

Abstract
Objective
The aim of this meta-analysis was to evaluate the efficacy and safety of levomilnacipran extended-release (ER) in the treatment of major depressive disorder (MDD).
Methods
Randomized controlled trials were searched by electronic databases. Unpublished data were also searched by the relevant websites. Weighted mean difference (WMD) and risk ratio (RR) with 95% confidence interval (CI) were calculated and pooled using fixed-effects model or random-effects model.
Results
Five randomized placebo-controlled trials including 2,637 patients were analyzed. Compared with placebo, levomilnacipran ER had a greater reduction in the Montgomery–Åsberg Depression Rating Scale (MADRS) total score and Sheehan Disability Scale (SDS) total score (MADRS: WMD −3.49 [95% CI −4.28, −2.70; P<0.00001]; SDS: WMD −2.41 [95% CI −3.05, −1.77; P<0.00001]). Significantly more patients in levomilnacipran ER achieved MADRS response rate (RR 1.35 [95% CI 1.23, 1.47; P<0.00001]) and MADRS remission rate (RR 1.30 [95% CI 1.06, 1.59; P=0.01]). In terms of safety, more patients discontinued due to adverse events (AEs) in levomilnacipran ER compared with placebo (RR 3.15 [95% CI 2.26, 4.39; P<0.00001]), but it was generally well tolerated in each eligible trial. The most common AEs were nausea, delay in ejaculation, erectile dysfunction, tachycardia, headache and increase in heart rate.
Conclusion
Levomilnacipran ER is a safe and effective short-term treatment for MDD (≤10 weeks). Long-term and head-to-head trials comparing levomilnacipran ER with other antidepressants are needed to confirm the conclusion.
Keywords: levomilnacipran ER, SNRI, major depressive disorder, meta-analysis
Introduction
Major depressive disorder (MDD) is one of the most prevalent mental disorder and is estimated to be the fourth leading cause of disease burden worldwide.1,2 Pharmacotherapy is the primary choice for MDD. However, most antidepressants lacked efficacy and tolerability for patients with MDD, and adverse effects were the leading reasons of discontinuation during the treatment.3,4 Therefore, new antidepressants that can offer a greater advantage in efficacy and tolerability are needed. In this regard, levomilnacipran, which has a unique pharmacological activity compared with currently marketed serotonin–norepinephrine reuptake inhibitors (SNRIs), may prove to be an appealing alternative.
Levomilnacipran (1S, 2R-milnacipran) extended-release (ER), as the fourth SNRI, was approved by the US Food and Drug Administration (FDA) in July 2013 with doses of 40–120 mg capsule once daily.5 In vitro studies have shown that levomilnacipran ER has twofold greater potency for norepinephrine compared with serotonin reuptake inhibition.6 Compared with duloxetine, desvenlafaxine, or venlafaxine, levomilnacipran ER showed 10-fold greater selectivity for inhibiting norepinephrine reuptake.7
The efficacy and safety of levomilnacipran ER have been evaluated in several clinical studies, but the evaluation results were not completely consistent. A recent review had pooled the efficacy of levomilnacipran ER for MDD, using Cohen’s d and number-needed-to-treat (NNT) as effect sizes,8 which did not evaluate the safety of levomilnacipran ER and the effect on Sheehan Disability Scale (SDS). However, a significant improvement in SDS may demonstrate efficacy in treating functional impairment.9 Thus, the aims of this article were to systematically review the existing published data regarding the treatment of MDD comparing levomilnacipran ER and placebo (including Montgomery–Åsberg Depression Rating Scale [MADRS] total score, SDS total score, response rate, remission rate, adverse effects, and cardiovascular effects) and to evaluate the efficacy and safety of levomilnacipran ER.
