

Abstract
Objectives:
Loss of foot sensitivity is a relevant parameter to assess and prevent in several diseases. It is crucial to determine the vibro-tactile sensitivity threshold response to acute conditions to explore innovative monitor tools and interventions to prevent and treat this challenge. The aims were: 1) to analyze the acute effects of a single whole body vibration session (4min-18Hz-4mm) on vibro-tactile perception threshold in healthy young adults. 2) to analyze the 48 hours effects of 3 whole body vibration sessions on vibro-tactile perception threshold in healthy young adults.
Methods:
A randomized controlled clinical trial over 3 sessions of whole body vibration intervention or 3 sessions of placebo intervention. Twenty-eight healthy young adults were included: 11 experimental group and 12 placebo group. The experimental group performed 3 sessions of WBV while the placebo group performed 3 sessions of placebo intervention.
Results:
The vibro-tactile threshold increased right after a single WBV session in comparison with placebo. Nevertheless, after 3 whole body vibration sessions and 48 hours, the threshold decreased to values lower than the initial.
Conclusions:
The acute response of the vibro-tactile threshold to one whole body vibration session increased, but the 48 hours short-term response of this threshold decreased in healthy young adults.
Keywords: Whole Body Vibration, Vibro-tactile Perception Threshold, Healthy People, Acute Effects, Short-term Effects
Introduction
Whole Body Vibration (WBV) is a forced oscillation, where energy is transferred from an actuator (the vibration device) to the body on it[1]. The WBV has the ability to induce sudden deformations of some elements of the muscle-skeletal system. These deformations cause a reflex muscle contraction what has been called tonic vibration reflex[2,3]. The tonic vibration reflex is a response of Peripheral Nervous System, consisting of a muscle contraction that occurs when the muscle spindle is elongated rapidly and repeatedly[4,5]. Following the detection of vibrations by the muscle spindles, more nervous discharge of these structures[6] occurs and this produces and increase of the potential transmitted to the muscles engines vibrated[7].
Previous studies demonstrated that every type of mechanoreceptor reply of better to a type of interval of vibration. These studies determinated that cospuscles that reply at high vibration intervals are those of Ruffini and Pacini. The Ruffini corpuscles have an interval of frequency from 15 to 400 Hz and the Pacini corpuscles go from 10 to 500 Hz, being a very rapid vibration in top intervals[8,9].
The vibration training (VT) might be used in specific neurological disturbances[10-12]. The effects of VT could be acute and/or chronic. Acute effects refer to the effects obtained immediately after undergoing a session vibration. Chronic effects refer to the effects obtained after undergoing several sessions of vibration. They will depend on the vibration characteristics (method of application, frequency and amplitude) and exercise protocols (type training intensity and volume) used[13].
Several studies have evaluated the acute effects of a single WBV session on Vibro-tactile Perception Threshold (VPT) showing[14,15]. Even one of these studies concludes that the sinusoidal vibration used during WBV training is not an adequate strategy to stimulate/improve vibration sensitivity”[14]. On the other hand, the unique previous study found evaluating the longitudinal effects of 12 weeks of VT showed a decrease of VPT in patients with low back pain[15]. VPT has been previously used as part of neuropathy screening[1] To know the effect of WBV in VPT could be important especially for patients with increased risk of neuropathy, such as diabetic patients.
The main objective is to describe and compare the acute effects of short-term intensive protocol VT on the threshold of sensitivity to vibration. For this purpose the following hypothesis are proposed:
Hypothesis 1: 1. The VPT is increased immediately after applying a WBV session.
Hypothesis 2: The VPT decreases after 48 hours application of WBV program of two sessions duration.
Material and methods
Trial design
Single center and single-blinded controlled randomized controlled trial. Allocation ratio was 1:1.
Participants
Eligibility criteria for participants were: 1) to be young adult (18 to 40), 2) healthy, 3) to be physically active (3 or more hours of the physical activity by week) and 4) not be under medication.
Twenty-eight people (4 women and 24 men) showed interest to participate in the study and signed the informed consent. There were 5 drop-out (3 in the WBV group and 2 in the placebo group). This is in Figure 1 (Flow diagram).
Figure 1.
