

Abstract
The global burden of disease study (GBD) provides valuable information for evaluating population health in terms of disease burden. This study collected and reviewed GBD data in Korea for the year 1990 and 2013. The burdens of cancer, cardiovascular disease, communicable disease, and injuries have decreased remarkably, thereby greatly diminishing the overall disease burden on Korea. Meanwhile, the burdens due to non-fatal chronic diseases such as neuropsychiatric and musculoskeletal disease became major burden contributors. Responding to this circumstance presents a complex challenge to the Korean health system and Korean health policy.
Keywords: Burden of Disease, Population Health, Health System, Health Policy
Graphical Abstract
INTRODUCTION
The life expectancy at birth of Korean people has increased considerably in recent decades: from 1970 to 2013, the life expectancy of men and women increased from 58.7 to 78.5 and from 65.6 to 85.1 years, respectively—increases of around 20 years (1). This large increase in life expectancy is directly attributable to large decreases in infant, communicable disease, and cardiovascular disease (CVD) mortalities (2,3). Meanwhile, this sharp increase in lifespan inevitably accompanies an increasing elderly population and a transition to a predominance of chronic disease; that is, an epidemiologic transition (4). Although most countries, including developing ones, either have experienced or are experiencing this demographic and epidemiologic transition, no country faces a faster and larger transition than Korea (5).
Responding to this circumstance presents a complex challenge to the Korean health system and Korean health policy. Up to now, economic development has principally improved population health in Korea by increasing Koreans' socioeconomic status (2); however, in the era of chronic disease and disability, the health policy and the health system will soon most strongly affect population health (6). Quantitative evaluation of health status and problems among Korean people is necessary in order for health policy and systems to manage population health adequately, as this methodology allows research to establish problems' priority and thereby make suggestions for the Korean health system's direction.
The global burden of disease study (GBD) provides highly valuable information regarding evaluation of population health. The GBD is a global research project established in 1991 by the World Bank and the World Health Organization (WHO). Currently, the Institute for Health Metrics and Evaluation (IHME) and global researchers have measured disease burden around the world using the disability-adjusted life year (DALY), a composite health measure (7). The DALY is calculated as the sum of years of life lost (YLL) due to premature death and years lived with disability (YLD), which captures a non-fatal aspect of health loss. The latest results of the project are from the GBD 2013, in which around 1,000 researchers from 188 countries including Korea participated (5,8,9). Raw data and estimated values of disease burden indices including mortality rate, DALY, YLL, and YLD are displayed for each studied country on the IHME website (10). Additionally, data from 1990 and 2013 are compared to illustrate temporal trends.
This study used data collected from Korea and the Organisation for Economic Cooperation and Development (OECD) (composed of 34 countries and chosen as a comparison group), sourced from the IHME website, and redesigned the values of the DALY, YLL, and YLD indices for 1990 and 2013. This constituted a comprehensive analysis of characteristics and trends in the absolute and relative health levels of the Korean public, and may identify challenges facing Korean health policy and systems.
THE OVERALL PICTURE OF DISEASE BURDEN IN KOREA
With population growth, the absolute size of the Korean overall disease burden (in DALYs) increased by 3% from 1990 to 2013; however, age-standardized DALY rates (per 100,000 people) largely fell (Fig. 1). Male and female DALY rates dropped 43% and 32%, respectively. These decreases were considerably larger than corresponding average decreases among OECD countries (men: 27%, women: 20%). In 1990, the disease burden on Korean men and women was larger than the OECD average; such a large decrease led to Koreans having a smaller disease burden than the OECD average in 2013. Specifically, the disease burden on Korean women was the second smallest among the OECD countries, following Japan.
Fig. 1.

1990-2013 change in age-standardized DALYs (per 100,000) of Korea and OECD average.
