

Abstract
To investigate the incidence and pattern of traumatic spinal fractures (TSFs) and associated spinal cord injury (SCI) resulting from motor vehicle collisions (MVCs).
This was a cross-sectional study. We retrospectively reviewed 698 patients with TSFs resulting from MVCs admitted to our university-affiliated hospitals from 2001 to 2011. The incidence and pattern were summarized with respect to different age groups, fracture levels, and the role of patients.
There were 464 males (66.5%) and 234 females (33.5%) aged 40.5 ± 13.8 years old. The most common roles of patients in MVCs were car drivers (189, 27.1%), pedestrians hurt by a car (155, 22.2%), and car passengers (145, 20.8%). The most common fracture levels were L1 (n = 198, 19.2%) and T12 (n = 116, 11.3%), followed by C2 (n = 86, 8.3%). A total of 298 (42.7%) patients suffered a spinal cord injury. The frequencies of SCIs decreased from 53.1% to 24.6% with increasing age. The patients in the 20 to 39 age group (45.3% of all patients) had the largest sex ratio (2.4) and highest frequency of complete SCIs (19.3%) and complications (3.2%). Motorcycle drivers had the youngest mean age (35.7 ± 10.2), largest sex ratio (10.4), and highest frequency of SCIs (56.0%) and complications (4.4%). Motorcycle passengers had the highest frequency of complete SCI (22.7%) and ASOIs (45.5%) and the largest mean injury severity scoring (ISS) (18.9 ± 9.6). The most common fracture levels of motorcycle drivers were C3–C7, while that of others were T11–L2.
The most common role of patients who sustained TSFs were car drivers who were 20 to 39 years old. Motorcycle drivers had the highest frequency of SCIs and complications. Motorcycle passengers had the highest frequency of complete SCIs and ASOIs and the largest ISS. Therefore, we should pay more attention to MVC patients, especially car drivers and motorcycle drivers and passengers.
Keywords: driver, MVCs, passenger, pedestrian, spinal cord injury, spine fracture
1. Introduction
Traumatic spine and spinal cord injuries are the most common cause of death among young people, and their influence on the social and financial well-being of the patient is often more significant than that of other injuries.[1–10] Motor vehicle collisions (MVCs) are a common cause of traumatic spinal fractures (TSFs), accounting for between 20.9% and 33.6% of all spinal fractures in different studies.[8–10] There were many studies about TSFs and especially MVCs, but they also had some limitations, such as single centre data,[11 12] a small numbers of cases,[13] and insufficient data to provide accurate information about clinical findings and crash characteristics.[14 15] MVCs can cause a diversity of injuries in pedestrians and vehicle drivers and passengers. Many factors affect the rate of spinal injuries, such as crash type,[16 17] vehicle type,[18] and age.[19 20] Data recently published by the National Spinal Cord Injury Statistical Centre showed that the most common cause of spinal cord injury (SCI) in the United States between 2010 and 2013 was MVCs (37.9%), followed by falls (29.9%).[21] Although much is known about SCIs, a comprehensive study of SCIs in MVCs is not available. To our knowledge, no previous studies have evaluated a database that provides comprehensive data on the incidence and pattern of TSFs resulting from MVCs in China especially regarding the characteristics of spinal fractures according to different roles/positions.
Delays in the diagnosis of spinal fractures and the associated spinal cord injury may result in significantly increased morbidity and mortality. They represent a major focus for traffic injury prevention. In the present study, we reviewed a multicentre (2 tertiary hospitals in Chongqing, China) database of motor vehicle accidents that happened over an 11-year period between 2001 and 2011. The incidence and pattern were summarized with respect to different age groups, fracture levels, and the role of patients.