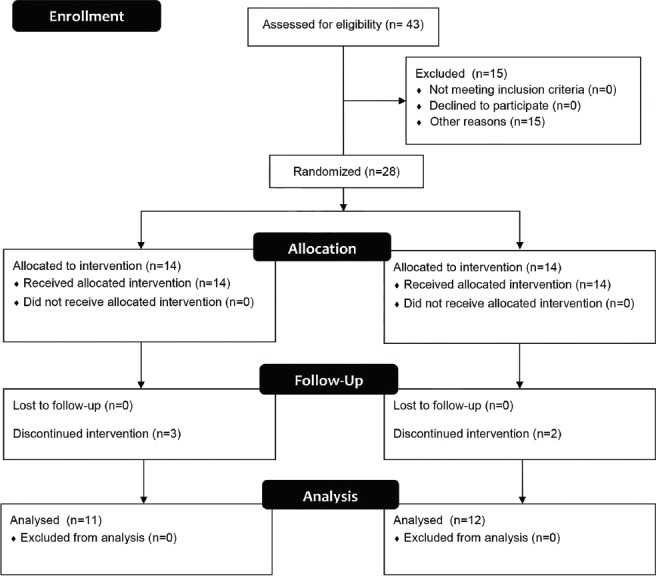
Flow diagram of participants.
Interventions
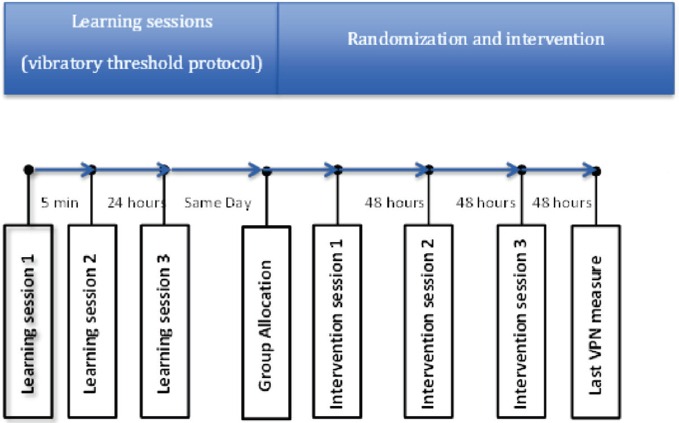
Participants performed 3 learning sessions of VPT test before to receive the interventions (WBV or placebo). Two learning sessions were performed in the same day (intra-session), between first and second session passed 5 minutes and the third session (inter-session) was performed at 24 hours. This data was used to calculate the reliability indices. There were two groups, WBV group and placebo group:
WBV group: this group performed 3 WBV sessions with the reciprocating Galileo 900 Platform (Novotec Medical GmbH, Pforzheim, Germany). VPT was evaluated with biothensiometer vibraton II before and after of each WBV session and 48 hours after the last WBV session. Between each WBV session there was a rest period of 48 hours. Experienced trainers administrated every WBV sessions. Sessions consisted in the application of four minutes of uninterrupted exposure of vibratory stimuli (frequency= 18 Hz, amplitude= 4 mm; knee flexion= 90º). Trainers gave the next instructions to participants: 1) right and left feet placed to 4 mm above the surface of the device, 2) Keep the back and head straight, 3) Bend knees at 90º and keep that posture during the trial knee angle and 4) up the surface of the platform without shoes.
Placebo group: this group performed 3 placebo sessions with specific software performed in this study connected to Galileo Fitness Platform. VPT was evaluated before and after of each placebo session and 48 hours after the last placebo session. Between each placebo session there was a rest period of 48 hours. Placebo consisted in simulated intervention based on real vibratory device implemented with hidden speaker controlled by the software. This placebo intervention was similar that another study[16]. Trainer showed to participants how to the software allowed to change amplitude, frequency and time of vibratory stimuli (In fact, amplitude changes performed by user elicited proportional changes in the speakers volume, creating an apparent sensation that session was a real intervention based on vibratory stimuli under-threshold). Vibration and trainer said to participants that they were exposed to vibratory stimuli with amplitude under the previously determined threshold; hence they should to sense nothing. The instructions that trainers gave the participants were the follow: 1) right and left feet placed to 4 mm above the surface of the WBV platform, 2) Keep the back and head straight, 3) Bend the knees and maintain a 45-degree knee angle and 4) up the surface of the platform without shoes.
