

Abstract
Background:
Nearly 14% of children worldwide do not reach their developmental potential in early childhood. The early identification of delays in achieving milestones is critical. The World Health Organization (WHO) has developed normal age ranges for the achievement of motor milestones by healthy children. This study aimed to assess the gross motor developmental achievements and associated factors among children in rural India.
Materials and Methods:
A cross-sectional study was conducted with rural children in North India. A pretested questionnaire was used to collect the data. The median age at the time of the highest observed milestone was calculated and compared with the WHO windows of achievement.
Results:
Overall, 221 children aged 4–18 months were included in the study. The median age of motor development exhibited a 0.1–2.1-month delay compared to the WHO median age of motor milestone achievement. The prevalence of the gross motor milestone achievements for each of the six milestones ranged from 91.6% to 98.4%. Developmental delay was observed in 6.3% of the children. After adjusting for different variables, children with birth order of second or more were found to be significantly associated with the timely achievement of gross motor milestones.
Conclusion:
The apparently healthy children of the rural area of Haryana achieved gross motor milestones with some delay with respect to the WHO windows of achievement. Although the median value of this delay was low, awareness campaigns should be implemented to promote timely identification of children with development delays.
Keywords: Achievement, children, milestone
Introduction
Development includes the qualitative and quantitative changes that occur in a child. Skills such as social smiling, crawling, the first walking steps, grasping, and the first spoken word are known as developmental milestones.[1] Important developmental milestones that are commonly studied include gross motor, fine motor, language, and social skills.[1] Children who do not achieve developmental milestones at the expected ages are said to have delayed developmental milestones.
Globally, 200 million children do not reach their developmental potential in their first five years.[2] In India, developmental delays affect nearly 10% of children in early childhood.[2] The achievement of gross motor milestones is frequently delayed, and these children exhibit divergent outcomes.[3] A number of children with gross motor development delays achieve typical milestones at later ages. Some children have permanent motor disabilities, such as cerebral palsy or others conditions, which generally become more evident as the child reaches the age of 5 years and older.[4]
The early identification of delays in achieving milestones is critical for a child's development. Parents are usually the first to notice delays in their child's development.[5] Clinicians often encounter children with motor developmental delays in their clinical practices. The early identification of motor developmental delays aids timely referral for diagnosis, interventions, and treatment.[6] Developmental status is determined by complex interactions between internal constitutional factors and the external environmental factor. Various factors that are known to be associated with delays in achieving milestones including early gestational age,[7] twin status,[8] nutrient intake,[9] and low socioeconomic status.[10]
The World Health Organization (WHO) has developed normal age ranges for the achievements of motor milestones by healthy children. The WHO Multicentre Growth Reference Study (MGRS) generated new growth curves for assessing growth and the achievement windows of six gross motor development milestones by infants and young children around the world.[11] This study aimed to assess the delay in gross motor developmental achievements and associated factors among 4–18-month-old children in rural India.
Materials and Methods
A community-based cross-sectional study was conducted in the intensive field practice area of the Comprehensive Rural Health Services Project (CRHSP) of Ballabgarh, northern India. The CRHSP, Ballabgarh caters to 28 villages, one secondary-level hospital in Ballabgarh, two primary health centers and 12 subcenters in the Ballabgarh Block of the Faridabad District of Haryana in North India. This project was established as collaboration between the All Indian Institute of Medical Sciences, New Delhi, and the State Government of Haryana in 1961 to develop a model for Rural Healthcare Practice in India. The CRHSP, Ballabgarh caters to a population of nearly 90,000 as of December 31, 2011. In addition to community-based research, this project provides preventive, promotive, and curative services to its population.[12]