2. Materials and methods
2.1. Study population
Our study included 698 patients who had acute TSFs that resulted from MVCs between January 2001 and May 2011 and who were admitted to our university-affiliated hospitals. Chongqing Municipality is a city located in southwest China. The data were collected from Third Military Medical University-affiliated hospitals that are the 2 biggest public tertiary hospitals located in the Shapingba district. The Shapingba district is a core district located in the northwest region of Chongqing. We made a definite diagnosis of upper cervical spinal fractures in all patients using X-rays, computed tomography (CT), and magnetic resonance imaging (MRI). The medical records were reviewed and assessed by 2 independent persons who had not participated in treating any patients. The ASIA scoring standard was used to assess spinal cord injury. The study protocol and this manuscript were approved by the committee on ethics and the institutional review board of our institution.
2.2. Statistical analysis
All statistical analyses were performed using SPSS 15.0 (SPSS, Inc., Chicago, IL). Continuous variables were compared between the 2 groups using the Student t test, whereas discrete variables were analyzed using the Chi-squared test. The measurement data among different groups were compared with a 1-way analysis of variance. The significance level was set at P < 0.05.
3. Results
3.1. Age and gender distribution
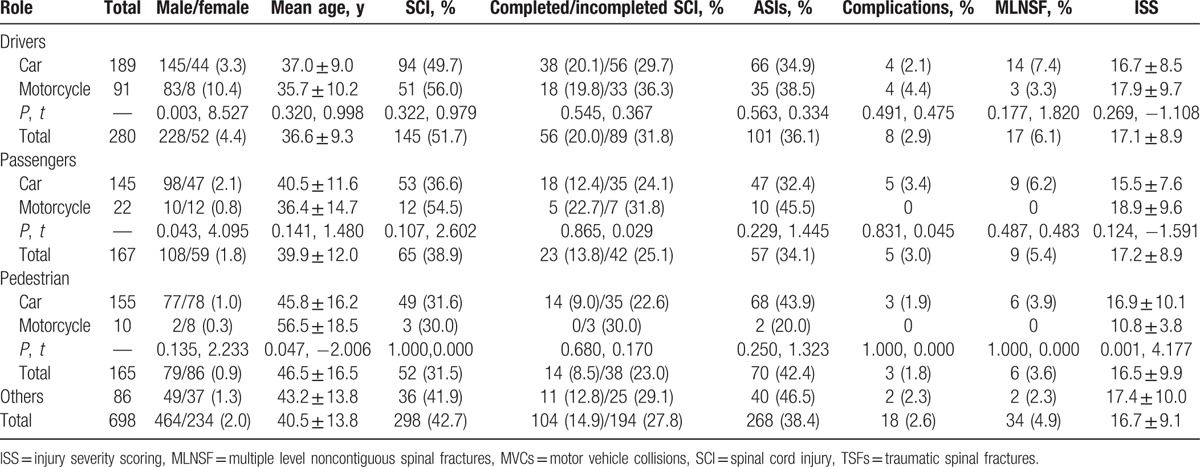
The study included 464 males and 234 female patients with a mean age of 40.5 ± 13.8 years old (range 4–88 years old) and a sex ratio of 2.0. The 20 to 39 years old age group accounted for the largest proportion of SCI (n = 316, 45.3%), followed by the 40 to 59 years old age group (n = 298, 41.4%). Significant differences were observed in the distribution of the sex ratio according to different age groups (P = 0.001, t = 16.504). Patients in the 20 to 39 age group had the largest sex ratio of 2.4. The patients in the ≥60 age group had the lowest sex ratio of 0.8 (Table 1, Fig. 1). The motorcycle driver patients had a larger sex ratio than the car driver patients (P = 0.003, t = 8.527), and the car passenger patients had a larger sex ratio than the motorcycle passenger patients (P = 0.043, t = 4.095). The pedestrians injured by a car had a younger mean age (P = 0.047, t = −2.006) and a larger injury severity scoring (ISS) (P = 0.001, t = 4.177) than the pedestrians hurt by a motorcycle (Table 2).
Table 1.
