

Abstract
Aim:
The aim of this study was to assess the existing knowledge, attitude, and practices of “oral health care” in the prevention of early childhood caries (ECCs) among parents of children in Belagavi city.
Materials and Methods:
A cross-sectional study was conducted in the outpatient Department of Pedodontics and Preventive Dentistry, KLE VK Institute of Dental Sciences, Belagavi, Karnataka. Institutional Ethical Clearance was obtained. The study was conducted during the month of April 2014 to October 2014 after taking prior informed consent from the 218 parents. Inclusion criteria were parents getting their children treated for dental caries and who were willing to participate. Parents who could not read and write were excluded from the study. The self-administered, close-ended questionnaire was written in English. It was then translated in local languages, i.e. Kannada and Marathi, and a pilot study was conducted on 10 parents to check for its feasibility and any changes if required were done.
Results:
The response rate was 100% as all 218 parents completed the questionnaire. Of 218 parents, 116 were mothers and 102 were fathers. The overall mean knowledge score was 69.5%. The overall mean attitude score was 53.5%. The overall attitude toward prevention of ECC was not in accordance to knowledge. The overall mean of “good” practices and “bad” practices score was 33.5% and 18.5%, respectively. Good knowledge and attitude toward oral health do not necessarily produce good practices.
Keywords: Attitude, early childhood caries, infant oral health, knowledge, practice
Introduction
Dental caries is the most common chronic disease of childhood, globally.[1] Although dental caries’ levels have been declining the world over, the problem of early childhood caries (ECCs) has remained unchanged in many areas of the world, especially the socially deprived.[2,3] Dental caries affecting the primary dentition of preschool children is referred to as ECCs. ECC is defined as “the presence of one or more decayed (noncavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child under the age of six.”[4] ECCs is a multifactorial disease with an etiology that involves a complex interaction between biological and socioeconomic factors. It is classified as mild, moderate, and severe. In children younger than 3 years of age, any sign of smooth-surface caries is indicative of severe ECCs (S-ECCs). From ages 3 through 5, 1 or more cavitated, missing (due to caries), or filled smooth surfaces in primary maxillary anterior teeth or a decayed, missing, or filled score of ≥4 (age 3), ≥5 (age 4), or ≥6 (age 5) surfaces constitutes S-ECC.[4]
ECC affects the deciduous dentition more commonly referred to as “milk” teeth. Deciduous teeth are very inappropriately referred to as “temporary teeth” when in reality they are responsible for general health, mastication, phonetics, esthetics and self-esteem, and also psychological comfort. Deciduous teeth are an integral part of oral, general health, and affect the quality of life.[5] Deciduous teeth if infected by dental caries can cause pain and disfigurement making children uncooperative for extensive treatment, sometimes necessitating the use of general anesthesia (GA). Treatment under GA in children is not without its associated risks. In addition, very few dentists are willing to do treatment in such young children due to its time-consuming nature, monetary returns and are not trained enough.[6,7,8]
Deciduous teeth and permanent teeth are directly related, and infection from deciduous teeth can directly pass on to permanent teeth.[9] To maintain the permanent teeth uninfected, dental practitioners advice pulp therapy or extraction and many parents prefer to get deciduous teeth extracted due to financial and time constraints.[10] Deciduous teeth are also the “best natural space maintainer.”[11]
Parents are responsible for their child's oral health care. Preschool children are not capable of brushing themselves and lack the manual dexterity and the psychological maturity to understand the importance of maintaining oral health. With changing lifestyles, a trend of having a single child and increased the cost of living, most of the parents are working with very less time left for performing day-to-day oral health care practices in their child's early years.[10] Especially in preschool children, parental role is the most important aspect of maintaining good oral health.[12,13]
In spite of two dental institutions in the Belagavi city, a recent study by Sankeshwari et al. reveals a high prevalence of dental caries, i e., 67.22%.[14] Tooth decay can be prevented and so can be ECC. It's indeed a matter of concern that in spite of so many “oral health promotion” activities, awareness campaigns, and advertisements on social media the prevalence of ECC is high. This study was undertaken with the aim of assessing the existing knowledge, attitude, and practices of oral health care in Belagavi city.
