

Abstract
Background:
Developmental disability is a term that refers to permanent cognitive and or physical impairment. Arrested development of physical or mental capacities can lead to number of problems for the sufferer as well as the carers.
Methodology:
This study was conducted to assess the quality of life (QOL) and coping mechanisms used by the carers of physically challenged children. In this cross-sectional study, all the 116 children from a school for children with special needs in Anand, Gujarat and their carers were included. World Health Organization-QOL (WHO-QOL) and BREF COPE were administered to measure QOL and coping strategies, respectively.
Results:
On WHO-QOL, the social relationship domain was observed to be the best while environment domain had the lowest score. The main coping style used by the caregivers was Active emotional coping.
Conclusions:
Significant differences were found in QOL of the caregivers of physically challenged children based on the type of disability of the child. Rehabilitation programs can be planned to provide psychological support to the caregivers to ease the burden if any through collaborative efforts.
Keywords: Carers of differently abled children, coping, developmental disability, quality of life
Introduction
Developmental disability refers to a range of conditions including intellectual disability, cerebral palsy, autistic spectrum disorder, learning disability, epilepsy, etc., Most childhood disabilities are referred to as developmental disabilities, defined as any physical or mental condition that may impair or limit a child's ability to develop cognitively, physically, and emotionally compared to other children.[1] Most of the disabilities unlike physical, which are noticed at birth, get undiagnosed until a child enters a school. It is difficult for parents to identify a developmental disability as they are normally not aware about the developmental stages of a child and more so if it is their first child. Professionals often have difficulty diagnosing a specific disability at such an early age, so the term developmental delay is utilized to qualify a child for services in infant and preschool programs.[2]
A disabled child's family adjusts on several aspects in life to suit his needs. The physical and mental stress associated with raising such children could be multifold. Caring for such children can be a physically and mentally tasking job, depending on the type of disability resulting in compromised quality of life (QOL) of the carers too. While treating and rehabilitating the disabled children, the needs of the carers are seldom thought about. It is quite possible that even the carers need help to cope with the physical, mental and emotional stress they bear while caring for their loved one. QOL as defined by the World Health Organization (WHO) is an individual's perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards, and concerns. Coping strategies can be defined as “the cognitive and behavioral efforts required to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person.”[3]
Care that is given to a normal child itself is taxing for the parents many a times and to provide a higher level of life long care to a child suffering from long-term functional limitations may be strenuous for the parents and thereby may be affecting their QOL. Becoming the parent of a child who has some disability in itself can be a time of great stress and change.[4] The birth of a disabled child can influence the relationships of all the family members. It also requires a reassessment of the family functioning.[5] Majority of families cope with the situation relatively well and are able to continue their life normally.[6] However, coping with a physically or intellectually disabled child is a highly individual process, and there is evidence to suggest that some families may never adjust fully to this event.[7] Coping requires a cognitive reappraisal of the situation to manage it properly. A number of studies have concentrated on the degree to which families with disabled children feel stress, how they manage, what factors support them, and what coping strategies they use.[8]
Disability in India
Over the last 50 years, right to education has evolved in India inspired by a host of factors including judicial interpretations, enactment of special laws, and amendment to the constitution. The constitution of India has made education a fundamental right for all children including the children with disabilities in the age group of 6–14 years. Section 26 of Persons with Disabilities Act (1995) affirms the capacity of Indian state to afford free education beyond 14 years of age, particularly in the context of children with disabilities.
According to the Census (2001), there are 2.19 crore people with disabilities in India who constitute 2.13% of the total population. This includes persons with visual, hearing, speech, loco motor, and mental disabilities. Seventy-five per cent of persons with disabilities live in rural areas, 49% of disabled population is literate and only 34% are employed. The earlier emphasis on medical rehabilitation has now been replaced by an emphasis on social rehabilitation. Approximately 3–5% of the population of children experience or get affected with physical, intellectual, and mental health problems according to the National Health Survey.
