

Abstract
Background
The benefits of physical activity for the mental health and well-being of children and young people are well-established. Increased physical activity during school hours is associated with better physical, psychological and social health and well‐being. Unfortunately many children and young people exercise insufficiently to benefit from positive factors like well-being.
The main aim of this study is to develop, implement and evaluate a multi-component, school-based, physical activity intervention to improve psychosocial well-being among school-aged children and youths from the 4th to the 6th grade (10–13 years).
Methods
A four-phased intervention – design, pilot, RCT, evaluation - is carried out for the development, implementation and evaluation of the intervention which are guided by The Medical Research Council framework for the development of complex interventions. 24 schools have been randomized and the total study population consists of 3124 children (baseline), who are followed over a period of 9 months. Outcome measure data at the pupil level are collected using an online questionnaire at baseline and at follow-up, 9 months later with instruments for measuring primary (general physical self-worth) and secondary outcomes (self-perceived sport competences, body attractiveness, scholastic competences, social competences and global self-worth; enjoyment of PA; self-efficacy; and general well-being) that are both valid and manageable in setting-based research. The RE-AIM framework is applied as an overall instrument to guide the evaluation.
Discussion
The intervention focuses on the mental benefits of physical activity at school, which has been a rather neglected theme in health promotion research during recent decades. This is unfortunate as mental health has been proclaimed as one of the most important health concerns of the 21st century. Applying a cluster RCT study design, evaluating the real-world effectiveness of the intervention, this study is one of the largest physical activity intervention projects promoting psychosocial well-being among children and youths. Through a comprehensive effectiveness evaluation and a similar substantial process evaluation, this study is designed to gain knowledge on a broad variety of implementation issues and give detailed information on project delivery and challenges at the school level – among other things to better inform future practice.
Trial registration
Date of registration: 24 April 2015 retrospectively registered at Current Controlled Trials with study ID ISRCTN12496336
Keywords: Well-being, School, Children, Youth, Physical activity, Physical education, Denmark
Background
The benefits of physical activity (PA) for the mental health and well-being of children and youths are well-established. Among other things, regular PA can help build social skills and self-esteem – the latter commonly viewed as a key indicator of positive well-being [1–4].
Unfortunately many children and young people exercise insufficiently to benefit from positive factors like the ones mentioned above [5, 6]. In recent years, a number of large school-based interventions have been conducted, in the effort to increase physical activity in larger, blended populations of children [7–14], as well as interventions aiming at children’s mental health and well-being [3, 15, 16]. An overall conclusion of these studies is that increased physical activity during school hours is associated with better physical, psychological and social health and well‐being.
A review on the effectiveness of school-based, physical activity interventions found significant, albeit varied, effects on self-concept and attitudes towards exercise [17]. A comprehensive review of reviews, by Biddle and Asare [1], substantiates the claim that PA has an overall positive effect on mental health and well-being. A few years ago, Bailey and colleagues summed up the issue and stated: ‘There is compelling evidence that regular PA can have a positive effect on emotional well-being, especially for children and young people’ [18]. At the same time, Bailey and colleagues underlined that there is no “automatism” regarding the connection. PA’s contribution to well-being is conditional to the context and especially the social climate generated by e.g. educators [18–20]. Positive experiences with PA form part of a “virtuous cycle” and improve self-concepts and even more, overall well-being, while negative experiences transform the relationship to a “vicious cycle” through which the person becomes more and more disaffected in relation to PA [18].
The school as the setting for PA interventions
In many countries, school-based approaches to PA have the obvious advantage that the children who need it most are fairly reachable, due to the fact that the vast majority of children and adolescents receive their primary education in public schools. Furthermore, health and well-being is an integrated part of the public school curriculum, which means that there are qualified educators and an existing culture for teaching and learning activities related to health, well-being and PA [21].
Research on the effectiveness of school-based physical activity interventions and other health interventions points out a number of methodological issues worth mentioning [17]. First of all, development of the intervention should be based on best available evidence and should be thoroughly pilot tested in settings similar to the actual intervention environments. Secondly, program fidelity - meaning the degree to which an intervention is implemented as intended – should be monitored and reported on. Tracking implementation fidelity is essential to understanding the program impact. Especially for the latter reason, intervention research should incorporate systematic evaluations on both the process and the effectiveness of school-based, physical activity intervention [17], hence known as hybrid type 2 studies (see Fig. 1).
Fig. 1.
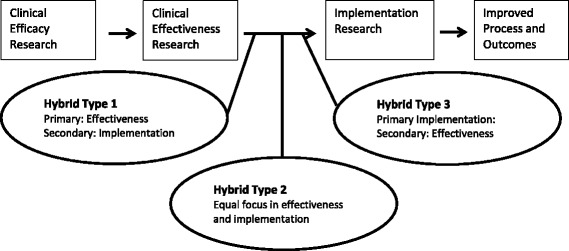
Hybrid-effectiveness continuum. Hybrid effectiveness-implementation designs as part of the clinical research continuum, adapted from [58]
Furthermore, a theoretical approach in intervention science is needed [22]. Theories dealing with both intervention processes and effectiveness contribute to explaining how and why certain outcomes are achieved; identifying core elements that influence implementation; distinguishing between program theory failure and program implementation failure and, finally, in further program development [22].
Taking these issues into account, the aim of this article is to present the development, design and main components of the Move for Well-being in Schools (MWS) intervention study.
Methods and design
Study aim and overview
The main aim of MWS is to develop, implement and evaluate a multi-component, school-based, physical activity intervention to improve psychosocial well-being among school-aged children and youths from the 4th to the 6th grade (age 10–13 in the Danish school system). The study has a special focus on the group of children who are most at risk of experiencing a ‘vicious cycle’ in physical activity at school, and thus could possess lower motivation and decreased self-confidence for engaging in normal PA activities in school.
The development, implementation and evaluation of the intervention are guided by The Medical Research Council framework for the development of complex interventions. Since it was first published in 2000, the framework has been widely used to identify and tailor activities for selected target audiences [23]. For this study, a four-phased intervention is carried out in the years 2014–2017 (Fig. 2). The four phases consist of a design phase, pilot testing phase, randomized controlled trial phase and a program evaluation phase.
