social Support Scale for Healthy and Unhealthy Eating Fitzgerlad 2013 92 |
X | X |
| Biometrics | ||||
| Height and Weight | Prevent unhealthy weight gain | Hopkins Road Rod Portable Stadiometer (Height) BalanceFrom High Accuracy Digital Scale (Weight) 2000 CDC sex-specific BMI-for-age growth chart93 |
X | X |
| Waist Circumference | Prevent increase in waist circumference | MyoTape tape measure CDC Waist Circumference Tables 94 |
X | X |
| Blood Pressure | Prevent increase in blood pressure | Panasonic Portable Blood Pressure Monitor NHBLI Standardized Blood Pressure Tables 95 |
X | X |
| Youth Mentor Outcomes | ||||
| Nutrition | ||||
| Food Attitudes and Preferences | Increase preference for fruits and vegetables | Fruit and Vegetable Preferences Domel 1993 85 |
X | X |
| Dietary Intake | Increase quality of diet (increase fruit and vegetable intake (quantity and variety), decrease intake of foods high in solid fats and added sugars; decrease sugar-sweetened beverages) | Youth Mentor reported 24-hour diet recall Lindquist et al 2000 96 |
X | X |
| Physical Activity | ||||
| Physical activity level and sedentary time | Increase estimated active time and decrease estimated sedentary time | SPAN questionnaire Hoelscher et al 2010 89 |
X | X |
| Mental Health | ||||
| Self-concept | Increase positive affect | PANAS Survey Laurent et al 1999 90 |
X | X |
| Decrease negative affect | ||||
| Retain positive changes in self-concept | ||||
| Social Support | ||||
| Social Support for Food and Physical Activity Habits | Increase social support for food and physical activity habits | Social Support Scale for Food and Physical Activity Habits Gadhoke 2015 91 |
X | X |
| Social Support for Healthy and Unhealthy Eating | Increase social support for healthy eating and decrease social support for unhealthy eating | Social Support Scale for Healthy and Unhealthy Eating Fitzgerlad 2013 92 |
X | X |
| Biometrics | ||||
| Height and Weight | Prevent unhealthy weight gain | Hopkins Road Rod Portable Stadiometer (Height) BalanceFrom High Accuracy Digital Scale (Weight) CDC sex-specific BMI-for-age growth chart93 |
X | X |
| Waist Circumference | Prevent increase in waist circumference | MyoTape tape measure CDC Waist Circumference Tables 94 |
X | X |
| Blood Pressure | Prevent increase in blood pressure | Panasonic Portable Blood Pressure Monitor NHBLI Standardized Blood Pressure Tables 95 |
X | X |
| Caregiver Outcomes | ||||
| Nutrition | ||||
| Caregiver Self-Efficacy | Improve caregiver self-efficacy to make healthy choices | Self-efficacy to make healthy choices Bohman 2014 97 |
X | X |
| Dietary Intake; Home Food Environment | Increase purchase and consumption of healthy foods; decrease purchase and consumption of unhealthy foods | Home Food Inventory Fulkerson 2008 98 |
X | X |
| Physical Activity | ||||
| Leisure Time Exercise | Increase engagement in leisure time exercise | Leisure Time Exercise Questionnaire Godin & Shepherd 1985 99 |
X | X |
| Retain positive changes in leisure time exercise | ||||
| Anthropometrics | ||||
| Height and Weight | Prevent unhealthy weight gain | Self-report | X | X |
| Weight | Prevent unhealthy weight gain | Self-report | X | X |
b0 = baseline; beginning of summer
t1 = post-intervention; end of summer
Interviews will be conducted at the home of the participants, the site, or another community location and are estimated to take approximately 30 min, 10 min, and 20 min to complete for the child, caregiver, and youth mentor, respectively. All assessment forms will be data collector-administered, where the data collector will read each question from the assessment form verbatim including all possible responses and record the participants’ response. If the participant provides an ambiguous response, the data collector will ask necessary questions to probe for a specific response. For younger children, caregivers will be asked to assist in completing and verifying responses from the child interview when deemed necessary.
Data analysis
The intervention will be tested by comparing change from baseline to post-intervention in diet quality, physical activity, mental health, and anthropometric outcomes for child participants (hypothesis 1.1) and psychosocial, physical activity, and anthropometric outcomes for adults (hypothesis 2.1). For each outcome variable of interest (Table 2), a mixed effects linear regression model will be fitted with site-type as the primary predictor. Other covariates will include race/ethnicity, income, and attendance, as well as baseline zBMI for all models that do not include weight status as the primary outcome. Using a mixed effects linear regression model allows us to capture the contributions of two sources of variability: (1) a between-site variability and (2) a between-subject or within-site variability. Impact of Camp NERF on Youth Mentors will be tested by comparing change from baseline to post-intervention in diet quality, physical activity, mental health, and anthropometric outcomes (hypothesis 3.1) using multiple linear regression analyses.