Characteristics of 698 TSFs resulting from MVCs according to different age range groups.

Figure 1.
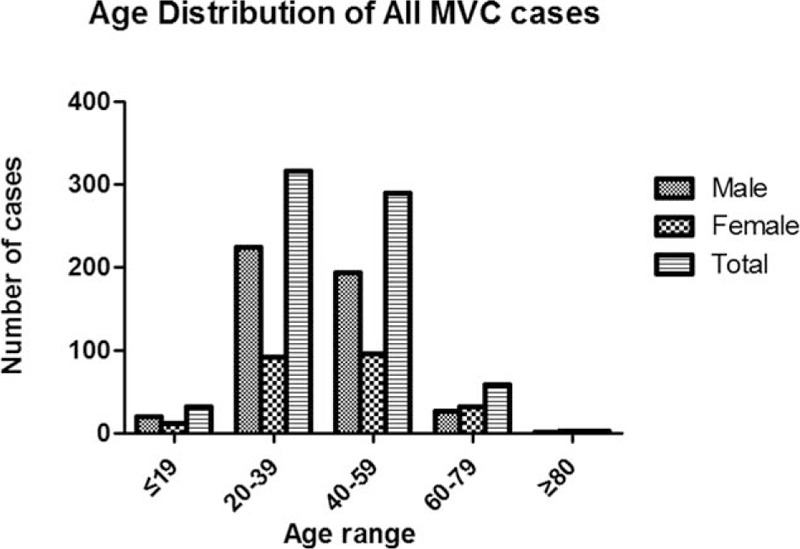
Age distribution of all 698 cases.
Table 2.
Characteristics of 698 TSFs resulting from MVCs according to different roles.
3.2. Roles/positions of patients in MVCs
The roles of patients in MVCs, their frequencies, sex ratio, and other characteristics are summarized in Table 2. The most common roles of patients in MVCs were car drivers (189, 27.1%), pedestrians hurt by a car (155, 22.2%), and car passengers (145, 20.8%) (Fig. 2). Motorcycle drivers had the younger mean age (35.7 ± 10.2), largest male-to-female sex ratio (10.4), and the highest frequency of SCI (56.0%) and complications (4.4%). Motorcycle passengers had the highest frequency of completed SCI (22.7%), ASOIs (45.5%), and the largest mean ISS (18.9 ± 9.6).
Figure 2.
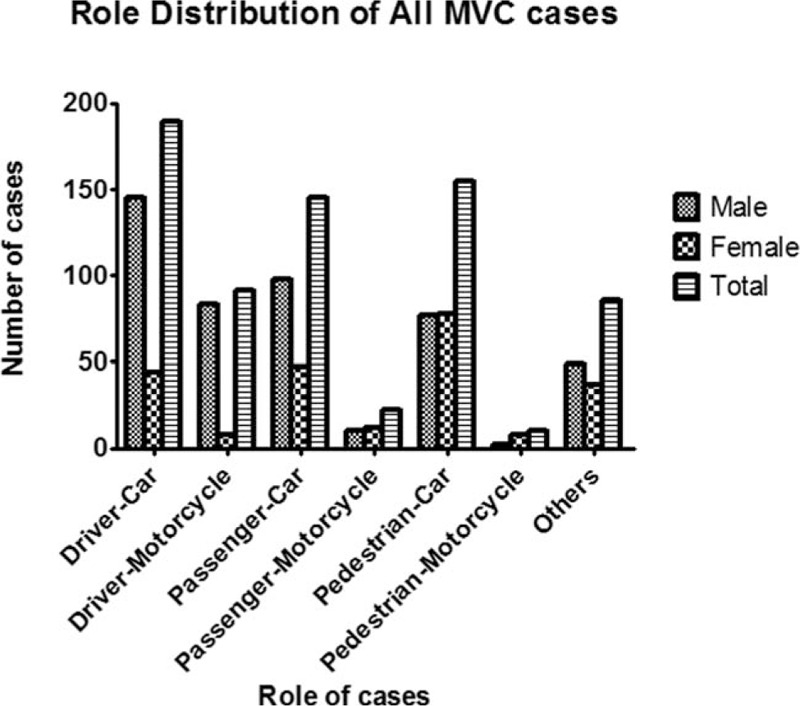
Role distribution of all 698 cases.