Methods
Data sources and search strategy
We searched PubMed, Embase, Medline, Ovid, the Cochrane Collaboration Library, Scopus and ScienceDirect, PsycInfo, and International Pharmaceutical Abstracts from inception to March 2016, without restriction of language. Potentially relevant unpublished data were searched by ClinicalTrials.gov, FDA website, European Union Drug Regulating Authorities Clinical Trials and the World Health Organization International Clinical Trials Registry Platform. We used the following terms: “levomilnacipran”, “LVM”, “fetzlma”, “F2695”, “major depressive disorder”, “depression or major depression”, and “MDD”. These terms were adjusted to comply with the relevant rules in each database.
Study election
Two investigators (QH and XZ) independently reviewed the title and abstract and selected randomized controlled trials of levomilnacipran ER for the treatment of MDD. All the studies met the following criteria:
All patients (18–80 years of age) were diagnosed for MDD by the Diagnostic and Statistical Manual of Mental Disorder, fourth edition, text revision and confirmed by the Mini International Neuropsychiatric Interview.
All patients were required to have baseline MADRS total score ≥26.
MADRS total score was used as the primary outcome in eligible studies.
Studies included one or more of the secondary outcomes: SDS total score, MADRS remission rate (total score ≤10), MADRS response rate (≥50% improvement from baseline), adverse events (AEs), and cardiovascular effects.
Full-text articles were retrieved independently by two investigators (QH and XZ). If they had a disagreement, the third investigator (YH) was used to solve the disagreement when necessary.
Data extraction
Data were extracted by two investigators (QH and XZ), and any discrepancies were resolved by consensus. For each study, two investigators (QH and XZ) extracted information on study characteristics, participants’ baseline characteristics, interventions of the trial, end points, and findings.
Quality assessment
Two investigators (QH and XZ) assessed the quality of included studies by using the risk of bias tool.10 The predefined key domains included random sequence generation, allocation concealment, blinding, and other items (ie, efficacy analysis, lost to follow-up, intention-to-treat analysis, and statistical analysis).
Statistical analysis
All outcomes were pooled by using RevMan 5.3 software (Nordiac Cochrane Center, Copenhagen, Denmark; http://www.cochrane.org/). For dichotomous data, risk ratio (RR) was calculated with 95% confidence intervals (CIs). On the other hand, in case of continuous data, we used weighted mean difference (WMD) with 95% CIs. We calculated the I2 statistic to estimate heterogeneity. If I2 was <50%, we chose fixed-effect model with the analyses of the Mantel–Haenszel method; otherwise, the random-effect model was adopted.
Results
Literature search and study characteristics
A total of 859 records were identified by our initial search. According to title and abstract, we excluded 825 records (irrelevant, annual meeting, animal, duplicates). Finally, we excluded 29 records and confirmed five studies that met the inclusion criteria by two investigators screening full-text articles. The flow of study search and selection is shown in Figure 1.
Figure 1.
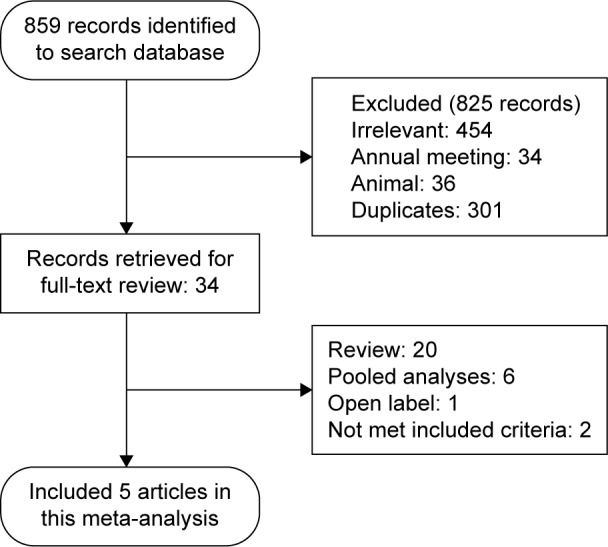
The flow of the study search and selection.