Process evaluation and environmental assessment
A Camp NERF Site Environmental Assessment Form was developed for this study and will be completed at baseline, mid-intervention (4 weeks), and post-intervention. The purpose of this form is to assess the demographic (i.e. predominant race/ethnicity of the staff at the sites), food environment (i.e. presence of vending machines, concession stands, and healthfulness of available foods), and physical activity environment (i.e. access to a gym, outdoor playground, equipment, etc.) characteristics of the sites. This information will be used in post-hoc analyses to determine if characteristics (i.e., access to a computer room) may have contributed to outcomes.
A Camp NERF Daily Process Evaluation Form was developed for this study and will be completed by trained process evaluators, who will not be involved with intervention implementation. This form assesses feasibility, fidelity, and acceptability of the intervention programming, assessment of food served, adherence to the USDA SFSP menus, and participant attendance.
Intervention
Educator training and structure
The Camp NERF counselors will be undergraduate and graduate students in fields related to nutrition, kinesiology, public health, and education. The Camp NERF counselors will complete a 3-day, 24-h training prior to the launch of Camp NERF. The training will begin with an overview of our community partners, the USDA child meal programs, other pertinent issues, e.g., underutilization of the USDA SFSP and unhealthy weight gain during the summer months. Camp NERF Counselors also will be provided with a didactic overview of each of the core components of the Camp NERF program – nutrition, physical activity, and mental health – and will be given an opportunity to practice delivery of these curricula. Additionally, they will undergo training on topics related to education delivery and necessary for work with underserved children, as well as other components of the Camp NERF intervention. Table 3 provides an overview of the Camp NERF training for the Camp Counselors. In addition to the intensive training prior to intervention launch, the Camp NERF Counselors will attend a weekly staff meeting throughout the summer to provide feedback on the lessons from the current week, to coach the staff on improvement of curricula delivery and to practice lessons for the upcoming week.
Table 3.
Camp NERF counselor training overview
| Day 1 | Welcome and Introductions |
| Community Partner Overview | |
| Overview of the USDA SFSP | |
| “The Problem” and Our Place at the Table | |
| How to Keep Kids’ Attention | |
| How to Identify and Report Child Abuse and Neglect | |
| Day 2 | CATCH Nutrition Education Overview |
| Practice CATCH Nutrition Education | |
| 4-H Programming Overview | |
| Practice 4-H Programming | |
| COPE Education Overview | |
| Practice COPE Education | |
| Day 3 | CATCH Physical Education Overview |
| Practice CATCH Physical Education | |
| Caregiver Engagement Overview | |
| Behavioral Economics Strategies Overview | |
| Meet and Greet with Youth Mentors |
Three Camp NERF Counselors will be assigned to each site: One Counselor will serve as the kindergarten through second grade educator, one as the third through fifth grade educator, and one as the process evaluator. The Camp NERF Counselors at the Enhanced Care sites will be assisted by high school-aged adolescents - Camp NERF Youth Mentors - from the neighborhoods in which Camp NERF will be delivered.
Youth mentor-assisted education
The use of peer-led interventions have been utilized among youth in areas pertaining to the use of alcohol, tobacco, illegal drugs, violence, and sexual behavior [43–50]. Data indicate that mentored youth compared to un-mentored youth are less likely to participate in these aforementioned risky behaviors [51, 52] and are more likely to succeed academically [53–56]. Until recent years, use of peers as an intervention strategy to improve nutrition and physical activity, and ultimately weight status, had not been employed, but emerging research has demonstrated positive results for biometric-, nutrition-, and physical activity-related outcomes [43, 56–68]. According to the SCT, self-efficacy is influenced by role modeling the behavior [69]. As such, the peers leading the education may experience positive behavior change as a result of child mentoring. Unfortunately, the educating of peer mentors has been understudied [56, 64, 65, 67, 68].
Youth Mentors from the neighborhoods in which Camp NERF will be implemented will be recruited and will assist in the Camp NERF education delivery at the Enhanced Care sites. The Youth Mentors will undergo a 20-h work-readiness training, as well as will attend the 2-hour weekly Camp NERF staff meetings, where feedback will be provided on the lessons for the current week and the upcoming weeks lessons will be reviewed and practiced. Additionally, professional development topics, such as how to interact with co-workers in the workplace, will be discussed in collaboration with the undergraduate- and graduate-level Camp NERF Counselors.
