

Abstract
The prevalence of masked hypertension (out‐of‐clinic daytime systolic/diastolic blood pressure (SBP/DBP) ≥135/85 mm Hg on ambulatory blood pressure monitoring [ABPM] among adults with clinic SBP/DBP <140/90 mm Hg) is high. It is unclear who should be screened for masked hypertension. The authors derived a clinic blood pressure (CBP) index to identify populations for masked hypertension screening. Index cut points corresponding to 75% to 99% sensitivity and prehypertension were evaluated as ABPM testing criterion. In a derivation cohort (n=695), the index was clinic SBP+1.3*clinic DBP. In an external validation cohort (n=675), the sensitivity for masked hypertension using an index ≥190 mm Hg and ≥217 mm Hg and prehypertension status was 98.5%, 71.5%, and 82.5%, respectively. Using National Health and Nutrition Examination Survey data (n=11,778), the authors estimated that these thresholds would refer 118.6, 44.4, and 59.3 million US adults, respectively, to ABPM screening for masked hypertension. In conclusion, the CBP index provides a useful approach to identify candidates for masked hypertension screening using ABPM.
In 2002, Pickering introduced the term masked hypertension, referring to individuals not taking antihypertensive medication who have nonelevated clinic‐measured blood pressure (BP) but elevated daytime BP when assessed outside of the clinic by ambulatory BP monitoring (ABPM).1 Masked daytime hypertension has been reported to be common among individuals with nonelevated clinic BP (CBP), with prevalence estimates ranging from 15% to 30% in population‐based studies.2 Compared with sustained normotension, defined as nonelevated CBP with nonelevated daytime BP on ABPM, masked daytime hypertension is associated with increased risk for target organ damage, cardiovascular disease, and mortality.3, 4
Some guidelines and position papers recommend ABPM to detect masked hypertension5, 6, 7; however, it is unclear which populations to screen with ABPM to detect masked hypertension.1, 5, 6, 7, 8, 9, 10, 11, 12, 13 One approach would be to offer ABPM to all adults with nonelevated CBP to identify those with masked hypertension.2 However, population‐wide screening for masked hypertension is not practical. Another approach is to offer ABPM to individuals with prehypertension, defined as a clinic systolic BP (SBP) of 120 mm Hg to 139 mm Hg or clinic diastolic BP (DBP) of 80 mm Hg to 89 mm Hg, due to the substantial overlap that exists between prehypertension and masked hypertension.22, 23 This too may result in a substantial proportion of US adults undergoing ABPM. A third approach is to develop an equation to identify individuals for ABPM screening.
In this study, we derived and validated a CBP diagnostic index for detecting masked hypertension among adults with nonelevated CBP who were not taking antihypertensive medication. Test characteristics for the identification of masked hypertension using this index, including sensitivity, specificity, and positive and negative predictive values, were calculated and compared with the test characteristics associated with using prehypertension. Data from the National Health and Nutrition Examination Survey (NHANES) 2009–2012 were used to estimate the number of US adults who would be recommended for ABPM to detect masked hypertension using each of these approaches.
Methods
Study Populations
The current analyses used data from four studies. The Masked Hypertension Study (MHT)22 (n=1010) was used to derive an equation (the CBP diagnostic index) for identifying masked daytime hypertension. We pooled data from the Improving the Detection of Hypertension Study (IDH) (n=408) and the Jackson Heart Study (JHS; n=5301; n=1148 who completed ABPM) to externally validate the CBP diagnostic index in samples having a high number of Hispanics and African Americans. NHANES 2009–2010 and 2011–2012 (n=11,778) were used to estimate the number of US adults 20 years and older who would be recommended for ABPM screening to identify masked hypertension with the approaches being compared.
Each of the studies used for the current analysis has been described in detail previously.22, 24, 25, 26 In brief, the MHT is a worksite‐based study comprising adult employees from Stony Brook University, University Hospital at Stony Brook, Columbia University, and a private hedge fund management organization in New York who work >20 hours per week and on at least two consecutive days. The goal of the MHT is to estimate the prevalence, predictors, and prognosis of masked hypertension.22 The IDH Study enrolled a community‐based sample of adults, primarily from upper Manhattan, New York City.24 It was designed to compare the cost‐effectiveness of different strategies for diagnosing ambulatory hypertension. The JHS is a prospective population‐based study comprised exclusively of African Americans from the tri‐county (Hinds, Madison, and Rankin counties) area of Jackson, Mississippi.25 The purpose of the JHS is to evaluate cardiovascular disease risk among African Americans.27 The aim of NHANES is to assess the health and nutritional status of adults and children in the United States. NHANES enrolled a multistage probability sample of noninstitutionalized US civilians and can be used to calculate nationally representative estimates of disease prevalence. It is conducted in 2‐year cycles, and these cycles can be pooled to provide stable prevalence estimates in population subgroups.
For the current analyses, the MHT, IDH, and JHS were restricted to participants who met criteria for a complete ABPM (defined below) and who had nonelevated CBP and were not taking antihypertensive medication (MHT: n=695; IDH: n=344; JHS: n=331). The NHANES sample was restricted to participants 20 years and older who had nonelevated CBP and were not taking antihypertensive medication (n=6835). ABPM was not performed in NHANES. Additional details on each study are available in the online Supplement. The current study was approved by all appropriate institutional review boards and is in agreement with the Declaration of Helsinki. All participants provided written informed consent.
Data Collection
The MHT and IDH studies collected data using self‐administered questionnaires during a clinic examination and through ABPM. The JHS collected data using interviewer‐administered questionnaires during a clinic examination and through ABPM. In each study, trained technicians measured height, weight, and CBP during a clinic examination. Questionnaires were used to document information on demographics (ie, age, sex, race/ethnicity), smoking status, current use of antihypertensive medication, and self‐reported diabetes status. In NHANES, interviewer‐administered questionnaires were used during the in‐home interview to collect demographic information and data on antihypertensive medication use.