The required sample size was calculated to be 213 based on a prevalence of developmental delay of 14%,[13] with an alpha error of 0.05, an absolute precision of 5%, and a nonresponse rate of 10%. The data were collected from November 2011 to January 2012. All eligible children in the studied sample were included in the study. Very sick children and those who could not be examined were excluded from the study. Pretesting was performed with 30 children to examine the feasibility of the survey and the questionnaire, and appropriate modifications were made. House-to-house surveys were performed in the selected villages. Three visits were made to each eligible child in a village/cluster before any child was excluded from the study. The mother/caregivers were given an information sheet and explanations of the study, its objectives and procedure and the rights of the participants. If the mother/caregiver agreed to participate in the study after reviewing the information sheet, written consent was collected, and the mother/caregiver was interviewed. After obtaining preliminary information about the child, each child was subjected to anthropometric measurements. The child's weight was measured via tared weighing with minimum clothing over the child's body and without shoes using an OMRON Weight Scale HN 283. The scale was adjusted to 0.0. For the measurement of length, the child was laid on an infantometer with its head positioned firmly against the fixed hardboard and eyes looking forward. The knees were extended via the application of firm pressure, and the feet were flexed at right angles to the lower legs on the board. The length was measured between the two boards to the nearest 0.1 cm. Each anthropometric index was measured twice, and the average of the two readings was calculated. The highest milestone achieved was assessed by observing the child and verbally confirming with the mother/caregiver that the child could complete a particular activity. Six WHO gross motor milestones described in the WHO Motor Development Study were determined.[10]
For this analysis, the World Health Organization (WHO) Anthro Software (version 3.2.2, January 2011) was used to compute the children's weight-for-age, weight-for-length, and length-for-age Z scores as per the WHO standards. Further analyses of the data were completed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). The median age at the highest observed milestone was calculated and compared with the WHO reported medians for each of the six milestones. For the logistic regressions of each gross motor milestone, the number of children who were within the “windows of achievement” (i.e., the age groups) was considered. The prevalence of achieving each of the motor milestones was calculated. The potential explanatory variables that were studied included the nutritional status of the child, sex, infant and child feeding practices, immunization, and others factors. Step-wise selection was employed to obtain the variables that were significant at the level of P < 0.05 and were entered into the final multivariate logistic regression models of the six motor milestones. Ethical clearance was obtained from the Ethics Committee of the All India Institute of Medical Sciences, New Delhi, India. Appropriate management and referrals to more advanced health facilities were provided for all children who required referrals.
Results
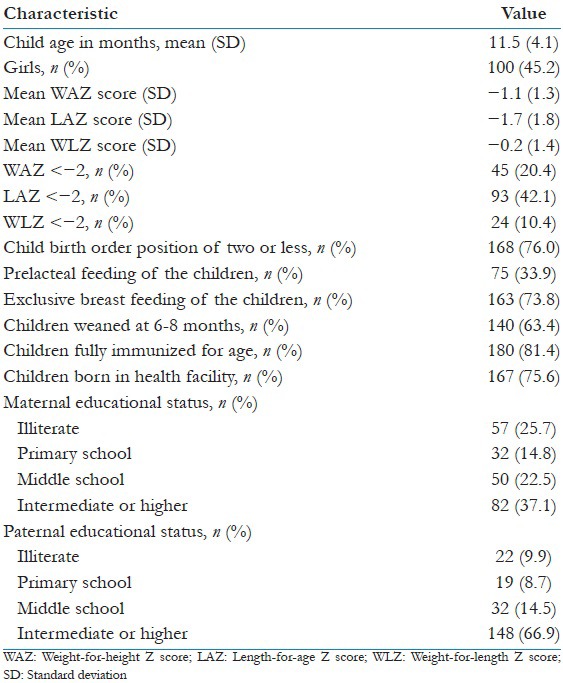
A total of 221 children ranging in age from 4 to 18 months were studied. The mother was the key informant for 86.4% of the studied children. The mean age of the children was 11.5 months (standard deviation: ±4.1). The proportion of girls and boys was nearly equal in the studied population. More than half of the mothers and fathers reported having a middle school education or higher. The details of the children, i.e., birth order position of 3 or lower, childbirth practices, infant feeding practices and immunization statuses, are presented in Table 1. The prevalence of underweight, stunting, and wasting was 20.4%, 42.1%, and 10.4%, respectively [Table 1].
Table 1.
