

Abstract
[Purpose] The purpose of this study was to examine the effect of the Schroth method (three-dimensional convergence exercise) of emphasis of active holding on pain and Cobb’s angle in patients with scoliosis. [Subjects and Methods] It applied the Schroth method program of emphasis of active holding individually to three subjects three time per week for 15 weeks. All subject were measured Cobb’s angle and pain. [Results] After 15 weeks, pain and Cobb’s angle decreased compared to values before. [Conclusion] These results demonstrate the benefit of the Schroth exercise program of emphasis of active holding on decreasing pain and Cobb’s angle in patients with idiopathic scoliosis.
Key words: Schroth method, Cobb’s angle, Idiopathic scoliosis
INTRODUCTION
The United States Scoliosis Research Society defines idiopathic scoliosis as a Cobb’s angle >10°, which increases the displacement and curvature of spine in the left and right sagittal plane1,2,3). Patients with idiopathic scoliosis have a three-dimensional deformation with lateral curvature and rotation of the vertebral body. About 70–80% of idiopathic scoliosis cases have an unknown cause3). The concave surface of the spinal curvature produces forward protrusion and the convex surface of the curvature produces a rearward protrusion in the ribs of the connecting vertebral body. Consequently, cardiopulmonary dysfunction and asymmetric ventilation occur in these patients4).
If the spinal red muscles becomes weak, the white muscle becomes overused and the red muscle becomes weaker because the deep spine muscles are mostly red slow-twitch muscle fibers5). Therefore, stability exercises with isotonic contractions are emphasized rather than simple mobility exercises to correct posture and regain control of white and red muscles in patients with idiopathic scoliosis6).
The Schroth method includes three-dimensional exercises used to treat treating scoliosis. These exercises provide sensorimotor and kinesthetic stimulation, thereby correcting the abnormal breathing patterns present in patients with scoliosis7).
The US Scoliosis Research Society recommends evaluating Cobb’s angle in patients with idiopathic scoliosis, which is measured from a standing posture radiograph8).
A detailed intervention with emphasis on active holding to regain stability is needed to improve idiopathic scoliosis with a broad range of deformation9). Therefore, this case study was performed to analyze the effect of the Schroth method with emphasis on active holding to regain stability, manage pain, and correct the Cobb’s angle in patients with idiopathic scoliosis.
CASE REPORT
The subjects were three patients with idiopathic scoliosis and Cobb’s angle ≥10°. It applied the Schroth method individually to subjects during 60 min sessions, three times per week, for 15 weeks. The Schroth method requires corrective movements and offers static or dynamic challenge. Intensity is based on the subject’s curve type and the level of passive support.
This study excluded subjects who had experienced treatments for idiopathic scoliosis, smokers, patients with asthma, lung disease, central nervous system disease, or a history of spine surgery. Consent was obtained from all subjects, and this study was approved by the University of Sahmyook University Ethics Board.
It evaluated idiopathic scoliosis by measuring Cobb’s angle (intersecting angle between the perpendicular to lines drawn parallel to the superior and inferior endplates of the most tilted vertebrae) at the coronal plane of the entire spine by X-ray (ED150L/R-500-150; Shimadzu Inc., Tokyo, Japan; Siremobil Compact/HRFC-100-P; Siemens Inc., Erlangen, Germany) and a computer-aided design program (CAD impact, Seoul, Korea)8).
A 21-year-old and male with idiopathic scoliosis had low back pain and iliocostal syndrome (visual analogue scale [VAS] score: 4), Cobb’s angle of 20°, and left deviation of the lumbar and right deviation of the hip and pelvis. It applied the Schroth method to stabilize the center area between the iliac crest and the twelfth thoracic vertebra. The apex of the lumbar curvature was mobilized in a muscle cylinder position of the right lateral. After applying the Schroth method, the VAS score decreased to 0 and Cobb’s angle was 10.8° (Fig. 1).
Fig. 1.