CBP in the MHT, IDH, JHS, and NHANES
In all four studies, CBP was measured by trained staff following a standardized protocol. Prior to CBP measurements, participants sat quietly for at least 5 minutes in an upright position with their back and arms supported, feet flat on the floor, and legs uncrossed. During the CBP measurements, an appropriately sized cuff, determined by measuring the mid‐arm circumference, was used.28, 29 One to two minutes elapsed between the readings in the MHT, IDH, and JHS studies; there was a 30‐second interval between the readings in NHANES. In the MHT, IDH, and NHANES, three CBP measurements were obtained using a mercury sphygmomanometer. In JHS, two CBP measurements were obtained using a random zero mercury sphygmomanometer. For each participant, the CBP measurements were averaged. Nonelevated CBP was defined as clinic SBP <140 mm Hg and clinic DBP <90 mm Hg. Prehypertension was defined as clinic SBP of 120 mm Hg to 139 mm Hg or clinic DBP of 80 to 89 mm Hg.
ABPM in MHT, IDH, and JHS
ABPM was conducted in MHT, IDH, and JHS using Spacelabs model 90207 (Snoqualmie, WA). For each study, participants were fitted with an appropriately sized ABPM arm cuff. BP on ABPM was recorded every 28 minutes in MHT, every 30 minutes in IDH, and every 20 minutes in JHS. For the current analysis, we defined diurnal periods using International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes (IDACO) criteria. Daytime was defined as the time period from 10 am to 8 pm and nighttime as 12 am to 6 am.30 Participants were considered to have a complete ABPM if they had 10 or more daytime and five or more nighttime SBP and DBP measurements.
The ABPM recordings were analyzed to obtain mean daytime and nighttime SBP and DBP. Daytime hypertension was defined as a mean SBP ≥135 mm Hg or mean DBP ≥85 mm Hg based on the daytime measurements, and nocturnal hypertension was defined as a mean SBP ≥120 mm Hg or mean DBP ≥70 mm Hg based on the nighttime measurements.5, 31, 32 Since the current analysis was restricted to participants with nonelevated CBP, those with daytime and nocturnal hypertension had masked daytime hypertension and masked nocturnal hypertension, respectively.
Statistical Analyses
In the MHT, the c‐statistic was calculated for three logistic regression models to identify factors that discriminated participants with and without masked daytime hypertension, defined as a mean daytime SBP ≥135 mm Hg or mean daytime DBP ≥85 mm Hg in participants with nonelevated CBP (SBP/DBP <140/90 mm Hg; Table S1).33 In these analyses, masked daytime hypertension was the dependent variable. The independent variables were clinic SBP and DBP in model 1; age, sex, body mass index, race, ethnicity, diabetes, and current smoking in model 2; and all variables from models 1 and 2 in model 3. As described below, model 1 discriminated masked daytime hypertension better than model 2. Discrimination was better in model 3 versus model 1. Model 1 was chosen for the diagnostic index as it provides a simple method using CBP alone and may be more easily implemented in practice.
A receiver operating characteristic curve was plotted to determine the CBP diagnostic index cut point with 99%, 95%, 90%, 85%, 80%, and 75% sensitivity (Figure S1). The CBP diagnostic index cut point for masked daytime hypertension corresponding to the respective sensitivity level was subsequently applied in the diagnostic index equation from the selected logistic regression model (model 1) to derive the cut points. The online Data S1 provides further details on the derivation of the CBP diagnostic index.
In the pooled IDH/JHS validation cohort, the c‐statistic and the Hosmer‐Lemeshow Goodness‐of‐Fit for deciles were calculated to determine the discrimination and calibration, respectively, of the diagnostic index. The external validity of the CBP diagnostic index was determined by taking the cut points associated with 99%, 95%, 90%, 85%, 80%, and 75% sensitivity from the MHT and calculating the test characteristics for detecting masked daytime hypertension in the pooled IDH/JHS validation cohort. As the 2013 European Society of Hypertension (ESH) position paper on ABPM recommends including nocturnal hypertension as a criterion for the definition of masked hypertension, we evaluated the test characteristics of the CBP diagnostic index for identifying masked daytime or masked nocturnal hypertension in a secondary analysis.5 For comparison, test characteristics were calculated for prehypertension and the upper range of prehypertension (ie, clinic SBP 130–139 mm Hg or clinic DBP 85–89 mm Hg). The upper range of prehypertension was selected for an a priori analysis as studies have reported that the prevalence of masked hypertension is very high in this range of CBP.4, 22, 34
Finally, using NHANES 2009–2012 data, the number and percentage of US adults 20 years and older who would be recommended testing with ABPM was estimated for individuals with an elevated CBP diagnostic index, prehypertension, and the upper range of prehypertension, separately. Estimates were calculated for the overall population and in subgroups defined by age (ie, <40, 40–59, ≥60 years), race/ethnicity (ie, non‐Hispanic white, non‐Hispanic black, Hispanic, other), and sex. NHANES analyses were conducted taking into account the study's complex multistage sampling design and were weighted to produce US population estimates. Analyses were conducted using SAS version 9.4 (SAS Institute, Cary, North CC) and SUDAAN 10.1 (Research Triangle Institute, Research Triangle Park, NC).
Results
Participant Characteristics
Compared with the derivation cohort (ie, MHT), the pooled validation cohort (ie, IDH/JHS) had a higher percentage of participants who were 60 years or older and black and Hispanic (Table 1). Participants with prehypertension and the upper range of prehypertension comprised 39.9% and 12.8% of the derivation cohort, respectively, and 47.4% and 19.3% of the pooled validation cohort, respectively. Whereas masked daytime and masked nocturnal hypertension was present in 19.3% and 20.0% of the derivation cohort, respectively, the prevalence was 20.3% and 32.9%, respectively, in the pooled IDH/JHS cohort. In addition, 30.2% and 37.6% of the MHT and pooled IDH/JHS cohort participants, respectively, had masked daytime and/or nocturnal hypertension.