Five studies were randomized, double-blind, placebo-controlled trials. These included two fixed-dose trials11,12 and three flexible-dose trials.13–15 Trial durations ranged from 8 to 10 weeks. A total of 2,637 patients were randomized to the levomilnacipran ER group and placebo group, 2,623 patients were used for safety analyses and 2,598 patients were used for modified intent-to-treat and efficacy analyses (1,032 were randomized to placebo and 1,566 to the levomilnacipran ER group). The basic characteristics of the study are listed in Table 1.
Table 1.
The basic characteristics of randomized controlled trials (mean ±SD)
| Study | Duration of intervention (wk) | Interventions (n) | Age (years) | Weight (kg) | Baseline MADRS score | Outcomes |
|---|---|---|---|---|---|---|
| Asnis et al11 | 8 | LVM 40 mg/d (178) | 41.6±13.1 | 79.5±17.1 | 35.6±4.5 | MADRS, SDS: response, remission |
| LVM 80 mg/d (179) | 41.0±12.8 | 83.0±17.3 | 36.0±4.1 | |||
| LVM 120 mg/d (180) | 40.3±11.9 | 84.2±18.6 | 36.1±3.9 | |||
| Placebo (176) | 41.3±11.3 | 83.8±19.3 | 36.0±3.9 | |||
| Bakish et al12 | 8 | LVM 40 mg/d (188) | 42.9±13.4 | 81.3±17.0 | 30.8±3.4 | MADRS, SDS: response, remission |
| LVM 80 mg/d (188) | 43.1±12.8 | 81.7±17.5 | 31.2±3.5 | |||
| Placebo (186) | 42.3±13.2 | 81.6±17.7 | 31.0±3.8 | |||
| Gommoll et al13 | 8 | LVM flexible dose (175) | 42.8±12.9 | 82.4±18.1 | 35.9±4.1 | MADRS, SDS: response, remission |
| Placebo (182) | 43.7±13.3 | 82.9±18.0 | 35.5±4.0 | |||
| Sambunaris et al14 | 8 | LVM flexible dose (222) | 45.0±13.2 | 84.4±18.9 | 35.0±3.6 | MADRS, SDS: response, remission |
| Placebo (220) | 44.6±13.9 | 84.5±18.1 | 35.2±3.8 | |||
| Montgomery et al15 | 10 | LVM flexible dose (282) | 45 | N/R | 30.9±4.1 | MADRS, SDS: response, remission |
| Placebo (281) | 44 | N/R | 30.5±3.7 |
Abbreviations: wk, week; MADRS, Montgomery–Åsberg Depression Rating Scale; LVM, levomilnacipran; d, day; SDS, Sheehan Disability Scale; N/R, not reported; SD, standard deviation.
Quality assessment
All eligible studies described the generation of the randomization sequence. However, allocation concealment was unclear in one study.14 All studies were at least double blind. Five studies reported adequate intention-to-treat analysis.11–15 Loss to follow-up was minimal and balanced in the five trials. Details of risk of bias assessment are shown in Table 2.
Table 2.
Risk of bias assessment
| Study | Random sequence generation | Allocation concealment | Blinding | Efficacy analysis | Lost to follow-up | ITT | Statistical analysis |
|---|---|---|---|---|---|---|---|
| Asnis et al11 | Y | Y | Y | MMRM | Y | Y | ANCOVA |
| Bakish et al12 | Y | Y | Y | MMRM | Y | Y | ANCOVA |
| Gommoll et al13 | Y | Y | Y | MMRM | Y | Y | ANCOVA |
| Sambunaris et al14 | Y | U | Y | FAS | Y | N | ANCOVA |
| Montgomery et al15 | Y | Y | Y | MMRM | Y | Y | ANCOVA |
Abbreviations: ITT, intention to treat; Y, yes; MMRM, mixed-model for repeated measures; ANCOVA, analysis of covariance; U, unclear; FAS, full analysis set; N, no.