Fig. 2.
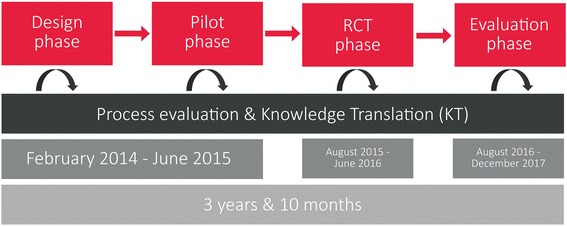
Study design. A four-phased intervention. Overview of the study period
Knowledge Translation (KT) is a key activity in all stages of the intervention (Fig. 2.). KT is understood as a dynamic process that includes synthesis, exchange and application of knowledge to improve health and well-being and provide more effective services [24]. For a number of years, it has been stressed that such processes must ensure the combination of best available research evidence and local contextual knowledge by facilitating close interaction between researchers, end users and other relevant stakeholders [25, 26].
Design phase
This phase started with a scoping review summarizing published knowledge on both implementation and effectiveness of similar interventions. Furthermore, a number of structured group interviews were conducted with members of the target group in order to get further, contextual insight with regard to the needs, wishes, challenges and perceived qualities formulated by pupils aged 10–13 in relation to engaging in and enjoying physical activity. Informed by findings from the mentioned materials, a preliminary intervention program was qualified via four workshops in which researchers, school managers, teachers, pedagogues, and organizations dealing with school sport and physical education participated. The stakeholders constituted the Project Development Group (PDG). The main aim was to incorporate professional and/or practice-based expertise and knowledge into the further development of the final intervention.
The design phase consolidated the project’s theory of change and facilitated close interaction between researchers, end users and other relevant stakeholders in connection with intervention development. Thus, besides guiding the intervention model, the design phase contributed to continuous, broad-based stakeholder involvement. Evidence suggests that evaluations and key intervention findings are more likely to be used on a long-term basis if stakeholders are involved in and committed to the program and assessment processes. Thus, it has been shown that co‐creation, where research users are directly involved in the research process, facilitates sustained and creative use of research results [27, 28].
The output of the design phase was a comprehensive intervention program based on best available evidence, close collaboration with stakeholders and grounded in a solid theoretical approach, in particular to the area of motivation – as construed by Edward Deci and Richard Ryan in their self-determination theory (SDT) [29]. According to Deci and Ryan, the main architects of SDT, human motivation is essentially based on three innate psychological needs: competence, autonomy and relatedness. The SDT theory’s distinction between self-determined or autonomous and controlled types of motivation reflects individual reasons for participating in activities. The PA in this particular intervention program is therefore designed to meet these three psychological needs in order to motivate all pupils [29, 30].
The intervention program itself consists of three components targeting four settings for school-based physical activity (Table 1). Basically, the intervention program strives to improve the activities conducted and the social and pedagogical climate in which they are performed. For this reason, the practitioners were equipped with a Tailored Activity Program (TAP), including educational materials, planning guides and course plans for incorporating PA throughout the school day. The materials were both delivered in printed versions and also made available on the intervention website, which also contained overall information on the program goals and deliverables.
Table 1.
Intervention program components. Overview of the intervention program, what it contains and the keyword that describes the components
| Intervention program | Part | What | Keywords |
|---|---|---|---|
| Components | Competence Development Program (CDP) | 4 Workshop days Vodcast – short video podcast with info and themes regarding the program. Inspirational day at the schools – “kick off – day” |
Focusing on underlying theory of PA intervention Trying out core activities Knowledge translation Inspiration |
| Tailored Activity Program (TAP) | Website Educational materials, planning guides and course plans |
Availability Support Inspiration |
|
| Coordination Group (CG) | A representative from 4th, 5th, and 6th grade and from school management | Connection between educators and management Supplying support Contact to research team Two supervision visits at each school |
|
| PA settings | Physical education classes | 6 PE courses each of 6 × 90 min where 2 of these are mandatory and the last 4 can be chosen from a variety of lesson plans | 8 different courses Team based Student involvement Competence focus |
| In-class activities | 2 activity breaks per day/50 mins per week | In-class activities/pause activities Differentiate purpose: social, energy, relax and coordination |
|
| Recess activities | 3 sessions per week, average 30 min per session | Initiation and support of recess PA | |
| Theme days | 2-3 theme days arranged over the school year | Development of activities with pupils. Focus on well-being at school. |
The TAP was supported by a Competency Development Program (CDP) for educators, focusing on the underlying theoretical approach and opportunities to try out core activities in practice. Furthermore, each school was supported in setting up a Coordination Group (CG), which received support via biweekly information e-mails, two local supervision visits with the research team during the intervention period and the possibility to contact the research team throughout the period by mail or phone. The four selected settings were: Physical education classes, in-class activities, recess activities and theme days.
Pilot phase
The pilot phase included a structured assessment of whether the initial intervention program could, in fact, be implemented and adapted to the school setting. This entailed systematic appraisals of the acceptability and feasibility of delivering the intervention [23]. The pilot phase was divided into a preparation phase that lasted three months and an action phase of four months, where the actual intervention was piloted at five schools.
In the preparation phase, the Competency Development Program (CDP) provided enrolled educators with knowledge and skills tailored to carry out differentiated instruction and teaching activities, with the aim of supporting pupil motivation for and engagement in school-based PA. A specific focus was to make sure that educators acquired further skills and competencies to engage with a diversified group of pupils, displaying a large variation in performance levels, and to provide additional support to pupils who, for various reasons, were less motivated to engage in school-based PA.
The action phase was conducted at the same five schools that initially delivered members to the above-mentioned Project Development Group. In this way, stakeholders taking part in the design phase were given the opportunity to continue their involvement and, importantly, to secure further development via active feedback on effectiveness, implementation and feasibility issues.
Adjustment of the intervention program
Pupil level assessment of the pilot action phase was conducted via qualitative focus group interviews, including two boys and two girls from each grade (4th to 6th grade) in three out of five pilot schools. The interviews lasted 30 min and were semi-structured. The pupils were encouraged to engage in joint dialogue on how best, on the one hand, to address perceived problems and deficiencies and, on the other hand, to strengthen key qualities of the various PA intervention components [31].