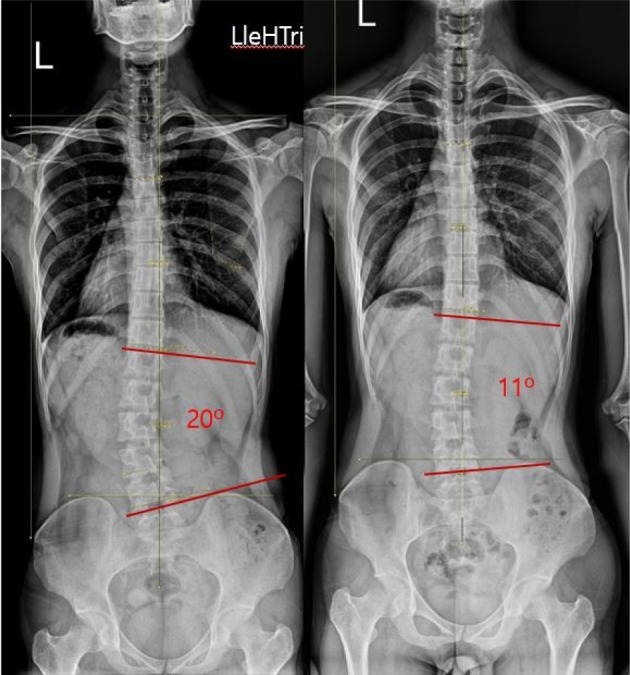
Change in Cobb’s angle in case 1
Subject was a 29-year-old female with idiopathic scoliosis had neck pain, headache (VAS score: 8), Cobb’s angle of 20.3° and a right deviation of the thoracic and a left deviation of the hip and pelvis. It applied the Schroth method with reverse force on the shoulder to stabilize the hip and pelvis. The thoracic area was mobilized in the Dresitz position. After applying the Schroth method, the VAS score decreased to 0 and Cobb’s angle was 4° (Fig. 2).
Fig. 2.
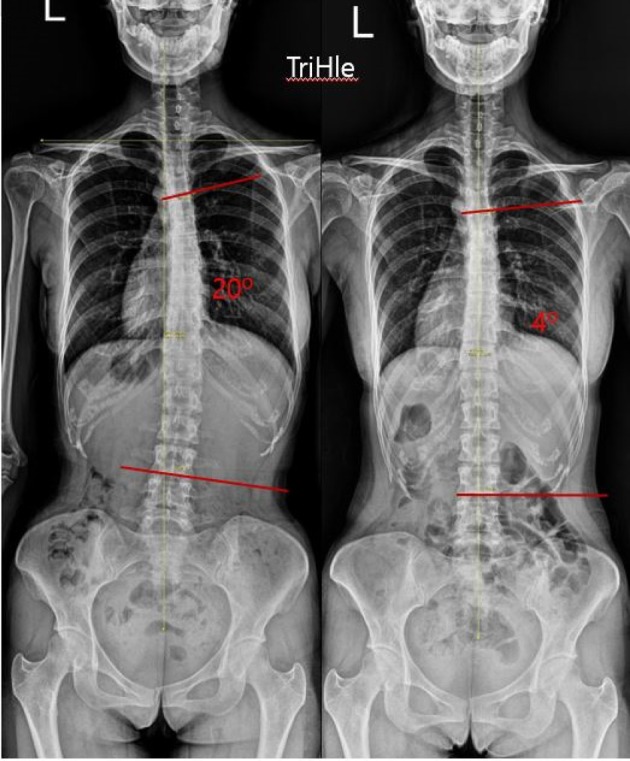
Change in Cobb’s angle in case 2
A 25-year-old female with idiopathic scoliosis had the neck pain and psoas syndrome (VAS score: 8), Cobb’s angle of 30.6°, and a right deviation of the lumbar and a left deviation of the thoracic. It applied the Schroth method to the center area between the iliac crest and the twelfth thoracic vertebra for stabilization. Then, the apex of the lumbar curvature was mobilized on left side by lying in the muscle cylinder position. After applying the Schroth method, the VAS score decreased to 3, and Cobb’s angle was 18.5° (Fig. 3).
Fig. 3.

Change in Cobb’s angle in case 3
DISCUSSION
The Schroth method was developed based on biomechanical and neurophysiological concepts without compensating for the curve in the spine, which undergoes axial elongation, deflexion, derotation, rotational breathing, and stabilization7). The Schroth method helps correct posture depending on the scoliosis type10, 11). In addition, a therapist educated in the memory of corrected posture recognizes abnormal during activities of daily living8, 9, 12, 13). Patients with idiopathic scoliosis must consider the of changed appearance after treatment and adjustment of Cobb’s angle8).
