

Abstract
The authors aimed to present a deep anterior lamellar keratoplasty (DALK) surgery case with mixed type bubble demonstrating Dua's layer (DL). This was a reported case of DALK surgery. The authors encountered cornea DL structure at DALK surgery while cleaning the remaining stromal pieces. We also observed perforation in the central part of DL. However, DALK surgery could be completed. It is possible to encounter DL in a DALK surgery performed with mixed type big-bubble.
Keywords: Deep anterior lamellar keratoplasty, Dua's layer, pre-Descemet's membrane
Introduction
Cornea Dua's layer (DL) was defined as a pre-Descemet's membrane (DM) between stroma and DM. It was demonstrated that DL separation happens along the last row of keratocytes, with an average thickness of 10.15 ± 3.6 microns (range 6.3–15.83).[1]
For patients who have corneal diseases that spare the DM and endothelium, in terms of DM and endothelium are intact, deep anterior lamellar keratoplasty (DALK) has gradually become a popular alternative to penetrating keratoplasty (PKP).[2]
Big-bubble (BB) technique might be utilized in DALK surgery. It was found that injection of air in the corneal stroma can form three types of BB: Type 1, Type 2, and mixed.[1]
The present study aimed to present a DALK surgery case with mixed type bubble demonstrating DL.
Case Report
A 54-years-old female who had blurry vision in the left eye applied to our polyclinic with a significant reduction in vision recently. Because of former keratitis [Figure 1a], she had corneal opacification on the left eye. The patient received DALK under general anesthesia.
Figure 1.
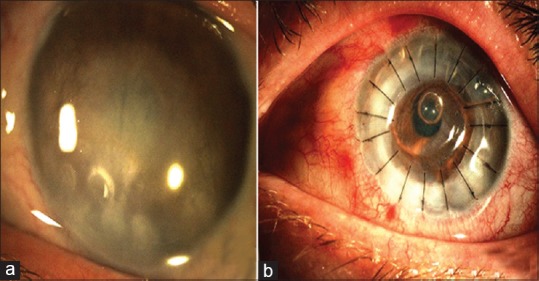
(a) Preoperative and (b) 1st day after surgery
In the DALK surgery of our case, the stromal layer at the top was resected after performing air injection for two times [Figure 2a–c]. However, by the help of the air bubbles in the anterior chamber, it was observed that BB did not develop and DM did not separate [Figure 2d]. Air was applied on DM for the third time with a view to forming BB. It was observed that DM was separated with the peripheral movements of the air bubbles in the anterior chamber. Posterior stroma was divided into quarters.
Figure 2.
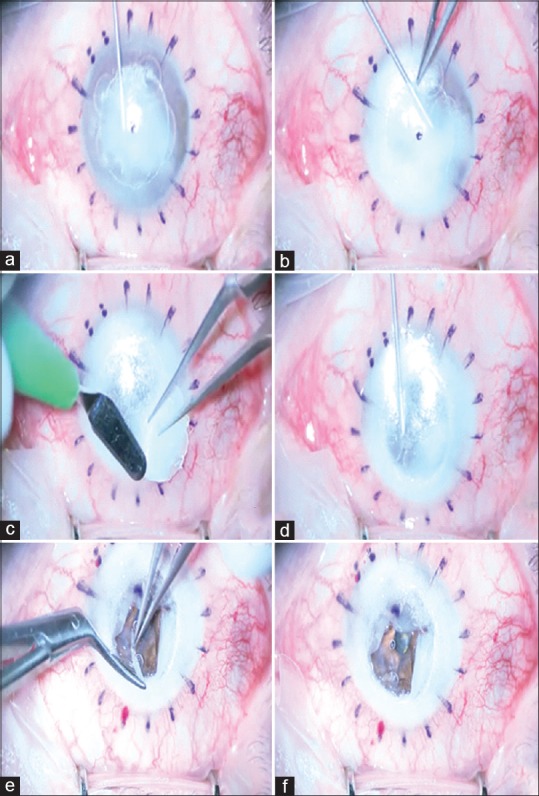
Figures of DALK surgery (a) first air injection, (b) second air injection, (c) resection of anterior stroma, (d) third air injection, (e) resection of one-quarter of the posterior stroma, (f) hole on the central DL. DALK: Deep anterior lamellar keratoplasty, DL: Dua's layer
While picking up the remaining stromal pieces, we encountered DM-like DL structure, [Figure 2e]. We also observed perforation in the central part of DL [Figure 2f]. We wanted to resect and convert DALK to PKP due to this membrane which was assumed DM (see the video of surgery at the supplementary material).
