

Dear Editor,
This is a case report of a male patient, 47 years of age, with a one-year history of an asymptomatic nodular mass on the left hallux. The patient reported gradual growth, with a rapid increase in size over the past two months.
The dermatological examination revealed a firm, painless mass, measuring approximately 5 x 4 cm, on the left hallux (Figures 1A and 1B).
Figure 1.

A. Firm mass on left hallux (front image). B: Medial fact image of left hallux
The radiographic examination showed no cortical erosion.
Microscopic examination revealed a lesion predominantly consisting of mononuclear cells and multinucleated giant cells, dispersed in hyalinized collagen fiber bundles. These findings are compatible with giant cell tumors of the tendon sheath (Figures 2 and 3).
Figure 2.
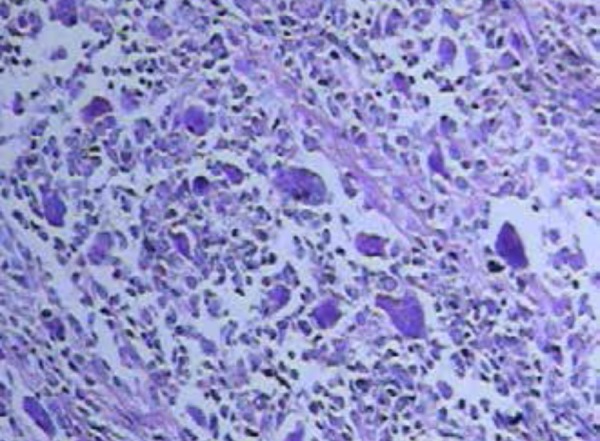
Lobed lesion consisting of mononuclear cells, multinucleated giant cells similar to osteoclasts, histiocytes, and lymphocytes. Dense collagenous stroma can be observed (HE 100x)
Figure 3.
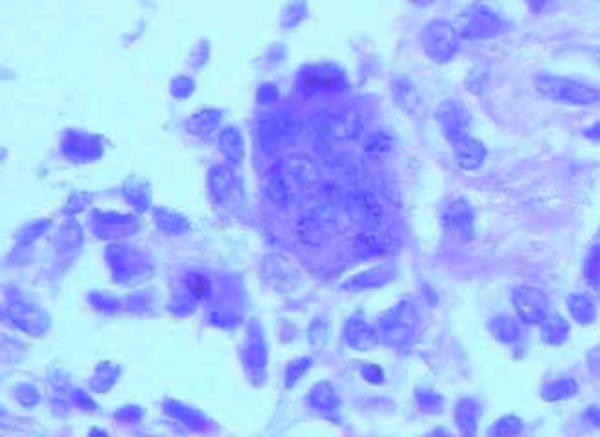
Detail of multinucleated giant cell similar to osteoclast (HE 400x)
The patient underwent tumor wide excision performed by the orthopedist.
Giant cell tumors of the tendon sheath (GCT-TS) are solitary benign tumors that represent the second most common tumor on the hand, after ganglion cysts. However, this type of lesion is rare on the foot. Chassaignac was the first to describe these benign masses in 1852 and referred to them as tendon sheath cancer. Jaffe was the first, in 1941, to describe GCT-TS as tenosynovitis, a non-neoplastic malignant reaction.1
Etiopathogenesis of GCT-TS is unknown, but some authors suggest that this disease results from alterations in lipid metabolism, inflammation or other benign neoplastic processes. The possibility of this disease being caused by trauma has been reported in prior literature. 1-4
Typically, the tumor appears between the third and fifth decades of life, slightly favoring females, at a 2:3 ratio. Lesions are usually local, solitary, appearing as painful or painless subcutaneous nodules.1
Radiographs may show whether or not there are erosions under the cortical bone.2,4
Histologically speaking, a typical GCT-TS consists of mononuclear cells and multinucleated giant cells spread throughout the hyalinized collagen bundles. Giant cells resemble osteoclasts, microscopically and ultrastructurally, and other smaller cells are stretched and resemble fibroblasts,1 as seen in the present case (Figures 2 and 3).
GCT-TS differential diagnoses include: proliferating pilomatricoma, ganglion cysts, pigmented villonodular synovitis, desmoid tumor, glomangioma, and rheumatoid nodule. 1-5
Preferred treatment is local excision.1-4 Tumor relapses have been described in prior literature.2,3 Despite being the second most common hand tumor, few GCT-TS cases have been published by dermatologists or found in prior English-language medical literature.
Footnotes
Conflict of Interest: None
Financial Support: None
Work conducted at the Dermatology Clinic of the Northern Paraná Regional University Hospital, Universidade Estadual de Londrina (UEL), Londrina , PR, Brazil.
REFERENCES
- 1.Di Grazia S, Succi G, Fragetta F, Perrotta RE. Giant cell tumor of tendon sheath study: of 64 cases and review of literature. G Chir. 2013;34:149–152. doi: 10.11138/gchir/2013.34.5.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Patel AS, Thaker P, Patel R, Ladumore M, Prabhakar MM. A rare case report of giant cell tumor of a tendon sheath. Int J Med Sci Public Health. 2016;5:829–831. [Google Scholar]
- 3.Occhipinti E, Heinrich SD, Craver R. Giant cell tumor of tendon sheath arising in the toe. Fetal Pediatr Pathol. 2004;23:171–179. doi: 10.1080/15227950490890441. [DOI] [PubMed] [Google Scholar]
- 4.Kuo CL, Yang SW, Chou YJ, Wong CY. Giant cell tumor of the EDL tendon sheath: an unusual cause of hallux valgus. Foot Ankle Int. 2008;29:534–537. doi: 10.3113/FAI-2008-0534. [DOI] [PubMed] [Google Scholar]
- 5.Kondo RN, Pontello R, Junior, Belinetti FM, Cilião C, Vasconcellos VR, Grimaldi DM. Pilomatricoma proliferante - relato de caso. An Bras Dermatol. 2015;90:94–96. doi: 10.1590/abd1806-4841.20153972. [DOI] [PMC free article] [PubMed] [Google Scholar]