MADRS total score
Compared with placebo, a statistically significant reduction in the MADRS total score was observed in the levomilnacipran ER group (WMD −3.49 [95% CI −4.28, −2.70; P<0.00001]; Figure 2). The subgroup analysis results were WMD −3.26 (95% CI −4.95, −1.57; P=0.0002) for 40 mg, WMD −3.45 (95% CI −5.14, −1.75; P<0.0001) for 80 mg, WMD −4.90 (95% CI −7.66, −2.14; P=0.0005) for 120 mg, and WMD −3.37 (95% CI −4.50, −2.24; P<0.00001) for 40–120 mg (Figure 2).
Figure 2.

Meta-analysis for change in the MADRS total score from baseline, levomilnacipran ER versus placebo.
Abbreviations: MADRS, Montgomery–Åsberg Depression Rating Scale; ER, extended-release; IV, inverse variance; CI, confidence interval; SD, standard deviation.
In a sensitivity analysis, pooling the data on MADRS showed that the overall estimate was not impacted by excluding a phase II study15 (WMD −3.24 [95% CI −4.16, −2.33; P<0.00001]).
SDS total score
The pooled effects estimate of the SDS total score was −2.41 (95% CI −3.05, −1.77; P<0.00001). The results of the subgroup analysis also demonstrated that levomilnacipran ER was superior to placebo on the SDS total score (40 mg: WMD −1.68 [95% CI −3.06, −0.30; P=0.02], 80 mg: WMD −2.67 [95% CI −4.05, −1.29; P=0.0001], 120 mg: WMD −2.5 [95% CI −4.61, −0.39; P=0.02], and 40–120 mg: WMD −2.35 [95% CI −3.88, −0.82; P=0.003]; Figure 3).
Figure 3.

Meta-analysis for change in the SDS total score from baseline, levomilnacipran ER versus placebo.
Abbreviations: SDS, Sheehan Disability Scale; ER, extended-release; IV, inverse variance; CI, confidence interval.
Response rate and remission rate
Levomilnacipran ER had a greater improvement in the MADRS response rate compared with placebo (40 mg: RR 1.36 [95% CI 1.12, 1.64; P=0.002], 80 mg: RR 1.34 [95% CI 1.10, 1.62; P=0.003], 120 mg: RR 1.42 [95% CI 1.06, 1.90; P=0.02], and 40–120 mg: RR 1.33 [95% CI 1.17, 1.51; P<0.0001]). The overall RR was 1.35 (95% CI 1.23, 1.47; P<0.00001; Figure 4).
Figure 4.

Meta-analysis for MADRS response rate (≥50% improvement from baseline), levomilnacipran ER versus placebo.
Abbreviations: MADRS, Montgomery–Åsberg Depression Rating Scale; ER, extended-release; M–H, Mantel–Haenszel; CI, confidence interval.
The overall RR for the MADRS remission rate was 1.30 (95% CI 1.06, 1.59; P=0.01). The subgroup analysis results were RR 1.38 (95% CI 0.91, 2.10; P=0.12) for 40 mg, RR 1.40 (95% CI 0.85, 2.32; P=0.19) for 80 mg, RR 1.05 (95% CI 0.69, 1.60; P=0.81) for 120 mg, and RR 1.24 (95% CI 0.81, 1.91; P=0.31; Figure 5) for 40–120 mg.
Figure 5.

Meta-analysis for MADRS remission rate (total score ≤10), levomilnacipran ER versus placebo.
Abbreviations: MADRS, Montgomery–Åsberg Depression Rating Scale; ER, extended-release; M–H, Mantel–Haenszel; CI, confidence interval.
Safety and tolerability
Compared with placebo, the overall rate of discontinuation and discontinuation due to AEs was higher for levomilnacipran ER (Table 3). Incidences of AEs (erectile dysfunction, delay in ejaculation, tachycardia, nausea, hedache, dry mouth, increase in heart rate) were higher for levomilnacipran ER (Table 3). The incidences of suicidal ideation and suicidal behavior were similar between the two groups (Table 3).
Table 3.