Table 1.
Characteristics of Participants in the MHT, IDH, and JHS
| MHT Study (Derivation Cohort) | IDH/JHS (Pooled Validation Cohort) | |
|---|---|---|
| (n=695) | (n=675) | |
| Age categories, No. (%), y | ||
| <40 | 213 (30.7) | 212 (31.4) |
| 40–59 | 435 (62.6) | 324 (48.0) |
| ≥60 | 47 (6.8) | 139 (20.6) |
| Male, No. (%) | 275 (39.6) | 241 (35.9) |
| Black race, No. (%) | 47 (6.8) | 5415 (61.5) |
| Hispanic ethnicity, No. (%) | 87 (12.5) | 216 (32.0) |
| Body mass index, No. (%), kg/m2 | 27.4 (5.4) | 28.5 (6.0) |
| Diabetes, No. (%) | 25 (3.8) | 37 (5.5) |
| Current smoker, No. (%) | 49 (7.4) | 62 (9.3) |
| Clinic BP | ||
| Systolic, mm Hg | 113.8 (10.7) | 115.0 (11.8) |
| Diastolic, mm Hg | 74.4 (7.5) | 74.3 (8.0) |
| Prehypertension, No. (%)a | 277 (39.9) | 320 (47.4) |
| Upper range of prehypertension, No. (%)b | 89 (12.8) | 130 (19.3) |
| Ambulatory BP | ||
| Daytime period | ||
| Systolic, mm Hg | 122.6 (10.1) | 118.6 (12.1) |
| Diastolic, mm Hg | 77.2 (7.5) | 71.8 (9.4) |
| Masked daytime hypertension, No. (%)c | 134 (19.3) | 137 (20.3) |
| Nighttime period | ||
| Systolic, mm Hg | 106.2 (10.7) | 108.6 (11.1) |
| Diastolic, mm Hg | 62.3 (7.9) | 63.5 (7.7) |
| Masked nocturnal hypertension, No. (%)d | 139 (20.0) | 222 (32.9) |
| Masked daytimec and/or nocturnald hypertension, No. (%) | 210 (30.2) | 254 (37.6) |
Abbreviations: BP, blood pressure; IDH, Improving the Detection of Hypertension Study; JHS, Jackson Heart Study; MHT, Masked Hypertension Study. Values are expressed as mean (standard deviation) unless otherwise indicated.
aPrehypertension: among adults with nonelevated clinic blood pressure (BP) (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥120 mm Hg and <140 mm Hg, or clinic diastolic BP ≥80 mm Hg and <90 mm Hg. bUpper range of prehypertension: among adults with nonelevated clinic BP (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥130 mm Hg and <140 mm Hg, or clinic diastolic BP ≥85 mm Hg and <90 mm Hg. cMasked daytime hypertension: clinic systolic/diastolic BP <140/90 mm Hg with mean ambulatory daytime systolic/diastolic BP ≥135/85 mm Hg. dMasked nocturnal hypertension: clinic systolic BP <140/90 mm Hg with mean ambulatory nocturnal systolic/diastolic BP ≥120/70 mm Hg.
Derivation of the CBP Diagnostic Index in MHT
The c‐statistic for masked daytime hypertension was 0.78 (95% confidence interval [CI], 0.74–0.82) for the model including only clinic SBP and DBP (model 1) and 0.72 (95% CI, 0.66–0.77) for the model that included age, sex, body mass index, race, ethnicity, diabetes, and current smoking status (model 2; Table S1). In the model that included all of the variables from models 1 and 2 (model 3), the c‐statistic was 0.81 (95% CI, 0.77–0.85). Using model 1, the CBP diagnostic index was defined as: clinic SBP + 1.3*clinic DBP.
A scatterplot of each participant's clinic SBP and DBP in the MHT is shown in Figure S2. The lines in the figure correspond to the CBP diagnostic index equation for sensitivity levels of 99%, 95%, 90%, 85%, 80%, and 75%. Using the CBP diagnostic index equation, the cut point for detecting masked daytime hypertension with 99% sensitivity was 190 mm Hg. The cut point for 95% sensitivity was 201 mm Hg, 90% sensitivity was 207 mm Hg, 85% sensitivity was 212 mm Hg, 80% sensitivity was 214 mm Hg, and 75% sensitivity was 217 mm Hg. The specificity and positive and negative predictive values for each level of sensitivity are provided in Table S2.
Validation of the CBP Diagnostic Index in the Pooled IDH/JHS Cohorts
In the validation cohort, the c‐statistic for masked daytime hypertension was 0.77 (95% CI, 0.73–0.81). The CBP diagnostic index was well calibrated in the validation cohort (Hosmer‐Lemeshow Goodness‐of‐Fit chi‐square for deciles with 8 degrees of freedom: 9.78; P=.281). A scatterplot of IDH and JHS participants’ clinic SBP and DBP readings and the boundary lines representing 99%, 95%, 90%, 85%, 80%, and 75% sensitivity for detecting masked daytime hypertension using the CBP diagnostic index are plotted in Figure. In the pooled IDH/JHS cohort, the sensitivity for detecting masked daytime hypertension using the cut points on the CBP diagnostic index from the MHT ranged from 98.5% to 71.5% and the specificity ranged from 18.8% to 64.1%, respectively (CBP diagnostic index ≥190 mm Hg to ≥217 mm Hg, respectively; Table 2, top panel). The sensitivity and specificity for detecting masked daytime hypertension was 82.5% and 61.5% for prehypertension and 42.3% and 86.6% for the upper range of prehypertension, respectively. The sensitivity for detecting masked daytime or nocturnal hypertension ranged from 97.2% to 64.6% (CBP diagnostic index ≥190 mm Hg to ≥217 mm Hg, respectively) using the CBP diagnostic index and was 71.3% for prehypertension and 34.3% for the upper range of prehypertension (Table 2, bottom panel).