Materials and Methods
Study design
A cross-sectional study was conducted in the outpatient Department of Pedodontics and Preventive Dentistry, KLE VK Institute of Dental Sciences, Belagavi, Karnataka. Ethical clearance was obtained from the Research and Ethical Committee, VK Institute of Dental Sciences. The study was conducted during the month of April 2014 to October 2014 after taking prior informed consent from the parents who were willing to participate. Inclusion criteria were parents getting their children treated for dental caries or had a past dental history and who were willing to participate. In addition, parents with children with no medical conditions or no medications prescribed to them were included in the study. Child's age could be from being a newborn till 72 months of age (ECC is referred to caries in children <72 months of age)[4] and also parents having more than two children were included in the study. Parents who could not read and write were excluded from the study. In addition, parents who were not the primary caretakers of their children or who had children with medical problems were excluded from the study.
Sampling and sample size
Convenience sampling was considered, and sample size was calculated based on a formula by Cochran when population is >500, the approximate sample size should be 218 with margin error = 0.05 and data at t = 1.96.[15]
Methodology
The self-administered questionnaire written in English was adapted from Mani et al.[10] It had 29 items, 10 each in the knowledge and practice components and 9 in the attitude component, and took about 10–15 min to complete. It was then translated in local languages, i.e. Kannada and Marathi. These questionnaires were later back-translated in English and verified with the original English questionnaire by pediatric dentists who were well-versed in all the three languages. The scoring for practice was based 4-point Likert scale, respectively while the scoring for knowledge and attitude included true/false/do not know responses. All aspects of oral health promoting factors in children including oral hygiene, diet, and fluoride, and awareness regarding infant oral health and practices were addressed. Suggestions from public health dentists, regarding the content of all the three questionnaires, were also taken and incorporated.
A pilot study was conducted on 10 parents to check for its feasibility, clarity, comprehensiveness, and acceptability; any changes if required were done. The respondents opined to have understood the content of the questionnaire and, also, understood what it intended to measure. The pilot study responses were not considered in the main study. This pretested questionnaire addressed the knowledge, attitude, and practices of oral health care for prevention of ECC.
Results
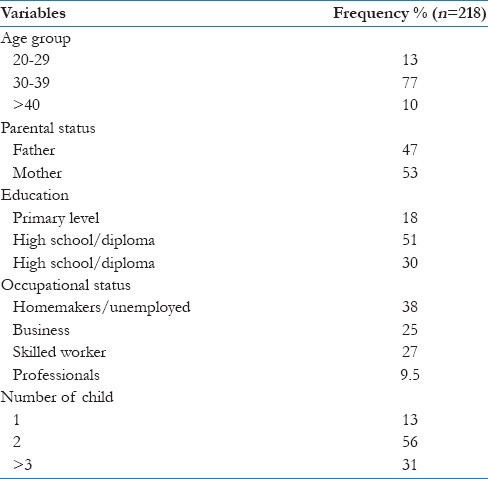
The response rate was 100% as all 218 parents completed the questionnaire. Of 218 parents, 116 were mothers and 102 were fathers. Nearly 77% of the participants were from 30 to 39 age groups. About 18% participants had primary education while 51%, i.e. maximum people had higher secondary education. Only 30% people had University level education, 38% of the participants were homemakers/unemployed, i.e., the mothers of children only. Other 61.5% people were either self-employed or salaried employees. Mothers had significantly better overall knowledge scores than fathers. In addition, participants with higher education level had significantly better overall knowledge scores than less educated parents [Table 1].
Table 1.
Sociodemographic characteristics of the study population
Knowledge
The overall mean knowledge score was 69.5%. The percentage of parents who answered correctly, for individual knowledge questions is shown in Figure 1. Nearly 69.5% of parents were aware that caries can affect infants below 2 years, but 19.5% of parents answered incorrectly, and 11% parents were in a dilemma about the same fact. When asked about food cariogenicity, 81.5% of parents knew that sweet food causes tooth decay but knowledge regarding when to begin using fluoridated toothpaste and whether deciduous teeth need treatment appeared to be low, i.e., 54% and 42.5%, respectively. However, 88% parents were knowing the importance of brushing teeth and 73.5% parents were aware of starting top-up foods along with breast/bottle feedings from 6 months of age.
Figure 1.