Meta-analysis for the safety outcomes (dichotomous data)
| Outcome | Levomilnacipran (n/N) |
Placebo (n/N) |
Effect estimate (95% CI) |
I2 (%) | P-value |
|---|---|---|---|---|---|
| Discontinuation due to all reasonsa | 405/1,583 | 324/1,040 | 1.24 (1.09, 1.42) | 42 | 0.008 |
| Discontinuation due to AE | 139/1,583 | 44/1,040 | 3.15 (2.26, 4.39) | 41 | <0.00001 |
| Erectile dysfunctionb | 29/406 | 9/204 | 3.26 (1.56, 6.81) | 0 | 0.002 |
| Ejaculation delayedb | 16/351 | 0/208 | 10.96 (2.09, 57.56) | 0 | 0.005 |
| Tachycardia | 74/1,408 | 15/858 | 3.12 (1.50, 6.47) | 43 | 0.002 |
| Nausea | 272/1,583 | 60/1,040 | 3.80 (2.47, 5.83) | 62 | <0.00001 |
| Headache | 262/1,583 | 136/1,040 | 1.40 (1.18, 1.66) | 0 | 0.0001 |
| Dry mouth | 160/1,583 | 73/1,040 | 1.40 (1.11, 1.76) | 25 | 0.004 |
| Insomnia | 67/1,207 | 41/854 | 1.22 (0.86, 1.73) | 0 | 0.26 |
| Heart rate increase | 98/1,088 | 13/544 | 0.06 (0.04, 0.09) | 33 | <0.00001 |
| Suicidal ideation | 316/1,573 | 172/1,037 | 1.03 (0.89, 1.19) | 9 | 0.72 |
| Suicidal behavior | 5/573 | 1/390 | 2.17 (0.49, 9.62) | 0 | 0.31 |
Notes:
Discontinuation due to AEs, insufficient therapeutic response, protocol violation, loss to follow-up and other reasons.
Based on the number of men in the safety population. Bold numbers are considered statistically significant.
Abbreviations: CI, confidence interval; AE, adverse event.
Compared with placebo, levomilnacipran ER showed greater increase in the pulse rate (WMD 7.56 [95% CI 6.81, 8.31; P<0.00001]), systolic blood pressure (WMD 3.14 [95% CI 2.37, 3.90; P<0.00001]), diastolic blood pressure (WMD 3.45 [95% CI 2.86, 4.05; P<0.00001]), and Bazett formula (QTcB; Table 4). In the five eligible studies, based on the Fridericia correction (QTcF), there was no QTc prolongation. None of the patients met potentially clinically significant criteria for PR (≥250 milliseconds), QTcB (>500 milliseconds), or QTcF (>500 milliseconds) interval.
Table 4.
Meta-analysis for the safety outcomes (continuous data)
| Outcome | Studies (n) | Participants analyzed (n)
|
WMD (95% CI) | I2 (%) | P-value | |
|---|---|---|---|---|---|---|
| Levomilnacipran | Placebo | |||||
| Pulse rate | 4 | 1,298 | 756 | 7.56 (6.81, 8.31) | 20 | <0.00001 |
| SBP | 4 | 1,300 | 756 | 3.14 (2.37, 3.90) | 0 | <0.00001 |
| DPB | 4 | 1,300 | 756 | 3.45 (2.86, 4.05) | 0 | <0.00001 |
| QTcB | 3 | 1,171 | 631 | 8.59 (6.97, 10.20) | 0 | <0.00001 |
Abbreviations: WMD, weighted mean difference; CI, confidence interval; SBP, systolic blood pressure; DPB, diastolic blood pressure.