Outcomes
Primary measures
Vibro-tactile Perception Threshold
Vibraton II (Sensortek, Inc. Clifton, NJ, EE. UU.)
The measured VPT was made from vibraton II device. The device is composed of two parts. The first is the vibration device driver which is located the power supply, four switches. whose functions are to connect the device, set the measurement range switch signal between modules A and B, and ‘false’ (equals the switch that toggles the signal, but it does change in the apparatus, with the function to do with the person being evaluated does not associate with the movement of the switch module that is vibrating) and a screen where the amplitude of vibration is displayed. The second part is composed of two box-shaped modules, with the dimensions of 23.5 × 12.5 × 8.5 (in centimeters), with a vibrating pole (cylinder with a 1,5 cm of diameter and 9,5 cm of height) on top of each module. These poles vibrate at a frequency of 120 Hz. The vibration amplitude is the controlled parameter in the determination protocol of the VPT. The evaluation procedure was the protocol called ‘Forced Two alternative choice procedure’, one of the given by the instrument manufacturer. It was requested to participants to place the fingertips of each big toe on the poles. The measurement starts when the subject expresses to feel the vibration in one of the modules, previously set by the researcher, yielding alternating sequence in accordance with the manual commands for the researcher. These commands are a random switching between ‘A’ and ‘B’. The vibration amplitude will be reduced progressively every time the participant gives a right anwser and increased when make an error. The assessment finishes when participant reaches 5 errors or is not able to tell which module is vibrating. The manufacturer suggests that the increases or decreases in the vibration amplitude should be done between a 5-10% in vibration unit. VPT is estimated using the amplitude values of the last 5 right answers and the 5 errors, omitting the extreme values (the lower and higher respectively). The average of the remaining 8 values[17] is determined as VPT. Randomization of the modules, the amplitudes of vibration, registration information and the average of the values were provided by script made for the study running in a Microsoft Excel program.
The reliability of the employed protocol has been previously summarized by other studies that concluded that the derived measures could be used to determine the VPT and its usefulness for neuropathy assessment[2,3].
Secondary measures
A portable stadiometer with 210 cm maximum capacity and a 0.1 cm precision (SECA 225, SECA, Hamburg, Germany) was used to measure height.
A portable bioelectrical impedance analyzer TANITA BC 418-MA (Tanita Corp., Tokyo, Japan) with a 200 kg maximum capacity and a ±100 g error margin was used to measure the weight, height, fat-free mass, fat mass, body water, fat percentage and body mass index. Individuals removed shoes and heavy cloths prior to weighing.
Sample size
The study sample size was determined using recommendations given in[18]. In order to find an effect size of 0.5 units of difference time-averaged as the found it by[19], with a 95% of confidence interval the sample size to obtain a statistical power of .95 was determined up to 19 participants per group. Finally, 12 and 11 participants were included into the analysis for WBV group and Placebo group respectively (see participants flow). That final sample implied a statistical power of 0.8.
Randomization
Participants were allocated into the experiment groups using Random Sorting algorithm (sort participants in a list after assign them a random number and estimating the median as cut-off point to allocate them into groups).
Timeline
This is the timeline of the study (Figure 2).
Figure 2.
Statistical analysis
Statistical methods performed for the present work included an exploratory analysis in order to describe the most important characteristics of participants and to contrast parametric assumptions. Means and standard deviations were calculated for each group before and immediately after every intervention session. Normality and errors’ homoscedasticity were also checked.
Repeated measures ANOVA model was adjusted including a six level intragroup factor and two level intergroup factor. Finally, polynomial and post hoc contrasts were estimated in order to analyze means differences and trends. Bonferroni adjustment was applied to control type I error propagation for post hoc contrasts. Statistical methods were conducted with 19 version of SPSS statistical package. Significance level was previously set at p<.05.
Results
The numbers of participants who were randomly assigned were 14 per group, in total 28. All received treatment but was 3 losses in vibration group and 2 losses in placebo group. The cause of leaves was loss of interest in all of the cases. Finally, 23 subjects participated in this study.