Fig. 2 illustrates the trend in overall Korean disease burden over the same period. YLDs, which accounted for 37% of all DALYs in 1990, gradually increased, reaching 51% in 2013. The absolute number of YLDs rose by 41%; that of YLLs fell by 19%. Non-communicable disease (NCD) was already a major contributor to DALYs in 1990, increasing to 82% of DALYs in 2013. DALYs due to injuries and communicable disease diminished by 30%, respectively, and each of these alone accounted for 11% and 6% of all DALYs, respectively. The fraction of disease burden on persons aged over 65, which was 19% in 1990, increased sharply to 35% in 2013; the absolute disease burden on persons aged 0–14 years decreased by 63%, and in consequence accounted for only 4% of all DALYs. In the same period, although the OECD showed a similar pattern of change, larger changes occurred in Korea.
Fig. 2.

1990-2013 change in pattern of disease burden (in total DALYs) in Korea.
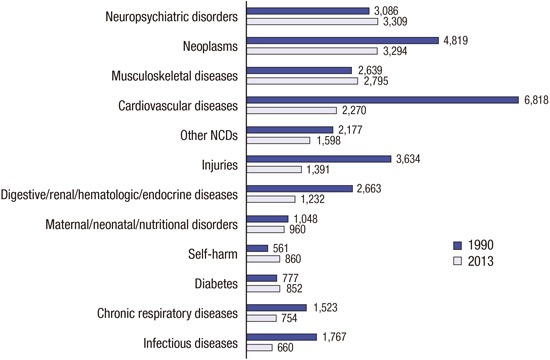
Disorders or conditions were classified into 12 categories. Fig. 3 presents these categories in order of burden size in 2013. Neuropsychiatric disorder was associated with the largest burden, followed by cancer, musculoskeletal disorder, CVD, and other NCDs. Although diabetes mellitus (DM) and suicide are single conditions, the burden of each was larger than that of all chronic respiratory disease or communicable diseases respectively. Of the 12 categories, communicable diseases were associated with the smallest burden. From 1990 until 2013, burdens of neuropsychiatric disorder (7%), musculoskeletal disorder (6%), DM (10%), and suicide (53%) increased, whereas the burdens of cancer (-32%), CVD (-67%), injuries (-62%), medical disease (-54%), chronic respiratory disease (-50%), and communicable disease (-63%) sharply decreased.
Fig. 3.

1990-2013 change in age-standardized DALYs (per 100,000) by cause in Korea.
Fig. 4 presents Korea's disease burden ranking among OECD member countries following the addition of stroke and ischemic heart disease (IHD) to the 12 categories of disorders and conditions. Male and female disease burdens of neuropsychiatric disorder, IHD, and other NCDs were relatively small (ranked lowly), whereas the burdens of stroke, DM, suicide, maternal/neonatal/nutritional disorder, and communicable disease were relatively large in Korea among OECD nations (ranked highly). Some categories exhibited opposing pictures of disease burden by sex compared with OECD averages. The burden of cancer was relatively larger than average in men, whereas that in women was smaller than average. In contrast, the burden of musculoskeletal disorder was larger than the OECD average in women but average in men.
Fig. 4.

Korea's ranking in age-standardized DALYs by cause and performance level among 34 OECD members.
Table 1 presents the 10 diseases or conditions associated with the largest disease burdens. Among these, the largest burden affecting men and women was lower back and neck pain (LBP & NP) and stroke. Regarding men, the next largest was suicide, followed in order by DM, lung cancer, and liver cancer; regarding women, the next largest was depressive disorder, followed in order by iron-deficiency anemia (IDA), musculoskeletal disorder, and DM. Diverging from the OECD averages, in Korea, stroke was more burdensome than IHD; suicide was ranked higher among all categories; and liver cancer was among the 10 most burdensome conditions. Regarding YLL in Korea and diverging from OECD averages, burdens due to stroke, suicide, and DM were ranked higher, and liver and stomach cancer were among the 10 most burdensome conditions.
