

Abstract
Background
The aetiology of constipation in Parkinson's disease remains poorly understood. Defaecatory dyssynergia, anal sphincter spasticity and slow transit constipation may, individually or collectively, play a role.
Aims
In this retrospective cohort analysis of patients with Parkinson's disease and chronic constipation, we determined the utility of high-resolution anorectal manometry, balloon expulsion and wireless motility capsule testing in defining the underlying aetiology for constipation.
Methods
In this retrospective cohort study, consecutive patients with Parkinson's disease and chronic constipation underwent clinical assessment, manometry with balloon expulsion and wireless motility capsule testing using standard protocols.
Results
We studied 66 patients fulfilling Rome IV criteria for functional constipation. Most patients (89%) had abnormal manometry, exhibiting various types of defaecatory dyssynergia (mostly types II and IV), abnormal balloon expulsion, diminished rectal sensation and, in some, lacking rectoanal inhibitory reflex. 62% exhibited colonic transit delay by wireless motility capsule study, while 57% had combined manometric and transit abnormalities, suggesting of overlap constipation. Symptoms of infrequent defaecation, straining and incomplete evacuation were not discriminatory. There was a relationship between constipation scores and colonic transit times (p=0.01); Parkinson's disease scores and duration were not correlated with either the manometric or transit findings. Faecal incontinence was seen in 26% of the patients.
Conclusions
Chronic constipation in patients with Parkinson's disease may reflect pelvic floor dyssynergia, slow transit constipation or both, and may be associated with faecal incontinence, suggesting both motor and autonomic dysfunction. Anorectal manometry and wireless motility capsule testing are useful in the assessment of these patients.
Keywords: CONSTIPATION, ANAL INCONTINENCE, ANORECTAL PHYSIOLOGY, COLORECTAL MOTILITY
Summary box.
What is already known about this subject?
-
▸
Chronic constipation and defaecatory dysfunction are quite prevalent in patients with Parkinson's disease (PD) and their pathophysiology is complex and multifactorial.
-
▸
High-resolution manometry (HRAM) and balloon expulsion testing (BET) are widely used method for the diagnosis of defaecatory dysfunction.
-
▸
The wireless motility capsule (WMC) can routinely quantify colonic transit.
What are the new findings?
-
▸
Chronic constipation in PD mostly reflects underlying defaecatory dyssynergia, but slow transit constipation and overlap syndromes occur.
-
▸
HRAM, BET and WMC are useful in the assessment of patients with PD with chronic constipation.
-
▸
There is a significant relationship between constipation scores and colonic transit times but PD scores and disease duration are not correlated with either the manometric or colonic transit findings.
How might it impact on clinical practice in the foreseeable future?
-
▸
The usage of HRAM, BET and WMC can transform the non-specific symptoms of constipation and defaecatory dysfunction into specific disorders, such as dyssynergia, slow transit constipation and overlap syndromes and may guide specific clinical management in patients with PD.
Introduction
Slow transit constipation, dyssynergic defaecation and faecal incontinence are common problems in patients with Parkinson's disease (PD); their aetiology is multifactorial and their management challenging.1 Radiological assessment of colonic transit using Sitzmarks2 and the assessment of anorectal pressures and sensation by anorectal manometry (ARM) and balloon expulsion test (BET) are important clinical tools for the diagnosis of slow transit constipation, dyssynergic defaecation and faecal incontinence in patients who do not respond to conservative therapy.3 4
In lieu of Sitzmarks study, recent guidelines have supported the wireless motility capsule (WMC) for the evaluation of colonic transit in chronic constipation,5 while high-resolution anorectal manometry (HRAM) and BET have being increasingly used for the diagnosis of dyssynergic defaecation and faecal incontinence, instead of conventional ARM. HRAM provides greater resolution, minimises artefacts, and generates three-dimensional topographical plots of intraluminal pressure profiles, increasing the diagnostic accuracy of anorectal dysfunction.6
The WMC (Smartpill) is an ambulatory non-invasive and non-radioactive diagnostic sensor that continuously samples intraluminal pH, temperature and pressure as it moves through the gastrointestinal tract. Studies have shown that the estimated interparticipant coefficients of variation in healthy and constipated participants are 1 and 0.99, respectively.7 This new technology has permitted routine quantification of transit in all gut regions in a single test and it has been increasingly used for the diagnosis of slow transit constipation.8 Used together, WMC, HRAM and BET are poised to guide optimal therapy for functional anorectal disorders in the general population as well as in special groups, such as in patients with PD.