Figure 1.
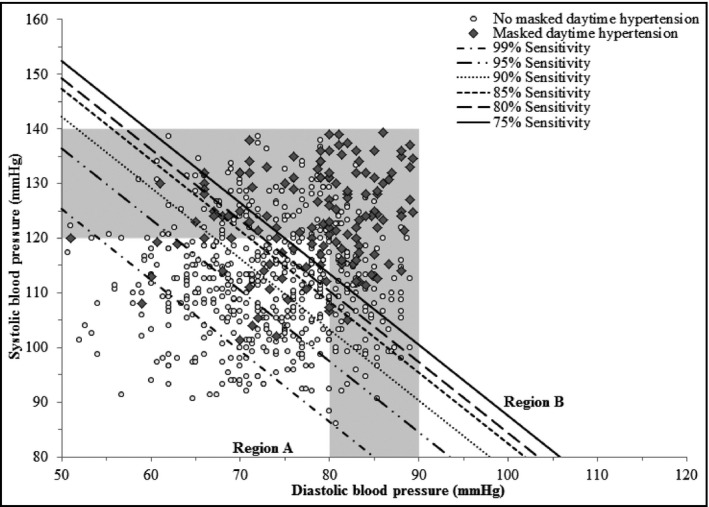
Scatterplot of clinic systolic vs diastolic blood pressure demonstrating derived cut points corresponding with specified sensitivity levels for detecting masked daytime hypertension using the clinic blood pressure index equation in the pooled validation cohort of participants in the Improving the Detection of Hypertension Study and Jackson Heart Study (n=675). The shaded region represents the clinic blood pressure values corresponding with prehypertension defined as systolic blood pressure ≥120 mm Hg and <140 mm Hg and/or diastolic blood pressure ≥80 mm Hg and <90 mm Hg. Region A: The clinic blood pressure diagnostic index, defined as systolic clinic blood pressure + 1.3*diastolic clinic blood pressure, was categorized as normal (ie, below the cut point corresponding with the specified sensitivity level). Region B: The clinic blood pressure diagnostic index, defined as systolic clinic blood pressure + 1.3*diastolic clinic blood pressure, was categorized as elevated (ie, at or above the cut point corresponding with the specified sensitivity level). Cut points for an elevated clinic blood pressure diagnostic index corresponding with the specified sensitivity levels are: sensitivity 99%: ≥190 mm Hg; sensitivity 95%: ≥201 mm Hg; sensitivity 90%: ≥207 mm Hg; sensitivity 85%: ≥212 mm Hg; sensitivity 80%: ≥214 mm Hg; and sensitivity 75%: ≥217 mm Hg.
Table 2.
Test Characteristics for Detecting Masked Daytime Hypertension (n=137; top panel) and Masked Daytime and/or Nocturnal Hypertension (n=254; bottom panel) Associated With Prehypertension, Upper Range of Prehypertension, and an Elevated Clinic BP Diagnostic Index in the Pooled Validation Cohort of Participants in the Improving the Detection of Hypertension Study and Jackson Heart Study (n=675)
| Prehypertensiona | Upper Range of Prehypertensionb | Elevated Clinic BP Diagnostic Index Using Different Derived Cut Pointsc | ||||||
|---|---|---|---|---|---|---|---|---|
| ≥190 mm Hg | ≥201 mm Hg | ≥207 mm Hg | ≥212 mm Hg | ≥214 mm Hg | ≥217 mm Hg | |||
| n=320 | n=130 | n=572 | n=472 | n=415 | n=351 | n=330 | n=291 | |
| Masked daytime hypertension | ||||||||
| Sensitivity, % (No.) | 82.5 (113/137) | 42.3 (58/137) | 98.5 (135/137) | 93.4 (128/137) | 89.8 (123/137) | 81.0 (111/137) | 78.8 (108/137) | 71.5 (98/137) |
| Specificity, % (No.) | 61.5 (331/538) | 86.6 (466/538) | 18.8 (101/538) | 36.1 (194/538) | 45.7 (246/538) | 55.4 (298/538) | 58.7 (316/538) | 64.1 (345/538) |
| PPV, % (No.) | 35.3 (113/320) | 44.6 (58/130) | 23.6 (135/572) | 27.1 (128/472) | 29.6 (123/415) | 31.6 (111/351) | 32.7 (108/330) | 33.7 (98/291) |
| NPV, % (No.) | 93.2 (331/355) | 85.5 (466/545) | 98.1 (101/103) | 95.6 (194/203) | 94.6 (246/260) | 92.0 (298/324) | 91.6 (316/345) | 89.8 (345/384) |
| Masked daytime and/or nocturnal hypertensiond | ||||||||
| Sensitivity, % (No.) | 71.3 (181/254) | 34.3 (87/254) | 97.2 (247/254) | 90.6 (230/254) | 83.9 (213/254) | 73.2 (186/254) | 71.3 (181/254) | 64.6 (164/254) |
| Specificity, % (No.) | 67.0 (282/421) | 89.8 (378/421) | 22.8 (96/421) | 42.5 (179/421) | 52.0 (219/421) | 60.8 (256/421) | 64.6 (272/421) | 69.8 (294/421) |
| PPV, % (No.) | 56.6 (181/320) | 66.9 (87/130) | 43.2 (247/572) | 48.7 (230/472) | 51.3 (213/415) | 53.0 (186/351) | 54.8 (181/330) | 56.4 (164/291) |
| NPV, % (No.) | 79.4 (282/355) | 69.4 (378/545) | 93.2 (96/103) | 88.2 (179/203) | 84.2 (219/260) | 79.0 (256/324) | 78.8 (272/345) | 76.6 (294/384) |
Abbreviations: BP, blood pressure; NPV: negative predictive value; PPV, positive predictive value.