3.3. Anatomical distribution
The most common fracture level was L1 (n = 198, 19.2%) and T12 (n = 116, 11.3%), followed by C2 (n = 86, 8.3%). The most common fracture levels of motorcycle drivers were C3–C7, while that of others were T11–L2. The 2 most common fracture levels were T11–L2 (n = 114, 39.7%) and C3–C7 (n = 71, 24.7%) in car drivers, C3–C7 (n = 48, 33.8%) and T11–L2 (n = 30, 21.1%) in motorcycle drivers, and T11–L2 (n = 92, 43.0%) and C3–C7 (n = 50, 23.4%) in car passengers. The 2 most common fracture levels were T11–L2 (n = 12, 35.3%) and T1–T10 (n = 10, 29.4%) in motorcycle passengers and both T11–L2 (n = 8, 57.1%) and T1–T10 (n = 3, 21.4%) in pedestrians who were hurt by motorcycles. The 2 most common fracture levels were T11–L2 (n = 121, 57.6%) and L3–L5 (n = 34, 16.2%) in pedestrians who were hurt by a car (Table 3, Fig. 3).
Table 3.
Fracture level distribution of 698 TSFs resulting from MVCs according to different roles.
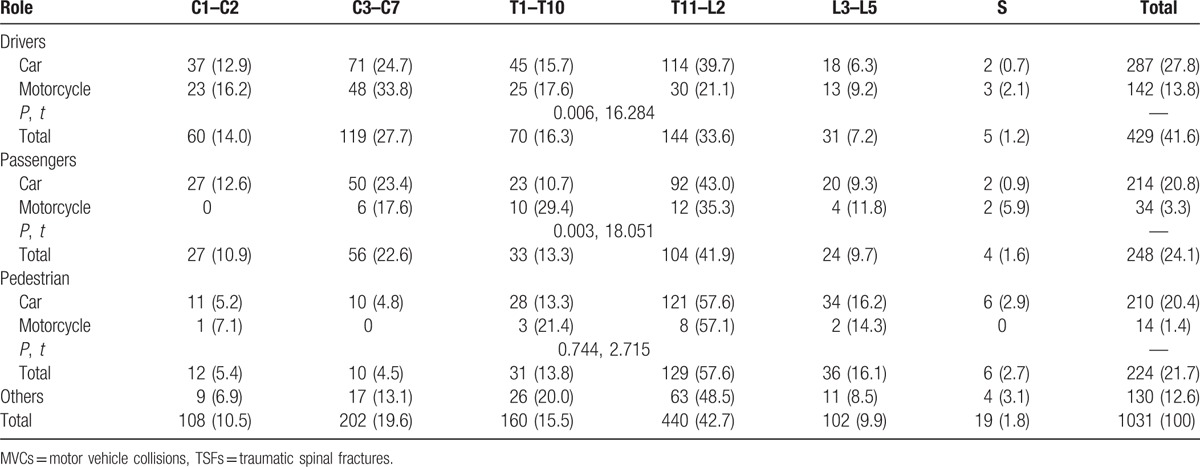
Figure 3.