The aim of this retrospective cohort study was to objectively characterise chronic constipation in patients with PD, assess the prevalence of defaecatory dyssynergia, slow transit constipation and the propensity to faecal incontinence, and to highlight objective parameters that can help in the current management algorithm for anorectal dysfunction in such patients.
Study population and methods
Patients
The study retrospective cohort study using prospectively collected data was approved by the Institutional Research Board of Stanford University and was conducted at the Neuro-gastroenterology and Motility Center of Silicon Valley Gastroenterology, in Mountain View, California, USA. The protocol was considered exempt from the need for individual informed consent from participating patients.
Inclusion criteria
We included consecutive patients with PD who were all evaluated because of constipation and defaecation difficulties and agreed to undergo HRAM with BET and WMC. All patients had recurrent symptoms persisting for >6 months, while those with faecal incontinence reported recurrent uncontrolled passage of faecal material, not related to a temporary diarrhoeal event.9 All patients fulfilled the Rome IV criteria for functional constipation defined as any two of the following features: straining, lumpy hard stools, sensation of incomplete evacuation, use of digital manoeuvres, sensation of anorectal obstruction or blockage with 25% of bowel movements, and decrease in stool frequency (<3 bowel movements per week).10
Exclusion criteria
Patients <18 years old, those with known gastrointestinal pathology (ie, inflammatory bowel disease, stricture), other systemic illnesses affecting motility (ie, scleroderma) and those who had previously undergone respective gastrointestinal surgery were excluded.
The study patients were part of a total cohort of 95 patients with PD referred and evaluated at our centre during the study period for various gastrointestinal symptoms, predominantly constipation, dysphagia, nausea, early satiety, malnutrition and weight loss (figure 1). All study participants had previously undergone colonoscopy or sigmoidoscopy without revealing any structural explanation for their constipation. Symptoms were recorded on questioning and formal quantitative questionnaire-based assessment. Neurological assessment of the patients was made using the previously validated modified Hoehn and Yahr scale (score 0–5)11 and the duration of PD was recorded in years since the time of diagnosis. Variable regimens of PD therapies were used and not discontinued for the conduct of any of the tests performed. Such therapies included carbidopa-levodopa, carbidopa-levodopa-entacapone, pramipexole, ropinirole, rotigotine, rasagiline, trihexyphenidyl, selegiline, tolcapone, rivastigmine and amantadine in various doses and schedules (table 1). Prospectively collected clinical, transit and manometric data from these patients were then analysed. Of note, the study, albeit community-based, was on a referral population to a gastrointestinal motility unit.
Figure 1.
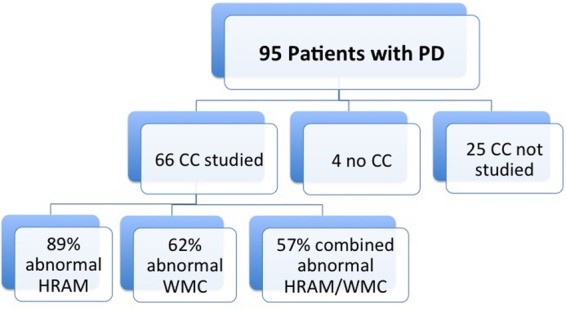
Study flow diagram. Of the entire population of 95 patients with PD referred, 66 were studied with HRAM and 53 of those with WMC as well. CC, chronic constipation; HRAM, high-resolution anorectal manometry; PD, Parkinson's disease; WMC, wireless motility capsule.
Table 1.
List of Parkinson's disease drugs used by the patients in the study (n=66) and the respective number of users
| Drug | Number of patients (out of 66) |
|---|---|
| Levodopa | 58 |
| Pramipexole | 11 |
| Ropinirole | 6 |
| Rotigotine | 11 |
| Amantadine | 9 |
| Rasagiline | 30 |
| Entacapone | 11 |
| Trihexyphenidyl | 1 |
| Selegiline | 1 |
| Tolcapone | 1 |
| Rivastigmine | 5 |
Many patients were using combination therapies.