The Persons with Disability Act, 1995 is built on the premise of equal opportunity, protection of rights and full participation. It provides definitions of disabled person by following the medical model. According to the Persons with Disabilities (Equal Opportunities, Protection of Rights and Full Participation) Act, 1995, “person with disability” means a person is suffering from not <40% of any disability as certified by a medical authority (any hospital or institution, specified for the purposes of this act by notification by the appropriate government).
It is also important to note that caring for a child with disability does not equally affect all parents. There are families who cope well despite the adversity. There could be number of factors that can affect the QOL of carers which could include severity of the disability of the child, presence of cognitive or behavioral problems, socioeconomic status of the families, lack of education, low social support, etc., Therefore, the following study has been undertaken to assess the QOL and also the kind of strategies used by the carers of disabled children.
Objectives
To explore the QOL of parents of children with developmental disabilities
To find out the coping strategies used by the parents of such children
To study the differences in the (QOL) of parents having a child with disability based on the type of disability variable.
Inclusion criteria
Caregivers meeting following inclusion criteria were included in the study: Caregiver having child/children with mental or physical incapacity either congenital or caused by injury and caregiver being the main carer of the disabled child.
Exclusion criteria
Carer who have not been living with the physically challenged child for continuous 2 years and caregiver having any severe mental illness reported at the time of interview.
Methodology
The study assesses the QOL and coping styles of caregivers of disabled children. Total 116 caregivers were included in the study. Apart from the information collected on basic demographic data, the following tests were administered to the caregivers of the mentally and physically challenged children.
World Health Organization-quality of life BREF
It is a self-administered instrument developed by WHO and translated and validated in Gujarati by the investigator. The scale contains 26 questions which measure four domains. The WHO-QOL scale places emphasis on subjective evaluation of respondent health and living conditions rather than their objective functional status. Four domains of QOL are measured: Physical health, psychological health, social relationship, and environment. The scale has 26 items, with total score range of 26–130. Its psychometric properties have been found to be comparable to that of the full version WHO-QOL - 100. This scale has shown good discriminant validity; content validity, internal consistency, and test-retest reliability.[9]
Brief COPE (Carver, 1997)
The Brief COPE[10] is a 28-item measure of coping style use derived from the longer COPE inventory.[11] It is a self-administered scale translated and validated in Gujarati. The brief COPE uses a 4-point Likert scale (I have not been doing this at all to I have been doing this a lot). It includes 14 subscales of two items each grouped into these three coping categories by summing items accordingly (with higher scores indicating a greater intensity of use of the coping strategy). The three coping strategies and their associated subscales were problem-focused coping (active coping, planning, instrumental support, and religion scales); active emotional coping (venting, positive reframing, humor, acceptance, and emotional support scales); and avoidant emotional coping (self-distraction, denial, behavioral disengagement, self-blame, and substance use scales).
Results
All 116 parents having a disabled child attending a special school were approached for participation in the study. Of 116 parents, 10 refused to fill the QOL questionnaire while total 18 parents denied to take the coping questionnaire. The demographic details of the not responding parents in QOL and COPE questionnaire was seen to be comparable to the responding ones (P < 0.05).
Table 1 shows the age and intelligence quotient (IQ) distribution of the participating children. There were 83 parents having a male child and 33 having a female child with some disability. The majority of the disabled were in the age group 6–12 years (65%) and next frequent age group was 13–18 years (31%).
Table 1.
Sex wise and age wise intelligence quotient distribution of the children with disability
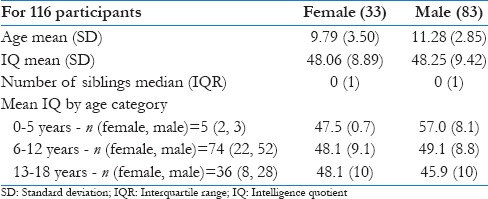
Out of 116 children, irrespective of age, the IQ scores of most of the participants (67) were in the moderate category while the decline in IQ scores was seen in age group (6–12 years). Of 33 females, the IQ scores of 17 participants lie in the moderate category with a major decline in 6–12 age group. Similarly, of 83 males, 50 lie in the moderate category. The majority of the children (58%) had a moderate (40–54 IQ score) level of retardation while 16% had severe retardation (IQ score 25–39).