Discussion
In our systematic review and meta-analysis, levomilnacipran ER resulted in reduction in the MADRS total score and SDS total score compared with placebo. Levomilnacipran ER has a unique pharmacological activity and is relatively more selective for norepinephrine reuptake inhibition than serotonin reuptake inhibition.6 The strong noradrenergic component of antidepressant may be especially effective in improving symptoms related to functioning.16,17 Symptomatic and functional improvements are both critical components of recovery from MDD. Symptomatic improvement may provide an early sign of treatment response, and functional improvement may be a better indicator of meaningful change.18 The MADRS total score >2 points for the test group versus placebo, which suggests that symptomatic improvement is clinically relevant.19 A significant improvement in SDS means that function is improved.9 In our study, the MADRS score exceeded 3.36 points for levomilnacipran ER compared with placebo. In addition, a significant difference in favor of levomilnacipran ER was also observed in the SDS total score. These observations may indicate that levomilnacipran ER might provide both symptomatic and functional efficacies.
If the response rate far exceeds the 10% average advantage for drug versus placebo, it is generally regarded as sufficient to establish antidepressant treatment advantage.20 In our results, the rate of MADRS response was significantly greater for levomilnacipran ER versus placebo.
Most likely due to levomilnacipran ER related to the twofold greater potency for norepinephrine reuptake inhibition compared with serotonin reuptake inhibition,6 levomilnacipran ER was generally well tolerated in the five eligible studies, which was consistent with the results of 48-week open-label study and the 39-week relapse prevention study.21,22 However, compared with placebo, most incidences of AEs were higher for levomilnacipran ER. The five eligible studies showed that the common AEs were nausea, delay in ejaculation, erectile dysfunction, tachycardia, headache, and increase in heart rate. Pulse rate and blood pressure increases were greater for levomilnacipran ER versus placebo. Greater increase in QTcB was observed in the levomilnacipran ER group compared with placebo, which was consistent with increases in heart rate. The mean QTcF changes were small in both groups. In suicidal ideation and suicidal behavior, levomilnacipran ER and placebo patients had similar numbers.
Milnacipran was approved for the management of fibromyalgia in the US and for the treatment of MDD in many countries outside the US.23,24 A earlier systematic review had shown that there was no difference in the overall effectiveness and tolerability between milnacipran and other antidepressants (selective serotonin reuptake inhibitors [SSRIs], tricyclic antidepressants [TCAs]). Additionally, it has some advantages over TCAs in terms of discontinuation due to AEs and the rates of AEs.25 Levomilnacipran is the levo enantiomer of milnacipran. Regulatory guidelines in the US and Europe recommend development of the enantiomers over racemates where appropriate.26 Given the favorable pharmacokinetic and pharmacodynamic characteristics of enantiomeric formulation, levomilnacipran ER may be more effective than milnacipran. However, head-to-head trials with levomilnacipran ER and milnacipran have not been performed.
Limitations
There were also limitations in this meta-analysis. First, our analysis highlighted the overall short-term safety and efficacy of levomilnacipran ER; the extended period is needed to understand the long-term benefits and risks. Second, agomelatine is another novel antidepressant that does not induce 5-HT2A stimulation, having a more favorable adverse-effect profile compared with the common SSRIs.27 However, the lack of head-to-head trials limited the ability to compare levomilnacipran ER with agomelatine or other antidepressants. Future studies will be needed to compare levomilnacipran ER with other antidepressants. Third, strict inclusion and exclusion criteria might have limited these findings to a smaller population. Future larger studies designed to evaluate patients with recurrent or treatment-resistant depression are necessary. Fourth, levomilnacipran ER appears to display greater noradrenergic activity at a lower dose and increasing effects on serotonergic neurotransmission as the dose increases.28 However, our study did not detect dose–response effects, since most of the clinical studies used flexible dosing.