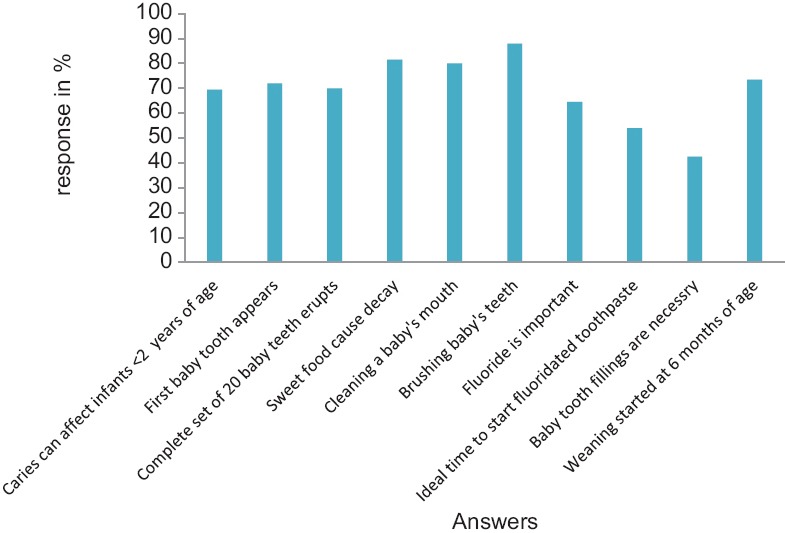
Percentage of correct answers for knowledge questions
Attitude
The overall mean attitude score was 53.5%. The overall attitude toward prevention of ECC was not in accordance to knowledge which had an average of 69.5%. The percentage of participants who correctly answered individual attitude questions is shown in Figure 2. Only 40.5% parents were aware that dental caries can be transmitted by sharing feeding utensils, i.e., mainly through saliva; on the contrary, majority, i.e., 45.5% parents believed it cannot be transmitted from parents to children. Similarly, night time bottle feeding is harmful was known to 45.5% parents but prolonged and frequent breastfeeding too can be harmful was known to only 39.5% parents while 48.5% disbelieved it. The most surprising revelation was that most of the parent's, i.e., 50.5% believed children can brush their teeth independently. Only 60% parents responded positively regarding child visit to dentist before 2 years of age. Attitude is just above 50%; hence, we can say it is above average, but parents need to be educated and motivated to improve their attitude toward prevention of ECC.
Figure 2.
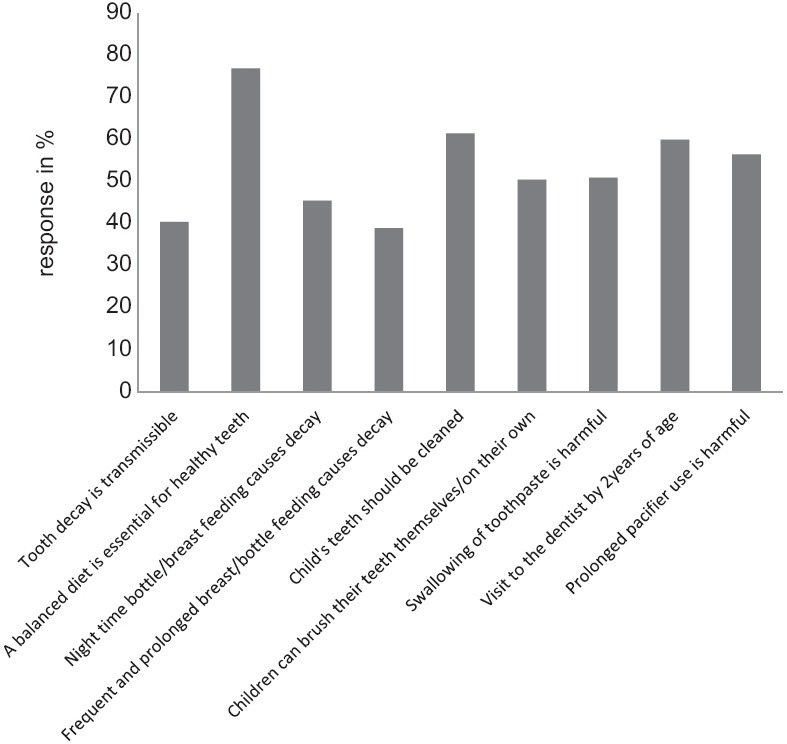
Percentage of correct answers for attitude questions
Practices
The practices were categorized into “good” practices and “bad” practices. The overall mean good practice and bad practice score were 33.5% and 18.5%, respectively. An analysis of the practice score for individual questions is shown in Figure 3. The most prevalent bad practice was giving sweet food frequently, i.e., 49.5%. Good practices for the instance use of fluoridated toothpaste was relatively low, i.e., 56%. The percentage prevalence of bad practices is low, but good practices are also relatively low. Therefore, good practices need to be increased. The education level of the parents had a positive effect on their practices. Parents who did not complete a high school education had lower mean practice score than those with a higher education.