Child education
Nutrition and physical activity
The Coordinated Approaches to Child Health (CATCH) Kid’s Club Healthy Habits and Nutrition Grades K-2 and Grades 3–5 curriculum and CATCH Kid’s Club Physical Education will be used for the Camp NERF nutrition and physical education components. The original CATCH program was initially implemented and evaluated from 1991–1994 in grades three through five in 96 schools in San Diego, CA, New Orleans, LA, Minneapolis, MN, and Austin, TX. Several positive findings on improvements in eating and physical activity behaviors came from these studies, including increased vigorous physical activity, decreased consumption of dietary fat, and reductions in children at-risk for being overweight and in children being overweight [70–74]. Due to the success of the original trial, the CATCH curriculum has continued to be adapted for and studied in various settings [75–82]. CATCH Kid’s Club is the modified curriculum for the after-school setting and has been shown to be effective in improving nutrition and physical activity knowledge and behaviors and reducing overweight and obesity.
Mental Health
The COPE curriculum will be the mental health component of the Camp NERF curriculum. COPE focuses on the thinking, feeling, behaving triangle and incorporates cognitive behavioral skill building in goal-setting, problem solving, coping, and emotional regulation [25]. The curriculum, originally developed for adolescents and young adults and more recently adapted to the younger audience of school-age children, consists of an introductory session and seven subsequent lessons. The lessons will be introduced and taught on the first day of Camp NERF each week, and the skills practice and review of lesson will be completed on the second day of Camp NERF each week.
4H Programming
In order to assess whether potential differences demonstrated between participants is due to the type of programming delivered, as opposed to mere exposure to daily structured programming, an active control group was chosen for Camp NERF. Thus, the Camp NERF research team worked closely with 4-H Extension Specialists to identify non-nutrition and physical activity related programming suited for our target population. Sixteen lessons from the Cloverbud [83] curriculum will be delivered to participants at the Active Control sites.
Caregiver engagement
The caregiver engagement component will be in the form of a texting program that will utilize a mass messaging platform, social media (Facebook and Instagram), and traditional education materials. Adult caregivers of Camp NERF participants in the Enhanced Care group will be provided the option to receive three text messages each week over the course of the intervention. The first message each week will introduce the main nutrition topic that was presented to their child during programming but will encourage completion of a specific family nutrition goal to be attained by the end of the week. For example, the message preceding the fourth week of programming may read as follows: “Today at Camp NERF, your child learned about healthy fast food items. Are you in for trying healthier items at fast food restaurants? Please reply with ‘Yes’ or ‘No’.” The second message content will consist of either a strategy to assist the caregivers in reaching the weekly goal or educational information related to the topic of the week. The final message will inquire about achievement of the goal-setting challenge proposed at the start of the week.
Social media outlets such as Facebook, Twitter, and Instagram will be offered as an alternative means for caregivers to receive insight on the nutrition topic for the week. Images or videos will be added to the websites for caregivers to view and interact with counselors as well as other caregivers. Nutrition topics will be explored in greater depth, such as links to simple food recipes, news items, and recent educational articles related to the weekly topic.
In addition to the text-messaging and social media campaigns, traditional educational materials also will be disseminated to caregivers at the Enhanced Care sites weekly. These educational materials are adapted from the CATCH Kids Club Healthy Habits and Nutrition curriculum handouts for parents [26]. The handouts are modified to include concepts from the CATCH Physical Education curriculum and the COPE curriculum [26, 27]. Child participants will be given handouts at the end of the week to take home to their caregivers.
Discussion
Despite the recent plateauing in prevalence, the number of obese children remains high, which is problematic due to the negative, short- and long-term health consequences for children [1–3]. Emerging research has indicated the summertime as a particular window of risk for unhealthy weight gain among children, especially underserved, minority children [4–10]. Few efforts have been directed at designing evidence-based nutrition and physical activity programs to equip children with the necessary knowledge, skills, and other resources to prevent excess weight gain during the summer recess.
The purpose of this paper is to describe the aims and research methods of Camp NERF, a multi-component, evidence-based nutrition, physical activity, and mental health intervention coupled with USDA SFSP open sites in Columbus, Ohio to address the disproportionate childhood weight gain in underserved children during the summer months. To our knowledge, Camp NERF is the first evidenced-based nutrition education research study and program to address this issue. This study will fill a critical research void and provide insight for effective programming to address child health during the summer months. The Camp NERF program is coupled with the USDA SFSP and utilized existing systems for implementation, which ensures the future sustainability of the program.
Several challenges or limitations have been identified. Engagement from caregivers in the target population may be a challenge, as it is a common issue with intervention research involving underserved families [84, 85]. However, this study was developed and designed to overcome this barrier. The research team and community collaborators will be present in the participating neighborhoods for several years throughout the development of the project. High-school aged students from the intervention communities will be engaged as Youth Mentors and will assist with education delivery throughout the entirety of the program. Traditional (educational handout materials) and innovative (text messaging and social media) strategies will be utilized to inform parents about the programming and encourage participation. Another limitation is the lack of a true negative control group. Because Camp NERF will be coupled with the USDA SFSP, a federal child nutrition program, the statutory right for participation applies. Ethically, the research team cannot ask children and families to not participate at the open SFSP sites. Additionally, recruitment methods are not designed to seek participants who do not intend to attend the SFSP sites during the summer.