School level assessments of the pilot action phase were based on face-to-face evaluation meetings with the practitioners and managers involved in the pilot intervention and on questionnaires distributed to them. The overall aim was to gather information on the participants’ evaluation of the relevance and impact of the interventions in relation to promoting PA and well-being in the school setting. The primary target group was the educators taking part in the aforementioned CDP. Interviews with school management and the CG were performed midway through the pilot phase and at the end of the pilot phase. In a fourth and final workshop, findings from pupil and school level assessments were discussed with the CG from the pilot schools.
The pilot phase led to a number of smaller intervention improvements, as well as an increased focus on securing a durable intervention delivery system. Furthermore, specific modifications were made to the CDP and TAP. An example of a modification was omitting an intended e-learning component through vodcasts (video podcasts) appertaining to the teacher study groups at the schools. Due to time constraints, the educators were not able to engage with the vodcasts in the study groups, and the themes were instead incorporated into workshop sessions and other materials. Another modification example is the length of each PE course (cf. Table 1), which was reduced from six to four 90 min lessons. The reason for that was that teachers voiced challenges with motivating pupils to fully engage with the same theme in six consecutive PE lessons.
RCT phase
The randomized controlled trial (RCT) entails the implementation of the final intervention program (Table 1) in the selected settings. Based on statistical power calculations and the capacity of the research set-up, a target of 12 schools was set for both the control and the intervention group. Municipalities were selected based on maximizing geographic spread, difference in size and difference in allocated budget for public schools [32]. Municipalities were not contacted if they already had large scale school development projects; were located near universities or university colleges other than the operating unit (University of Southern Denmark); located in relatively hard to reach locations; or had less than 6 schools in the entire school district. Based on initial screening, 11 of 98 Danish municipalities were contacted. After consent, local authorities initiated the first contact with schools or gave the research team permission to contact the schools directly. The research team held individual meetings with all interested schools and a total of 24 schools were enrolled. A stratified randomization was then conducted with three strata and with the constraint of an even distribution of schools from each municipality in the intervention group and the control group respectively. The three strata were defined by school typology, based on school size and district socio-economic status. Stratum A: Small schools, <70 pupils in grades 4–6, often located in small rural villages; Stratum B: Larger schools, >70 pupils, with low socio-economic status; and Stratum C: Larger schools with high socio-economic status. Beginning with Stratum A, schools were randomly assigned to either intervention or comparison by means of simple randomization - while adhering to the constraint of even distribution of schools from the various municipalities in the intervention and control group.
The initial part of the RCT phase is illustrated in Fig. 3.
Fig. 3.
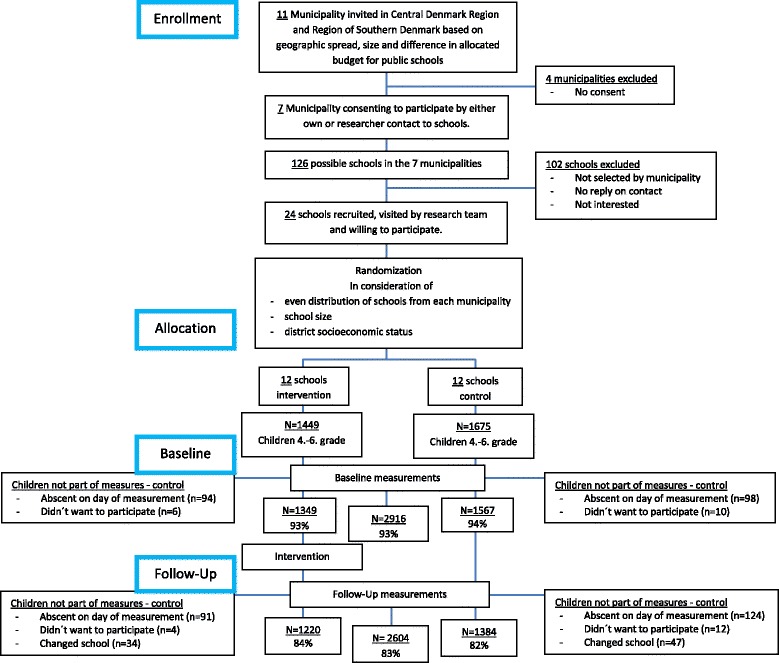
Flowchart of recruitment, randomization and baseline questionnaire
Program evaluation
The program evaluation phase examines the final intervention program with a focus on both effectiveness and implementation: Did the intervention go as planned; what actually happened; and was the intervention effective in improving the psychosocial well-being of the target population? In addition to the effectiveness issue, the program evaluation provides insight on how the intervention was delivered, what barriers and opportunities it created for teachers, and how the intervention was experienced by the pupils. A mixed-method evaluation design, combining qualitative and quantitative approaches, is applied to gather valid information on both effectiveness and implementation issues. The RE-AIM framework is applied to ensure a holistic assessment of intervention impacts [33]. RE-AIM has been widely used to enhance the quality, speed, and public health impact of efforts to translate research into practice [33]. The framework is made up of five key elements - Reach, Effectiveness, Adaptation, Implementation and Maintenance.
Outcome measures
The design and pilot phase also comprised testing, selecting and adapting instruments for measuring primary (general physical self-worth) and secondary outcomes (self-perceived sport competences, body attractiveness, scholastic competences, social competences and global self-worth; enjoyment of PA; self-efficacy; and general well-being) that were both valid, reliable and manageable in setting-based research.
The selected survey instruments have systematically been translated and adapted in order to secure Danish versions that are conceptually equivalent to the original English instruments (if not already available in Danish). The procedure used in this study is guided by the WHO1 Process of translation and adaptation of instruments. An initial forward translation from English to Danish was conducted by a professional translator familiar with the terminology of themes covered by the instruments, followed by a cross-cultural adaptation. A second professional translator conducted a back translation of the Danish instruments to English. Two bilingual experts compared the original and back-translated English versions of the survey instruments. The experts discussed their findings and suggestions with the research team, supplemented by other content resource people, which led to minor revisions [34].