Figure 3.
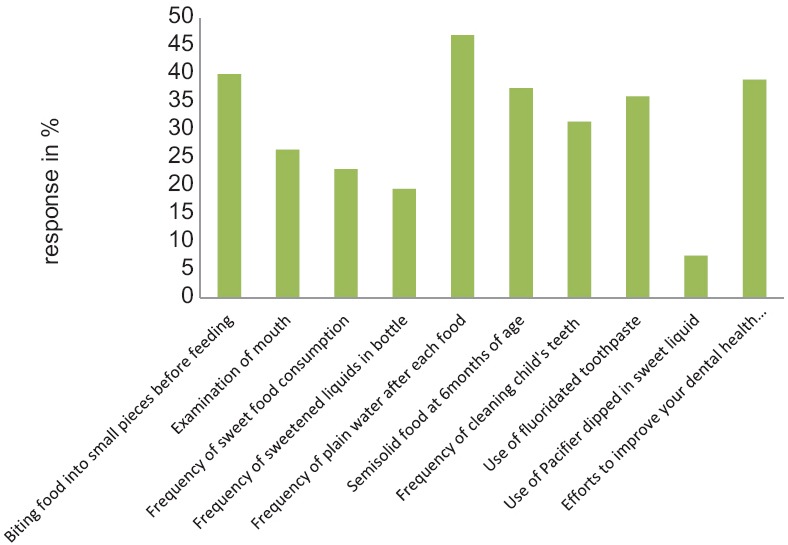
Percentage of correct answers for practice questions
To summarize, it is interesting to note that the percentage of knowledge about ECC in parents was high, i.e., 69.5%, followed by attitude, i.e., 53.5% but that of good practices was low, i.e., 33.56%.
Discussion
Parents are role models for their children. Children learn habits by imitating their role models and the best way to teach them is to practice these oral hygiene practices ourselves. Dental caries is a preventable disease and if it is noticed at an early stage, children cooperate better and parents save their valuable time and money spent on dental treatments which are also inclusive of the loss of pay for multiple visits for the treatment. Hence, prevention at the root level, i.e., primordial prevention and oral health education of parents is essential as the preschool age group (2–4 years of age) is dependent on them for their oral health care needs. Later, from 2 years onward, oral health promotion strategies such as fluoridated toothpaste, etc., can be begun in cooperation with the parents. To attain these goals, one needs to assess the existing levels of knowledge, attitude, and practices to bring about the necessary changes.
In addition, children with primary dentition affected by dental caries are prone to the development of dental caries in permanent dentition. Hence, children reinforced at an early age by their parents are motivated and trained for a lifetime.
Studies assessing the parents ability to care for child's oral health reveal that parents do not have enough time, lack of knowledge in brushing, job/employment stress, and last but not the least, due to nuclear families and working parents many parents do not raise their children themselves, and leave them at day-care centers or crèches.[16]
Several studies have found that good knowledge and attitude toward oral health does not necessarily produce good practices.[10,17,18] From this study, it is clear that awareness regarding bad practices is abundant which is indicated by the low prevalence, i.e. 18.5% approximately. This reveals an important take home message for us dentists that parents need to be trained and motivated to carry out oral hygiene practices in a proper way and efficiently. In addition, knowledge regarding the use of fluoridated toothpaste (level of evidence for the use of fluoridated toothpaste is 1++ to 1+)[4,19] and whether deciduous teeth need treatment appeared to be low, i.e., 54% and 62.5%, respectively.