In summary, Camp NERF builds on successful childhood obesity prevention interventions which include nutrition and physical activity components, concurrent knowledge and skill building, coupling of the intervention curriculum to availability of healthy foods, and opportunity for physical activity and play [18, 86]. Studying the impact of such an intervention over the summer months will provide valuable information in tackling a time period during which children may be at increased risk for excessive weight gain.
Acknowledgements
We thank our community collaborators, particularly Children’s Hunger Alliance, Columbus Recreation and Parks Department, and the Godman Guild Association.
Funding
The Aetna Foundation.
Availability of data and material
Not applicable.
Authors’ contributions
CG led the conceptual development of the study with input from LCH, BM, JDG, MF, IE, and JAK. LCH and CG led intervention preparations with assistance from JDG, BM, MF, JAK, and IE. LCH and CG took primary responsibility for writing the manuscript. IE, JDG, JAK, MF, and BM contributed to editing the manuscript. CG, LCH, MF, JDG, IE, JAK, and BM read and approved the final manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by The Ohio State University Behavioral and Social Sciences Institutional Review Board. Parent consent and parent permission, as well as child assent will be received from participants prior to study enrollment.
Contributor Information
Laura C. Hopkins, Email: Hopkins.laurac@gmail.com, Email: Hopkins.774@osu.edu
Mary Fristad, Email: mary.fristad@osumc.edu.
Jacqueline D. Goodway, Email: goodway.1@osu.edu
Ihuoma Eneli, Email: ihuoma.enelia@nationwidechildrenshospital.org.
Chris Holloman, Email: holloman.5@osu.edu.
Julie A. Kennel, Email: kennel.3@osu.edu
Bernadette Melnyk, Email: melnyk.15@osu.edu.
Carolyn Gunther, Email: gunther.22@osu.edu.
References
- 1.Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311(8):806–814. doi: 10.1001/jama.2014.732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Halfon N, Larson K, Slusser W. Associations between obesity and comorbid mental health, developmental, and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad Pediatr. 2013;13(1):6–13. doi: 10.1016/j.acap.2012.10.007. [DOI] [PubMed] [Google Scholar]
- 3.Taras H, Potts-Datema W. Obesity and student performance at school. J Sch Health. 2005;75(8):291–295. doi: 10.1111/j.1746-1561.2005.00040.x. [DOI] [PubMed] [Google Scholar]
- 4.von Hippel PT, Powell B, Downey DB, Rowland NJ. The effect of school on overweight in childhood: gain in body mass index during the school year and during summer vacation. Am J Public Health. 2007;97(4):696–702. doi: 10.2105/AJPH.2005.080754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moreno JP, Johnston CA, Woehler D. Changes in Weight Over the School Year and Summer Vacation: Results of a 5-Year Longitudinal Study. J Sch Health. 2013;83(7):473-7. [DOI] [PubMed]
- 6.Moreno JP, Johnston CA, Chen T-A, et al. Seasonal variability in weight change during elementary school. Obesity (Silver Spring) 2015;23(2):422–428. doi: 10.1002/oby.20977. [DOI] [PubMed] [Google Scholar]
- 7.Kobayashi M, Kobayashi M. The relationship between obesity and seasonal variation in body weight among elementary school children in Tokyo. Econ Hum Biol. 2006;4(2):253–261. doi: 10.1016/j.ehb.2005.08.002. [DOI] [PubMed] [Google Scholar]
- 8.Smith DT, Bartee RT, Dorozynski CM, Carr LJ. Prevalence of overweight and influence of out-of-school seasonal periods on body mass index among American Indian schoolchildren. Prev Chronic Dis. 2009;6(1):A20. [PMC free article] [PubMed] [Google Scholar]
- 9.Baranowski T, O’Connor T, Johnston C, et al. School year versus summer differences in child weight gain: a narrative review. Child Obes. 2014;10(1):18–24. doi: 10.1089/chi.2013.0116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Franckle R, Adler R, Davison K. Accelerated weight gain among children during summer versus school year and related racial/ethnic disparities: a systematic review. Prev Chronic Dis. 2014;11(12):1–10. doi: 10.5888/pcd11.130355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tovar A, Lividini K, Economos CD, Folta S, Goldberg J, Must A. School’s out: what are urban children doing? The Summer Activity Study of Somerville Youth (SASSY) BMC Pediatr. 2010;10:16. doi: 10.1186/1471-2431-10-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sallis JF, Glanz K. Physical activity and food environments: solutions to the obesity epidemic. Milbank Q. 2009;87(1):123–154. doi: 10.1111/j.1468-0009.2009.00550.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378(9793):804–814. doi: 10.1016/S0140-6736(11)60813-1. [DOI] [PubMed] [Google Scholar]
- 14.Briefel RR, Crepinsek MK, Cabili C, Wilson A, Gleason PM. School food environments and practices affect dietary behaviors of US public school children. J Am Diet Assoc. 2009;109(2 Suppl):S91–S107. doi: 10.1016/j.jada.2008.10.059. [DOI] [PubMed] [Google Scholar]
- 15.United States Department of Agriculture Food and Nutrition Service. Summer Food Service Program. http://www.fns.usda.gov/sfsp/sfsp-meals-and-snacks. Accessed 12 Apr 2015.