In connection with the pilot phase, the compiled survey instrument was tested by groups of pupils followed by a cognitive validation process. Questionnaire characteristics - e.g. completion time and numbers of questions, and repeated clarifying questions on specific topics - were evaluated. The cognitive validation consisted of interviews with selected pupils and focused on their understanding of the various survey items [31]. Based on the evaluation, the questions were modified to decrease reading load and completion time, and a short version of the the Physical Activity Enjoyment Scale (PACES) questions was chosen.
In the RCT phase, data at the pupil level are collected using an online questionnaire at baseline and at follow-up, 9 months later. The questionnaire is administered in a quiet setting during school hours. A research assistant and an educator are present during data collection to ensure independent and confidential responding, to provide verbal information on how to respond to items and to answer possible questions from the pupils. The questionnaire design and purpose is described below.
Self-perception
Thirty six questions are used to measure participant’s self-perception. The Sport Competences, Body Attractiveness and Physical Self-worth subscales from the Children’s Physical Self-Perception Profile (C-PSPP) is used to assess changes in the primary outcome measures: Physical self-concept [35, 36]. The Scholastic Competence, Social Competence and Global Self-worth subscales from the Self-perception Profile for Children (SPPC) are included to measure aspects of psychosocial well-being. The SPPC, developed by Susan Harter, is widely used and found to be valid and reliable [37–39]. All scales in the SPPC and C-PSPP are calculated as the mean of 6 items. Each item consists of two statements, which are scored on a four-point scale using a structured alternative format designed to reduce social desirability. Firstly, the pupil is asked to decide what kind of kid he or she is most like in each statement. E.g. “Some kids do very well at all kinds of sports, BUT other kids don’t feel that they are very good when it comes to sports”. Next, the pupil has to decide whether the selected description is “Really True for Me” or “Sort of True for me”. A score of 1 indicates the lowest perceived competence or adequacy, and a score of 4 reflects the highest level of competence or adequacy.
Socio-demographics
Four structured questions are used to determine the socio-demographic characteristics of the pupils. Furthermore, family social class is measured based on information on parental occupation. The information is coded into occupational social class I-V, economically active, or unclassifiable (VI), economically inactive (VII), unclassifiable (VIII), missing information (IX). Family social class is equal to the parent with the highest occupation social class [40].
Physical activity
Leisure time physical activity is assessed using two structured questions. Firstly, pupils are asked to choose from four statements denoting different levels of leisure time PA (e.g. engaging in organized sports several times a week or preferring sedentary activities e.g. playing with the computer and listening to music) [41]. Secondly, the pupils are asked how often they are physically active at a level that makes them breathe hard and fast and/or gets them sweating. This item is scored on a 6-point Likert scale from “Everyday” through “Never”. The frequency of physical activity during recess is measured with a single question using a 4-point Likert format ranging from “Several times a day” to “Rarely or never”. Lastly, the pupils are required to answer how often they walk or bike to school on a 4-point Likert Scale (“Everyday” to “Never”).
Self-efficacy
Measured using 8 questions. The scale uses a single factor 5-point Likert format and is an adapted version of an 8-item questionnaire previously developed for use with 5th, 6th and 8th-grade girls (PASES) [42–44]. In accordance with Bartholomew et al. [45], the original wording is changed from an explicit focus on leisure time physical activity, to encompass self-efficacy regarding PA in general (leisure and school time). The pupils are asked to select how much they agree with eight statements ranging from “Disagree a lot” to “Agree a lot”. Each item is scored from 1 to 5, with a score of 1 indicating lowest self-efficacy.
Enjoyment
Is measured using seven negatively worded questions from the Physical Activity Enjoyment Scale (PACES). The scale uses a 5-point Likert format and is an adapted version of the 16-item version of PACES. This instrument has been validated for use with children and adolescents [46–51]. Pupils are asked to select how much they agree with seven statements relating to different feelings about physical activity (“Agree a lot” to “Disagree a lot”). Each item is scored from 1 to 5, with a score of 1 indicating lowest enjoyment. E.g. “When I am physically active…I feel bored”.
Perception of physical education (PE)
Five structured questions are used to measure the perception of PE in relation to the frequency of participation and involvement in, the motivation for and the enjoyment of PE. Each question is scored on a 4 or 5-point Likert scale.
School and general well-being
Information relating to psychological well-being and school physical and psychosocial environment is measured using 13 questions stemming from the Danish national survey of well-being in the school-aged population. These questions are implemented to enable comparison not only within the study sample but also with national distributions on these key elements.
Health-related quality of life (HRQoL)
Information relating to the participant’s perception of general well-being is measured using the KIDSCREEN-27 Quality of Life Questionnaire for Children and Adolescents [52] - The KIDSCREEN Group Europe 2006). This tool consists of 27 items on physical well-being (5 items), psychological well-being (7 items), autonomy and parent relationship (7 items), peer and social support (5 item), and school environment (5 items). Each item is scored on a 5-point Likert scale with a timeframe of one week. Higher scores indicate better HRQoL, e.g. “Thinking about the last week…Have you felt lonely?”
Evaluating implementation
This part of the program evaluation considers the adoption, implementation and short-term maintenance of the intervention program according to the RE-AIM framework. The focus is on three levels of operation: the strategic level (school managers and coordination group CG), the operational level (educators) and the user/beneficiary level (the pupils).
At the user/beneficiary level, the main objective is to assess pupils’ experiences with the intervention components. Did they experience a change, and did the change increase their motivation for and participation in physical activities at school? There is a specific focus on pupils who are most at risk of experiencing a ‘vicious cycle’ in relation to physical activity at school. Pupils at two schools are especially closely followed by a researcher using ethnographic methods, taking part in everyday school life. Informal interviews are conducted, which are supported by focus group interviews with pupils and individual interviews with educators. Approximately 25–30 days of observation, 10 focus group interviews and interviews with 4 educators are conducted at the two selected schools. To increase the information on the user-level, class evaluations are conducted at the end of the study in one random class at each grade level at all 24 schools. The class evaluation collects the immediate experience of school PA for pupils at all schools and focuses on the four settings for PA included in the intervention program (Table 1).