Conclusion
This meta-analysis indicated that levomilnacipran ER might be safe and effective for short-term treatment of MDD. However, large, multicenter, randomized controlled trials are still needed to assess the safety and efficacy of levomilnacipran ER. Furthermore, head-to-head trials comparing levomilnacipran ER with other antidepressants are needed to confirm the conclusion.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Ustün TB, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJ. Global burden of depressive disorders in the year 2000. Br J Psychiatry. 2004;184(5):386–392. doi: 10.1192/bjp.184.5.386. [DOI] [PubMed] [Google Scholar]
- 2.Tsuang MT, Taylor L, Faraone SV. An overview of the genetics of psychotic mood disorders. J Psychiatr Res. 2004;38(1):3–15. doi: 10.1016/s0022-3956(03)00096-7. [DOI] [PubMed] [Google Scholar]
- 3.Fava M. Diagnosis and definition of treatment-resistant depression. Biol Psychiatry. 2003;53(8):649–659. doi: 10.1016/s0006-3223(03)00231-2. [DOI] [PubMed] [Google Scholar]
- 4.Demyttenaere K, Enzlin P, Dewe W, et al. Compliance with antidepressants in a primary care setting, 1: beyond lack of efficacy and adverse events. J Clin Psychiatry. 2001;62(suppl 22):30–33. [PubMed] [Google Scholar]
- 5.Food and Drug administration US Food and Drug Administration Letter of New Drug Application Approval for Levomilnacipran Extended-Release Capsules (NDA204168) 2013. [Accessed November 27, 2013]. Available from: www.accessdata.fda.gov/drugsatfda_docs/appletter/2013/204168Orig1s000ltr.pdf.
- 6.Auclair AL, Martel JC, Assie MB, et al. Levomilnacipran (F2695), a norepinephrine-preferring SNRI: profile in vitro and in models of depression and anxiety. Neuropharmacology. 2013;70(5):338–347. doi: 10.1016/j.neuropharm.2013.02.024. [DOI] [PubMed] [Google Scholar]
- 7.Deecher DC, Beyer CE, Johnston G, et al. Desvenlafaxine succinate: a new serotonin and norepinephrine reuptake inhibitor. J Pharmacol Exp Ther. 2006;318(2):657–665. doi: 10.1124/jpet.106.103382. [DOI] [PubMed] [Google Scholar]
- 8.Montgomery SA, Gommoll CP, Chen C, Greenberg WM. Efficacy of levomilnacipran extended-release in major depressive disorder: pooled analysis of 5 double-blind, placebo-controlled trials. CNS Spectr. 2015;20(2):148–156. doi: 10.1017/S1092852914000273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hirschfeld RM, Montgomery SA, Keller MB, et al. Social functioning in depression: a review. J Clin Psychiatry. 2009;61(4):268–275. doi: 10.4088/jcp.v61n0405. [DOI] [PubMed] [Google Scholar]
- 10.Lundh A, Gotzsche PC. Recommendations by Cochrane Review Groups for assessment of the risk of bias in studies. BMC Med Res Methodol. 2008;8(3):57. doi: 10.1186/1471-2288-8-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Asnis GM, Bose A, Gommoll CP, Chen C, Greenberg WM. The efficacy and safety of levomilnacipran sustained release 40 mg, 80 mg, or 120 mg in major depressive disorder: a phase 3, randomized, double-blind, placebo-controlled study. J Clin Psychiatry. 2013;74(3):242–248. doi: 10.4088/JCP.12m08197. [DOI] [PubMed] [Google Scholar]
- 12.Bakish D, Bose A, Gommoll C, et al. Levomilnacipran ER 40 mg and 80 mg in patients with major depressive disorder: a phase III, randomized, double-blind, fixed-dose, placebo-controlled study. J Psychiatry Neurosci. 2014;39(1):40–49. doi: 10.1503/jpn.130040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gommoll C, Greenberg WM, Chen C, et al. A randomized double-blind, placebo-controlled, study of flexible doses of levomilnacipran ER (40–120 mg/day) in patients with major depressive disorder. J Drug Assess. 2014;3(1):10–19. doi: 10.3109/21556660.2014.884505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sambunaris A, Bose A, Gommoll CP, Chen C, Greenberg WM, Sheehan DV. A phase III, double-blind, placebo-controlled, flexible-dose study of levomilnacipran extended-release in patients with major depressive disorder. J Clin Psychopharmacol. 