Questionnaires
In order to qualify for inclusion into the study, patients had to be symptomatic on a simple and previously validated questionnaire. In this questionnaire, the symptoms were graded with scores for bloating, reduced frequency of bowel evacuation (<3/week), straining at evacuation, sensation of incomplete evacuation and faecal incontinence (0=no symptom, 1=mild symptom, 2=moderate symptom and 3=severe symptom, occurring at various frequencies (once a week=0, 2–6 times a week=1, 7–15 times a week=2 and more than 15 times a week=3)).12
Wireless motility capsule
The WMC (Smartpill; Medtronic, Sunnyvale, California, USA) is an ambulatory, non-invasive and non-radioactive diagnostic sensor that continuously samples intraluminal pH, temperature and pressure as it moves through the gastrointestinal tract.13 Patients first ingested a meal in order to initiate the postprandial motility pattern following an overnight fast. The meal consisted of a SmartBar (260 kcal, 2% fat, 2 g fibre), followed by 120 mL water. Immediately after the meal, patient swallowed the capsule with 50 mL water. Patients were then released and they were given the data receiver and a diary for recording bowel movements, food intake, sleep and gastrointestinal symptoms. Physical restrictions included no strenuous activities such as sit-ups, abdominal crunches and prolonged aerobic activity (>15 min), which could affect pressure measurements. Additionally, patients refrained the use of gastrointestinal medications that could affect motility (ie, laxatives) or gastric pH (ie, proton pump inhibitors). Patients were asked to fast for 6 hours after capsule ingestion, after which they ingested a regular meal. This meal would allow for the evaluation of the fed response, which is the change in contractile pattern of the small bowel from a fasting to postprandial pattern. Patients were then instructed to continue their regular diet and routine and to return the data receiver and diary to our facility after 5 days. Downloaded data are analysed using the display software (Medtronic, Sunnyvale, California, USA).
HRAM and BET
HRAM was performed using a solid-state catheter (Manoscan Anorectal Manometry, Medtronic, Sunnyvale, California, USA).14 15 All procedures were performed as follows: prior to inserting the HRAM catheter, the participants were trained to understand how to squeeze or push and bear down to simulate defaecation. After ∼60 s resting period for patient's equilibrium and familiarity with the catheter in the rectum, HRAM and BET were performed in a standardised sequence with a 30 s recovery between the various phases. After initial determination of the anal resting pressure, the anal squeeze pressure was measured as the highest squeeze pressure obtained during 5 s of voluntary contraction of the anal sphincter. The average of three attempts was recorded. Rectal and anal pressures during simulated evacuation were then measured before and after filling of a rectal balloon with 60 mL of water. For simulated defaecation, patients were asked to push as previously instructed for 5 s. Rectoanal inhibitory reflex, minimal volumes for the first sensation, desire to defaecate and urgency were also measured. BET was performed with the balloon filled with 60 mL of water. Balloon expulsion was considered normal if an elapsed time of <1 min was noted.16
Data analysis
Clinical information, including age, gender and gastrointestinal symptoms, was collected in all patients. WMC, HRAM and BET were analysed under blinded conditions. WMC colonic transit time (CTT) >59 hours was considered diagnostic of slow transit constipation. HRAM was considered as the gold standard for the diagnosis of dyssynergia. Those patients with abnormal CTT and HRAM were considered as suffering of overlap constipation. Based on the results of HRAM, patients were classified as having normal coordination or dyssynergia types I–IV.17 Type I dyssynergia was characterised by adequate rectal propulsion with paradoxical anal contraction. Type II dyssynergia was characterised by impaired rectal propulsion associated with paradoxical anal contraction. Type III dyssynergia was characterised by adequate rectal propulsion with an incomplete anal relaxation. Type IV dyssynergia was characterised by impaired rectal propulsion with incomplete anal relaxation. Impaired rectal propulsion, or the insufficient rectal pressure elevation during attempted defaecation, was defined as <40 mm Hg in men and <25 mm Hg in women. Normal anal relaxation during attempted defaecation was defined as a pressure decrease of ≥20%.18 Incomplete anal relaxation during attempted defaecation was defined as absence or pressure decrease of <20%, and paradoxical anal contraction was defined as an anal pressure increase over the resting pressure when the patients were asked to push. Anal sphincter length and resting sphincter and squeeze pressures were separately analysed for patients with faecal incontinence. Normal anal sphincter length was defined as >3.9 cm for men and >3.8 cm in women. Normal anal resting pressure was defined as >67 mm Hg in men and > 60mm Hg in women. Normal anal squeeze pressure was defined as >200 mm Hg in men and >164 mm Hg in women.
Statistical analysis
Statistical analysis was performed using Minitab software. When applicable, p values of <0.05 were considered statistically significant.