Table 1. Top ten most burdensome diseases/conditions in Korea, 2013.
| Rank | DALY | YLL | YLD | |||
|---|---|---|---|---|---|---|
| Male | Female | Male | Female | Male | Female | |
| 1 | Low back pain & neck pain | Low back pain & neck pain | Stroke | Stroke | Low back pain & neck pain | Low back pain & neck pain |
| 2 | Stroke | Stroke | Self-harm | Self-harm | Skin disease | Depression |
| 3 | Self-harm | Depression | Liver cancer | Ischemic heart disease | Diabetes | Iron-deficiency anemia |
| 4 | Diabetes | Iron-deficiency anemia | Lung cancer | Diabetes | Sense organ disease | Migraine |
| 5 | Liver cancer | Other musculoskeletal disorders | Stomach cancer | Stomach cancer | Iron-deficiency anemia | Other musculoskeletal disorders |
| 6 | Lung cancer | Diabetes | Ischemic heart disease | Lung cancer | Migraine | Skin disease |
| 7 | Ischemic heart disease | Migraine | Road injuries | Liver cancer | Depression | Sense organ disease |
| 8 | Road injuries | Skin disease | Diabetes | Road injuries | Other musculoskeletal disorders | Anxiety |
| 9 | Stomach cancer | Ischemic heart disease | Colorectal cancer | Colorectal cancer | Drug use | Diabetes |
| 10 | COPD | Self-harm | COPD | Breast cancer | COPD | Gynecologic problems |
Based on age-standardized calculation; Each values for diseases are presented at website of Institute for Health Metrics and Evaluation, http://vizhub.healthdata.org/gbd-compare.
DALY, disability-adjusted life year; YLL, years of life lost; YLD, years lived with disability; COPD, chronic obstructive pulmonary disease.
A DETAILED PICTURE OF DISEASE BURDEN IN KOREA
Neuropsychiatric disorder
The burdens due to neuropsychiatric disorders have increased somewhat, and are now the biggest health burden on the Korean public. Specifically, migraine and mild-to-moderate mental disorders such as depressive and anxiety disorders were the main causes of burden in this category, accounting for almost half of the total burden due to neuropsychiatric disorder (46%). Specifically, this category burdened women relatively heavily. Regarding YLD ranking, depressive disorder was ranked second, migraine 5th, and anxiety disorder 8th in women.
Nonetheless, among the OECD countries, Korean men and women were least burdened by neuropsychiatric disorders, and particularly regarding depressive and anxiety disorders and dementia. Exceptionally, migraine was associated with a relatively large burden, and Korean men and women showed the third and 10th largest DALY rates among OECD countries, respectively.
Cancer
Over the last two decades, the cancer mortality rate has continued to decrease (11,12). The GBD's results indicate that the DALY rate due to cancer fell by 32%. Nonetheless, cancer remains the leading cause of death in Korea, accounting for around 30% of all deaths (13). The GBD's results indicate that cancer, together with the neuropsychiatric disorders remains the largest disease burden on Korea.
In 1990, the burden of stomach cancer, which was the largest of all cancer types, has decreased substantially. Nonetheless, the DALY rates for stomach cancer among men and women in Korea were the largest among the OECD countries; OECD Health Data indicated that Korea had the highest stomach cancer mortality rate among the OECD countries (14). Liver and lung cancer mortality rates continued to fall and their DALY rates diminished by 6% and 18%, respectively. Of all cancer types, lung and liver cancer became the largest burden contributors to the Koreans. Although a large burden of lung cancer was typical among OECD countries, the burden of liver cancer was the largest in Korea among OECD countries in both sexes. In particular, the DALY rate due to liver cancer in men was four times higher than the OECD average. OECD Health Data comparing between OECD countries indicate that Korea had outstandingly high male and female liver cancer mortality rates (14). The large burden of liver cancer in Korea may largely reflect the fact that Korea is a hepatitis B endemic area, and hepatitis B is closely related with liver cancer (15). In contrast with most other cancer types, colorectal cancer that was ranked ninth in YLL, increased in DALY rate by 14% in men. Considering the relatively high incidence of colorectal cancer (ranked 1st among OECD countries according to OECD Health Data), this cancer is expected to increase the burden of disease on the Korean public.