In addition, a general low score was found in the knowledge, attitude, and good practices in infant oral health care such as timing for first dental visit, ideal time to start use of fluoridated toothpaste, need to restore deciduous teeth, ill-effects of night time, frequent and prolonged breast/bottle feeding, harm caused by swallowing of toothpaste.[4,10,16,20]
The role of bacteria in the causation of dental caries was not acknowledged by the majority of the parents which was reflected by the prevalent practice of sharing utensils and biting food into small pieces before feeding in this study. This is in accordance with studies by Mani et al. and Togoo et al.[20] The focus should be on parents/carers to encourage to limit their child childir childlent practice of sharing utensils and biting food iivated to carry out oral hygiene practices in a proper way carers and children should be advised that foods and drinks containing sugar substitutes are available, but should be consumed in moderation. Sugar-free medicines should be used when available. Parents/carers should be encouraged to brush their child childaged soon as the first tooth appears, using a soft toothbrush and water only. Children who use a baby bottle should be advised never to put sweet drinks, including fruit juice, into the bottle and breast-feeding should not be practiced at will of the child. Parents/carers should be advised not to let their child sleep or nap with a baby bottle or being breast-fed.[4,19,21] Other studies by Oredugba et al. and Al-Zahrani et al. also revealed that parents are aware of the fact that milk teeth are as important as permanent teeth and also affect the general health of the child.[22,23,24] In spite of these facts being known to parents, their inability to take proper oral health care is indeed surprising, and the hurdles in practicing oral health practices along with other reasons behind this situation can be further explored using qualitative study.
The limitations of this study were that it was carried out in one institution only by convenience sampling or nonprobability sampling with a small sample size.
Conclusion
This study shows that in spite of good knowledge among parents, their attitude, and practices are lacking to keep up with necessary standards. Parents play a pivotal role and are the primary caretakers. Therefore, the main focus should be on parents during oral health promotion for children, especially of preschoolers and children <6 years. In addition, awareness to visit the dentist before child's first birthday should be insisted.[4]
Parents should be informed to brush their children's teeth at least once by parents themselves at night before going to bed. This shows that parents need to be trained and motivated to carry out oral hygiene practices in a proper way and efficiently.[4,19,21]
In addition, due to inability of parents to carry out oral hygiene practices, additive professional preventive practices such as (a) topical fluoride application and, (b) pit and fissure sealants should be carried at primary health centers (PHCs) along with vaccinations after complete eruption of all deciduous teeth, especially deciduous molars as they have a longer lifespan in the oral cavity of children. For this purpose, more dentists should be recruited in PHCs or else nurses should be trained in carrying out these preventive therapies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to thank all the parents who participated in the study and spared their time to fill the questionnaire. We would also like to acknowledge Dr. Shilpa Salsawad, Dr. Chandrashekhar, Dr. Vidyavathi, and Dr. Neeraj Gokhale for their help in the process of Kannada and Marathi translations as also the back-translation of the questionnaires.
References
- 1.Douglass JM, Douglass AB, Silk HJ. A practical guide to infant oral health. Am Fam Physician. 2004;70:2113–20. [PubMed] [Google Scholar]
- 2.Bedi R, Lewsey JD, Gilthorpe MS. Changes in oral health over ten years amongst UK children aged 4-5 years living in a deprived multiethnic area. Br Dent J. 2000;189:88–92. doi: 10.1038/sj.bdj.4800692. [DOI] [PubMed] [Google Scholar]
- 3.Williams NJ, Whittle JG, Gatrell AC. The relationship between socio-demographic characteristics and dental health knowledge and attitudes of parents with young children. Br Dent J. 2002;193:651–4. doi: 10.1038/sj.bdj.4801652. [DOI] [PubMed] [Google Scholar]
- 4.American Academy of Pediatric Dentistry. Policy on early childhood caries (ECC): Classifications, consequences, and preventive strategies. Pediatr Dent 2014. 2015;36:50–2. [PubMed] [Google Scholar]
