

Abstract
Objective:
With more antiepileptic drugs (AED) becoming available in generic form, we estimated the risk of seizure-related events associated with refilling generic AEDs and the effect of switching between different manufacturers of the same generic drug.
Methods:
We designed a population-based case-crossover study using the Medicaid Analytic eXtract and a US commercial health insurance database. We identified 83,001 generic AED users who experienced a seizure-related hospital admission or emergency room visit between 2000 and 2013 and assessed whether they received a refill of the same AED from the same manufacturer or a different manufacturer. Patients served as their own controls and conditional logistic regression was used to compare exposure to a refill during the hazard period, defined as days 2–36 preceding the seizure-related event, to exposure during the control period, defined as days 51–85 preceding the seizure-related event.
Results:
Generic AED refilling was associated with an 8% increase in the odds of seizure-related events (odds ratio [OR] 1.08; 95% confidence interval [CI] 1.06–1.11). The OR following a switch to a different manufacturer of the same AED was 1.09 (95% CI 1.03–1.15); however, after adjusting for the process of refilling, there was no association between switching and seizure-related hospital visits (OR 1.00; 95% CI 0.94–1.07).
Conclusions:
Among patients on a generic AED, refilling the same AED was associated with an elevated risk of seizure-related event; however, there was no additional risk from switching during that refill to a different manufacturer. Generic AEDs available to US patients, with Food and Drug Administration–validated bioequivalence, appear to be safe clinical choices.
Generic antiepileptic drug (AED) use may be associated with increased risk of seizure outcomes.1 According to anecdotal reports and several observational studies, some patients with epilepsy on brand-name AEDs experience seizures after receiving a generic2–5 or switch back after changing to a generic.6 Other reviews and large observational studies have found no link between generic AEDs and seizure activity.7–9 Recent randomized trials of lamotrigine (Lamictal) did not link seizure activity to any small pharmacokinetic differences between brand-name and generic versions10 or between generic versions.11 This was particularly reassuring since prior observational studies had revealed high switchback rates among lamotrigine users.5
The possibility that patients prescribed a generic AED could be switched among different generic manufacturers when a pharmacy changes its supply source or a generic manufacturer exits the market has raised particular concern.12 Different generics could fall at either extreme of the reference product range for bioequivalence parameters, exacerbating the risk of changes in patient seizure control (though one prior review found an average pharmacokinetic difference of only 4%13).
One explanation for the apparent link between AED switching and seizures is the act of refilling, which in one large cohort was associated with a doubling in risk of seizure-related events.8 Another might be that otherwise bioequivalent generic medications do not need to look like each other, or their brand-name counterparts, which has been linked to a substantial increased risk of patient nonadherence.14,15 We therefore sought to focus on switches among generic AEDs to determine if they are associated with an increased incidence of seizures, and whether refilling or pill appearance changes might modify any association.
METHODS
Data sources.
The study was conducted using the Medicaid Analytic Extract database covering the period 2000–2010, including claims data for patients from 49 states and the District of Columbia as well as a commercial health insurance database (Optum Research Database, Eden Prairie, MN) covering the period 2005–2013. These data sources have been used extensively in pharmacoepidemiologic research and cover more than 100 million individuals during the study period (2000–2013).16–18
As done in prior work, pharmacy claims data were linked by National Drug Code (NDC) number to the First DataBank National Drug Data File, which contains descriptive drug information, including the manufacturer, formulation type (capsule, tablet, oral suspension), strength, and color and shape.15 We separately noted brand name and generic manufacturers.
Study design.
We used a case-crossover design to evaluate the relation between seizure-related outcomes and refilling AEDs, either from the same or a different generic manufacturer. We evaluated the following AEDs for which generic versions in pill form were available during the study period: carbamazepine, divalproex, ethosuximide, gabapentin, lamotrigine, levetiracetam, phenytoin, topiramate, valproic acid, and zonisamide. Similar to a crossover trial, participants acted as their own controls and provided information on outcome risk under both exposed and unexposed states, eliminating confounding by factors that are constant within individuals over the study period (figure 1). Case-crossover studies are well-suited for studying the relation between transient exposures, such as medication refilling, and abrupt-onset outcomes, such as seizures, over short periods during which time confounding by factors that vary within individuals is limited.19
Figure 1. Case-crossover study design.