Results
Clinical characteristics of the study population
Sixty-six patients with PD fulfilling Rome IV criteria for functional chronic constipation were enrolled in the study; 17 (26%) of them also reported faecal incontinence. As shown in figure 1, these patients represented 69% of the total number of patients with PD evaluated at our centre because of various gastrointestinal symptoms. Of the remaining 29, 4 (4%) did not have constipation, while 25 (27%) had constipation but could not be studied for various reasons (ie, not interested, too ill, insurance non-authorisation, etc). Clinically, these 25 patients were not significantly different than those in our cohort, suggesting that our study cohort was representative of a larger PD population with gastrointestinal symptoms referred for evaluation and management. Specifically, their median age was 76 (range 57–95), 28% were female, and their median cumulative symptom score was 1.25 (95% CI 0.38 to 1.75; as compared with the cohort's median score of 1.58 (95% CI 0.41 to 1.91)).
The median age of the 66 patients in the study was 71 years (range 52–91 years), and 26 (39%) of them were women. The median Hoehn and Yahr score was 3 (95% median CI 2.72 to 3.00); median duration of their PD was 8.5 years (range 3–20). Figure 2 depicts the mean scores for the individual symptoms assessed by questionnaires; bloating 1.05 (95% median CI 0.00 to 1.00), constipation 1.91 (95% median CI 1.00 to 3.00), straining at defaecation 1.83 (95% median CI 1.98 to 2.00), incomplete evacuation 1.34 (95% median CI 1.00 to 2.00) and faecal incontinence 0.41 (95% median CI 0.00 to 0.00).
Figure 2.
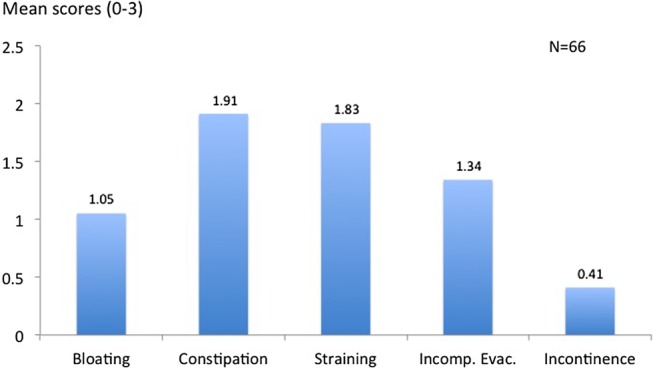
Mean symptom scores of the study cohort.
High-resolution anorectal manometry
The median anal sphincter length was 3.1 cm (95% CI 2.79 to 3.30). Figure 3 depicts box plot graphs highlighting resting and squeeze anal sphincter pressures in mm Hg (top) and sphincter lengths in cm (bottom). By HRAM, decreased anal resting pressure was noted in 38 patients (58%), increased in 14 (21%) and normal in 14 (21%). Decreased anal squeeze pressure was noted in 50 patients (76%), increased in 7 (11%) and normal in 9 (14%) of patients; the median anal resting pressure and squeeze pressure were 61 mm Hg (95% CI 52.83 to 74.01) and 160 mm Hg (95% CI 140.90 to 169.01), respectively. The median rectal pressure and anal pressure during simulated evacuation were 18 (95% CI 12.9 to 22) and 75 mm Hg (95% CI 63.9 to 86), respectively. The median percentage of anal relaxation was 5 (95% CI 1.9 to 7.00). The median first sensation was elicited with 60 cc of balloon distention (95% CI 60.0 to 60.0). During BET, only eight patients (12%) were able to expel the balloon in 1 min. This latter group of patients was also noted to have normal defaecatory coordination on HRAM (see below).
Figure 3.

Box plot graphs highlighting resting and squeeze anal sphincter pressures in mm Hg (top) and sphincter lengths in cm (bottom). The plots display the distribution of data as: minimum (bottom whisker), first quartile (lower part of box), median (line in box), third quartile (upper part of box) and maximum (top whisker).
When analysed separately, the median age of the 17 patients with faecal incontinence was 72 years (range 61–82 years), and 65% were men. In this group, the median sphincter length was 2.8 cm (95% median CI 1.89 to 3.49), median anal resting pressure was 64 (95% median CI 41.29 to 90.24) and the median squeeze pressure was 134 (95% median CI 100.88 to 160.19). These values were not statistically different from those of the 49 remaining cohort patients without faecal incontinence, in whom the median sphincter length was 3.1 cm (95% median CI 2.82 to 3.40), median anal resting pressure was 61 (95% median CI 53.21 to 74.78) and the median squeeze pressure was 168 (95% median CI 152.28 to 184.78). Although the number of observations is small, these results suggest that the HRAM values may not reflect the clinical occurrence of faecal incontinence in this group of patients. Overall, 24% had passive faecal incontinence and 76% had urge incontinence (data not shown).