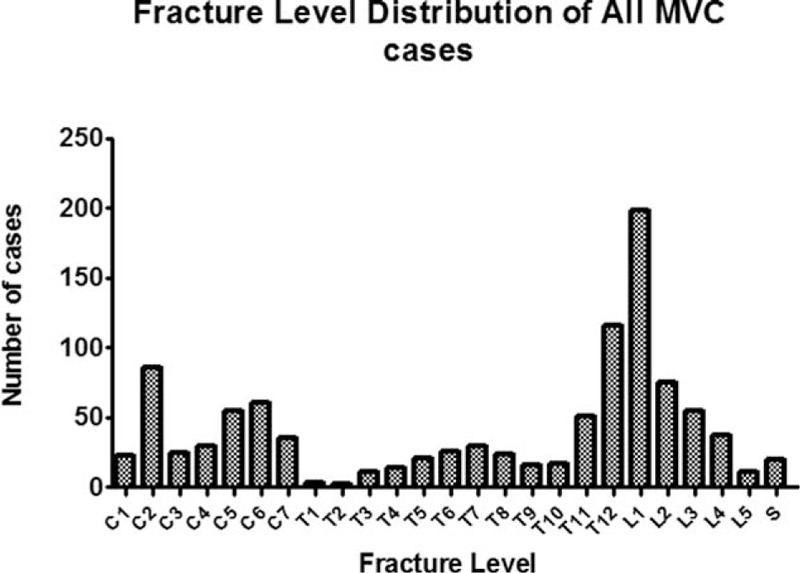
Fracture level distribution of all 698 cases.
3.4. Neurological status, associated injuries, complications, and MLNSF
A total of 298 (42.7%) patients suffered a spinal cord injury. Two hundred sixty-eight patients (38.4%) sustained a total of 353 associated injuries (ASOIs), including a thoracic injury in 119 (44.4%) patients, a head and neck injury in 67 (25.0%) patients, an abdomen injury in 5 (1.9%) patients, a pelvic injury in 23 (8.6%) patients, a fracture of an upper extremity in 37 (13.8%) patients, and a fracture of a lower extremity in 42 (15.7%) patients. Eighteen patients sustained a total of 21 complications, such as a pulmonary infection in 11 patients, a bedsore in 6 patients, a deep venous thrombosis in 3 patients, and a postoperative infection in 1 patient. Thirty-four patients (n = 34, 4.9%) presented with MLNSF (multiple level noncontiguous spinal fractures).
Significant differences were observed in the frequencies of SCI according to different age groups (P = 0.004, t = 13.310). The frequencies of SCI decreased from 53.1% to 24.6% with increasing age. The patients in the 20 to 39 age group had the highest frequency of complete SCI (19.3%) and complications (3.2%). The patients in the ≤19-year-old age group presented with the highest frequency of SCI (53.1%) and the highest ISS (17.5 ± 8.7). The patients in the 40 to 59 age group presented with the highest frequency of ASOIs (41.5%) and MLNSF (6.6%). The patients in the ≥60 age group had the lowest frequency of SCI (24.6%), complications (0), and the lowest of ISS (13.5 ± 6.0).
4. Discussion
In the present study, the most common roles of patients in MVCs were car drivers, pedestrians hurt by a car and car passengers. There were 464 males and 234 female patients with a sex ratio of 2.0 in the study. The results can be explained by the fact that males, such as car or motorcycle drivers, are more involved in daily activities. The 20- to 39-year-old age group accounted for the largest proportion and had the largest male-to-female sex. The most common fracture levels were T11–L2 in car drivers, car passengers, motorcycle passengers, and pedestrians hurt by a motorcycle and car, but C3–C7 in motorcycle drivers. Previous studies have shown that patients in different subgroups of traffic accidents had a diverse distribution of injury subtypes and that the results are directly related to the population studied and the local traffic situation, including transportation devices and traffic regulations. Hill et al[22] reported that advanced life support measures are appropriate at the scene to stabilize the airway and to protect the entire spine of pedestrians with multiple injuries because of the high frequency of brain and vertebral trauma. Thus, we should pay more attention to the prevention and treatment of SCIs in MVCs involving cars among those between 20 and 39 years old, especially C3–C7 fractures in motorcycle drivers and T11–L2 fractures in patients involved with other type of MVCs.