ER = emergency room.
Standard protocol approvals, registrations, and patient consents.
The study was approved by the Institutional Review Board at Brigham and Women's Hospital.
Case ascertainment.
Cases were identified as patients with an emergency room (ER) visit or hospitalization for seizures using ICD-9-CM codes 345.xx (epilepsy), 333.2x (myoclonus), or 780.3x (convulsions) as the primary discharge diagnosis.20 The index date was defined as the date of the ER visit or hospital admission. Patients had to have at least 6 months of continuous health plan enrollment prior to the index date with no seizure-related hospitalizations or ER visits during that period and at least one dispensing of an eligible AED during at least one study period (figure 1). If more than one eligible seizure-related event occurred during the study period, only the first event was included in the analysis.
Exposure assessment.
First, we evaluated the effect of refilling of the same AED from the same manufacturer. A refill was defined as a dispensing preceded by a prescription record for the medication with the same NDC (except for last 2 digits indicating package size), as long as that second prescription occurred during the days' supply of the previous dispensing (plus a 5-day grace period). Days' supply is defined as the number of days that a prescription fill will last if taken as directed.
Second, we evaluated the effect of a switch from one generic manufacturer to another, defined as a dispensing of the same dose and the same formulation of the same generic AED product, but from a different manufacturer, within the days' supply of the previous dispensing, plus a 5-day grace period. Among manufacturer switches, we separately looked at switches that involved pill appearance (color or shape) changes and switches that did not involve such changes.
Statistical analysis.
We used conditional logistic regression analysis to compare the odds of exposure to a refill or a refill with a switch in manufacturer during the hazard period to the odds of exposure in the control period. The hazard period was defined as days 2–36 preceding the seizure-related event (day 1 preceding the seizure was chosen as an induction period). The control period was defined as days 51–85 preceding the index date. Each individual served as his or her own control and formed his or her own stratum. The 35-day periods were chosen to allow patients to run out of a filled medication (assuming a 30-day fill on average), given that switching to a differently appearing product has been associated with nonadherence. We also conducted a sensitivity analysis with 21-day case and control periods.
To account for the effect of the refilling process, we conducted a conditional logistic regression analysis among patients who either refilled or switched. We included as independent variables a binary indicator for exposure (1 = refill or a switch, 0 = otherwise) and an “exposure × group” interaction term, where group was an indicator for type of change (1 = switch, 0 = refill). The antilogarithm of the coefficient for the product term can be interpreted as the increase in the odds of seizure-related outcome associated with switching among different manufacturers of the same AED product beyond that associated with the refilling process.
All analyses were performed using the SAS statistical package version 9.4 (SAS Institute, Cary, NC).
RESULTS
We identified 83,001 patients with 112,306 episodes of ER visits or hospitalizations for seizures meeting our eligibility criteria. Among them, there were 5,200 patients with at least one generic-to-generic switch (either of the same or different appearance) during the relevant observation periods (figure 2) and 59,344 patients with at least one refill of a prescription from the same manufacturer.
Figure 2. Patient flow chart.

AED = antiepileptic drug; ER = emergency room.