aPrehypertension: among adults with nonelevated clinic blood pressure (BP) (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥120 mm Hg and <140 mm Hg, or clinic diastolic BP ≥80 mm Hg and <90 mm Hg. bUpper range of prehypertension: among adults with nonelevated clinic BP (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥130 mm Hg and <140 mm Hg, or clinic diastolic BP ≥85 mm Hg and <90 mm Hg. cClinic BP diagnostic index cut points associated with 99% (190 mm Hg), 95% (201 mm Hg), 90% (207 mm Hg), 85% (212 mm Hg), 80% (214 mm Hg), and 75% (217 mm Hg) sensitivity. dMasked daytime and/or nocturnal hypertension: clinic systolic/diastolic BP <140/90 mm Hg and daytime hypertension (ie, mean daytime systolic BP ≥135 mm Hg or mean diastolic BP ≥85 mm Hg) and/or nocturnal hypertension (ie, mean nighttime systolic BP ≥120 mm Hg or mean diastolic BP ≥70 mm Hg).
Testing for Masked Daytime Hypertension in the US Population
In 2009–2012, an estimated 152.7 million US adults had nonelevated CBP and were not taking antihypertensive medication (Table 3). Using the CBP diagnostic index, the number of US adults recommended ABPM to detect masked daytime hypertension ranged from 44.4 million using a cut point of 217 mm Hg to 118.6 million using a cut point of 190 mm Hg. Using prehypertension as the criterion for ABPM would result in referring 59.3 million US adults for ABPM. There would be 20.3 million US adults referred for ABPM if the upper range of prehypertension is used.
Table 3.
US Adults With Nonelevated Clinic BP a Not Taking Antihypertensive Medication Who Would be Referred for ABPM Using Prehypertension, the Upper Range of Prehypertension, and Cut Points Derived Using the Clinic BP Diagnostic Index
| Prehypertensionb | Upper Range of Prehypertensionc | Elevated Clinic BP Diagnostic Index Using Different Derived Cut Pointsd | ||||||
|---|---|---|---|---|---|---|---|---|
| ≥190 mm Hg | ≥201 mm Hg | ≥207 mm Hg | ≥212 mm Hg | ≥214 mm Hg | ≥217 mm Hg | |||
| Number in millions (percentage) of US adultse | ||||||||
| Overall | 59.3 (39.1) | 20.3 (14.0) | 118.6 (76.5) | 90.4 (58.1) | 73.1 (46.8) | 58.3 (37.4) | 53.0 (34.0) | 44.4 (28.5) |
| Age categories, y | ||||||||
| <40 y | 22.3 (29.0) | 6.4 (8.4) | 53.7 (69.8) | 38.0 (49.5) | 29.0 (37.8) | 22.0 (28.4) | 19.2 (25.2) | 15.9 (20.6) |
| 40–59 | 26.5 (45.3) | 8.7 (15.3) | 49.2 (83.9) | 39.7 (67.4) | 33.7 (56.7) | 27.9 (47.4) | 26.2 (43.9) | 22.2 (37.5) |
| ≥60 | 10.5 (57.4) | 5.3 (28.8) | 15.7 (81.1) | 12.7 (65.0) | 10.4 (53.3) | 8.4 (43.8) | 7.7 (40.0) | 6.3 (33.4) |
| Race/ethnicity | ||||||||
| Non‐Hispanic white | 40.1 (39.2) | 13.7 (14.0) | 79.8 (77.5) | 61.5 (59.4) | 49.9 (47.5) | 39.6 (37.3) | 36.1 (34.2) | 30.3 (28.5) |
| Non‐Hispanic black | 6.6 (46.1) | 2.6 (18.3) | 11.6 (78.5) | 9.1 (61.4) | 7.4 (50.9) | 6.1 (41.6) | 5.5 (38.1) | 4.7 (32.5) |
| Hispanic | 9.1 (35.0) | 3.2 (12.9) | 20.6 (76.4) | 15.6 (59.7) | 12.4 (48.9) | 10.1 (41.0) | 9.1 (37.3) | 7.8 (32.4) |
| Other race | 4.5 (34.7) | 1.3 (10.6) | 9.2 (75.6) | 6.7 (55.8) | 5.5 (45.7) | 4.6 (37.4) | 4.3 (34.7) | 3.5 (28.9) |
| Sex | ||||||||
| Female | 24.0 (29.9) | 8.4 (10.6) | 55.2 (67.6) | 39.4 (48.1) | 30.7 (37.2) | 23.4 (28.5) | 21.3 (25.6) | 17.7 (21.5) |
| Male | 35.3 (48.6) | 11.9 (17.5) | 63.4 (85.7) | 50.9 (68.5) | 42.3 (56.7) | 34.8 (46.7) | 31.7 (42.8) | 26.7 (35.7) |
Abbreviation: ABPM, ambulatory blood pressure monitoring; BP, blood pressure.
aNonelevated clinic blood pressure (BP): clinic systolic BP <140 mm Hg and clinic diastolic BP <90 mm Hg. bPrehypertension: among adults with nonelevated BP (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥120 mm Hg and <140 mm Hg, or clinic diastolic BP ≥80 mm Hg and <90 mm Hg. cUpper range of prehypertension: among adults with nonelevated clinic BP (ie, systolic BP <140 mm Hg and diastolic BP <90 mm Hg), clinic systolic BP ≥130 mm Hg and <140 mm Hg, or clinic diastolic BP ≥85 mm Hg and <90 mm Hg. dClinic BP diagnostic index cut points associated with 99% (190 mm Hg), 95% (201 mm Hg), 90% (207 mm Hg), 85% (212 mm Hg), 80% (214 mm Hg), and 75% (217 mm Hg) sensitivity. eNumber and percentage of US adults were derived from the National Health and Nutrition Examination Survey 2009–2012. There were approximately 152.7 million US adults with nonelevated clinic BP who were not taking antihypertensive medication.