In our study population, the frequencies of spinal cord injury and ASOIs were 42.7% and 38.4%, respectively. The frequencies of SCI decreased from 53.1% to 24.6% with increasing age. The patients in the 20 to 39 age group had the highest frequency of complete SCIs (19.3%). The patients in the ≤19 age group presented with the highest frequency of SCIs (53.1%) and the largest ISS. Thus, we should pay more attention to young patients, especially regarding spinal cord injury. The most frequent ASOIs were thoracic injury, followed by head and neck injuries. We should pay more attention to patients who had thoracic vertebral fractures to minimize further complications and mortality.[23] Car occupants had fewer extremity injuries due to the protective nature of the car cage.[24] In previous studies, it has been shown that pedestrians are prone to head injuries due to multiple impacts.[25 26] However, in our study, motorcycle drivers had the youngest mean age, largest male-to-female sex ratio, and the highest frequencies of SCIs and complications. Motorcycle passengers had the highest frequency of complete SCIs and ASOIs and the largest mean ISS. In many developing urban cities, the increasing rate of MVCs results from economic growth and increasing use of motor vehicles. In Chongqing, which is a mountainous city, the use of motor vehicles is rapidly increasing. Because of a lack of strict traffic safety regulations in China, the probability of sustaining a serious trauma in a vehicle collision is high. We should pay more attention to these injuries and inform younger patients of these injuries, especially those resulting from MVCs involving motorcycles to prevent nerve injuries, respiratory dysfunctions, or death. As is the case in many other countries undergoing similar development, traffic safety regulations need to be adopted.[27 28]
Eighteen patients (2.6%) sustained complications, such as a pulmonary infection in 11 patients, a bedsore in 6 patients, a deep venous thrombosis in 3 patients, and a postoperative infection in 1 patient; therefore, we should pay more attention to pulmonary infections and bedsores, which were the 2 most common complications. We should pay more attention to pulmonary infections, bedsores, and deep venous thromboses especially among patients aged 40 to 59 years old. Thirty-four patients had MLNSF. The patients in the 40 to 59 age group had the highest frequency of MLNSF. Car drivers and car passengers had a greater frequency of MLNSF than did motorcycle occupants. Previous studies noted that MVCs were the primary cause of multiple noncontiguous spine fractures. The failure to use seat belts and ejection from the vehicle were the main factors associated with multiple noncontiguous spine injuries.[29] Multiple noncontiguous injuries had a more complicated mechanism of injury and tended to be more severe injuries than single-level injuries as they were combined more frequently with injuries of other parts of the body.[30 31] Multilevel spine injuries are most common in children between 9 and 16 years of age and are mainly located in the cervical region.[32] Although multiple level noncontiguous fractures of the spine are uncommon, they constitute a threat to neurologic function and therefore warrant radiographic evaluation of the entire spine with multiple injuries.[33] Imaging studies that evaluate patients with spinal injuries should include at least three levels above and below the primary level of injury in addition to the entire thoracic spine and thoracolumbar junction.[34] We should pay more attention to car drivers and passengers, especially if MLNSF are found among them to avoid a missed diagnosis. This study has several limitations. First, it was limited by the retrospective study design and the small number of patients. Second, there may be selection bias because this study includes patients referred to our teaching hospitals.
Footnotes
Abbreviations: ASOIs = associated injuries, CT = computed tomography, ISS = injury severity scoring, MRI = magnetic resonance imaging, MVCs = motor vehicle collisions, TSCI = traumatic spinal cord injury, TSFs = traumatic spinal fractures.
Funding: This work was supported by the Foundation of the State Key Laboratory of Robotics (2014-O12), the Medjaden Academy & Research Foundation for Young Scientists (MJR20150013), and the Liaoning Province Doctor Startup Fund (201601389).
HW and XL contributed equally to this work.
The authors have no conflicts of interest to disclose.