The relative burdens of cancers were reversed depending on sex. In men, liver, lung, and stomach cancers were among the 10 most burdensome diseases in Korea. Their burden on Korean men was the sixth largest among the OECD countries. In contrast, in Korean women, no cancer type was among the 10 most burdensome diseases, and Korea, together with Japan, had the smallest cancer burden in women in the OECD. OECD Health Data corroborated these results: Korean men's cancer mortality rate was the eighth highest among the OECD countries, whereas that of women was the third lowest. Among the OECD countries, the disease with the largest burden in women was breast cancer; however, the breast cancer mortality rate in Korean women was the lowest among the OECD countries.
Musculoskeletal disorder
In 2010, the GBD commenced full-scale research of musculoskeletal disorders as well as neuropsychiatric disorders (16). The results indicated that the burden due to musculoskeletal disorders, which had been underestimated compared to CVD and cancer, was globally very large (9). In Korea, the burden of musculoskeletal disorder is steadily increasing, and that disorder has become a major burden contributor. In particular, LPB and NP accounted for around three quarters of all musculoskeletal disorders, and were the largest burden contributors among individual disorders in men and women. Among younger people aged 20–49, musculoskeletal disorder was overwhelmingly the most burdensome disorder, with more than double the burden due to suicide (ranked second).
Musculoskeletal disorder's burden on women was larger, burdening women most heavily of the 12 burden cause categories. Women's total DALY rate for musculoskeletal disorder was 1.7 times higher than men's was. In addition, among women in the OECD countries, musculoskeletal disorder placed the second-heaviest burden on Korean women, following Germany.
Cardiovascular disease & diabetes
In 1990, CVDs burdened Korean people most heavily, and the DALY rate associated with stroke was the largest among the OECD countries. However, from 1990 to 2013, the DALY rate for CVDs decreased by 67%, reflecting sharply dropping IHD and stroke mortality rates. Studies analyzing GBD data have found that CVDs' mortality rates in Korea dropped more than 60% from 1990 to 2013—the largest reduction in the world—and that the stroke incidence rate had decreased more sharply in Korea than anywhere else in the world (17,18).
Nonetheless, in Korea, stroke was associated with the largest disease burden, being ranked the second and the first in the top ten causes of DALY and YLL in 2013, respectively. Unlike the OECD average, Korea is much more burdened by stroke than by IHD. Among the OECD countries: the burden of IHD is twice as large as that of stroke; the reverse is the case in Korea. OECD Health Data indicates that Korea has the lowest IHD mortality rate and the highest stroke mortality rate of the OECD countries.
Unlike CVDs, the DALY rate for DM increased by 10% from 1990 to 2013. In addition, the Korean burden of DM is the largest in the OECD, excepting several East European countries, and DM was among the top 10 causes of YLL.
Other non-communicable diseases
The burdens associated with almost all diseases in the category of other NCDs (i.e. digestive/renal/hematologic/endocrine and chronic respiratory disease) diminished from 1990 to 2013. Their burden on Korea was the smallest among the OECD countries. Exceptionally, the burden of liver cirrhosis in men was relatively high among the OECD.
Self-harm & other injuries
Suicide in men and women was ranked in the third and 10th places in Korean DALY ranking, respectively. In particular, suicide among people aged 20–49 was associated with the second largest burden, following LBP and NP. The Korean burden due to suicide was the largest in the OECD, and twice as high as the OECD average. Over the last 23 years, OECD countries had reduced the burden of suicide by 16%, whereas the burden of suicide increased 53% in Korea.