The pie charts of composite figure 4 highlight several HRAM characteristics of the study cohort, such as (A) the percentage of abnormal BETs (88%, 58 patients) and (B) the per cent prevalence of certain anal sphincter measurements, such as low internal anal sphincter (IAS) and low external anal sphincter (EAS), predisposing to faecal incontinence (48%, 32 patients); normal sphincter profiles for IAS and EAS (47%, 31 patients); and high IAS and EAS (anismus) predisposing to constipation (5%, 3 patients). Further, they depict (C) the percentage of abnormal balloon sensation tests denoting impaired rectal sensation (30%, 20 patients), and (D) the percentage of patients with absent rectoanal inhibitory reflex, suggestive of impaired rectoanal coordination (18%, 12 patients).
Figure 4.
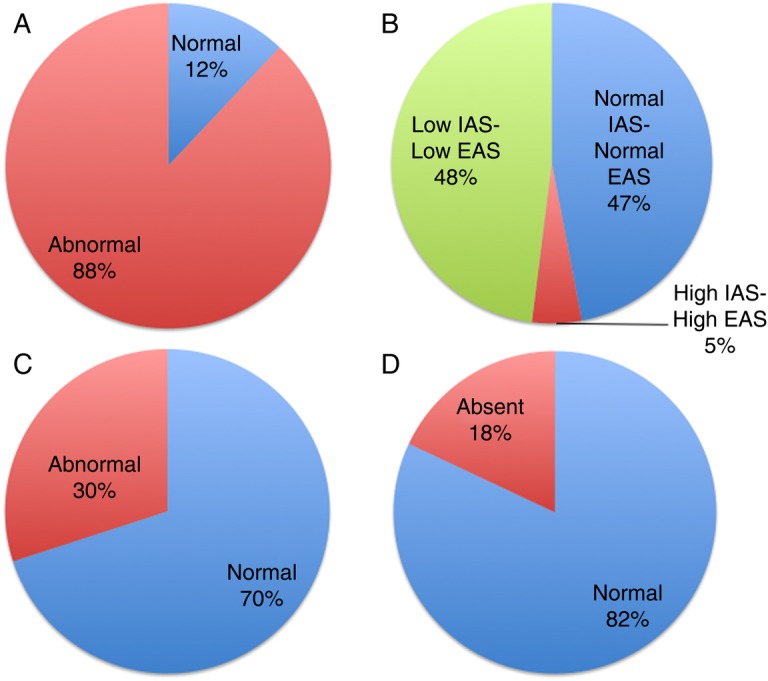
Composite figure (pie charts) highlighting several HRAM characteristics of the study cohort. (A) Balloon expulsion test; (B) per cent prevalence of certain anal sphincter measurements, such as low IAS and low EAS, predisposing to faecal incontinence; normal sphincter profiles for IAS and EAS; and high IAS and EAS (anismus) predisposing to constipation. (C) Per cent prevalence of abnormal balloon sensation tests (in red) denoting impaired rectal sensation. (D) Percentage of patients with absent rectoanal inhibitory reflex (in red), suggestive of impaired rectoanal coordination. EAS, external anal sphincter; HRAM, high-resolution anorectal manometry; IAS, internal anal sphincter.
Classification of dyssynergia
Of the 66 patients with chronic constipation, 9 patients (14%) had normal defaecatory coordination, based on HRAM. Except for one, these patients were also noted to have normal BET (see above). Among the remaining 57 patients with dyssynergia, type II dyssynergia was the most common (n=27, 41%), followed by type IV (n=26, 39%), type III (n=4, 6%). There were no patients with type I dyssynergia (figure 5). Overall, 59 of the study patients (89%) exhibited significantly abnormal HRAM or BET parameters and features suggestive of defaecatory dyssynergia (figure 1). There was no relationship between any HRAM abnormalities and the Hoehn and Yahr scores or disease duration.
Figure 5.