- 5.Sheiham A. Oral health, general health and quality of life. Bull World Health Organ. 2005;83:644. [PMC free article] [PubMed] [Google Scholar]
- 6.Almeida AG, Roseman MM, Sheff M, Huntington N, Hughes CV. Future caries susceptibility in children with early childhood caries following treatment under general anesthesia. Pediatr Dent. 2000;22:302–6. [PubMed] [Google Scholar]
- 7.Tate AR, Ng MW, Needleman HL, Acs G. Failure rates of restorative procedures following dental rehabilitation under general anesthesia. Pediatr Dent. 2002;24:69–71. [PubMed] [Google Scholar]
- 8.Halawany HS, Al-Fadda SA, Hussain BK, Al-Homaied MA. The attitude of private dental practitioners towards treatment and management of children in Riyadh, Saudi Arabia. J Pak Dent Assoc. 2011;20:245–9. [Google Scholar]
- 9.Cordeiro MM, Rocha MJ. The effects of periradicular inflamation and infection on a primary tooth and permanent successor. J Clin Pediatr Dent. 2005;29:193–200. doi: 10.17796/jcpd.29.3.5238p10v21r2j162. [DOI] [PubMed] [Google Scholar]
- 10.Mani SA, John J, Ping WY, Ismail NM. Knowledge, attitude and practice of oral health promoting factors among caretakers of children attending day-care centers in Kubang Kerian, Malaysia: A preliminary study. J Indian Soc Pedod Prev Dent. 2010;28:78–83. doi: 10.4103/0970-4388.66741. [DOI] [PubMed] [Google Scholar]
- 11.Wright GZ, Kennedy DB. Space control in the primary and mixed dentitions. Dent Clin North Am. 1978;22:579–601. [PubMed] [Google Scholar]
- 12.Castilho AR, Mialhe FL, Barbosa Tde S, Puppin-Rontani RM. Influence of family environment on children's oral health: A systematic review. J Pediatr (Rio J) 2013;89:116–23. doi: 10.1016/j.jped.2013.03.014. [DOI] [PubMed] [Google Scholar]
- 13.Naidu R, Nunn J, Forde M. Oral healthcare of preschool children in Trinidad: A qualitative study of parents and caregivers. BMC Oral Health. 2012;12:27. doi: 10.1186/1472-6831-12-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sankeshwari RM, Ankola AV, Tangade PS, Hebbal MI. Feeding habits and oral hygiene practices as determinants of early childhood caries in 3- to 5-year-old children of Belgaum City, India. Oral Health Prev Dent. 2012;10:283–90. [PubMed] [Google Scholar]
- 15.Barlett JE, Kotrlik JW, Higgins CC. Organizational research: Determining appropriate sample size in survey research. Inf Technol Learn Perform J. 2001;19:43–50. [Google Scholar]
- 16.Ashkanani F, Al-Sane M. Knowledge, attitudes and practices of caregivers in relation to oral health of preschool children. Med Princ Pract. 2013;22:167–72. doi: 10.1159/000341764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Colak H. Do the more caries in early primary dentition indicate the more caries in permanent dentition? Results of a 5-years follow-up study in rural-district. J Int Soc Prev Community Dent. 2012;2:48–52. doi: 10.4103/2231-0762.109364. D72-167-7. CT. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mitrakul K, Laovoravit V, Vanichanuwat V, Charatchaiwanna A, Charatchaiwanna A, Bunpradit W, et al. Factors associated with parent capability on child's oral health care. Southeast Asian J Trop Med Public Health. 2012;43:249–55. [PubMed] [Google Scholar]
- 19.Irish Oral Health Services Guideline Initiative. Strategies to Prevent Dental Caries in Children and Adolescents: Guidance on Identifying High Caries Risk Children and Developing Preventive Strategies for High Caries Risk Children in Ireland. 2009 [Google Scholar]
- 20.Nagarajappa R, Kakatkar G, Sharda AJ, Asawa K, Ramesh G, Sandesh N. Infant oral health: Knowledge, attitude and practices of parents in Udaipur, India. Dent Res J (Isfahan) 2013;10:659–65. [PMC free article] [PubMed] [Google Scholar]
- 21.Bertness J, Holt K. Promoting Oral Health in Young Children: A Resource Guide. Washington, DC: National Maternal and Child Oral Health Resource Centre; 2013. [Google Scholar]
- 22.Togoo RA, Zakirulla M, Yaseen SM, Nasim VS, Al Qahtani AR, Al-Turki AA. Cross-sectional study of awareness and knowledge of causative factors for early childhood caries among Saudi parents: A step towards prevention. Int J Health Sci Res. 2012;2:1–7. [Google Scholar]
- 23.Oredugba F, Agbaje M, Ayedun O, Onajole A. Assessment of mothers’ oral health knowledge: Towards oral health promotion for infants and children. Health. 2014;6:908–15. [Google Scholar]
- 24.Al-Zahrani AM, Al-Mushayt AS, Otaibi MF, Wyne AH. Knowledge and attitude of Saudi mothers towards their preschool children's oral health. Pak J Med Sci. 2014;30:720–4. doi: 10.12669/pjms.304.5069. [DOI] [PMC free article] [PubMed] [Google Scholar]