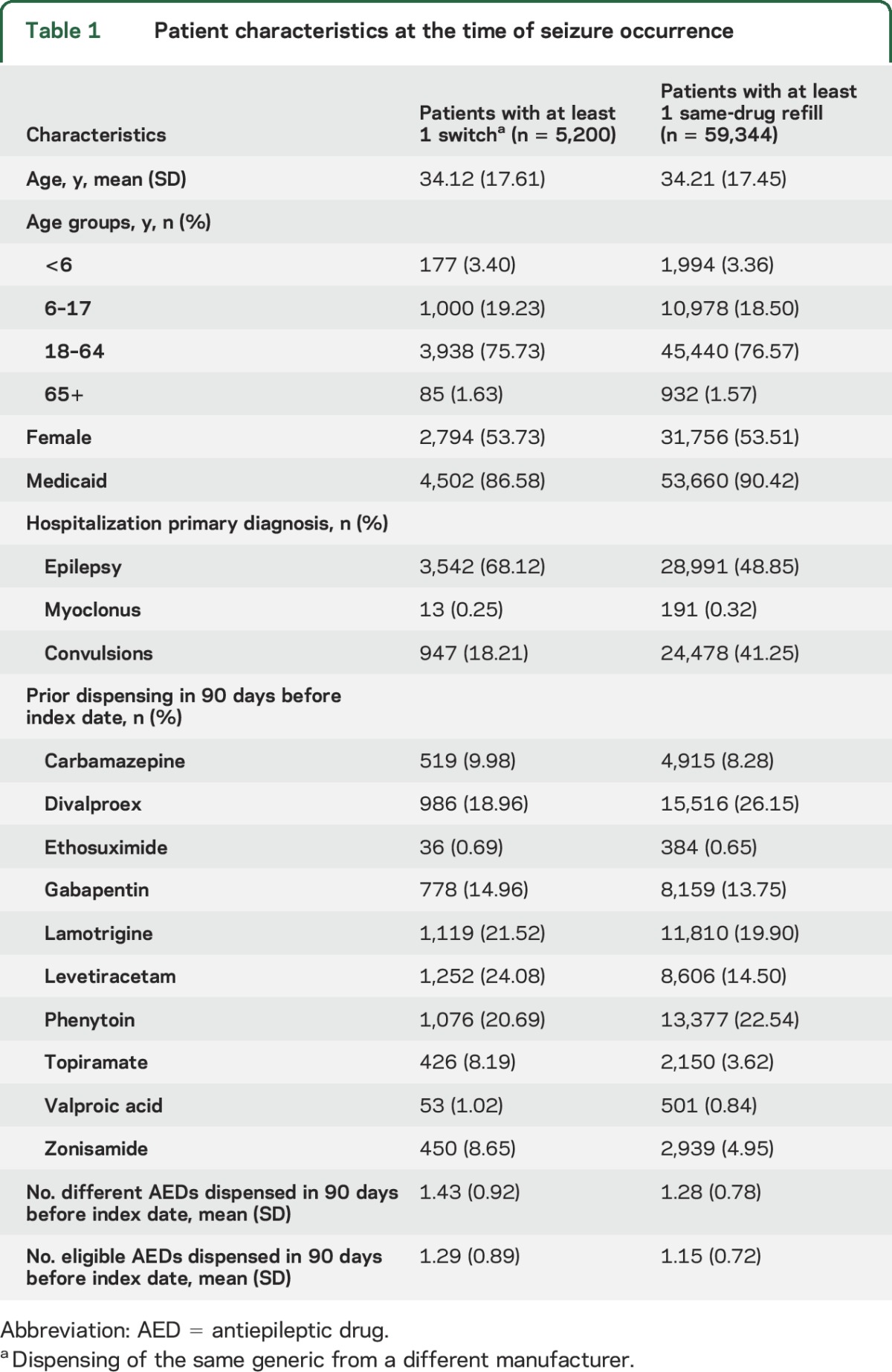
As compared to patients whose refill came from the same manufacturer, patients who experienced a generic-to-generic switch were more likely to have diagnosis codes for epilepsy (as compared to convulsion) associated with the index ER visit or hospitalization and to be on newer medications, such as levetiracetam, topiramate, and zonisamide (table 1).
Table 1.
Patient characteristics at the time of seizure occurrence
Effect of refilling.