Patients with idiopathic scoliosis have a severely deformed spine1). Thus, the general treatment approach is to correct the deformation. Therefore, a detailed intervention is required with emphasis on active holding to gain mobility and stability9). This case study was performed to analyze the effect of the Schroth method on decreasing pain and Cobb’s angle in patients with idiopathic scoliosis.
This case study showed a decrease in pain and Cobb’s angle in all subjects after applying the Schroth method with emphasis on active holding. Previous studies have also reported significant decreases in pain and Cobb’s angle and increased quality of life8,9,10,11, 13). Thus, the Schroth method allows patients to regain normal posture of elongation, de-rotation, and de-flexion of the spine by continuous feedback of visual information8,9,10,11, 13). Therefore, the Schroth method decreases pain and Cobb’s angle by inhibiting compensation and restoring appearance.
However, this study included a small sample size. Therefore, further research may be needed with more subjects to verify the effect of applying the Schroth method to treat patients with idiopathic scoliosis.
Acknowledgments
This study was supported by Sahmyook University.
REFERENCES
- 1.Kane WJ: Scoliosis prevalence: a call for a statement of terms. Clin Orthop Relat Res, 1977, (126): 43–46. [PubMed] [Google Scholar]
- 2.Fusco C, Zaina F, Atanasio S, et al. : Physical exercises in the treatment of adolescent idiopathic scoliosis: an updated systematic review. Physiother Theory Pract, 2011, 27: 80–114. [DOI] [PubMed] [Google Scholar]
- 3.Negrini S, Atanasio S, Zaina F, et al. : Rehabilitation of adolescent idiopathic scoliosis: results of exercises and bracing from a series of clinical studies. Europa Medicophysica-SIMFER 2007 Award Winner. Eur J Phys Rehabil Med, 2008, 44: 169–176. [PubMed] [Google Scholar]
- 4.Steffan K: [Physical therapy for idiopathic scoliosis]. Orthopade, 2015, 44: 852–858. [DOI] [PubMed] [Google Scholar]
- 5.Borysov M, Borysov A: Scoliosis short-term rehabilitation (SSTR) according to ‘Best Practice’ standards-are the results repeatable? Scoliosis, 2012, 7: 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lenssinck ML, Frijlink AC, Berger MY, et al. : Effect of bracing and other conservative interventions in the treatment of idiopathic scoliosis in adolescents: a systematic review of clinical trials. Phys Ther, 2005, 85: 1329–1339. [PubMed] [Google Scholar]
- 7.Weiss HR: The method of Katharina Schroth—history, principles and current development. Scoliosis, 2011, 6: 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang JM, Lee JH, Lee DH: Effects of consecutive application of stretching, Schroth, and strengthening exercises on Cobb’s angle and the rib hump in an adult with idiopathic scoliosis. J Phys Ther Sci, 2015, 27: 2667–2669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kuru T, Yeldan İ, Dereli EE, et al. : The efficacy of three-dimensional Schroth exercises in adolescent idiopathic scoliosis: a randomised controlled clinical trial. Clin Rehabil, 2016, 30: 181–190. [DOI] [PubMed] [Google Scholar]
- 10.Rigo M, Quera-Salvá G, Villagrasa M, et al. : Scoliosis intensive out-patient rehabilitation based on Schroth method. Stud Health Technol Inform, 2008, 135: 208–227. [PubMed] [Google Scholar]
- 11.Otman S, Kose N, Yakut Y: The efficacy of Schroth s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey. Saudi Med J, 2005, 26: 1429–1435. [PubMed] [Google Scholar]
- 12.Schreiber S, Parent EC, Moez EK, et al. : The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis—an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner”. Scoliosis, 2015, 10: 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schreiber S, Parent EC, Hedden DM, et al. : Effect of Schroth exercises on curve characteristics and clinical outcomes in adolescent idiopathic scoliosis: protocol for a multicentre randomised controlled trial. J Physiother, 2014, 60: 234, discussion 234. [DOI] [PubMed] [Google Scholar]