At the operational level, the main objective is to assess the fidelity and feasibility of the intervention. Did the educators receive enough information about the intervention and were they able to conduct activities as intended? The evaluation focus’ on self-efficacy in relation to executing activity components, perceived relevance and educators experienced resistance from the pupils regarding intervention participation. Three times during the intervention period, educators are asked to fill in online questionnaires on issues like these. Additionally, a selected group of PE teachers at four intervention schools are more intensively followed - focusing on their practice of the PE lessons designed for this particular intervention program (Table 1). Finally, the research group is informed about general progress, barriers and successes in connection with the previously mentioned supervision visits to each school. At the meetings, the researchers follow PE classes, observe recess and in-class activities and engage in informal conversations with the educators.
At the strategic level, the main objective is to assess the context in which the educators are operating. Did the school managers and CG support the intervention program, and did they ensure a collaborative effort to make it a whole-school approach? School managers are interviewed as regards their role in both leading and managing the intervention, and the CGs participate in two meetings with the research team during the supervision visits. The meetings center on four statements related to the role of the CG:
Well-being in school is running fully as intended in our school
Our colleagues are positive towards Well-being in school
Well-being in school is a priority at our school and receives adequate support from the school management
The three bearing SDT-principles - competence, autonomy and relatedness – are evident for all involved as leading principles of Well-being in school.
The statements are visually presented via analog continuum scales and the CGs are asked to state the level of implementation by placing a mark on scales for each of the four statements. The rest of the meeting concerns the reasons for the level of implementation, and how the CGs can improve the current status. The individual ratings from the members of the CGs are summarized into one ‘Room For Improvement’ (RFI) score for each school.
Statistical considerations
Sampling is school-based (cluster randomized) and individual respondents are therefore not independent. Some of the variances in measurements can be ascribed to class, school and surrounding environment [32]. This internal variation at school and class level was accounted for in the sample size calculations and will be accounted for in the effect analyses.
Based on baseline data from the pilot study, an intracluster correlation coefficient (ICC) was calculated for the primary outcome (mean of ‘physical self-worth’ from the Children’s Physical Self-Perception Profile) using ‘clustersampsi’ in STATA version 14 [53]. With a mean of 3.12, an SD of 0.70, a significance level of 0.05, a statistical power of 0.80, an ICC of 0.025 at school-class level, 72 classes from 12 schools on each arm and approximately 20 pupils in each class, it will be possible to detect a difference of 0.09. The mean of ‘physical self-worth’ should, therefore, be increased from 3.12 to 3.21 before a significant effect can be detected.
The effect of the intervention is tested using multilevel models adjusted for relevant, potentially confounding factors (e.g. baseline outcome measure, gender, age and family social class).
When testing the overall effectiveness of the intervention, the primary outcome measures will be evaluated both as a continuous outcome and as a logistic outcome evaluating the proportion of students below a given threshold. All analyses will be performed according to the intention-to-treat principle, and supplemented with exploratory analyses to test associations between outcome measures and implementation fidelity using data from the process analyses. Because of the cluster structure of the data, random effects for school and class will be included in all analyses.
Ethical considerations
In conducting research with human subjects, and especially children, ethical considerations should be highly prioritized - both in relation to the intervention and the evaluation thereof. PA interventions are often designed to change individual and/or collective views on the qualities of a physically active lifestyle. This could increase the pressure of living up to such active-living ideals and possibly cause adverse side effects, for example, eating disorders, excessive training and stigmatization of overweight individuals [54]. The current intervention is based on principles of an inclusive approach to PA in school, where students have positive experiences together with classmates. Still, it is possible that the interventions have adverse side effects and cause uncomfortable situations for some children. The likelihood of such unintended, negative side effects occurring is deemed as rather limited.
The main risk to the participants in the current study is potential embarrassment and disclosure of sensitive information to others [55]. The nature of some of the survey questions regarding self-perception and well-being could be regarded as sensitive, and some children could feel uncomfortable answering these. In particular, if the pupil has low self-perceptions or is struggling with bullying or exclusion in school, this could be an issue. Pupils were informed to complete the questionnaires individually and dividing cardboard was used between the tables to maximize privacy (for further information see Ethics approval and consent to participate).
Discussion
Standing on the verge of the program evaluation phase, the developed school-based, physical activity intervention holds some promising strengths, as well as considerations. These will be summarized and discussed in the following section.
First of all, the intervention focuses on the mental benefits of physical activity at school, which has been a rather neglected theme in health promotion research during recent decades. This is unfortunate. Mental health has been proclaimed as one of the most important health concerns of the 21st century, as stated early on by WHO in their 2004 summary report, Promoting Mental Health. On top of this the mutually dependent relationship between physical activity and mental health has not yet been fully uncovered [1, 56].
Another characteristic feature of the study is the cluster RCT study design, which evaluates the real-world effectiveness of an intervention. 24 schools were randomized and the total study population consists of 3124 children (baseline), who are followed over a period of 9 months. To our knowledge, this makes it one of the largest physical activity intervention projects promoting psychosocial well-being among children and youths.
Alongside the comprehensive effectiveness evaluation, the study is designed to gain knowledge on a broad variety of implementation issues. This knowledge will be highly usable for educators, school managers and policy makers when tackling, for instance local challenges regarding school-based PA.
The detailed information on project delivery and roll-out at the school level makes it possible to better inform future practice. This study is co-created with and delivered by educators and school managers, which ensures that the findings and experiences are particularly relevant for practice.
There are considerations within the study, which must be taken into account. Firstly, the measurement of psychosocial well-being relies on data generated via survey tools, which can only grasp parts of this complex phenomenon. Secondly, the multi-component design makes it difficult to single out the effectiveness of, for instance, individual PA activities. Thirdly, although 3124 pupils and nine months follow-up are considered a comprehensive design, there is still limited power to detect a real intervention effect. Facilitating and detecting robust improvements in psychosocial well-being among children and youths via PA may very well take years instead of months. Fourthly, the intervention has to be balanced between tailoring the intervention to the individual school and ensuring a certain degree of comparability. Too much tailoring could lead to a non-comparable intervention and too much conformity could entail lower motivation for implementation among key stakeholders.