2014;34(1):47–56. doi: 10.1097/JCP.0000000000000060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Montgomery SA, Mansuy L, Ruth A, Bose A, Li H, Li D. Efficacy and safety of levomilnacipran sustained release in moderate to severe major depressive disorder: a randomized, double-blind, placebo-controlled, proof-of-concept study. J Clin Psychiatry. 2013;74(4):363–369. doi: 10.4088/JCP.12m08141. [DOI] [PubMed] [Google Scholar]
- 16.Kasper S, Meshkat D, Kutzelnigg A. Improvement of the noradrenergic symptom cluster following treatment with milnacipran. Neuropsychiatr Dis Treat. 2014;7(suppl 1):21–27. doi: 10.2147/NDT.S19615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Keller M. Role of serotonin and noradrenaline in social dysfunction: a review of data on reboxetine and the Social Adaptation Self-evaluation Scale (SASS) Gen Hosp Psychiatry. 2001;23(1):15–19. doi: 10.1016/s0163-8343(00)00115-8. [DOI] [PubMed] [Google Scholar]
- 18.McKnight PE, Kashdan TB. The importance of functional impairment to mental health outcomes: a case for reassessing our goals in depression treatment research. Clin Psychol Rev. 2009;29(3):243–259. doi: 10.1016/j.cpr.2009.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sheehan KH, Sheehan DV. Assessing treatment effects in clinical trials with the discan metric of the Sheehan Disability Scale. Int Clin Psychopharmacol. 2008;23(2):70–83. doi: 10.1097/YIC.0b013e3282f2b4d6. [DOI] [PubMed] [Google Scholar]
- 20.Thase ME. The small specific effects of antidepressants in clinical trials: what do they mean to psychiatrists? Curr Psychiatry Rep. 2011;13(6):476–482. doi: 10.1007/s11920-011-0235-x. [DOI] [PubMed] [Google Scholar]
- 21.Shiovitz T, Greenberg WM, Chen C, Forero G, Gommoll CPA. Randomized, double-blind, placebo controlled trial of the efficacy and safety of levomilnacipran ER 40–120 mg/day for prevention of relapse in patients with major depressive disorder. Innov Clin Neurosci. 2014;11(1–2):10–22. [PMC free article] [PubMed] [Google Scholar]
- 22.Mago R, Forero G, Greenberg WM, Gommoll C, Chen C. Safety and tolerability of levomilnacipran ER in major depressive disorder: results from an open-label, 48-week extension study. Clin Drug Investig. 2013;33(10):761–771. doi: 10.1007/s40261-013-0126-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Savella® (milnacipran) [package insert] St Louis, MO: Forest Laboratories Inc.; 2013. Available from: http://www.savellahcp.com/savella-dosage.aspx. [Google Scholar]
- 24.Montgomery S, Briley M. Milnacipran: recent findings in depression. Neuropsychiatr Dis Treat. 2010;6(suppl 1):1–2. doi: 10.2147/NDT.S19611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nakagawa A, Watanabe N, Omori IM, et al. Efficacy and tolerability of milnacipran in the treatment of major depression in comparison with other antidepressants: a systematic review and meta-analysis. CNS Drugs. 2008;22(7):587–602. doi: 10.2165/00023210-200822070-00004. [DOI] [PubMed] [Google Scholar]
- 26.FDA’s policy statement for the development of new stereoisomeric drugs. Chirality. 1992;4(5):338–340. doi: 10.1002/chir.530040513. [DOI] [PubMed] [Google Scholar]
- 27.Pompili M, Serafini G, Innamorati M, et al. Agomelatine, a novel intriguing antidepressant option enhancing neuroplasticity: a critical review. World J Biol Psychiatry. 2013;14(6):412–431. doi: 10.3109/15622975.2013.765593. [DOI] [PubMed] [Google Scholar]
- 28.Palmer EC, Binns LN, Carey H. Levomilnacipran: a new serotonin-norepinephrine reuptake inhibitor for the treatment of major depressive disorder. Ann Pharmacother. 2014;48(8):1030–1039. doi: 10.1177/1060028014535074. [DOI] [PubMed] [Google Scholar]