Discussion
In the current study, we developed and validated a CBP diagnostic index that identifies adults as having masked daytime hypertension. We externally validated cut points for identifying masked daytime hypertension using the CBP diagnostic index with sensitivity ranging from 75% to 99%. Although the CBP diagnostic index can be used to identify almost all adults with masked hypertension (ie, approximately 99% sensitivity), this would require that 118.6 of the 152.7 million US adults with nonelevated CBP undergo ABPM. By choosing a cut point associated with lower sensitivity, specificity would be higher and ABPM would be required for far fewer US adults. For example, using a cut point that identified 89.8% of individuals with masked daytime hypertension would require testing 73.1 million US adults. For comparison, using prehypertension as a criterion to screen for masked daytime hypertension provides 82.5% sensitivity and would require 59.3 million US adults to undergo ABPM. While the upper range of prehypertension would only require screening 20.3 million US adults, less than 50% of masked daytime hypertension cases (42.3% sensitivity) would be referred to ABPM.
Guidelines and position papers recommend ABPM to detect masked hypertension but agreement has not been reached on who should be offered ABPM.1, 2, 5, 6, 7, 8, 9, 10, 11, 12 The current study provides evidence that it is impractical to perform ABPM in all US adults (approximately 153 million) with nonelevated CBP who are not taking antihypertensive medication. A more reasonable approach would be to test adults with a CBP diagnostic index above a specified cut point. For any selected cut point, there is a balance between sensitivity to detect masked daytime hypertension and the number of US adults who require testing with ABPM. Using a low cut point provides high sensitivity and almost all adults with masked daytime hypertension would be detected. However, this would result in performing ABPM in a majority of US adults with nonelevated CBP. In contrast, using a higher cut point on the CBP diagnostic index, the sensitivity will be lower but substantially fewer US adults would need to undergo ABPM.
There are proponents of offering ABPM to adults with prehypertension in order to detect masked hypertension.22, 34 Supporting this approach are prior studies that have examined the overlap of prehypertension with masked daytime hypertension.22 In the MHT, 35.0% of participants with prehypertension but only 8.9% of those with normal CBP had masked daytime hypertension.22 Similarly, masked daytime hypertension was more common among IDH/JHS participants with prehypertension (35.3%) compared with normal CBP (6.8%).35 In the MHT, masked daytime hypertension was almost twice as common in adults with CBP in the upper vs lower range of prehypertension (ie, clinic SBP/DBP 130–139/85–89 mm Hg vs 120–129/80–84 mm Hg): 51.7% vs 26.5%.22 These studies may be interpreted as recommending ABPM for adults with CBP in the upper range of prehypertension and may be an appropriate approach for detecting masked hypertension. Although these prior studies demonstrate high positive predictive value of prehypertension to identify masked daytime hypertension, the current study shows that the upper range of prehypertension has low sensitivity for detecting masked daytime hypertension. Therefore, referring only individuals with CBP in the upper range of prehypertension for ABPM would miss the majority of individuals with masked daytime hypertension.
Increasing evidence suggests that CVD risk is higher for individuals with compared to without elevated nighttime BP.36 The 2013 ESH ABPM position paper incorporates elevated nighttime BP as a criterion for masked hypertension. The current study suggests that the cut points from the CBP diagnostic index chosen for detecting masked daytime hypertension may also be useful for detecting masked daytime or nocturnal hypertension.
ABPM and home BP monitoring (HBPM) can also be used to identify masked hypertension. Some evidence suggests that some individuals have masked hypertension on ABPM or HBPM, but not by both approaches. It is unclear whether the current results apply to masked hypertension identified by HBPM.
Study Strengths and Limitations
The current study has several strengths. First, there were four cohorts available for analysis. This allowed us to derive the CBP diagnostic index, externally validate it, and estimate the number of US adults who would be recommended for ABPM across a range of cut points on the index. The large number of participants from each cohort with nonelevated CBP provided large samples to derive and externally validate the CBP diagnostic index. Furthermore, these cohorts allowed us to compare test characteristics for cut points on the CBP diagnostic index with prehypertension and the upper range of prehypertension. In addition, the pooled validation cohort had a high representation of minorities including Hispanics in IDH and African Americans in JHS.
Several limitations should be considered when interpreting the current results. Although the CBP diagnostic index was validated in a pooled cohort of IDH and JHS participants, it may not be generalizable to other populations. Masked hypertension was diagnosed using one 24‐hour ABPM period. While some individuals with masked daytime and/or nocturnal hypertension on a single ABPM may not have it when repeated, conducting only one 24‐hour ABPM period is common clinical practice.24 The cut points may be different if an oscillometric device were used to measure CBP. In addition, while all four studies used trained staff who followed standardized protocols to measure CBP, the effect of different intervals on successive CBP measurements (eg, 30 seconds in the NHANES vs 1 to 2 minutes in other studies) is unclear. Further, CBP was measured following a research protocol in each of the individual studies. However, CBP measured in clinical practice is generally of poorer quality. Last, a possible limitation of the use of ABPM in clinical practice is that self‐reported sleep disturbances are relatively common among those who undergo ABPM.