Acknowledgements
The authors would like to thank Research and Innovation Centre for Human Movement and Learning (FIIBL), University College Lillebaelt (UCL) and the involved schools, teachers and children.
Funding
The study is funded by a donation from TrygFonden, Denmark. The funder has no role or authority in conducting the research project, except acceptance of adjustments of the research plan.
Availability of data and materials
The datasets collected and/or analyzed during the current study are available from the corresponding authors upon reasonable request.
Authors’ contributions
TS acts as principal investigator. LBC acts as daily manager and coordinator of the research project in coordination with PLC and SS. TS, LBC, PLC and SS developed the intervention in coordination with the PDG. SS initiated this paper and wrote the first draft. All of the authors contributed to writing the manuscript and critically reviewing its content. All authors approved the final version before submission.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
We used a passive informed consent procedure, which means that the pupils are included in the study until their parents or the pupils themselves withdraw consent. Prior to the data collection, pupils and their parents received information about the nature and procedure of the study. The information was delivered as a personal message to the parents through the intranet of schools. It was emphasized that participation was voluntary, that parents and pupils could withdraw consent at any time, and that data would be treated confidentially and anonymously. The points from the written information were repeated orally at the beginning of each questionnaire session, and the pupils had the possibility to withdraw consent. However, participation in the activities and programs during school hours at the intervention schools was part of the curriculum and could not be avoided. The passive informed consent procedure has been found ethical appropriate for low-risk research, where low-risk is defined as the same level of risk as the pupils normally could encounter in daily life [55]. Spence et al. [57] repeated that recommendation recently and showed that active parental consent decreased participation rate especially for pupils with lower socioeconomic status. The recommendation was followed by underlining that children rights should be safeguarded, i.e. making clear that participation is voluntary; there should be no pressure to participate, and they can change their mind and leave the study at any point [57].
At the two schools involved in the qualitative process evaluation, pupils and parents were informed of the presence of the researcher, and active informed consent was collected via a parent-signed form for all pupils who had been selected for focus group interviews. All data are stored and treated in accordance with Danish law for data protection, and the project is notified to the Danish Data Protection Agency and to the system of health research ethics committees in Denmark (De Videnskabsetiske Komitéer for Region Syddanmark) and is on the ISRCTN registry (DOI 10.1186/ISRCTN12496336).
Abbreviations
- CDP
Competence development program
- CG
Coordination group
- C-PSPP
Children’s physical self-perception profile
- HRQoL
Health-related quality of life
- ICC
Intracluster correlation coefficient
- KT
Knowledge translation
- MWS
Move for well-being in school
- PA
Physical activity
- PACES
Physical activity enjoyment scale
- PASES
Physical activity self-efficacy scale
- PDG
Project development group
- PE
Physical education
- RCT
Randomized controlled trial
- RFI
Room for improvement
- SDT
Self-determination theory
- SPPC
Self-perception profile for children
- TAP
Tailored activity program
- WHO
World Health Organisation
Footnotes
WHO: Process of translation and adaptation of instruments.
Contributor Information
Søren Smedegaard, Email: ssmedegaard@health.sdu.dk.
Lars Breum Christiansen, Email: lbchristiansen@health.sdu.dk.
Pernille Lund-Cramer, Email: plcramer@health.sdu.dk.
Thomas Bredahl, Email: tbredahl@health.sdu.dk.
Thomas Skovgaard, Email: tskovgaard@health.sdu.dk.
References
- 1.Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. 2011;45(11):886–895. doi: 10.1136/bjsports-2011-090185. [DOI] [PubMed] [Google Scholar]
- 2.Ekeland E, Heian F, Hagen KB. Can exercise improve self esteem in children and young people? A systematic review of randomised controlled trials. Br J Sports Med. 2005;39(11):792–798. doi: 10.1136/bjsm.2004.017707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Landry BW, Driscoll SW. Physical activity in children and adolescents. PM R. 2012;4(11):826–832. doi: 10.1016/j.pmrj.2012.09.585. [DOI] [PubMed] [Google Scholar]
- 4.Biddle SJ, Mutrie N, Gorely T. Psychology of Physical Activity: Determinants, Well-Being and Interventions. 3rd ed. Abingdon: Routledge; 2015.
- 5.Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10:98. doi: 10.1186/1479-5868-10-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hills AP, Dengel DR, Lubans DR. Supporting public health priorities: recommendations for physical education and physical activity promotion in schools. Prog Cardiovasc Dis. 2015;57(4):368–374. doi: 10.1016/j.pcad.2014.09.010. [DOI] [PubMed] [Google Scholar]
- 7.Dobbins M, Husson H, DeCorby K, LaRocca RL. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane database sys rev. 2013;2:Cd007651. doi: 10.1002/14651858.CD007651.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sollerhed AC, Ejlertsson G. Physical benefits of expanded physical education in primary school: findings from a 3-year intervention study in Sweden. Scand J Med Sci Sports. 2008;18(1):102–107. doi: 10.1111/j.1600-0838.2007.00636.x. [DOI] [PubMed] [Google Scholar]