- 16.Food Research Action Center . Federal Nutrition Programs. 2013. [Google Scholar]
- 17.Food Research and Action Center . Hunger Doesn’t Take a Vacation: Summer Nutrition Status Report. 2016. pp. 1–20. [Google Scholar]
- 18.Contento I, Balch G, Bronner Y, et al. The effectiveness of nutrition education and implications for nutrition education policy, programs, and research: A review of research. J Nutr Educ. 1995;27:280–319.
- 19.Bronfenbrenner U. Ecology of the family as a context for human development: research perspectives. Dev Psychol. 1986;22:723–742. doi: 10.1037/0012-1649.22.6.723. [DOI] [Google Scholar]
- 20.Bandura A. Social Foundations of Thought and Action a Social Cognitive Theory. Engelwood: Prentice Hall; 1986. [Google Scholar]
- 21.Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–1184. doi: 10.1037/0003-066X.44.9.1175. [DOI] [PubMed] [Google Scholar]
- 22.Lytle LA, Seifert S, Greenstein J, McGovern P. How do children’s eating patterns and food choices change over time? Results from a cohort study. Am J Health Promot. 2000;14(4):222-28. [DOI] [PubMed]
- 23.Melnyk BM, Jacobson D, Kelly S, O’Have J, Small L, Mays M. Improving the Mental Health, Healthy Lifestyle Choices, and Physical Health of Hispanic Adolescents: a randomized controlled pilot study. J Sch Health. 2009;79(12):575–584. doi: 10.1111/j.1746-1561.2009.00451.x. [DOI] [PubMed] [Google Scholar]
- 24.Kelly S, Melnyk BM, Belyea M. Predicting physical activity and fruit and vegetable intake in adolescents: a test of the information, motivation, behavioral skills model. Res Nurs Health. 2012;35(2):146–163. doi: 10.1002/nur.21462. [DOI] [PubMed] [Google Scholar]
- 25.Zabinski MF, Daly T, Norman GJ, et al. Psychosocial correlates of fruit, vegetable, and dietary fat intake among adolescent boys and girls. J Am Diet Assoc. 2006;106(6):814–821. doi: 10.1016/j.jada.2006.03.014. [DOI] [PubMed] [Google Scholar]
- 26.Luton S, Berry J. CATCH Kids Club Healthy Habits & Nutrition: An After-School Curriculum for Grades K-5. Hasbrouck Heights: FlagHouse, Inc.; 2011. [Google Scholar]
- 27.Melnyk BM. Creating Opportunities for Personal Empowerment: a 7-Session Cognitive Behavioral Skills Builidng Program for Children. Powell: Cope2Thrive, LLC; 2015. [Google Scholar]
- 28.Bluford D a a, Sherry B, Scanlon KS. Interventions to prevent or treat obesity in preschool children: a review of evaluated programs. Obesity (Silver Spring) 2007;15(6):1356–1372. doi: 10.1038/oby.2007.163. [DOI] [PubMed] [Google Scholar]
- 29.Pearson N, Biddle SJH, Gorely T. Family correlates of fruit and vegetable consumption in children and adolescents: a systematic review. Public Health Nutr. 2009;12(2):267–283. doi: 10.1017/S1368980008002589. [DOI] [PubMed] [Google Scholar]
- 30.Gustafson SL, Rhodes RE. Parental correlates of physical activity in children and early adolescents. Sport Med. 2006;36(1):79–97. doi: 10.2165/00007256-200636010-00006. [DOI] [PubMed] [Google Scholar]
- 31.Hopkins LC, Rose A, Gunther C. Camp NERF: Feasibility, Acceptability, and Potential Efficacy of a Theory-Based Nutrition Education Recreation and Fitness Program Aimed at Preventing Unhealthy Weight Gain in Disadvantaged Children during Summer Months. FASEB J. 2015;29:911.6.
- 32.Hopkins LC, Rose A, Higgins E, Gunther C. Methods and Fidelity of a Nutrition Education Recreation and Fitness Program to Prevent Child Weight Gain during Summer. J Nutr Educ & Behav 2015;47:S34.