Conclusions
There are approximately 153 million adults with nonelevated CBP who are not taking antihypertensive medication in the United States. Performing ABPM in all of these people in order to detect masked hypertension is not practical. Using the CBP diagnostic index, developed and validated in the current study, provides a simple approach to identify a subgroup of individuals for whom ABPM is better targeted. If identifying all individuals with masked hypertension is viewed as necessary, a cut point of 190 mm Hg on the CBP diagnostic index could be used. NHANES data indicate that 118.6 million US adults would be referred for ABPM under this approach. In contrast, fewer US adults would be referred to ABPM using higher cut points on the CBP diagnostic index, but at the expense of lower sensitivity. The use of the upper range of prehypertension as screening criteria would result in masked hypertension not being identified in many people. The current study provides empirical data on various approaches for identifying masked hypertension in untreated adults with nonelevated CBP.
Funding Sources
JNBIII: receives support through F31 HL129701 from the National, Heart, Lung, and Blood Institute; PM: receives research support from National Institutes of Health grant R01 HL080477 and Amgen, Inc.; KMD: receives support through R01 HL116470‐02S1 from the National, Heart, Lung, and Blood Institute; AJV: receives support through grant R01‐HL098604; JES: receives support through grant P01‐HL047540; DS: receives support through grants P01‐HL047540, R01 HL117323‐01, and K24‐HL125704 from the National Heart, Lung, and Blood Institute.
Disclosures
Dr Muntner received an institutional grant from Amgen Inc. Dr Viera has served on the Medical Advisory Board for Suntech Medical, a manufacturer of a brand of ambulatory blood pressure monitor. There are no other conflicts of interest.
Supporting information
Data S1. Supplementary Methods
Figure S1. Receiver operating characteristic curve with different sensitivities (99%, 95%, 90%, 85%, 80%, and 75%) for detecting masked daytime hypertension using predicted probabilities based on clinic systolic and diastolic blood pressure in patients in the Masked Hypertension Study.
Figure S2. Scatterplot of clinic systolic vs diastolic blood pressure demonstrating derived cut points corresponding with specified sensitivity levels for detecting masked daytime hypertension using the clinic blood pressure index equation in patients in the Masked Hypertension Study (n=695).
Table S1. Odds ratio and area under the receiver operator characteristic curve for masked daytime hypertension† associated with clinic blood pressure and other characteristics of patients in the Masked Hypertension Study with nonelevated‡ clinic blood pressure and not taking antihypertensive medication.
Table S2. Test characteristics for detecting masked daytime hypertension (n=134) associated with prehypertension, upper range of prehypertension, and an elevated clinic blood pressure diagnostic index in patients in the Masked Hypertension Study (n=695).
Authors' Contributions
Study conception and design: JNBIII, PM, KMD, JES, DS; acquisition, analysis, or interpretation of data: JNBIII, PM, KMD, JES, DS; statistical analysis: JNBIII, PM, DS; drafting of the manuscript: JNBIII; critical revision of the manuscript: JNBIII, PM, KMD, AJV, NB, JES, DS; critical revision of the manuscript for important intellectual content: JNBIII, PM, KMD, AJV, NB, JS, DS, JNBIII, KMD, JES, and DS had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
J Clin Hypertens (Greenwich). 2016;18:1086–1094. DOI: 10.1111/jch.12830. © 2016 Wiley Periodicals, Inc.
References
- 1. Pickering TG, Davidson K, Gerin W, Schwartz JE. Masked hypertension. Hypertension. 2002;40:795–796. [DOI] [PubMed] [Google Scholar]
- 2. Peacock J, Diaz KM, Viera AJ, et al. Unmasking masked hypertension: prevalence, clinical implications, diagnosis, correlates and future directions. J Hum Hypertens. 2014;28:521–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Hansen TW, Kikuya M, Thijs L, et al. Prognostic superiority of daytime ambulatory over conventional blood pressure in four populations: a meta‐analysis of 7,030 individuals. J Hypertens. 2007;25:1554–1564. [DOI] [PubMed] [Google Scholar]
- 4. Diaz KM, Veerabhadrappa P, Brown MD, et al. Prevalence, determinants, and clinical significance of masked hypertension in a population‐based sample of African Americans: the Jackson Heart Study. Am J Hypertens. 2015;28:900–908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. O'Brien E, Parati G, Stergiou G, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31:1731–1768. [DOI] [PubMed] [Google Scholar]
- 6. Krause T, Lovibond K, Caulfield M, et al. Guideline Development G. Management of hypertension: summary of NICE guidance. BMJ. 2011;343:d4891. [DOI] [PubMed] [Google Scholar]
- 7. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–2219. [DOI] [PubMed] [Google Scholar]
- 8. O'Brien E, Asmar R, Beilin L, et al. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003;21:821–848. [DOI] [PubMed] [Google Scholar]
- 9. O'Brien E, Coats A, Owens P, et al. Use and interpretation of ambulatory blood pressure monitoring: recommendations of the British hypertension society. BMJ. 2000;320:1128–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–1252. [DOI] [PubMed] [Google Scholar]
- 11. Mancia G, De Backer G, Dominiczak A, et al. 2007 ESH‐ESC Practice guidelines for the management of arterial hypertension: ESH‐ESC task force on the management of arterial hypertension. J Hypertens. 2007;25:1751–1762. [DOI] [PubMed] [Google Scholar]
- 12. Head GA, McGrath BP, Mihailidou AS, et al. Ambulatory blood pressure monitoring in Australia: 2011 consensus position statement. J Hypertens. 2012;30:253–266. [DOI] [PubMed] [Google Scholar]
- 13. Verdecchia P, O'Brien E, Pickering T, et al. When can the practicing physician suspect white coat hypertension? Statement from the working group on blood pressure monitoring of the European Society of Hypertension. Am J Hypertens. 2003;16:87–91. [DOI] [PubMed] [Google Scholar]