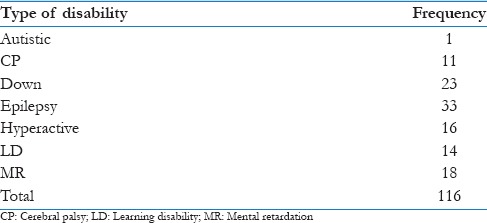
Eighty percent of caregivers had at least one more child other than the child attending the special school. There was, however, no association found between the number of children and QOL of the caregivers. The majority of children had a speech problem (74%). Ten percent of children had hyperactivity, and another 10% were having down syndrome. Learning disorder was observed in 12% children and also another 2% children had emotional problems [Table 2].
Table 2.
Disability wise frequency distribution of children
Most of the female participants (56%) and male participants (64%) did not have siblings. There was no association found between number of siblings and sex of the physically challenged child (P = 0.718) on applying Chi-square test.
Table 3 shows the mean scores and standard deviation (SD) for each domain of parents having a child with a disability on the WHOQOL scale. According to the domains scores, DOMAIN 3 (social relationship) had the highest score (both mean and median), whereas the domain 4 (environmental) had the lowest scor (both mean and median), suggesting that QOL is best in domain 3 and worst in domain 4.
Table 3.
Domain wise distribution of World Health Organization quality of life scores of carers
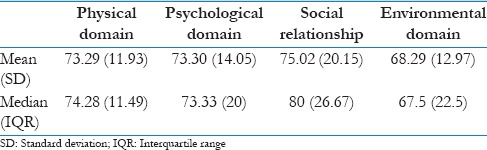
The coping style used by the caregivers mainly was active emotional coping (mean = 28.26, SD = 4.886).
The mean and SD have been extracted of parents’ “total” and also domain wise scores on the WHOQOL scale (data of some of the participants could not be gathered for QOL and coping due to availability and feasibility issues of the participants). ANOVA test suggested a significant difference in scores when the mean QOL scores of parents were compared by the type of their child's disability for social relationship domain and overall score. The post hoc analysis of the same using Least Significant Difference method indicated that the social relationship domain scores of parents of children with epilepsy was significantly lower against parents with children having Down's syndrome (P = 0.004) and hyperactivity (P = 0.008). The overall QOL score was also observed to be lowest for carers of epilepsy children (significantly lower compared to carers with children having Down's syndrome (P = 0.017) and hyperactivity (P = 0.009) [Table 4].
Table 4.
Comparison of mean (standard deviation) quality of life scores domain-wise by type of disability

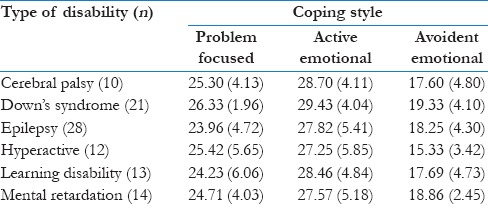
As given in Table 5, the main coping strategy used by parents of learning disabled, epilepsy and Cerebral Palsy was Active emotional. Problem focused coping was mainly used by parents of child with Down syndrome while avoidant emotional coping was used by parents of children with attention-deficit/hyperactivity disorder (ADHD). An interesting finding shows that parents of mentally retarded children used both Problem focused and active emotional coping equally.
Table 5.
Coping strategies and type of disability
Discussion
This study investigated the QOL of parents having a child with a developmental disability. The results of this study postulated that there are significant differences in the QOL of parents having a child with a disability based on the type of disability. Parents having a child with Down syndrome and ADHD had the lowest QOL scores while parents having a child with speech problems had the highest degree of QOL. The highest scores in domain 3, i.e., the social relationship can be attributed to the joint family culture in general and support provided from the spouse as well as the society which helps these parents in dealing with severe stress while domain 4, i.e., environment domain had the lowest scores indicating that the financial resources and leisure activities are greatly affected in such homes.