References
- 1. Pickett GE, Campos-Benitez M, Keller JL, et al. Epidemiology of traumatic spinal cord injury in Canada. Spine (Phila Pa 1976) 2006; 31:799–805. [DOI] [PubMed] [Google Scholar]
- 2. Kattail D, Furlan JC, Fehlings MG. Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma 2009; 67:936–943. [DOI] [PubMed] [Google Scholar]
- 3. Jansson KA, Blomqvist P, Svedmark P, et al. Thoracolumbar vertebral fractures in Sweden: an analysis of 13,496 patients admitted to hospital. Eur J Epidemiol 2010; 25:431–437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lieutaud T, Ndiaye A, Frost F. A 10-year population survey of spinal trauma and spinal cord injuries after road accidents in the Rhone area. J Neurotrauma 2010; 27:1101–1107. [DOI] [PubMed] [Google Scholar]
- 5. Ning GZ, Yu TQ, Feng SQ, et al. Epidemiology of traumatic spinal cord injury in Tianjin, China. Spinal Cord 2011; 49:386–390. [DOI] [PubMed] [Google Scholar]
- 6. Frost M, Wraae K, Abrahamsen B, et al. Osteoporosis and vertebral fractures in men aged 60–74 years. Age Ageing 2012; 41:171–177. [DOI] [PubMed] [Google Scholar]
- 7. Robertson A, Giannoudis PV, Branfoot T, et al. Spinal injuries in motorcycle crashes: patterns and outcomes. J Trauma 2002; 53:5–8. [DOI] [PubMed] [Google Scholar]
- 8. Leucht P, Fischer K, Muhr G, et al. Epidemiology of traumatic spine fractures. Injury 2009; 40:166–172. [DOI] [PubMed] [Google Scholar]
- 9. Wang H, Zhang Y, Xiang Q, et al. Epidemiology of traumatic spinal fractures: experience from medical university-affiliated hospitals in Chongqing, China, 2001–2010. J Neurosurg Spine 2012; 17:459–468. [DOI] [PubMed] [Google Scholar]
- 10. Liu P, Yao Y, Liu MY, et al. Spinal trauma in mainland China from 2001 to 2007: an epidemiological study based on a nationwide database. Spine (Phila Pa 1976) 2012; 37:1310–1315. [DOI] [PubMed] [Google Scholar]
- 11. Inamasu J, Guiot BH. Thoracolumbar junction injuries after motor vehicle collision: are there differences in restrained and nonrestrained front seat occupants? J Neurosurg Spine 2007; 7:311–314. [DOI] [PubMed] [Google Scholar]
- 12. Ball ST, Vaccaro AR, Albert TJ, et al. Injuries of the thoracolumbar spine associated with restraint use in head-on motor vehicle accidents. J Spinal Disord 2000; 13:297–304. [DOI] [PubMed] [Google Scholar]
- 13. Miniaci A, McLaren AC. Anterolateral compression fracture of thoracolumbar spine. A seat belt injury. Clin Orthop Relat Res 1989; 240:153–156. [PubMed] [Google Scholar]
- 14. Huelke DF, Mackay GM, Morris A. Vertebral column injuries and lap-shoulder belts. J Trauma 1995; 38:547–556. [DOI] [PubMed] [Google Scholar]
- 15. Wang MC, Pintar F, Yoganandan N, et al. The continued burden of spine fractures after motor vehicle crashes. J Neurosurg Spine 2009; 10:86–92. [DOI] [PubMed] [Google Scholar]
- 16. Bambach MR, Grzebieta RH, McIntosh AS, et al. Cervical and thoracic spine injury from interactions with vehicle roofs in pure rollover crashes. Accid Anal Prev 2013; 50:34–43. [DOI] [PubMed] [Google Scholar]
- 17. Funk JR, Cormier JM, Manoogian SJ. Comparison of risk factors for cervical spine, head, serious, and fatal injury in rollover crashes. Accid Anal Prev 2012; 45:67–74. [DOI] [PubMed] [Google Scholar]