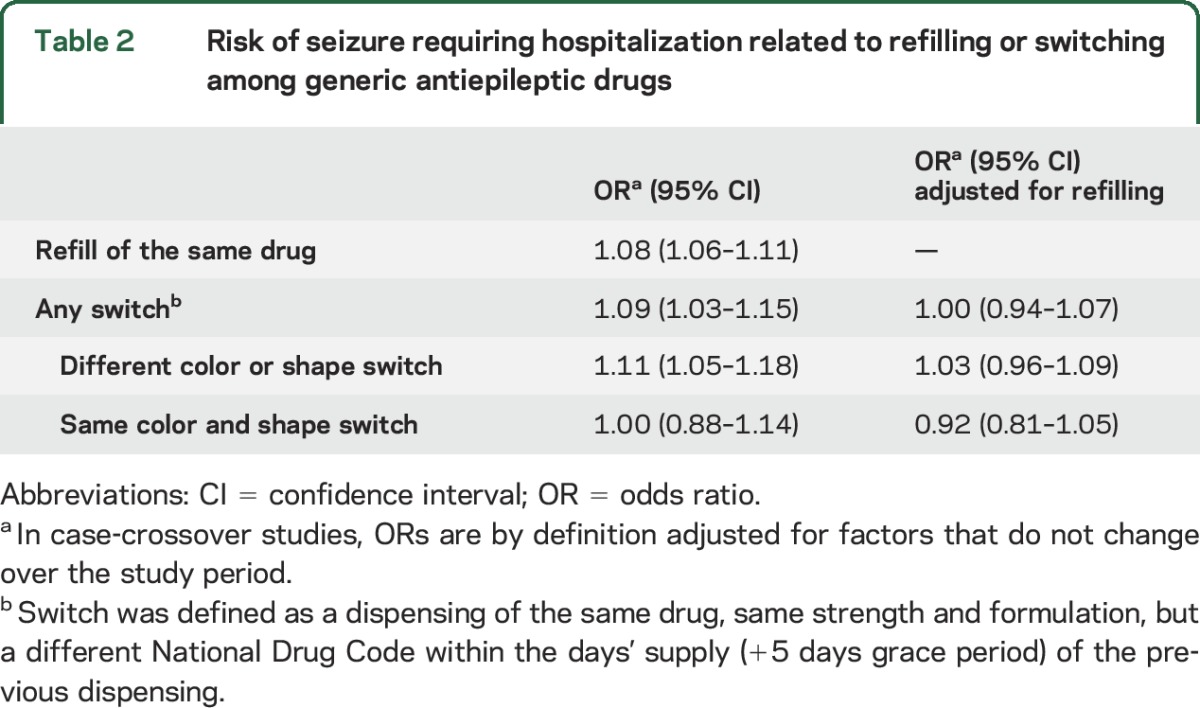
Of the 59,344 patients with refills of exactly the same medication from the same manufacturer, 46% had a refill in one period but not both, and thus, contributed to the analysis; 52% had a refill during the hazard period and 48% during the control period. Odds of exposure were 8% higher in the hazard period immediately preceding the seizure-related ER visit or hospitalization (odds ratio [OR] 1.08; 95% confidence interval [CI] 1.06–1.11) (table 2).
Table 2.
Risk of seizure requiring hospitalization related to refilling or switching among generic antiepileptic drugs
Effect of switching generic AED manufacturer.
Of the 5,200 generic-to-generic switch cases, 4,310 (83%) had a switch that involved a change in either a shape or color and 1,012 (19%) had a switch that was of the same shape and color. In the analysis of any generic-to-generic switch, 92% of cases had a switch in one period but not the other; 52% had a refill during the hazard period and 48% during the control period. Odds of a switch in the hazard period were 9% higher than the odds in the control period (OR 1.09; 95% CI 1.03–1.15). When we considered generic-to-generic switching that involved a change in color or shape or generic-to-generic switching in which color and shape stayed the same, the ORs were 1.11 (95% CI 1.05–1.18) and 1.00 (0.88–1.14), respectively.
After adjusting for the process of refilling, ORs were 1.00 (95% CI 0.94–1.07) for any switch, 1.03 (95% CI 0.96–1.09) for a generic-to-generic switch between medications of different color or shape, and 0.92 (95% CI 0.81–1.05) for a generic-to-generic switch between medications of the same color and shape (table 2).
Sensitivity analysis.
In the 21-day sensitivity analysis, the OR for refilling was 1.01 (95% CI 0.99–1.04) and refill-adjusted ORs were 1.03 (95% CI 0.96–1.11) for any generic-to-generic switch, 1.04 (0.96–1.13) for a generic-to-generic switch to pills of different color or shape, and 1.00 (95% CI 0.85–1.17) for a generic-to-generic switch to a medication of the same color and shape (see table e-1 at Neurology.org).