- 33.Boylan K, Macpherson H a, Fristad M a. Examination of disruptive behavior outcomes and moderation in a randomized psychotherapy trial for mood disorders. J Am Acad Child Adolesc Psychiatry. 2013;52(7):699–708. doi: 10.1016/j.jaac.2013.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Contento IR, Manning AD, Shannon B. Research perspective on school-based nutrition education. J Nutr Educ. 1992;24(5):247–260. doi: 10.1016/S0022-3182(12)81240-4. [DOI] [Google Scholar]
- 35.Fristad M, Verducci J, Walters K, Young M. The impact of multi-family psychoeducational psychotherapy in treating children aged 8-12 with mood disorders. Arch Gen Psychiatry. 2009;66(9):1013–1021. doi: 10.1001/archgenpsychiatry.2009.112. [DOI] [PubMed] [Google Scholar]
- 36.Goodway JD, Branta CF. Influence of a motor skill intervention on fundamental motor skill development of disadvantaged preschool children. Res Q Exerc Sport. 2003;74(1):36–46. doi: 10.1080/02701367.2003.10609062. [DOI] [PubMed] [Google Scholar]
- 37.Goodway JD, Crowe H, Ward P. Effects of Motor Skill Instruction on Fundamental Motor Skill Development. Adapt Phys Act Q. 2003:20;298–314.
- 38.Kim JS. Effects of a voluntary summer reading intervention on reading achievement: results from a randomized field trial. Educ Eval Policy Anal. 2006;28(4):335–355. doi: 10.3102/01623737028004335. [DOI] [Google Scholar]
- 39.Lusk P, Melnyk BM. COPE for depressed and anxious teens: a brief cognitive-behavioral skills building intervention to increase access to timely, evidence-based treatment. J Child Adolesc Psychiatr Nurs. 2013;26(1):23–31. doi: 10.1111/jcap.12017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Melnyk BM, Jacobson D, Kelly S, et al. Promoting healthy lifestyles in high school adolescents: a randomized controlled trial. Am J Prev Med. 2013;45(4):407–415. doi: 10.1016/j.amepre.2013.05.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Robinson LE, Rudisill ME, Goodway JD. Instructional climates in preschool children who are at-risk. Part II: perceived physical competence. Res Q Exerc Sport. 2009;80(3):543–551. doi: 10.1080/02701367.2009.10599592. [DOI] [PubMed] [Google Scholar]
- 42.Rose AM, Wagner AK, Kennel JA, et al. Determining the feasibility and acceptability of a Nutrition Education and Cooking Program for preschoolers and their families delivered over the dinner hour in a low-income day care setting. Infant, Child Adolesc Nutr. 2014;6(3):144–151. doi: 10.1177/1941406414524274. [DOI] [Google Scholar]
- 43.Birnbaum AS, Lytle L a, Story M, Perry CL, Murray DM. Are differences in exposure to a multicomponent school-based intervention associated with varying dietary outcomes in adolescents? Health Educ Behav. 2002;29(4):427–443. doi: 10.1177/109019810202900404. [DOI] [PubMed] [Google Scholar]
- 44.Black DR, Tobler NS, Sciacca JP. Peer helping/involvement: an efficacious way to meet the challenge of reducing alcohol, tobacco, and other drug use among youth? J Sch Health. 1998;68(3):87–93. doi: 10.1111/j.1746-1561.1998.tb03488.x. [DOI] [PubMed] [Google Scholar]
- 45.Fors SW, Jarvis S. Evaluation of a Peer-Led Drug Abuse Risk Reduction Project for Runaway/homeless Youths. J Drug Educ. 1995;25(4):321–333. doi: 10.2190/TU92-LX8W-G7FD-9LEM. [DOI] [PubMed] [Google Scholar]
- 46.Klepp KI, Halper A, Perry CL. The efficacy of peer leaders in drug abuse prevention. J Sch Health. 1986;56(9):407–411. doi: 10.1111/j.1746-1561.1986.tb05783.x. [DOI] [PubMed] [Google Scholar]
- 47.Komro KA, Perry CL, Murray DM, Veblen-Mortenson S, Williams CL, Anstine PS. Peer-planned social activities for preventing alcohol use among young adolescents. J School Health. 1996;66(9):328–344. doi: 10.1111/j.1746-1561.1996.tb03413.x. [DOI] [PubMed] [Google Scholar]
- 48.Orpinas P, Parcel GS, McAlister A, Frankowski R. Violence prevention in middle schools: a pilot evaluation. J Adol Health. 1995;17(6):360–371. doi: 10.1016/1054-139X(95)00194-W. [DOI] [PubMed] [Google Scholar]
- 49.Perry CL. Prevention of alcohol use and abuse in adolescence: teacher- vs peer-led intervention. Crisis. 1989;10(1):52–61. [PubMed] [Google Scholar]
- 50.Sawyer RG, Pinciaro P, Bedwell D. How peer education changed peer sexuality educators’ self-esteem, personal development, and sexual behavior. J Am Coll Health. 1997;45(5):211–217. doi: 10.1080/07448481.1997.9936887. [DOI] [PubMed] [Google Scholar]