The burdens due to all injury types except suicide decreased. As shown in Fig. 3, in 1990, injury was associated with the third largest burden, following CVD and cancer, but this fell 62% by 2013. Although the DALY rate for road injury dropped by 71%, Korea had the largest burden due to road injury (the second for men; the first for women) among the OECD countries. This result is corroborated by OECD Health Data showing that Korea was ranked second for road mortality in both men and women among the OECD countries.
Communicable disease & maternal/neonatal/nutritional disorder
Although the burden of communicable disease in Korea decreased by 63% (in DALY rates) from 1990 to 2013, and communicable disease's burden was the smallest of the 12 causal categories, Korea had a relatively large burden of communicable disease among the OECD countries, due to outstanding burdens of tuberculosis and pneumonia. The burden of tuberculosis in both Korean men and women was overwhelmingly the largest among the OECD countries. Pneumonia is still one of the main causes of death in Korea (13).
The absolute burden of maternal/neonatal/nutritional disorders decreased, but was relatively large compared to the corresponding burdens in OECD countries; compared to the OECD countries, Korea had the largest burden of IDA in both men and women. In particular, the burden of IDA on women was large, and the largest burden of disease was found in those aged 5–14.
DISCUSSION
Analysis of GBD data for Korea showed that the burdens of cancer, CVD, communicable disease, and injuries, which had been the largest health burdens on the Korean public over the last two decades, have decreased remarkably, thereby greatly diminishing the overall disease burden on Korea. Additionally, the present study found that Korean population health has improved rapidly and was as good as that of other advanced countries. OECD Health Data and many reports from WHO support this conclusion (19).
With decreases in the burdens due to the mortalities, the structure of the disease burden in Korea has naturally changed to include a larger fraction of burdens due to morbidities, particularly in NCDs. Notably, neuropsychiatric and musculoskeletal disorders provide the largest health burdens to the Korean public. So far, mild-to-moderate mental and neurological disorders such as depressive and anxiety disorder and migraine did not draw significant attention; disease such as LBP was not clearly understood sufficiently (20). Recent GBD studies have addressed morbidity and disability more comprehensively, and has indicated that these diseases present large challenges to public health (21).
Unfortunately, there is a general lack of research and research funding for mental disorders. In Korea, only 3% of all national health care expenditure targets mental health; up to two thirds of all expenditure targets hospitals (22). Over the last 20 years, Korea, unlike other advanced countries, has seen the number of beds in mental hospitals increase, and periods of hospitalization are remarkably long (22). Korea therefore needs to research and invest in community-based mental health systems, similarly to other advanced countries.
The burden of cancer on Korean men was found to be very large. Globally, the burden of cancer on men is larger than on women; however, this difference is very large in Korea. This phenomenon affects subsequent statistics: the life expectancy gap between Korean men and women is 6.5 years, which is the largest among the OECD countries excepting some Eastern European nations (14). Although the reasons for this sex gap in cancer burden require careful research, it is likely related to smoking and alcohol consumption. According to OECD Health Data, smoking and heavy drinking are more common among Korean men than the OECD average; in contrast, these behaviors are relatively rare among Korean women. A study using GBD data has shown that smoking and heavy drinking were most important risk factors contributing to health burden in Korean men (23). If smoking and heavy drinking are controlled to recommended levels, the current CVD mortality rate in Korea, which has already declined sharply, is expected to fall by more than 50% (24). Specifically, younger Koreans aged 30–49 and people of low socioeconomic status showed elevated rates of smoking and heavy drinking (25,26). It is therefore necessary to implement policies addressing these groups. Well-designed policy addressing this issue may diminish health inequality (27).