DISCUSSION
In this study of patients in 2 large national US databases who experienced seizures over the last decade while being treated with a generic AED, we determined that there was no association between switches among generic manufacturers and seizure outcomes after accounting for the refill process. We found that among patients with seizures on AEDs who successfully refilled their medications, the outcome was not affected by whether that refill was characterized by a different Food and Drug Administration (FDA)–approved manufacturer or a pill of a different appearance.
These results add to the growing literature supporting the routine use of interchangeable generic AEDs among patients with seizure disorders. However, numerous states have special carve-outs to their pharmacy laws that restrict pharmacists' abilities to substitute generic AEDs when physicians refer to the brand-name version on their prescriptions.21 Such positions were taken to help protect patients from products believed to be substandard, but they may need to be updated in light of more recent data contrary to this perception. Some organizations have updated their views on the topic. In January 2016, the American Epilepsy Society issued a new statement on AED substitution, concluding, “drug formulation substitution with FDA-approved generic products usually reduces cost, and does not compromise efficacy.”22 We agree that generic drugs that have been proven to be safe and reliable have numerous benefits for patients, including reducing cost-related nonadherence23 and improving patient outcomes.24
Our study also highlights the importance to patient seizure outcomes of the act of AED refilling. We found that refilling the same strength of the same AED from the same manufacturer is itself associated with seizure events. The refilling process is often not straightforward. Patients have expressed frustration with delays and other complicating factors relating to refilling.25 Some pharmacies and prescription benefits managers have experimented with programs to enhance the patient experience and encourage timely medication refilling, such as CVS Caremark's ReadyFill, an automated refill service, even showing that they improve medication adherence.26 Greater work to enhance the refilling process, and to determine whether mail order pharmacies successfully improve outcomes on this point, is necessary. Another possibility is that the refilling effect we observed may be due to lot variations within a particular manufacturer, although manufacturing consistency is a core element of FDA-certified Good Manufacturing Practices that generic manufacturers must employ. Of note, while previous studies have found that pill shape and color was associated with nonpersistence with AEDs and cardiovascular medications, this study showed that pill appearance was not a separate predictor of seizure outcomes, at least among patients who took the pills home.
A major strength of our study was the large-scale population-based cohort of patients who experienced seizures while being treated with a generic AED, with complete ascertainment of AED history prior to a seizure event. In addition, by using the case-crossover design, we eliminated confounding due to measured and unmeasured differences between individuals, as well as by factors that might change within individuals but were likely to stay stable for the duration of the study period (3 months prior to the seizure event).
Several limitations should be noted. We identified seizures using hospital or ER ICD-9 codes; therefore, our study is limited to the patients whose seizures were severe enough to warrant either an ER visit or hospitalization. Thus, we are missing patients who experienced seizures that did not require hospital visits or medical care. However, our case definition did allow us to focus on the most clinically relevant seizures, and internal validity of the results was high due to improved specificity of the case definition. Fewer than 2% of the patients were 65 years of age or older. Older patients might become more confused when dispensed pills of different color and shape and thus more susceptible to nonadherence caused by a switch. Associations between switches and seizures in this population remain to be explored. Misclassification of exposure is possible, since pharmacy claims data provide accurate information about drugs dispensed to patients, but do not provide information on whether patients actually consumed the medications. Finally, as an administrative data source, our data represent billed transactions between providers and a payer and there is a lack of information about important clinical parameters that could have contributed to the observed associations. While case-crossover designs inherently control for differences between patients due to clinical characteristics that do not change over the study period (90 days in our study), confounding due to an individual's changing health status or other factors that might have influenced the seizure risk during that period is possible and cannot be ruled out. Of note, the results of our study are limited to epilepsy patients who take generic drugs and are therefore at risk for pill appearance changes, and not the fraction of patients who remain on brand-name versions of AEDs, even when generic versions of those products become available.