[Table 1] shows that the two groups not differed significantly in Weight, Height, Fat-Free Mass, Fat Mass, Body Water, Fat Percentage, Body Mass Index and Vibration Threshold.
Table 1.
Sociodemographic characteristics of healthy young adults.
| Intervention (Mean (SD)) | Placebo (Mean (SD)) | All (Mean (SD)) | p | |
|---|---|---|---|---|
| Height (m) | 1.72±0.06 | 1.74±0.04 | 1.73 ±0.06 | .424 |
| Weight (kg) | 69.75±8.16 | 73.25±9.36 | 71.50±8.80 | .301 |
| Fat-Free Mass (%) | 83.95±4.33 | 85.95±7.01 | 84.95±5.81 | .374 |
| Fat Mass (%) | 16.05±4.33 | 14.09±6.99 | 15.07±5.79 | .380 |
| Body Water (%) | 61.59±3.23 | 62.92±5.13 | 62.26±4.26 | .418 |
| Fat Percentage (%) | 16.26±4.95 | 14.07±6.99 | 15.17±6.04 | .349 |
| Body Mass Index (Kg/m2) | 23.43±1.95 | 24.14±3.22 | 23.78±2.64 | .489 |
| Vibration Threshold (vu) | 1.26±0.41 | 1.28±0.69 | 1.27±0.56 | .914 |
[Table 2] shows the VPT results of acute effects of VT. In this table shows ANOVA for VPT and the estimated effect size. The three measurements had difference as per statistics significant.
Table 2.
Acute effects of Vibratory Training.
| Outcome measure | Baseline | Acute effect | ł | Treatment effectc mean (95%CI) | ||
|---|---|---|---|---|---|---|
| WBVGa (n= 12) mean (SD) | PGb (n=11) mean (SD) | WBVGa (n= 12) mean (SD) | PGb (n=11) mean (SD) | |||
| VPTd 1 (vu) | 1.24 (0.44) | 1.37 (0.72) | 2.22 (0.53) | 1.4 (0.61) | <0.01 | 0.95 (-0.04-1.94) |
| VPTd 2 (vu) | 1.32 (0.47) | 1.24 (0.64) | 2.27 (1.06) | 1.36 (0.53) | <0.01 | 0.83 (-0.35-2.01) |
| VPTd 3 (vu) | 0.97 (0.37) | 1.36 (0.62) | 1.92 (0.63) | 1.29 (0.65) | <0.01 | 1.02 (0.04-2) |
WBVG: Whole Body Vibration Group.
PG: Placebo Group.
Treatment affect was compute as difference of mean differences.
VPT (Vibro-tactile Perception Threshold) 1 to 3 expresses acute effects or intrasession effects in 3 non-consecutives days. ł Statistical Significance.
[Table 3] shows the VPT results of short-term effect of VT. In this table shows ANOVA for VPT and the estimated effect size. The Statistical Significance was .08.
Table 3.
Short effects of Vibratory Training.
| Outcome measure | Baseline | Acute effect | ł | Treatment effectc mean (95%CI) | ||
|---|---|---|---|---|---|---|
| WBVGa (n=12) mean (SD) | PGb (n=11) mean (SD) | WBVGa (n= 12) mean (SD) | PGb (n=11) mean (SD) | |||
| VPTd 4 (vu) | 1.24 (0.44) | 1.37 (0.72) | 0.97 (0.37) | 1.36 (0.62) | 0.08 | -0.26 (-1.2-0.68) |
WBVG: Whole Body Vibration Group.
PG: Placebo Group.
Treatment affect was compute as difference of mean differences.
VPT (Vibro-tactile Perception Threshold) 1 to 3 expresses acute effects or intrasession effects in 3 non-consecutives days. ł Statistical Significance. VPT 4 expressed one-week effect. Effect size associated to time effect was 0.77 explained variance computed with partial eta squared.
Discussion
The main findings of this study are that there is a relevant immediately following acute effect of increasing VPT sessions VT compared to Placebo group. Regarding the longitudinal effects, it is observed that there is a slight improvement of VPT after four VT sessions in WBV group participants regarding Placebo group participants.