- 14. Williams B, Poulter NR, Brown MJ, et al. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004‐BHS IV. J Hum Hypertens. 2004;18:139–185. [DOI] [PubMed] [Google Scholar]
- 15. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the subcommittee of professional and public education of the American Heart Association council on high blood pressure research. Hypertension. 2005;45:142–161. [DOI] [PubMed] [Google Scholar]
- 16. Alessi A, Brandao AA, Pierin A, et al. IV Guideline for ambulatory blood pressure monitoring. II Guideline for home blood pressure monitoring. IV ABPM/II HBPM. Arq Bras Cardiol. 2005;85(Suppl 2):1–18. [DOI] [PubMed] [Google Scholar]
- 17. Parati G, Omboni S, Palatini P, et al. Italian Society of Hypertension guidelines for conventional and automated blood pressure measurement in the office, at home and over 24 hours. High Blood Press Cardiovasc Prev. 2008;15:283–310. [DOI] [PubMed] [Google Scholar]
- 18. Ogihara T, Kikuchi K, Matsuoka H, et al. The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2009). Hypertens Res. 2009;32:3–107. [PubMed] [Google Scholar]
- 19. Daskalopoulou SS, Khan NA, Quinn RR, et al. The 2012 Canadian hypertension education program recommendations for the management of hypertension: blood pressure measurement, diagnosis, assessment of risk, and therapy. Can J Cardiol. 2012;28:270–287. [DOI] [PubMed] [Google Scholar]
- 20. Seedat YK, Rayner BL, Southern African Hypertension Society . South African hypertension guideline 2011. S Afr Med J. 2012;2:57–83. [PubMed] [Google Scholar]
- 21. Group JCSJW. Guidelines for the clinical use of 24 hour ambulatory blood pressure monitoring (ABPM) (JCS 2010): ‐ digest version. Circ J. 2012;76:508–519. [DOI] [PubMed] [Google Scholar]
- 22. Shimbo D, Newman JD, Schwartz JE. Masked hypertension and prehypertension: diagnostic overlap and interrelationships with left ventricular mass: the Masked Hypertension Study. Am J Hypertens. 2012;25:664–671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Elliott WJ, Black HR. Prehypertension. Nat Clin Pract Cardiovasc Med. 2007;4:538–548. [DOI] [PubMed] [Google Scholar]
- 24. Abdalla M, Goldsmith J, Muntner P, et al. Is isolated nocturnal hypertension a reproducible phenotype? Am J Hypertens. 2016;29:33–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Taylor HA Jr, Wilson JG, Jones DW, et al. Toward resolution of cardiovascular health disparities in African Americans: design and methods of the Jackson Heart Study. Ethn Dis. 2005;4(Suppl 6):S6–4. [PubMed] [Google Scholar]
- 26. NCHS Statistics . National Health and Nutrition Examination Survey: Center for Disease Control and Prevention. http://www.cdc.gov/nchs/nhanes.htm. Accessed September 10, 2015.
- 27. Wilson JG, Rotimi CN, Ekunwe L, et al. Study design for genetic analysis in the Jackson Heart Study. Ethn Dis. 2005;4(Suppl 6):S6–S30. [PubMed] [Google Scholar]
- 28. Barker MH, Erlanger J, Meakins J, et al. Standard method for taking and recording blood pressure readings. J Am Med Assoc 1939;113:294–297. [Google Scholar]
- 29. Investigators. TJHS. Jackson Heart Study Protocol Manual 4: Blood Pressure, Visit 1. February 18, 2001 2001.
- 30. Thijs L, Hansen TW, Kikuya M, et al. The International Database of Ambulatory Blood Pressure in relation to Cardiovascular Outcome (IDACO): protocol and research perspectives. Blood Press Monit. 2007;12:255–262. [DOI] [PubMed] [Google Scholar]
- 31. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the subcommittee of professional and public education of the American Heart Association council on high blood pressure research. Circulation. 2005;111:697–716. [DOI] [PubMed] [Google Scholar]
- 32. Fan HQ, Li Y, Thijs L, et al. Prognostic value of isolated nocturnal hypertension on ambulatory measurement in 8711 individuals from 10 populations. J Hypertens. 2010;28:2036–2045. [DOI] [PubMed] [Google Scholar]
- 33. Shimbo D, Kuruvilla S, Haas D, et al. Preventing misdiagnosis of ambulatory hypertension: algorithm using office and home blood pressures. J Hypertens. 2009;27:1775–1783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Pickering TG. The natural history of hypertension: prehypertension or masked hypertension? J Clin Hypertens (Greenwich). 2007;9:807–810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Redmond N, Booth JN III, Tanner RM, et al. Associations of masked hypertension and prehypertension with subclinical cardiovascular disease in African Americans: results from the Jackson Heart Study. (under review). [DOI] [PMC free article] [PubMed]
- 36. Fagard RH, Celis H, Thijs L, et al. Daytime and nighttime blood pressure as predictors of death and cause‐specific cardiovascular events in hypertension. Hypertension. 2008;51:55–61. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1. Supplementary Methods
Figure S1. Receiver operating characteristic curve with different sensitivities (99%, 95%, 90%, 85%, 80%, and 75%) for detecting masked daytime hypertension using predicted probabilities based on clinic systolic and diastolic blood pressure in patients in the Masked Hypertension Study.
Figure S2. Scatterplot of clinic systolic vs diastolic blood pressure demonstrating derived cut points corresponding with specified sensitivity levels for detecting masked daytime hypertension using the clinic blood pressure index equation in patients in the Masked Hypertension Study (n=695).
Table S1. Odds ratio and area under the receiver operator characteristic curve for masked daytime hypertension† associated with clinic blood pressure and other characteristics of patients in the Masked Hypertension Study with nonelevated‡ clinic blood pressure and not taking antihypertensive medication.
Table S2. Test characteristics for detecting masked daytime hypertension (n=134) associated with prehypertension, upper range of prehypertension, and an elevated clinic blood pressure diagnostic index in patients in the Masked Hypertension Study (n=695).