Characteristics of the study subjects (children aged 4-18-months) and their parents (n=221)
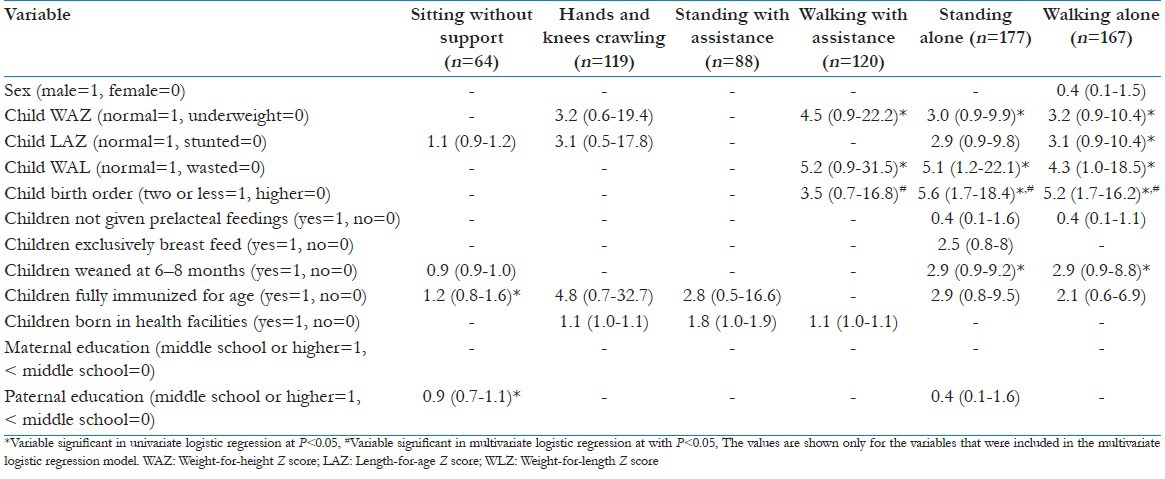
The median motor development age exhibited a 0.1–2.1-month delay compared with the median age reported by the WHO [Table 2]. The prevalences of the achievements of each of the gross motor milestones ranged from 91.6% to 98.4% Table 3. Developmental delays were found in 14 (6.3%) children. Univariate analyses revealed that complete immunization for age, normal nutritional status, greater paternal education level, timely weaning, and low birth order position were significantly associated with achievement of gross motor milestones. The birth order positions of one and two were found to be significantly associated with the timely achievement of gross motor milestones in the multivariate logistic regression [odds ratio (confidence interval), P value: Walking with assistance 2.1 (0.25–4.1), 0.02; standing alone 6.5 (0.5–3.2), <0.001; and walking alone 5.2 (0.4–2.9), 0.01; Table 4]. Gender, nutritional status, infant and child feeding practices, immunization status, institutional delivery and maternal and paternal education levels were not significantly associated with the achievements of any of the motor milestones in the multivariate analyses [data not shown].
Table 2.
Comparison of median ages (months) of motor milestone achievement between the World Health Organization, the published literature, and the present study
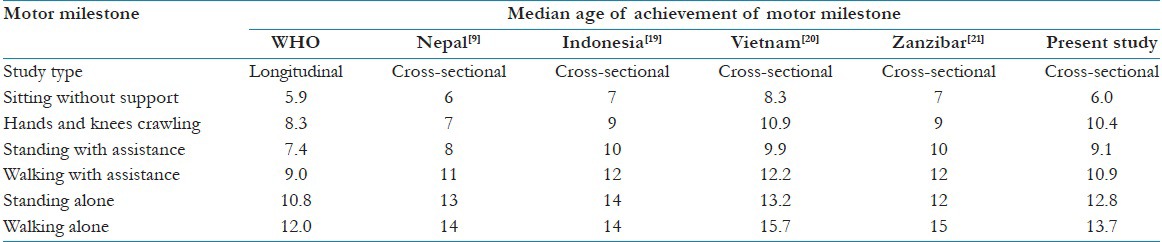
Table 3.
Proportions of children who achieved age-appropriate motor milestones per the World Health Organization windows of achievement in the present study (n=221)
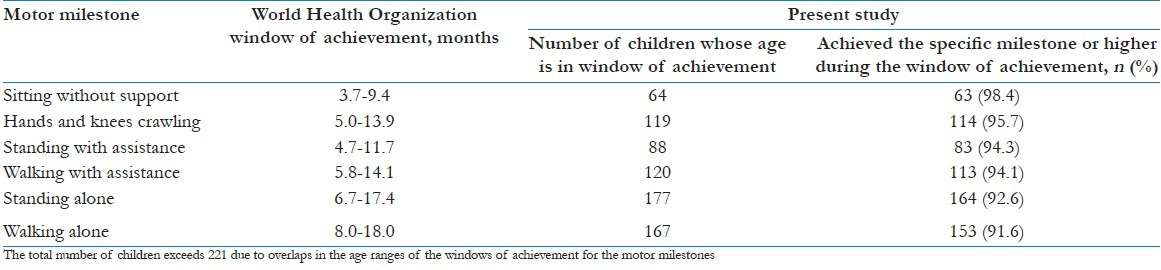
Table 4.