The results of this study suggest that all three coping mechanisms are relevant to parents having a child with developmental disabilities. Active avoidance coping and problem-focused coping appear to map quite clearly onto a typical emotion focused versus problem focused categorization prevalent in much stress and coping research.[12] Problem focused coping and active emotional coping in this study is associated with good QOL. The coping style mainly used by the caregivers was active emotional coping which is an unhelpful approach in dealing with the demands of raising children with disabilities. According to their responses, the parents have accepted the situation and trying to look for something good in it, they try to make fun of the situation which can provide an outlet for stress for some time but which is more of an escape tendency which does not help them realistically in dealing with the situation in the long run.
The QOL of the parents who get social support is good because in Indian setting family plays an important role in providing support to the distressed members and the members stay together at the time of crisis. Open communication is allowed in well-functioning families and it has been reported as a supportive factor in many family studies.[13] Family cooperation helped them to cope with the situation in a better way. Moreover, the spouse support in taking care of the child as well as supporting each other helped them in care taking. Some of the mothers had left their jobs and sit the whole day in the school with the child to see and repeat the same activities at home. It also helps the parent in the emotional release,[14] parents regarded family cohesion and co-operation as the factor most helpful for coping.[15] The fact that the spouses support each other,[16] and share caretaking tasks and other housework equally is of major importance for their marital relationship.[17]
There can be many reasons for using problem focused and active emotional (both positive) coping in parents of children with developmental disabilities. The parents felt that a realistic outlook of the child's disability and acceptance of the situation had helped them to cope. After the information provided by the schools and other agencies about the supporting systems available, they were more optimistic about the future of the child. Putting the child in a special school helps the parents to find out other parents who are also facing the same problems and sharing of their concerns and problems helps them cope better. Informal support from friends and relatives was regarded as essential for managing in everyday life. Parental positive perceptions about children with disabilities might also serve as an adaptive function by helping parents to cope with relatively high levels of stress. Because of the acceptance of their child's status, parents had a realistic and optimistic attitude towards their own and their child's life and future. Since all the children were from special schools, this also indicates parents’ positive approach to give a better platform to their child.
The parents who acquired an avoidant way of coping reported more of a fearful attitude and following a kind of escapism not to acknowledge the problem and think about it at all. They considered it as an extra burden on their shoulders which they have to carry somehow. They felt cheated and also felt a kind of social isolation where people looked at them in a different way. They also felt ashamed of their situation. In these cases, parents were mainly discussing the problems caused by the child and not emphasizing the efforts they are taking to cope with it. Whereas the parents may suspect that something is wrong with their child, uncertainty about what it is or unwillingness to admit it may give rise to insecurity and frustration in the family, which strains the relationship between the spouses and also affects the siblings.[5] Some of the parents perceived their physically challenged child as an extension of themselves and felt ashamed, socially rejected, ridiculed or embarrassed. Parents’ reactions may be affected due to economic status, level of stress, personality traits, emotional maturity or immaturity, and marital stability or status. Adequate information about the child's disability is important and helps the parents to cope, whereas an ambiguity of diagnosis and expectations give rise to stress and isolation in the family.[13] Complete education and information about the child's disability seemed to be a very important factor for good parental coping.