- 51.Beier SR, Rosenfeld WD, Spitalny KC, Zansky SM, Bontempo AN. The potential role of an adult mentor in influencing high-risk behaviors in adolescents. Arch Pediatr Adolesc Med. 2000;154(4):327–331. doi: 10.1001/archpedi.154.4.327. [DOI] [PubMed] [Google Scholar]
- 52.Zimmerman MA, Bingenheimer JB, Notaro PC. Natural mentors and adolescent resiliency: a study with urban youth. Am J Community Psychol. 2002;30(2):221–243. doi: 10.1023/A:1014632911622. [DOI] [PubMed] [Google Scholar]
- 53.DuBois DL, Silverthorn N. Natural mentoring relationships and adolescent health: evidence from a national study. Am J Public Health. 2005;95(3):518–524. doi: 10.2105/AJPH.2003.031476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Klaw EL, Rhodes JE. Mentor relationships and the career development of pregnant and parenting African-American teenagers. Psychol Women Q. 1995;19(4):551–562. doi: 10.1111/j.1471-6402.1995.tb00092.x. [DOI] [PubMed] [Google Scholar]
- 55.Rhodes JE, Grossman JB, Resch NL. Agents of change: pathways through which mentoring relationships influence adolescents’ academic adjustment. Child Dev. 2000;71(6):1661–1671. doi: 10.1111/1467-8624.00256. [DOI] [PubMed] [Google Scholar]
- 56.Black MM, Arteaga SS, Sanders J, et al. College mentors: a view from the inside of an intervention to promote health behaviors and prevent obesity among low-income, urban, African American adolescents. Health Promot Pract. 2012;13(2):238–244. doi: 10.1177/1524839910385899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Black MM, Hager ER, Le K, et al. Challenge! Health promotion/obesity prevention mentorship model among urban, black adolescents. Pediatrics. 2010;126:280–288. doi: 10.1542/peds.2009-1832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Lo E, Coles R, Humbert ML, Polowski J, Henry CJ, Whiting SJ. Beverage intake improvement by high school students in Saskatchewan, Canada. Nutr Res. 2008;28:144–150. doi: 10.1016/j.nutres.2008.01.005. [DOI] [PubMed] [Google Scholar]
- 59.Cawley J, Cisek-Gillman L, Roberts R, et al. Effect of HealthCorps, a high school peer mentoring program, on youth diet and physical activity. Child Obes. 2011;7(5):364–371. doi: 10.1089/chi.2011.0022. [DOI] [Google Scholar]
- 60.Dowd AJ, Chen MY, Jung ME, Beauchamp MR. “Go Girls!”: psychological and behavioral outcomes associated with a group-based healthy lifestyle program for adolescent girls. Transl Behav Med. 2015;5(1):77–86. [DOI] [PMC free article] [PubMed]
- 61.Spencer R, Bower J, Kirk SFL, Hancock Friesen C. Peer Mentoring Is Associated With Positive Change in Physical Activity and Aerobic Fitness of Grades 4, 5, and 6 Students in the Heart Healthy Kids Program. Health Promot Pract. 2014:15;803–11. [DOI] [PubMed]
- 62.Smith LH. Piloting the use of teen mentors to promote a healthy diet and physical activity among children in Appalachia. J Spec Pediatr Nurs. 2011;16(1):16–26. doi: 10.1111/j.1744-6155.2010.00264.x. [DOI] [PubMed] [Google Scholar]
- 63.Perry CL, Klepp K-I, Halper A, et al. Promoting healthy eating and physical activity patterns among adolescents: a pilot study of “Slice of Life”. Heal Educ Res. 1987;2(2):93–103. doi: 10.1093/her/2.2.93. [DOI] [Google Scholar]
- 64.Bogart LM, Elliott MN, Uyeda K, Hawes-Dawson J, Klein DJ, Schuster MA. Preliminary healthy eating outcomes of SNaX, a pilot community-based intervention for adolescents. J Adolesc Health. 2011;48(2):196–202. doi: 10.1016/j.jadohealth.2010.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hamdan S, Story M, French S a, Fulkerson J a, Nelson H. Perceptions of adolescents involved in promoting lower-fat foods in schools: associations with level of involvement. J Am Diet Assoc. 2005;105:247–251. doi: 10.1016/j.jada.2004.11.030. [DOI] [PubMed] [Google Scholar]
- 66.Lytle L, Murray DM, Perry CL, et al. School-based approaches to affect adolescents’ diets: results from the TEENS study. Health Educ Behav. 2004;31(2):270–287. doi: 10.1177/1090198103260635. [DOI] [PubMed] [Google Scholar]
- 67.Story M, Lytle L a, Birnbaum AS, Perry CL. Feasibility and process evaluation of the TEENS Study. J Sch Health. 2002;72:121–127. doi: 10.1111/j.1746-1561.2002.tb06529.x. [DOI] [PubMed] [Google Scholar]