However, with the removal of this layer, it was observed that the air bubbles in anterior chamber did not disperse, and DM and endothelium were intact [Figure 3a–d]. In this phase, Type 3 (mixed) BB was formed in our case, and it was realized that DM and DL were resolved separately. The remaining posterior stromal pieces and DL were resected [Figure 3e]. DM and donor cornea whose endothelium was peeled off were sutured to recipient cornea bed by separately, and the surgery was ended [Figure 3f].
Figure 3.
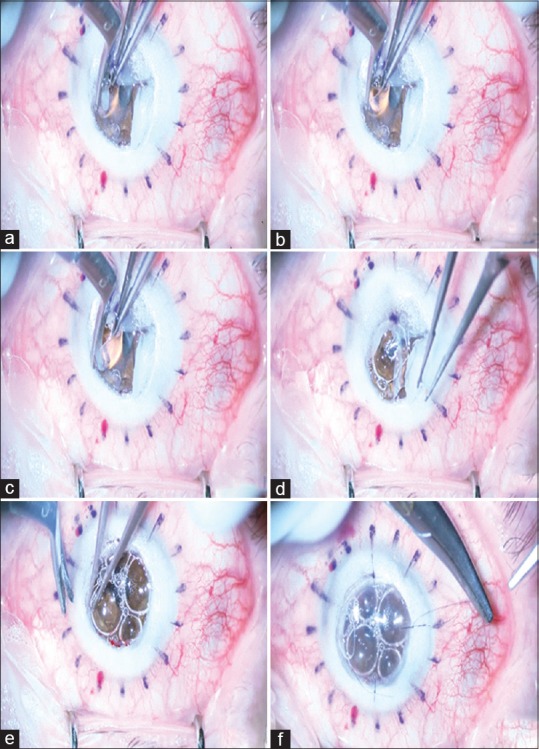
(a-d) Resection of DL, (e) resection of last quarter of the posterior stroma, (f) transplantation of graft with no DM and endothelium. DL: Dua's layer, DM: Descemet's membrane
On the 1st postoperative day and in the follow-ups, DM was attached, and graft transparency was achieved [Figure 1b].
Discussion
In the surgery of our case, we had difficulty in the phase of DM separation. Although we performed air injection two times, after trepanation, the cornea at the beginning, DM could not be separated. As a result of separately encountering DL structure which is DM and DM-like during the resection of the posterior stromal pieces, it was observed that mixed type BB was developed.
DL was reported to be durable membrane in a study.[3] Another study demonstrated a new technique called pre-Descemet's endothelial keratoplasty (PDEK). It was indicated that unrolling could be easier in anterior chamber with DL, DM, and endothelial.[4]
DL was defined in 2013, and its existence was supported in the experimental studies on donor corneas. This case made it possible to make an intraoperative definition of DL during DALK surgery and displayed how it could affect the course of the operation.
Conclusion
It is possible to encounter DL in a DALK surgery performed with mixed type BB. In these cases, the lamellar surgery should not be converted to penetrating surgery by mistake because of mixing DL and DM. In the present case, the authors have found that even if DL is removed, DALK surgery can be completed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Dua HS, Faraj LA, Said DG, Gray T, Lowe J. Human corneal anatomy redefined: A novel pre-Descemet's layer (Dua's layer) Ophthalmology. 2013;120:1778–85. doi: 10.1016/j.ophtha.2013.01.018. [DOI] [PubMed] [Google Scholar]
- 2.Tan DT, Dart JK, Holland EJ, Kinoshita S. Corneal transplantation. Lancet. 2012;379:1749–61. doi: 10.1016/S0140-6736(12)60437-1. [DOI] [PubMed] [Google Scholar]
- 3.Chérif HY, Gueudry J, Afriat M, Delcampe A, Attal P, Gross H, et al. Efficacy and safety of pre-Descemet's membrane sutures for the management of acute corneal hydrops in keratoconus. Br J Ophthalmol. 2015;99:773–7. doi: 10.1136/bjophthalmol-2014-306287. [DOI] [PubMed] [Google Scholar]
- 4.Agarwal A, Dua HS, Narang P, Kumar DA, Agarwal A, Jacob S, et al. Pre-Descemet's endothelial keratoplasty (PDEK) Br J Ophthalmol. 2014;98:1181–5. doi: 10.1136/bjophthalmol-2013-304639. [DOI] [PubMed] [Google Scholar]