- 18. O’Connor PJ, Brown D. Relative risk of spinal cord injury in road crashes involving seriously injured occupants of light passenger vehicles. Accid Anal Prev 2006; 38:1081–1086. [DOI] [PubMed] [Google Scholar]
- 19. Bilston LE, Clarke EC, Brown J. Spinal injury in car crashes: crash factors and the effects of occupant age. Inj Prev 2011; 17:228–232. [DOI] [PubMed] [Google Scholar]
- 20. Stein DM, Kufera JA, Ho SM, et al. Occupant and crash characteristics for case occupants with cervical spine injuries sustained in motor vehicle collisions. J Trauma 2011; 70:299–309. [DOI] [PubMed] [Google Scholar]
- 21. National Spinal Cord Injury Statistical Center: 2013 Annual Statistical Report for the Spinal Cord Injury Model Systems. Birmingham, AL: University of Alabama at Birmingham; 2013. [Google Scholar]
- 22. Hill DA, Delaney LM, Duflou J. A population-based study of outcome after injury to car occupants and to pedestrians. J Trauma 1996; 40:351–355. [DOI] [PubMed] [Google Scholar]
- 23. Wang H, Zhou Y, Ou L, et al. Traumatic vertebral fractures and concomitant fractures of the rib in Southwest China, 2001 to 2010: an observational study. Medicine (Baltimore) 2015; 94:e1985. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Price C, Makintubee S, Herndon W, et al. Epidemiology of traumatic spinal cord injury and acute hospitalization and rehabilitation charges for spinal cord injuries in Oklahoma, 1988–1990. Am J Epidemiol 1944; 139:37–47. [DOI] [PubMed] [Google Scholar]
- 25. Lane PL, McClafferty KJ, Nowak ES. Pedestrians in real world collisions. J Trauma 1994; 36:231–236. [DOI] [PubMed] [Google Scholar]
- 26. Vives MJ, Kishan S, Asghar J, et al. Spinal injuries in pedestrians struck by motor vehicles. J Spinal Disord Tech 2008; 21:281–287. [DOI] [PubMed] [Google Scholar]
- 27. Wang Y, Hasselberg M, Wu Z, et al. Distribution and characteristics of road traffic crashes in the Chaoyang District of Beijing, China. Accid Anal Prev 2008; 40:334–340. [DOI] [PubMed] [Google Scholar]
- 28. Zhang W, Tsimhoni O, Sivak M, et al. Road safety in China: analysis of current challenges. J Safety Res 2010; 41:25–30. [DOI] [PubMed] [Google Scholar]
- 29. Henderson RL, Reid DC, Saboe LA. Multiple noncontiguous spine fractures. Spine (Phila Pa 1976) 1991; 16:128–131. [PubMed] [Google Scholar]
- 30. Dai LY, Jia LS. Multiple non-contiguous injuries of the spine. Injury 1996; 27:573–575. [DOI] [PubMed] [Google Scholar]
- 31. Wittenberg RH, Hargus S, Steffen R, et al. Noncontiguous unstable spine fractures. Spine (Phila Pa 1976) 2002; 27:254–257. [DOI] [PubMed] [Google Scholar]
- 32. Mortazavi MM, Dogan S, Civelek E, et al. Pediatric multilevel spine injuries: an institutional experience. Childs Nerv Syst 2011; 27:1095–1100. [DOI] [PubMed] [Google Scholar]
- 33. Korres DS, Boscainos PJ, Papagelopoulos PJ, et al. Multiple level noncontiguous fractures of the spine. Clin Orthop Relat Res 2003; 411:95–102. [DOI] [PubMed] [Google Scholar]
- 34. Mahan ST, Mooney DP, Karlin LI, et al. Multiple level injuries in pediatric spinal trauma. J Trauma 2009; 67:537–542. [DOI] [PubMed] [Google Scholar]