With regard to the acute effect observed in the three sessions, it is important to say that this was not only statistically significant, but its magnitude was approximately four times the minimum detectable change estimated in the first phase of the study. This effect has already been reported by other studies[14], however this is the first study in which a design with control group subjected to a placebo intervention applies. The study concludes that the WBV based training could be negative for VPT in healthy subjects because the threshold worsened significantly after 4 minutes of VT with a frequency of 27 Hz and amplitude of 2 mm. However, this conclusion is based solely on immediate results from exposure to vibration and not in the short-term effect, according to the principles of training if the training load is sufficient to cause adaptations involves a loss of fair return after training due to fatigue. In that study no measurements are performed on consecutive days, so they cannot know whether that training would lead to an improvement in the short or medium term. This immediate effect could be partly due to the overstimulation of receptors.
The second findings were short-term effects, a slight improvement effect on the threshold after 2 VT sessions. A previous study of our laboratory using similar VT’s dose during 36 sessions in persons with low back pain reported bigger and significant effects on the threshold[15]. Therefore, it is warranted to apply and multimodal assesses longer interventions using the features of the current VT to improve VPT.
Overall, the evolution of VPT cubes showed a decreasing trend in the WBV group with respect to Placebo group, suggesting that this parameter could behave according to the principles of training derived from the Theory of General Adaptation Syndrome described by Selye[20].
Study limitations
The VPT is an important clinical parameter in some health problems such as neuropathies; therefore the clinical implications of the results found in this study directly are minimal given the characteristics of the participants, since all began the study with values of sensitivity to vibration considered normal and ended within those limits. However, note that to find such a clear effect in young healthy suggests that the effectiveness of the WBV in people with impaired sensitivity could be even higher but this test requires another specific design different the current study. Moreover, the present study design does not allow to isolate the potential effects on vibro-tactile perception from other well-known effects attributable to WBV. Future studies should include additional groups where participants will be exposed to vibratory stimuli avoiding WBV, for instance in a seated position in front of the vibratory devices. Finally, the 3 sessions programs was short in physically active healthy participants, but the effects on specific-disease populations with neuropathy or longer programs remains unknown requiring further specific research.
Prospects
Sensitivity limitations associated with certain health conditions such as diabetic neuropathy has been identified as a risk factor in the development of serious complications of the disease such as diabetic foot ulcers some[21]. In this sense, whether similar effects to found in this study were applicable to patients with those characteristics, VT could help in prevention of diabetic foot, especially through the improvement of the self-protection mechanism that makes patients aware of their own feet’ injuries.
Therefore, we can conclude that the VPT increases an average of four times the minimum detectable change immediately after exposure to intensive training session WBV and the basal VPT decreases after exposure to three intensive training sessions vibratory warranting new research and applications to other dose-response and populations.
Acknowledgement
Thanks all participants in the study.
Footnotes
Edited by: J. Rittweger
References
- 1.Rittweger J. Vibration as an exercise modality: how it may work, and what its potential might be. European journal of applied physiology. 2010;108(5):877–904. doi: 10.1007/s00421-009-1303-3. [DOI] [PubMed] [Google Scholar]
- 2.Eklund G, Hagbarth K. Motor effects of vibratory muscle stimuli in man. Electroencephalogr Clin Neurophysiol. 1965;19:619. [Google Scholar]
- 3.Eklund G, Hagbarth K-E. Normal variability of tonic vibration reflexes in man. Experimental neurology. 1966;16(1):80–92. doi: 10.1016/0014-4886(66)90088-4. [DOI] [PubMed] [Google Scholar]