It is critical that Korea has a relatively large burden of DM. Specific Korean susceptibility such as poor insulin secretion is often noted as a cause of this burden (28), however, this does not explain the large burden of premature death due to DM found in this study. Many studies have reported that patient education is poor and patient blood glucose is not well controlled in Korea (29,30); this elevates Korea's DM mortality and hospitalization rates in comparison with other OECD countries (14). If DM is effectively controlled by primary care in the community, hospitalization may be largely prevented; hence, the aforementioned DM outcomes may indicate that Korean primary care is partly ineffective. Statistics supporting this inference include high rates of hospitalization caused by primary care sensitive conditions (PCSCs) such as asthma, chronic obstructive pulmonary disease (COPD), and hypertension in OECD countries (14).
Until now, the Korean health system has achieved considerable success in treating fatal diseases and cancer, and has increased the life expectancy of the Korean population, as mentioned earlier. However, the Korean health system now faces the difficult task of addressing the current epidemic of chronic disease. Extreme increases in the elderly population and medical costs reflect this task's difficulty. Numerous domestic and foreign experts have noted that the Korean health system needs to reinforce and enhance primary care, and implement policies supporting health promotion and preventive medical service (31).
Meanwhile, current major health problems in Korea cannot be addressed within the Korean health system alone. Korea's large burdens of suicide and road traffic injury, its burden of musculoskeletal disorder among women and young people, and the large difference in disease burden between men and women—which is attributable to lifestyle risk factors—are social issues as well as health issues. Managing health issues requires improvement in social determinants of health. Health should therefore be addressed through all types of public policy, namely 'health in all policies', and through multisectoral effort (32).
The GBD's results for Korea provide highly valuable information; however, the following limitations apply. Most significantly, the data reflect estimation rather than measurement and therefore, its internal validity can be criticized, although the estimations are based on the various population-based health surveys in Korea (33). In particular, it might be difficult to capture the Korean characteristics of disease sequela regarding the determination of disability weights, which greatly affect the YLD calculation (34). Indeed, GBD researchers actively promote country-specific research in each nation for this reason (35). More researchers need to participate in estimating national and subnational disease burden in Korea with more valid methodologies.
This study examined the health status of the Korean population by reviewing the GBD data for Korea. Although the burden of disease in Korea has greatly decreased, many challenges remain due to the rising burden of chronic disease. Organizational effort to collect high-quality data is required in order to address these challenges through the Korean health system and health policy.
Footnotes
Funding: This study was supported by a grant of the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (Grant No. HI 13C0729).
DISCLOSURE: The authors have no potential conflicts of interest to disclose.
AUTHOR CONTRIBUTION: Conception and design of the study: Lee Y, Yoon SJ, Kim A, Seo H, Ko SK. Acquisition of data and interpretation: Lee Y, Yoon SJ, Kim A, Seo H, Ko SK. Writing manuscript: Lee Y. Critical review of manuscript: Yoon SJ, Kim A, Seo H, Ko SK. Supervision of whole study: Yoon SJ. Final approval of manuscript: all authors.
References
- 1.Korean Statistical Information Service. Abridged life tables 1970-2014 [Internet] [accessed on 1 December 2015]. Available at http://kosis.kr/eng/statisticsList/statisticsList_01List.jsp?vwcd=MT_ETITLE&parentId=A#SubCont.