Behavioral and developmental disability were associated with higher parenting stress than medical disability.[18] Many researchers from India have reported that people often find relief in religious propitiation and surrender to the will of God when faced with intractable disease and disability.[19] Higher parenting stress in parents of girls raises the possibility of abuse and neglect. Little support from informal family resources underscores the need for developing formal resources for supporting the parents.[20] Lower socioeconomic status of the family is reported to be associated with more stress because of fewer resources.[21] Due to poverty in the family; a child with a disability is regarded as a burden, an evil spirit, and an object of charity without rights, rather than as an unfortunate child.[22]
Research in India has indicated that receiving maximum social-emotional support from the spouse, family members, relatives, and friends are facilitators for effective coping. The physical support from within and outside the family is one of the greatest facilitators in coping.[23] A study designed to understand the differences in perceived disability impact and related coping in mothers having children with intellectual disabilities alone compared to those having children with intellectual disabilities and additional disabilities found that group differences for disability impact were present in specific domains but not overall. Both positive and negative coping strategies were observed in both groups.[24] Another study documenting family coping using a pretested self-administered questionnaire found that 74% families had adequately adapted to having a mentally retarded child in their family, as measured on the global adaptation scale. The remaining 26% families had inadequately adapted, of which 7% showed poor coping.[25] Present research indicates 28% of the parents are extremely well adapted, whereas 8% of the parents show very poor coping or adaptation on global adaptation scale. The social support or self-help groups have become increasingly popular forms of family support among families who have children with disabilities.[26]
In a qualitative study of parents of children with physical and/or intellectual disabilities, it was found that families with better functioning actually searched for information about the disability and its treatment, worked to maintain family cohesion by sharing problems and seeking emotional support among family members, sought social support (both from formal health resources and by contacting other parents of children with disabilities and family and friends), expressed their emotions, looked for a space to be on their own and practice their hobbies and also had higher self-confidence and self-efficacy.[27] How well a family copes with the disability depends on multiple factors, including parental support, the parents’ evaluation of the situation, their ability to function, and any additional stress they are experiencing.[28] Parental attitudes influence the way parents treat their children and their treatment of the children, in turn, influences their children's attitudes toward them and the way they behave.[29]
Conclusion
To conclude, the results of the study postulated that there were significant differences in the QOL of parents having a child with a disability based on the type of disability the child had. Parents having a child with ADHD had the highest QOL scores while parents having a child with epilepsy had lowest QOL score overall.
Limitations
Any interpretation or generalization of the present findings should take into consideration some possible limitations of the study. First, the sample size is small and may affect the strength of the results. These children with disabilities were all attending the same special school (not representative of all socioeconomic classes). We need a large sample to validate the findings of this study. This is a cross-sectional study that does not allow us to find causal relations. More variables could be included to understand the relationship between various variables better.
Suggestions
By recognizing the coping strategies used by the family and the risk indicators of poor coping, professionals and service providers can find suitable ways to support family adaptation. The QOL of child and the family gets affected differently in different disabilities which again requires further empirical research. As the role of physicians, nursing staff and other professionals in this process is very important, more attention should be focused on the collaboration between these groups.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank the administration of the special school and the participants of the study for all the support and co-operation.
References
- 1.Pueschel SM, Bernier JC, Weidenman LE. The Special Child. Baltimore, MD: Paul H. Brooks Publishing Co; 1988. [Google Scholar]