- 68.Stock S, Miranda C, Evans S, et al. Healthy Buddies: a novel, peer-led health promotion program for the prevention of obesity and eating disorders in children in elementary school. Pediatrics. 2007;120(4):e1059–68. [DOI] [PubMed]
- 69.Bandura A. Health promotion by social cognitive means. Health Educ Behav. 2004;31:143–164. doi: 10.1177/1090198104263660. [DOI] [PubMed] [Google Scholar]
- 70.Nader PR, Stone EJ, Lytle LA, et al. Three-year maintenance of improved diet and physical activity: the CATCH Cohort. Child and adolescent trial for cardiovascular health. JAMA Ped. 1999;151(7):695–704. doi: 10.1001/archpedi.153.7.695. [DOI] [PubMed] [Google Scholar]
- 71.Coleman J, Tiller C, Sanchez J, et al. Prevention of the epidemic increase in child risk of overweight in low-income schools: the El Paso coordinated approach to child health. Am J Heal Promot. 2008;22(4):217–224. doi: 10.1001/archpedi.159.3.217. [DOI] [PubMed] [Google Scholar]
- 72.Luepker RV, Perry CL, McKinlay SM, et al. Outcomes of a field trial to improve children’s dietary patterns and physical activity. The Child and Adolescent Trial for Cardiovascular Health. CATCH Collaborative Group. JAMA. 1996;275(10):768–776. doi: 10.1001/jama.1996.03530340032026. [DOI] [PubMed] [Google Scholar]
- 73.Hoelscher DM, Mitchell P, Dwyer J, Elder J, Clesi A, Snyder P. How the CATCH eat smart program helps implement the USDA regulations in school cafeterias. Health Educ Behav. 2003;30(4):434–446. doi: 10.1177/1090198103253517. [DOI] [PubMed] [Google Scholar]
- 74.Hoelscher DM, Kelder SH, Pérez A, et al. Changes in the regional prevalence of child obesity in 4th, 8th, and 11th grade students in Texas from 2000–2002 to 2004–2005. Obesity (Silver Spring) 2010;18(7):1360–1368. doi: 10.1038/oby.2009.305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kelder S, Hoelscher DM, Barroso CS, Walker JL, Cribb P, Hu S. The CATCH Kids Club: a pilot after-school study for improving elementary students’ nutrition and physical activity. Public Health Nutr. 2005;8(2):133–140. doi: 10.1079/PHN2004678. [DOI] [PubMed] [Google Scholar]
- 76.Dzewaltowski DA, Rosenkranz RR, Geller KS, et al. HOP’N after-school project: an obesity prevention randomized controlled trial. Int J Behav Nutr Phys Act. 2010;7:90. doi: 10.1186/1479-5868-7-90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Slusser WM, Sharif MZ, Erausquin JT, Kinsler JJ, Collin D, Prelip ML. Improving overweight among at-risk minority youth: results of a pilot intervention in after-school programs. J Health Care Poor Underserved. 2013;24(2 Suppl):12–24. doi: 10.1353/hpu.2013.0111. [DOI] [PubMed] [Google Scholar]
- 78.Werner D, Teufel J, Holtgrave PL, Brown SL. Active generations: an intergenerational approach to preventing childhood obesity. J Sch Health. 2012;82(8):380–386. doi: 10.1111/j.1746-1561.2012.00713.x. [DOI] [PubMed] [Google Scholar]
- 79.Han J, McGaugh M. Oklahoma CATCH Kids Club: 2010 Analysis; 2009.
- 80.Hans J, McGaugh M. Oklahoma CATCH Kids Club: 2011–2012 Analysis; 2011.
- 81.Sharpe E, Forrester S, Mandigo J, Delion S. Evaluation of CATCH Kinds Club in Ontario after-School Programs: Final Report; 1999.
- 82.Conroy J. Evaluation of Healthy U: After School, Year 5 Executive Summary; 2002.
- 83.Banbury-Robinson J. Ohio’s 4H Cloverbud Program. Columbus: The Ohio State University Extension; 1999. [Google Scholar]
- 84.Corbie-Smith G, Thomas S, St George D. Distrust, race, and research. Arch Intern Med. 2002;162:2458–2463. doi: 10.1001/archinte.162.21.2458. [DOI] [PubMed] [Google Scholar]
- 85.Goode TD, Harrison S. Policy Brief 3: Cultural competence in primary health care: partnerships for a research agenda. Washington: National Center for Cultural Competence, Georgetown University Child Development Center, Center for Child Health and Mental Health Policy-University Affiliated Program; 2000 Summer.
- 86.Katz DL, O’Connell M, Yeh M-C, et al. Public health strategies for preventing and controlling overweight and obesity in school and worksite settings: a report on recommendations of the Task Force on Community Preventive Services. MMWR Recomm Rep. 2005;54(RR-10):1–12. [PubMed] [Google Scholar]