Despite these limitations, we found that patients with seizure disorder on a generic AED had a modest increase in risk of severe seizures in the period shortly after a refill, but that there was no additional risk from switching during that refill to a different manufacturer. These data provide further reassurance to patients with seizures who receive generic AEDs, even if those patients may experience changes in the manufacturer of that AED. Generic AEDs available to US patients, with FDA-validated bioequivalence, appear to be safe clinical choices.
Supplementary Material
GLOSSARY
- AED
antiepileptic drug
- CI
confidence interval
- ER
emergency room
- FDA
Food and Drug Administration
- ICD-9-CM
International Classification of Diseases, 9th Revision, Clinical Modification
- NDC
National Drug Code
- OR
odds ratio
Footnotes
Supplemental data at Neurology.org
Editorial, page 1754
AUTHOR CONTRIBUTIONS
All authors: drafting/revising the manuscript for content, study concept or design, analysis or interpretation of data. A.S.K., N.K.C.: study supervision or coordination.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
A. Kesselheim's work is supported the Laura and John Arnold Foundation, the Harvard Program in Therapeutic Science, and the Greenwall Faculty Scholars in Bioethics. Dr. Kesselheim has received grants from the FDA Office of Generic Drugs unrelated to this work. K. Bykov is supported by a training grant from Takeda through Harvard T.H. Chan School of Public Health. J. Gagne has received grants from the FDA Office of Generic Drugs unrelated to this work. Dr. Gagne is Principal Investigator of a grant from Novartis Pharmaceuticals Corporation to Brigham and Women's Hospital for unrelated work and he is a consultant to Aetion, Inc., a software company, and to Optum, Inc. S. Wang is supported by grant R00HS022193 from the Agency for Healthcare Research and Quality and is a consultant to Aetion, Inc. N. Choudhry has received unrestricted research grants from CVS Caremark, Aetna, the Commonwealth Fund, and the Robert Wood Johnson Foundation to study medication adherence. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Liow K, Barkley GL, Pollard JD, et al. Position statement on the coverage of anticonvulsant drugs for the treatment of epilepsy. Neurology 2007;68:1249–1250. [DOI] [PubMed] [Google Scholar]
- 2.Fitzgerald CL, Jacobson MP. Generic substitution of levetiracetam resulting in increased incidence of breakthrough seizures. Ann Pharmacother 2011;45:e27. [DOI] [PubMed] [Google Scholar]
- 3.Makus KG, McCormick J. Identification of adverse reactions that can occur on substitution of generic for branded lamotrigine in patients with epilepsy. Clin Ther 2007;29:334–341. [DOI] [PubMed] [Google Scholar]
- 4.Berg MJ, Gross RA, Tomaszewski KJ, Zingaro WM, Haskins LS. Generic substitution in the treatment of epilepsy: case evidence of breakthrough seizures. Neurology 2008;71:525–530. [DOI] [PubMed] [Google Scholar]
- 5.Andermann F, Duh MS, Gosselin A, Paradis PE. Compulsory generic switching of antiepileptic drugs: high switchback rates to branded compounds compared with other drug classes. Epilepsia 2007;48:464–469. [DOI] [PubMed] [Google Scholar]
- 6.Duh MS, Paradis PE, Latrémouille-Viau D, et al. The risks and costs of multiple-generic substitution of topiramate. Neurology 2009;72:2122–2129. [DOI] [PubMed] [Google Scholar]
- 7.Kesselheim AS, Stedman MR, Bubrick EJ, et al. Seizure outcomes following use of generic vs. brand-name antiepileptic drugs: a systematic review and meta-analysis. Drugs 2010;70:605–621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gagne JJ, Avorn J, Shrank WH, Schneeweiss S. Refilling and switching of antiepileptic drugs and seizure-related events. Clin Pharmacol Ther 2010;88:347–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Devine ST, Weisbart E, Barron J, et al. Acute epilepsy exacerbations in patients switched between A-rated anti-epileptic drugs. Curr Med Res Opin 2010;26:455–463. [DOI] [PubMed] [Google Scholar]