Odds ratios (95% confidence interval) from univariate logistic regressions of the factors associated with achieving motor milestones during the World Health Organization windows of achievement in the present study
Discussion
To the best of our knowledge, this study is the first of its type to assess delays in the achievement of six gross motor milestones using the WHO MGRS windows of achievement scale for these milestones[11] among children in a rural community in India. In addition, there is a lack of published literature about the rural community of India in the delayed achievement of six gross motor milestones based on the WHO MGRS windows of achievement scale. In this study, developmental delays in the achievement of gross motor milestones were present in 6.3% of children. Similarly, other population-based studies have reported that the prevalence of any developmental delay ranges from 3.5% to 10%.[14,15]
According to the WHO, approximately 5% of children below the age of 14 years exhibit a developmental delay or disability.[16] In India, the prevalence of developmental delay among those under the age of 2 years is approximately, 2%.[16,17] The higher prevalence of delayed developmental milestones observed in this study might be due to the small sample size or differences in the study instrument used.
The prevalence of delayed milestones was lower than that reported in another clinic-based study conducted in Bhopal, India, among children below the age of two years. The authors of this study found that the prevalence of any developmental delay was 9.5% using the Trivandrum Developmental Screening Chart.[7] In addition to motor milestones, this study tool also assesses the achievement of language and social milestones. Furthermore, this study was a community-based cross-sectional study. The prevalence of delayed milestones was nearly 50% in a study conducted using the Ages and Stages Questionnaire followed by the Developmental Assessment Scale for Indian Infants in a Tertiary Care Setting in North India.[18]
The median age of motor development exhibited a 0.1–2.1-month delay relative to the median age reported by the WHO. The primary reason for this delay might be that the present study was a cross-sectional study, whereas the MGRS was a longitudinal study. Similar delays have also been found in other cross-sectional studies from Nepal,[9] Indonesia,[19] Vietnam,[20] and Zanzibar.[21] Birth order was the only variable that was found to be significantly associated with the achievement of gross motor milestones in a study conducted in a Tertiary Care Setting in North India.[18] Other studies have documented the role of birth order in personality and language milestones.[22]
The major limitation of this study is that we were not able to assess all of the developmental milestones for logistic reasons. The history of development was assessed based on the report from the informant; therefore, some degree of recall bias cannot be ruled out. Moreover, the past histories of the children, for example, feeding history, breastfeeding, and weaning, could not be confirmed based on documentation.
Conclusion
Although low, the prevalence of delayed gross motor milestone achievements supports the need for a health facility-based awareness campaign to promote the timely identification of and interventions for children with delayed milestones. The apparently healthy children in the rural area of Haryana achieved the gross motor milestones with some delays as compared to the WHO windows of achievement. A further evaluation of the problem of the delay in achieving milestones needs to be performed and should utilize a mixed methods approach to facilitate understanding of issues related to both identification and management.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Developmental Milestones. Centre for Disease Control and Prevention. [Last cited on 2015 Aug 01]. Available from: http://www.cdc.gov/ncbddd/actearly/milestones/
- 2.Rashtriya Bal Swasthya Karyakram. Ministry of Health and Family Welfare, Government of India. 2013. [Last cited on 2015 Aug 01]. Available from: http://www.mdm.nic.in/Files/School%20Health%20Programme/Nutrition_Support/Rastriya_Bal_Swaasthya_Karyakram.pdf .