- 2.Yang S, Khang YH, Harper S, Davey Smith G, Leon DA, Lynch J. Understanding the rapid increase in life expectancy in South Korea. Am J Public Health. 2010;100:896–903. doi: 10.2105/AJPH.2009.160341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lim D, Ha M, Song I. Trends in the leading causes of death in Korea, 1983-2012. J Korean Med Sci. 2014;29:1597–1603. doi: 10.3346/jkms.2014.29.12.1597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Weisz G, Olszynko-Gryn J. The theory of epidemiologic transition: the origins of a citation classic. J Hist Med Allied Sci. 2010;65:287–326. doi: 10.1093/jhmas/jrp058. [DOI] [PubMed] [Google Scholar]
- 5.Murray CJ, Barber RM, Foreman KJ, Abbasoglu Ozgoren A, Abd-Allah F, Abera SF, Aboyans V, Abraham JP, Abubakar I, Abu-Raddad LJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition. Lancet. 2015;386:2145–2191. doi: 10.1016/S0140-6736(15)61340-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Khang YH. Burden of noncommunicable diseases and national strategies to control them in Korea. J Prev Med Public Health. 2013;46:155–164. doi: 10.3961/jpmph.2013.46.4.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369:448–457. doi: 10.1056/NEJMra1201534. [DOI] [PubMed] [Google Scholar]
- 8.GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;386:743–800. doi: 10.1016/S0140-6736(15)60692-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Institute for Health Metrics and Evaluation (IHME) GBD compare [Internet] [accessed on 1 December 2015]. Available at http://vizhub.healthdata.org/gbd-compare.
- 11.Lim D, Ha M, Song I. Trends in major cancer mortality in Korea, 1983-2012, with a joinpoint analysis. Cancer Epidemiol. 2015;39:939–946. doi: 10.1016/j.canep.2015.10.023. [DOI] [PubMed] [Google Scholar]
- 12.Jung KW, Shin HR, Kong HJ, Park S, Won YJ, Choi KS, Park EC. Long-term trends in cancer mortality in Korea (1983-2007): a joinpoint regression analysis. Asian Pac J Cancer Prev. 2010;11:1451–1457. [PubMed] [Google Scholar]
- 13.Korean Statistical Information Service. Death and death rates by casuse [Internet] [accessed on 1 December 2015]. Available at http://kosis.kr/eng/statisticsList/statisticsList_01List.jsp?vwcd=MT_ETITLE&parentId=A#SubCont.
- 14.Organisation for Economic Cooperation and Development. OECD health statistics [Internet] [accessed on 1 December 2015]. Available at http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT.
- 15.Yeo Y, Gwack J, Kang S, Koo B, Jung SJ, Dhamala P, Ko KP, Lim YK, Yoo KY. Viral hepatitis and liver cancer in Korea: an epidemiological perspective. Asian Pac J Cancer Prev. 2013;14:6227–6231. doi: 10.7314/apjcp.2013.14.11.6227. [DOI] [PubMed] [Google Scholar]
- 16.Hoy DG, Smith E, Cross M, Sanchez-Riera L, Blyth FM, Buchbinder R, Woolf AD, Driscoll T, Brooks P, March LM. Reflecting on the global burden of musculoskeletal conditions: lessons learnt from the global burden of disease 2010 study and the next steps forward. Ann Rheum Dis. 2015;74:4–7. doi: 10.1136/annrheumdis-2014-205393. [DOI] [PubMed] [Google Scholar]
- 17.Shepard D, VanderZanden A, Moran A, Naghavi M, Murray C, Roth G. Ischemic heart disease worldwide, 1990 to 2013: estimates from the global burden of disease study 2013. Circ Cardiovasc Qual Outcomes. 2015;8:455–456. doi: 10.1161/CIRCOUTCOMES.115.002007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, Moran AE, Sacco RL, Anderson LM, Truelsen T, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990-2010: findings from the global burden of disease study 2010. Lancet Glob Health. 2013;1:e259–81. doi: 10.1016/S2214-109X(13)70089-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Health Organization. World health statistics 2015 [Internet] [accessed on 1 December 2015]. Available at http://apps.who.int/iris/bitstream/10665/170250/1/9789240694439_eng.pdf?ua=1&ua=1.
- 20.Storheim K, Zwart JA. Musculoskeletal disorders and the global burden of disease study. Ann Rheum Dis. 2014;73:949–950. doi: 10.1136/annrheumdis-2014-205327. [DOI] [PubMed] [Google Scholar]
- 21.Patten SB. The global burden of disease 2010 update: keeping mental health in the spotlight. Epidemiol Psychiatr Sci. 2014;23:255–257. doi: 10.1017/S2045796014000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Organisation for Economic Cooperation and Development. Korea's increase in suicides and psychiatric bed numbers is worrying, says OECD [Internet] [accessed on 1 December 2015]. Available at http://www.oecd.org/els/health-systems/MMHC-Country-Press-Note-Korea.pdf.