- 2.Aron LY, Loprest PJ, Steuerle CE. Serving Children with Disabilities. Washington, D.C: Urban Institute Press; 1996. [Google Scholar]
- 3.Lazarus RS, Folkman S. Stress, Appraisal and Coping. New York: Springer; 1984. [Google Scholar]
- 4.Thompson CE. Raising a Handicapped Child. New York: Oxford University Press Inc; 2000. [Google Scholar]
- 5.Dyson L, Edgar E, Crnic K. Psychological predictors of adjustment by siblings of developmentally disabled children. Am J Ment Retard. 1989;94:292–302. [PubMed] [Google Scholar]
- 6.Rimmerman A. Provision of respite care for children with developmental disabilities: Changes in maternal coping and stress over time. Ment Retard. 1989;27:99–103. [PubMed] [Google Scholar]
- 7.Koller H, Richardson SA, Katz M. Families of children with mental retardation: Comprehensive view from an epidemiologic perspective. Am J Ment Retard. 1992;97:315–32. [PubMed] [Google Scholar]
- 8.Beckman PJ. Comparison of mothers’ and fathers’ perceptions of the effect of young children with and without disabilities. Am J Ment Retard. 1991;95:585–95. [PubMed] [Google Scholar]
- 9.WHO. Manual of the International Classification of Disease, Injuries and Causes of Death. Vol. 1, 10th revision. Geneva: WHO; 1992. [Google Scholar]
- 10.Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. 1998;28:551–8. doi: 10.1017/s0033291798006667. [DOI] [PubMed] [Google Scholar]
- 11.Carver CS. You want to measure coping but your protocol's too long: Consider the brief COPE. Int J Behav Med. 1997;4:92–100. doi: 10.1207/s15327558ijbm0401_6. [DOI] [PubMed] [Google Scholar]
- 12.Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. J Health Soc Behav. 1980;21:219–39. [PubMed] [Google Scholar]
- 13.Beavers J, Hampson RB, Hulgus YF, Beavers WR. Coping in families with a retarded child. Fam Process. 1986;25:365–78. doi: 10.1111/j.1545-5300.1986.00365.x. [DOI] [PubMed] [Google Scholar]
- 14.Burr WR, Klein SR, Burr RG, Doxey C, Harker B, Holman TB, et al. Re-examining Family Stress: New Theory and Research. Thousand Oaks, CA: Sage; 1994. [Google Scholar]
- 15.Barbarin OA, Hughes D, Chesler MA. Stress, coping, and marital functioning among parents of children with cancer. J Marriage Fam. 1985;47:473–80. [Google Scholar]
- 16.Snowdon AW, Cameron S, Dunham K. Relationships between stress, coping resources, and satisfaction with family functioning in families of children with disabilities. Can J Nurs Res. 1994;26:63–76. [PubMed] [Google Scholar]
- 17.Benson BA, Gross AM. The effect of a congenitally handicapped child upon the marital dyad: A review of the literature. Clin Psychol Rev. 1989;9:747–58. [Google Scholar]
- 18.Gupta VB. Comparison of parenting stress in different developmental disabilities. J Dev Phys Disabil. 2007;19:417–25. [Google Scholar]
- 19.Dalal AK. Living with chronic disease: Healing and psychological adjustment in Indian society. Psychol Dev Soc. 2000;12:67–82. [Google Scholar]
- 20.Gupta VB, Mehrotra P, Mehrotra N. Parental stress in raising a child with disabilities in India. J Disability CBR Inclusive Dev. 2012;23:41–52. [Google Scholar]
- 21.Sameroff AJ, Seifer R, Barocas R, Zax M, Greenspan S. Intelligence quotient scores of 4-year-old children: Social-environmental risk factors. Pediatrics. 1987;79:343–50. [PubMed] [Google Scholar]
- 22.Pal DK, Chaudhury G. Preliminary validation of a parental adjustment measure for use with families of disabled children in rural India. Child Care Health Dev. 1998;24:315–24. doi: 10.1111/j.1365-2214.1998.tb00950.x. [DOI] [PubMed] [Google Scholar]
- 23.Peshwaria R. Parent involvement in the training and management of their mentally handicapped persons. J Pers Clin Stud. 1989;5:217–21. [Google Scholar]
- 24.Kishore MT. Disability impact and coping in mothers of children with intellectual disabilities and multiple disabilities. J Intellect Disabil. 2011;15:241–51. doi: 10.1177/1744629511431659. [DOI] [PubMed] [Google Scholar]
- 25.Farheen A, Dixit S, Bansal SB, Yesikar V. Coping strategies in families with mentally retarded children. Indian J Pract Doct. 2008;5:11–12. [Google Scholar]
- 26.Pearson JE, Sternberg A. A mutual help project for families of handicapped children. J Couns Dev. 1986;65:213–5. [Google Scholar]
- 27.Taanila A, Järvelin MR, Kokkonen J. Parental guidance and counselling by doctors and nursing staff: Parents’ views of initial information and advice for families with disabled children. J Clin Nurs. 1998;7:505–11. doi: 10.1046/j.1365-2702.1998.00190.x. [DOI] [PubMed] [Google Scholar]
- 28.McCubbin HI, Patterson JM. In: The family stress process: The double ABCX model of adjustment and adaptation. Social Stress and the Family. McCubbin HI, Sussman MB, Patterson JM, editors. New York: Hawthorne Press; 1983. pp. 7–37. [Google Scholar]
- 29.Gallimore R, Weisner T, Kaufman S, Fernheimer L. The social construction of ecocultural niches: Family accommodation of developmentally delayed children. Am J Ment Retard. 1989;94:216–30. [PubMed] [Google Scholar]