- 3.Ehrmann Feldman D, Couture M, Grilli L, Simard MN, Azoulay L, Gosselin J. When and by whom is concern first expressed for children with neuromotor problems? Arch Pediatr Adolesc Med. 2005;159:882–6. doi: 10.1001/archpedi.159.9.882. [DOI] [PubMed] [Google Scholar]
- 4.Harris SR. Parents’ and caregivers’ perceptions of their children's development. Dev Med Child Neurol. 1994;36:918–23. [PubMed] [Google Scholar]
- 5.Meenai Z, Longia S. A study on prevalence and antecedents of developmental delay among children less than 2 years attending well baby clinic. Peoples J Sci Res. 2009;2:9–12. [Google Scholar]
- 6.Noritz GH, Murphy NA Neuromotor Screening Expert Panel. Motor delays: Early identification and evaluation. Pediatrics. 2013;131:e2016–27. doi: 10.1542/peds.2013-1056. [DOI] [PubMed] [Google Scholar]
- 7.Black MM, Sazawal S, Black RE, Khosla S, Kumar J, Menon V. Cognitive and motor development among small-for-gestational-age infants: Impact of zinc supplementation, birth weight, and caregiving practices. Pediatrics. 2004;113:1297–305. doi: 10.1542/peds.113.5.1297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brouwer SI, van Beijsterveldt TC, Bartels M, Hudziak JJ, Boomsma DI. Influences on achieving motor milestones: A twin-singleton study. Twin Res Hum Genet. 2006;9:424–30. doi: 10.1375/183242706777591191. [DOI] [PubMed] [Google Scholar]
- 9.Siegel EH, Stoltzfus RJ, Kariger PK, Katz J, Khatry SK, LeClerq SC, et al. Growth indices, anemia, and diet independently predict motor milestone acquisition of infants in south central Nepal. J Nutr. 2005;135:2840–4. doi: 10.1093/jn/135.12.2840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kolobe TH. Childrearing practices and developmental expectations for Mexican-American mothers and the developmental status of their infants. Phys Ther. 2004;84:439–53. [PubMed] [Google Scholar]
- 11.WHO Multicentre Growth Reference Study Group. WHO motor development study: Windows of achievement for six gross motor development milestones. Acta Paediatr Suppl. 2006;450:86–95. doi: 10.1111/j.1651-2227.2006.tb02379.x. [DOI] [PubMed] [Google Scholar]
- 12.Gupta A, Kalaivani M, Gupta SK, Rai SK, Nongkynrih B. Burden of undernutrition, composite index of anthropometric failure (CIAF) and perception of caregivers about undernutrition among under five children in rural India. Indian J Nutr Diet. 2015;52:140–52. [Google Scholar]
- 13.Lakhan R, Mario A, Qureshi FN, Hall ML. Early intervention services to children with developmental delay in resource poor settings in India. Nepal J Med Sci. 2013;2:149–55. [Google Scholar]
- 14.Nair MK, Radhakrishnan SR. Early childhood development in deprived urban settlements. Indian Pediatr. 2004;41:227–37. [PubMed] [Google Scholar]
- 15.Louise H, Alison S, Jon D, Paul G. Evidence based case reviews: Investigation of children with “Developmental Delay”. West J Med. 2002;176:29–33. doi: 10.1136/ewjm.176.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Developmental Delay/Delayed Milestones. Institute of Child Development. Government of India. [Last cited on 2015 Aug 11]. Available from: http://www.icddelhi.org/developmental_delayed_milestone.html .
- 17.Nair MK, George B, Padmamohan J, Sunitha RM, Resmi VR, Prasanna GL, et al. Developmental delay and disability among under – 5 children in a rural ICDS block. Indian Pediatr. 2009;46(Suppl 1):s75–8. [PubMed] [Google Scholar]
- 18.Juneja M, Mohanty M, Jain R, Ramji S. Ages and stages questionnaire as a screening tool for developmental delay in Indian children. Indian Pediatr. 2012;49:457–61. doi: 10.1007/s13312-012-0074-9. [DOI] [PubMed] [Google Scholar]
- 19.Pollitt E, Husaini MA, Harahap H, Halati S, Nugraheni A, Sherlock AO. Stunting and delayed motor development in rural West Java. Am J Hum Biol. 1994;6:627–35. doi: 10.1002/ajhb.1310060511. [DOI] [PubMed] [Google Scholar]
- 20.Kulkarni S, Ramakrishnan U, Dearden KA, Marsh DR, Ha TT, Tran TD, et al. Greater length-for-age increases the odds of attaining motor milestones in Vietnamese children aged 5-18 months. Asia Pac J Clin Nutr. 2012;21:241–6. [PubMed] [Google Scholar]
- 21.Kariger PK, Stoltzfus RJ, Olney D, Sazawal S, Black R, Tielsch JM, et al. Iron deficiency and physical growth predict attainment of walking but not crawling in poorly nourished Zanzibari infants. J Nutr. 2005;135:814–9. doi: 10.1093/jn/135.4.814. [DOI] [PubMed] [Google Scholar]
- 22.Eckstein D, Kaufman JA. The role of birth order in personality: An enduring intellectual legacy of Alfred Adler. J Individ Psychol. 2012;68:60–74. [Google Scholar]