- 23.GBD 2013 Risk Factors Collaborators. Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, Brauer M, Burnett R, Casey D, Coates MM, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;386:2287–2323. doi: 10.1016/S0140-6736(15)00128-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Roth GA, Nguyen G, Forouzanfar MH, Mokdad AH, Naghavi M, Murray CJ. Estimates of global and regional premature cardiovascular mortality in 2025. Circulation. 2015;132:1270–1282. doi: 10.1161/CIRCULATIONAHA.115.016021. [DOI] [PubMed] [Google Scholar]
- 25.Kang YW, Ko YS, Kim KY, Sung C, Lee DH, Jeong E. Trends in health-related behaviors of Korean adults: study based on data from the 2008-2014 Community Health Surveys. Epidemiol Health. 2015;37:e2015042. doi: 10.4178/epih/e2015042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Khang YH, Lynch JW, Jung-Choi K, Cho HJ. Explaining age-specific inequalities in mortality from all causes, cardiovascular disease and ischaemic heart disease among South Korean male public servants: relative and absolute perspectives. Heart. 2008;94:75–82. doi: 10.1136/hrt.2007.117747. [DOI] [PubMed] [Google Scholar]
- 27.Cho HJ. The status and future challenges of tobacco control policy in Korea. J Prev Med Public Health. 2014;47:129–135. doi: 10.3961/jpmph.2014.47.3.129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ohn JH, Kwak SH, Cho YM, Lim S, Jang HC, Park KS, Cho NH. 10-year trajectory of beta-cell function and insulin sensitivity in the development of type 2 diabetes: a community-based prospective cohort study. Lancet Diabetes Endocrinol. 2016;4:27–34. doi: 10.1016/S2213-8587(15)00336-8. [DOI] [PubMed] [Google Scholar]
- 29.Ha KH, Kim DJ. Trends in the diabetes epidemic in Korea. Endocrinol Metab (Seoul) 2015;30:142–146. doi: 10.3803/EnM.2015.30.2.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jung JH, Lee JH, Noh JW, Park JE, Kim HS, Yoo JW, Song BR, Lee JR, Hong MH, Jang HM, et al. Current status of management in type 2 diabetes mellitus at general hospitals in South Korea. Diabetes Metab J. 2015;39:307–315. doi: 10.4093/dmj.2015.39.4.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Atun R. Transitioning health systems for multimorbidity. Lancet. 2015;386:721–722. doi: 10.1016/S0140-6736(14)62254-6. [DOI] [PubMed] [Google Scholar]
- 32.Bert F, Scaioli G, Gualano MR, Siliquini R. How can we bring public health in all policies? Strategies for healthy societies. J Public Health Res. 2015;4:393. doi: 10.4081/jphr.2015.393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Byass P, de Courten M, Graham WJ, Laflamme L, McCaw-Binns A, Sankoh OA, Tollman SM, Zaba B. Reflections on the global burden of disease 2010 estimates. PLoS Med. 2013;10:e1001477. doi: 10.1371/journal.pmed.1001477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nord E. Disability weights in the global burden of disease 2010: unclear meaning and overstatement of international agreement. Health Policy. 2013;111:99–104. doi: 10.1016/j.healthpol.2013.03.019. [DOI] [PubMed] [Google Scholar]
- 35.Burstein R, Fleming T, Haagsma J, Salomon JA, Vos T, Murray CJ. Estimating distributions of health state severity for the global burden of disease study. Popul Health Metr. 2015;13:31. doi: 10.1186/s12963-015-0064-y. [DOI] [PMC free article] [PubMed] [Google Scholar]