- 10.Ting TY, Jiang W, Lionberger R, et al. Generic lamotrigine versus brand-name Lamictal bioequivalence in patients with epilepsy: a field test of the FDA bioequivalence standard. Epilepsia 2015;56:1415–1424. [DOI] [PubMed] [Google Scholar]
- 11.Privitera MD, Welty TE, Gidal BE, et al. Generic-to-generic lamotrigine switches in people with epilepsy: the randomised controlled EQUIGEN trial. Lancet Neurol 2016;15:365–372. [DOI] [PubMed] [Google Scholar]
- 12.Kesselheim AS, Bykov K, Tong A, Doherty M, Avorn J, Choudhry NK. Burden of pill appearance changes for patients taking generic cardiovascular medications after myocardial infarction: cohort and nested case-control studies. Ann Intern Med 2014;161:96–103. [DOI] [PubMed] [Google Scholar]
- 13.Davit BM, Nwakama PE, Buehler GJ, et al. Comparing generic and innovator drugs: a review of 12 years of bioequivalence data from the United States Food and Drug Administration. Ann Pharmacother 2009;43:1583–1597. [DOI] [PubMed] [Google Scholar]
- 14.Yu LX, Geba GP. Generic pills from the patient perspective: dressed for success? JAMA Intern Med 2013;173:208–209. [DOI] [PubMed] [Google Scholar]
- 15.Kesselheim AS, Misono AS, Shrank WH, et al. Variations in pill appearance of antiepileptic drugs and the risk of nonadherence. JAMA Intern Med 2013;173:202–208. [DOI] [PubMed] [Google Scholar]
- 16.Eng P, Johannes C, Chiang C, West W, Seeger J, Walker A. Survey of disability, medication use, and medication satisfaction among members with rheumatoid arthritis of a large health care plan database. Pharmacoepidemiol Drug Saf 2005;14:S1–S218. [Google Scholar]
- 17.Kesselheim AS, Bykov K, Avorn J, Tong A, Doherty M, Choudhry NK. Burden of changes in pill appearance for patients receiving generic cardiovascular medications after myocardial infarction: cohort and nested case–control studies. Ann Intern Med 2014;161:96–103. [DOI] [PubMed] [Google Scholar]
- 18.Seeger JD, Daniels G. Commercial databases. In: Strom B, Hennessey S, Kimmel S, editors. Pharmacoepidemiology, 5th ed. Chichester: Wiley; 2012:189–208. [Google Scholar]
- 19.Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. Am J Epidemiol 1991;133:144–153. [DOI] [PubMed] [Google Scholar]
- 20.Kee VR, Gilchrist B, Granner MA, et al. A systematic review of validated methods for identifying seizures, convulsions, or epilepsy using administrative and claims data. Pharmacoepidemiology and Drug Safety 2012;21(suppl 1):183–193. [DOI] [PubMed] [Google Scholar]
- 21.Tennessee Code Annotated §53-10-210; 2015. [Google Scholar]
- 22.American Epilepsy Society. Substitution of Different Formulations of Antiepileptic Drugs for the Treatment of Epilepsy; 2016. Available at: https://www.aesnet.org/about_aes/generic-position-statement. Accessed September 16, 2016. [Google Scholar]
- 23.Shrank WH, Hoang T, Ettner SL, et al. The implications of choice: prescribing generic or preferred pharmaceuticals improved medication adherence for chronic conditions. Arch Intern Med 2006;166:332–337. [DOI] [PubMed] [Google Scholar]
- 24.Gagne JJ, Choudhry NK, Kesselheim AS, et al. Comparative effectiveness of generic and brand-name statins on patient outcomes: a cohort study. Ann Intern Med 2014;161:400–407. [DOI] [PubMed] [Google Scholar]
- 25.Hsu C, Lemon JM, Wong ES, et al. Factors affecting medication adherence: patient perspectives from five veterans affairs facilities. BMC Health Serv Res 2014;14:533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Matlin OS, Kymes SM, Averbukh A, et al. Community pharmacy automatic refill program improves adherence to maintenance therapy and reduces wasted medication. Am J Manag Care 2015;21:785–791. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.