- 9.Graf C, Koch B, Falkowski G, Jouck S, Christ H, Staudenmaier K, Tokarski W, Gerber A, Predel H-G, Dordel S. School-based prevention: Effects on obesity and physical performance after 4 years. J Sports Sci. 2008;26(10):987–994. doi: 10.1080/02640410801930176. [DOI] [PubMed] [Google Scholar]
- 10.Donnelly JE, Greene JL, Gibson CA, Smith BK, Washburn RA, Sullivan DK, DuBose K, Mayo MS, Schmelzle KH, Ryan JJ, et al. Physical Activity Across the Curriculum (PAAC): a randomized controlled trial to promote physical activity and diminish overweight and obesity in elementary school children. Prev Med. 2009;49(4):336–341. doi: 10.1016/j.ypmed.2009.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kriemler S, Zahner L, Schindler C, Meyer U, Hartmann T, Hebestreit H, Brunner-La Rocca HP, van Mechelen W, Puder JJ. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: cluster randomised controlled trial. BMJ. 2010;340:c785. doi: 10.1136/bmj.c785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. 2011;45(11):923–930. doi: 10.1136/bjsports-2011-090186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lai SK, Costigan SA, Morgan PJ, Lubans DR, Stodden DF, Salmon J, Barnett LM. Do school-based interventions focusing on physical activity, fitness, or fundamental movement skill competency produce a sustained impact in these outcomes in children and adolescents? A systematic review of follow-up studies. Sports Med. 2014;44(1):67–79. doi: 10.1007/s40279-013-0099-9. [DOI] [PubMed] [Google Scholar]
- 14.Jago R, Rawlins E, Kipping RR, Wells S, Chittleborough C, Peters TJ, Mytton J, Lawlor DA, Campbell R. Lessons learned from the AFLY5 RCT process evaluation: implications for the design of physical activity and nutrition interventions in schools. BMC Public Health. 2015;15:946. doi: 10.1186/s12889-015-2293-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Babic MJ, Morgan PJ, Plotnikoff RC, Lonsdale C, White RL, Lubans DR. Physical activity and physical self-concept in youth: systematic review and meta-analysis. Sports Med. 2014;44(11):1589–1601. doi: 10.1007/s40279-014-0229-z. [DOI] [PubMed] [Google Scholar]
- 16.Kohl III HW, Cook HD. Educating the student body: Taking physical activity and physical education to school. Washington, DC: National Academies Press; 2013. [PubMed]
- 17.Demetriou Y, Höner O. Physical activity interventions in the school setting: A systematic review. Psychol Sport Exerc. 2012;13(2):186–196. doi: 10.1016/j.psychsport.2011.11.006. [DOI] [Google Scholar]
- 18.Bailey R, Hillman C, Arent S, Petitpas A. Physical activity: an underestimated investment in human capital? J Phys Act Health. 2013;10(3):289–308. doi: 10.1123/jpah.10.3.289. [DOI] [PubMed] [Google Scholar]
- 19.Brunelle J, Danish SJ, Forneris T. The impact of a sport-based life skill program on adolescent prosocial values. Appl Dev Sci. 2007;11(1):43–55. doi: 10.1080/10888690709336722. [DOI] [Google Scholar]
- 20.Holland MJG. The role and development of life skills in young sports participants. Birmingham: University of Birmingham; 2012.
- 21.Naylor PJ, McKay HA. Prevention in the first place: schools a setting for action on physical inactivity. Br J Sports Med. 2009;43(1):10–13. doi: 10.1136/bjsm.2008.053447. [DOI] [PubMed] [Google Scholar]
- 22.Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015;10(1):1–13. doi: 10.1186/s13012-015-0242-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M, Medical Research Council G Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. doi: 10.1136/bmj.a1655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Straus S, Tetroe J, Graham ID. Knowledge translation in health care: moving from evidence to practice: Wiley; 2013.
- 25.Glasgow RE, Emmons KM. How can we increase translation of research into practice? Types of evidence needed. Annu Rev Public Health. 2007;28:413–433. doi: 10.1146/annurev.publhealth.28.021406.144145. [DOI] [PubMed] [Google Scholar]
- 26.Kessler R, Glasgow RE. A proposal to speed translation of healthcare research into practice: dramatic change is needed. Am J Prev Med. 2011;40(6):637–644. doi: 10.1016/j.amepre.2011.02.023. [DOI] [PubMed] [Google Scholar]
- 27.Lavis J, Davies H, Oxman A, Denis JL, Golden-Biddle K, Ferlie E. Towards systematic reviews that inform health care management and policy-making. J Health Serv Res Policy. 2005;10(Suppl 1):35–48. doi: 10.1258/1355819054308549. [DOI] [PubMed] [Google Scholar]
- 28.Pope C, Mays N, Popay J. Informing policy making and management in healthcare: the place for synthesis. Healthcare policy. 2006;1(2):43–48. [PMC free article] [PubMed] [Google Scholar]
- 29.Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi: 10.1037/0003-066X.55.1.68. [DOI] [PubMed] [Google Scholar]
- 30.Deci EL, Ryan RM. Intrinsic motivation and self-determination in human behavior. New York: Plenum. 1985
- 31.Collins D. Pretesting survey instruments: an overview of cognitive methods. Qual Life Res. 2003;12(3):229–238. doi: 10.1023/A:1023254226592. [DOI] [PubMed] [Google Scholar]
- 32.Raudenbush SW, Martinez A, Spybrook J. Strategies for improving precision in group-randomized experiments. Educ Evaluation Policy Analysis. 2007;29(1):5–29. doi: 10.3102/0162373707299460. [DOI] [Google Scholar]
- 33.Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89(9):1322–1327. doi: 10.2105/AJPH.89.9.1322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sperber AD. Translation and validation of study instruments for cross-cultural research. Gastroenterology. 2004;126(Supplement 1):S124–S128. doi: 10.1053/j.gastro.2003.10.016. [DOI] [PubMed] [Google Scholar]
- 35.Fox KR, Corbin CB. THE PHYSICAL SELF-PERCEPTION PROFILE - DEVELOPMENT AND PRELIMINARY VALIDATION. J Sport Exerc Psychol. 1989;11(4):408–430. doi: 10.1123/jsep.11.4.408. [DOI] [Google Scholar]
- 36.Whitehead J. A Study of Children’s Physical Self-Perceptions Using an Adapted Physical Self-Perception Profile Questionnaire. Pediatr Exerc Sci. 1995;7:132–151. doi: 10.1123/pes.7.2.132. [DOI] [Google Scholar]