- 4.Roll J, Gilhodes J, Tardy-Gervet M. Effets perceptifs et moteurs des vibrations musculaires chez l’homme normal: mise en évidence d’une réponse des muscles antagonistes. Arch Ital Biol. 1980;118(1):51–71. [PubMed] [Google Scholar]
- 5.Romaiguere P, Vedel J-P, Azulay J, Pagni S. Differential activation of motor units in the wrist extensor muscles during the tonic vibration reflex in man. The Journal of Physiology. 1991;444(1):645–67. doi: 10.1113/jphysiol.1991.sp018899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nishihira Y, Iwasaki T, Hatta A, et al. Effect of whole body vibration stimulus and voluntary contraction on motoneuron pool. Advances in Exercise and Sports Physiology. 2002;8(4):83–6. [Google Scholar]
- 7.Kossev A, Siggelkow S, Kapels H-H, Dengler R, Rollnik J. Crossed effects of muscle vibration on motor-evoked potentials. Clinical neurophysiology. 2001;112(3):453–6. doi: 10.1016/s1388-2457(01)00473-4. [DOI] [PubMed] [Google Scholar]
- 8.Bolanowski SJ, Gescheider GA, Verrillo RT. Hairy skin: psychophysical channels and their physiological substrates. Somatosensory & motor research. 1994;11(3):279–90. doi: 10.3109/08990229409051395. [DOI] [PubMed] [Google Scholar]
- 9.Bolanowski SJ, Jr, Gescheider GA, Verrillo RT, Checkosky CM. Four channels mediate the mechanical aspects of touch. The Journal of the Acoustical Society of America. 1988;84(5):1680–94. doi: 10.1121/1.397184. [DOI] [PubMed] [Google Scholar]
- 10.Figueroa A, Gil R, Wong A, et al. Whole-body vibration training reduces arterial stiffness, blood pressure and sympathovagal balance in young overweight/obese women. Hypertension research: official journal of the Japanese Society of Hypertension. 2012;35(6):667–72. doi: 10.1038/hr.2012.15. [DOI] [PubMed] [Google Scholar]
- 11.Rittweger J, Mutschelknauss M, Felsenberg D. Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clinical physiology and functional imaging. 2003;23(2):81–6. doi: 10.1046/j.1475-097x.2003.00473.x. [DOI] [PubMed] [Google Scholar]
- 12.Torvinen S, Kannus P, Sievanen H, et al. Effect of four-month vertical whole body vibration on performance and balance. Medicine and science in sports and exercise. 2002;34(9):1523–8. doi: 10.1097/00005768-200209000-00020. [DOI] [PubMed] [Google Scholar]
- 13.Luo J, McNamara B, Moran K. The use of vibration training to enhance muscle strength and power. Sports Medicine. 2005;35(1):23–41. doi: 10.2165/00007256-200535010-00003. [DOI] [PubMed] [Google Scholar]
- 14.Schlee G, Reckmann D, Milani TL. Whole body vibration training reduces plantar foot sensitivity but improves balance control of healthy subjects. Neuroscience letters. 2012;506(1):70–3. doi: 10.1016/j.neulet.2011.10.051. [DOI] [PubMed] [Google Scholar]
- 15.del Pozo-Cruz B, Hernandez Mocholi MA, Adsuar JC, Parraca JA, Muro I, Gusi N. Effects of whole body vibration therapy on main outcome measures for chronic non-specific low back pain: a single-blind randomized controlled trial. Journal of rehabilitation medicine. 2011;43(8):689–94. doi: 10.2340/16501977-0830. [DOI] [PubMed] [Google Scholar]
- 16.Gassner H, Janzen A, Schwirtz A, Jansen P. Random Whole Body Vibration over 5 Weeks Leads to Effects Similar to Placebo: A Controlled Study in Parkinson’s Disease. Parkinson’s disease. 2014;2014:3–5. doi: 10.1155/2014/386495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Deng H, He F, Zhang S, Calleman CJ, Costa LG. Quantitative measurements of vibration threshold in healthy adults and acrylamide workers. International Archives of Occupational and Environmental Health. 1993;65(1):53–6. doi: 10.1007/BF00586059. [DOI] [PubMed] [Google Scholar]
- 18.Liu H, Wu T. Sample size calculation and power analysis of time-averaged difference. Journal of Modern Applied Statistical Methods. 2005;4(2):9. [Google Scholar]
- 19.Schlee G, Reckmann D, Milani TL. Whole body vibration training reduces plantar foot sensitivity but improves balance control of healthy subjects. Neuroscience letters. 2012;506(1):70–3. doi: 10.1016/j.neulet.2011.10.051. [DOI] [PubMed] [Google Scholar]
- 20.Seyle H. The stress of life. New York: McGraw-Hill; 1956. [Google Scholar]
- 21.Young MJ, Breddy JL, Veves A, Boulton AJ. The prediction of diabetic neuropathic foot ulceration using vibration perception thresholds: a prospective study. Diabetes care. 1994;17(6):557–60. doi: 10.2337/diacare.17.6.557. [DOI] [PubMed] [Google Scholar]