- 37.Muris P, Meesters C, Fijen P. The self-perception profile for children: Further evidence for its factor structure, reliability, and validity. Pers Individ Dif. 2003;35(8):1791–1802. doi: 10.1016/S0191-8869(03)00004-7. [DOI] [Google Scholar]
- 38.Harter S. The Self-Perception Profile for Children: Revision of the Perceived Competence Scale for Children. Denver, CO: University of Denver; 1985. [Google Scholar]
- 39.Harter S. Self-Perception Profile for Children: Manuals and Questionnaires (Grades 3–8)..University of Denver Arts, Humanities and Social Sciences Department of Psychology. 2012
- 40.Christensen U, Krolner R, Nilsson CJ, Lyngbye PW, Hougaard CO, Nygaard E, Thielen K, Holstein BE, Avlund K, Lund R. Addressing social inequality in aging by the Danish occupational social class measurement. J Aging Health. 2014;26(1):106–127. doi: 10.1177/0898264314522894. [DOI] [PubMed] [Google Scholar]
- 41.Grimby G, Borjesson M, Jonsdottir IH, Schnohr P, Thelle DS, Saltin B. The “Saltin-Grimby Physical Activity Level Scale” and its application to health research. Scand J Med Sci Sports. 2015;25(Suppl 4):119–125. doi: 10.1111/sms.12611. [DOI] [PubMed] [Google Scholar]
- 42.Dishman RK, Motl RW, Saunders RP, Dowda M, Felton G, Ward DS, Pate RR. Factorial invariance and latent mean structure of questionnaires measuring social-cognitive determinants of physical activity among black and white adolescent girls. Prev Med. 2002;34(1):100–108. doi: 10.1006/pmed.2001.0959. [DOI] [PubMed] [Google Scholar]
- 43.Motl RW, Dishman RK, Trost SG, Saunders RP, Dowda M, Felton G, Ward DS, Pate RR. Factorial validity and invariance of questionnaires measuring social-cognitive determinants of physical activity among adolescent girls. Prev Med. 2000;31(5):584–594. doi: 10.1006/pmed.2000.0735. [DOI] [PubMed] [Google Scholar]
- 44.Saunders RP, Pate RR, Felton G, Dowda M, Weinrich MC, Ward DS, Parsons MA, Baranowski T. Development of questionnaires to measure psychosocial influences on children’s physical activity. Prev Med. 1997;26(2):241–247. doi: 10.1006/pmed.1996.0134. [DOI] [PubMed] [Google Scholar]
- 45.Bartholomew JB, Loukas A, Jowers EM, Allua S. Validation of the physical activity self-efficacy scale: Testing measurement invariance between Hispanic and Caucasian children. J Phys Act Health. 2006;3(1):70. doi: 10.1123/jpah.3.1.70. [DOI] [Google Scholar]
- 46.Motl RW, Dishman RK, Saunders R, Dowda M, Felton G, Pate RR. Measuring enjoyment of physical activity in adolescent girls. Am J Prev Med. 2001;21(2):110–117. doi: 10.1016/S0749-3797(01)00326-9. [DOI] [PubMed] [Google Scholar]
- 47.Moore JB ZY, Hanes J, Joan D, Berard G, Barbeau P. Measuring Enjoyment of Physical Activity in Children: Validation of the Physical Activity Enjoyment Scale. J Appl Sport Psychol. 2009;21(S1):S116–s129 [DOI] [PMC free article] [PubMed]
- 48.Dishman RK, Motl RW, Saunders R, Felton G, Ward DS, Dowda M, Pate RR. Enjoyment mediates effects of a school-based physical-activity intervention. Med Sci Sports Exerc. 2005;37(3):478–487. doi: 10.1249/01.MSS.0000155391.62733.A7. [DOI] [PubMed] [Google Scholar]
- 49.Dishman RK, Hales DP, Sallis JF, Saunders R, Dunn AL, Bedimo-Rung AL, Ring KB. Validity of social-cognitive measures for physical activity in middle-school girls. J Pediatr Psychol. 2010;35(1):72–88. doi: 10.1093/jpepsy/jsp031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Paxton RJ, Nigg C, Motl RW, Yamashita M, Chung R, Battista J, Chang J. Physical Activity Enjoyment Scale short form--does it fit for children? Res Q Exerc Sport. 2008;79(3):423–427. doi: 10.1080/02701367.2008.10599508. [DOI] [PubMed] [Google Scholar]
- 51.Carraro A, Young MC, Robazza C. A contribution to the validation of the physical activity enjoyment scale in an Italian sample. Soc Behav Personal Int J. 2008;36(7):911–918. doi: 10.2224/sbp.2008.36.7.911. [DOI] [Google Scholar]
- 52.Ravens-Sieberer U, Herdman M, Devine J, Otto C, Bullinger M, Rose M, Klasen F. The European KIDSCREEN approach to measure quality of life and well-being in children: development, current application, and future advances. Qual Life Res. 2014;23(3):791–803. doi: 10.1007/s11136-013-0428-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hemming K, Marsh J. A menu-driven facility for sample-size calculations in cluster randomized controlled trials. Stata J. 2013;13(1):114–135. [Google Scholar]
- 54.Schwartz MB, Henderson KE. Does Obesity Prevention Cause Eating Disorders? J Am Acad Child Adolesc Psychiatry. 2009;48(8):784–786. doi: 10.1097/CHI.0b013e3181acfb88. [DOI] [PubMed] [Google Scholar]
- 55.Santelli JS, Smith Rogers A, Rosenfeld WD, DuRant RH, Dubler N, Morreale M, English A, Lyss S, Wimberly Y, Schissel A. Guidelines for adolescent health research. A position paper of the Society for Adolescent Medicine. J Adolesc Health. 2003;33(5):396–409. [PubMed] [Google Scholar]
- 56.Lubans DR, Plotnikoff RC, Lubans NJ. Review: A systematic review of the impact of physical activity programmes on social and emotional well-being in at-risk youth. Child Adolesc Mental Health. 2012;17(1):2–13. doi: 10.1111/j.1475-3588.2011.00623.x. [DOI] [PubMed] [Google Scholar]
- 57.Spence S, White M, Adamson AJ, Matthews JNS. Does the use of passive or active consent affect consent or completion rates, or dietary data quality? Repeat cross-sectional survey among school children aged 11–12 years. BMJ Open. 2015;5(1). [DOI] [PMC free article] [PubMed]
- 58.Cully JA, Armento ME, Mott J, Nadorff MR, Naik AD, Stanley MA, Sorocco KH, Kunik ME, Petersen NJ, Kauth MR. Brief cognitive behavioral therapy in primary care: a hybrid type 2 patient-randomized effectiveness-implementation design. Implement Sci. 2012;7:64. doi: 10.1186/1748-5908-7-64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets collected and/or analyzed during the current study are available from the corresponding authors upon reasonable request.