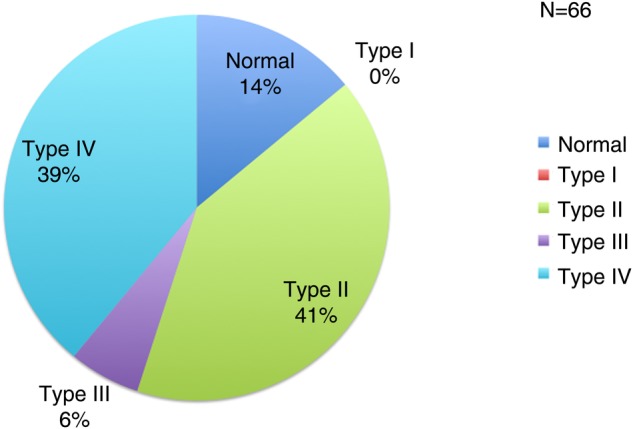
Pie chart highlighting the prevalence of defaecatory dyssynergia types (I–IV) in the PD cohort studied by HRAM. HRAM, high-resolution anorectal manometry; PD, Parkinson's disease.
Colonic transit time
Of the 66 study patients, 5 could not swallow the motility capsule, 4 had technical issues not allowing computing of the regional transit times and 4 could not get insurance authorisation. Therefore, only 53 patients underwent a WMC. Of these, 20 (38%) had normal CTT with median time of 43 hours (95% CI 38.32 to 45.00). In the 33 patients (62% of the cohort) with prolonged transit, the median CTT was 84.5 hours (95% CI 71.99 to 87.00; figure 6). Overall, 38 patients (57% of the total) exhibited overlapping features of dyssynergia and slow transit constipation (figure 1). There was no correlation between Hoehn and Yahr scores or disease duration and CTT. These results are not surprising since constipation in PD might be ‘early’ manifestation of PD due to increased α-synuclein in the enteric nervous system (ENS). However, there was a significant relationship between constipation scores and CTT (Pearson correlation 0.32, p value 0.01; figure 7).
Figure 6.

Box plot graphs highlighting the CTT (hours) defined by WMC. The 53 patients studied were separated into normal (CTT<59 hours) and abnormal (CTT>59 hours) groups. The plots display the distribution of data as: minimum (bottom whisker), first quartile (lower part of box), median (line in box), third quartile (upper part of box), and maximum (top whisker). CTT, colonic transit time; WMC, wireless motility capsule.
Figure 7.
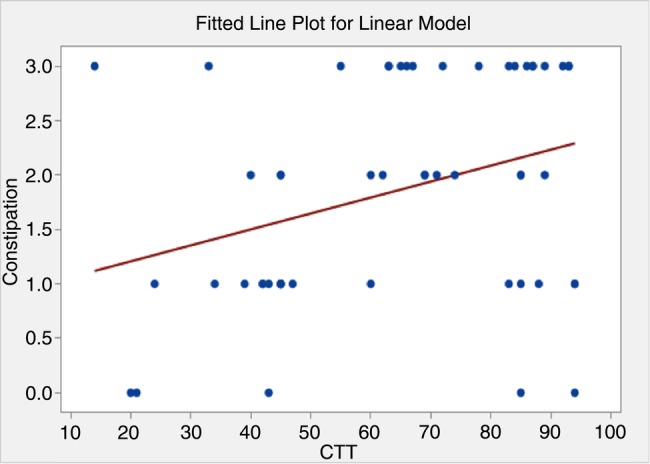
Fitted linear plot depicting the relationship between CTT and constipation scores. A significant relationship between constipation scores and CTT was found. CTT, colonic transit time.
Discussion
The aim of our study was to determine any clinical utility in performing HRAM, BET and WMC in patients with PD and chronic constipation. Using these modern day clinical tools, we have demonstrated that the majority of these patients (89%) have defaecatory dyssynergia (mainly types II and IV), 62% have slow transit constipation and 57% have overlap constipation. Obviously, these results have therapeutic implications, since different targeted therapies can be applied, alone or in combination, for each patient.
The pathophysiology of chronic constipation in PD is complex and difficult to decipher without the use of specialised tests like the ones used in this study. One mechanism, as shown here as well as in other studies, is prolonged colon transit time.19 Another is defaecatory dyssynergia, or paradoxical contraction of the striated anal sphincter muscles and/or puborectalis during defaecation, and associated, depending on the type (I–IV) with normal or weak rectal contraction;20 this seems—in our study—to be the most prevalent abnormality. Our data also suggest that poor rectal sensation and lacking rectoanal inhibitory reflex, both suggestive of autonomic and ENS neuropathy, may play a role in 12–30% of cases, frequently coexisting with anorectal motor dystonia and slow transit constipation. It remains unclear whether rectal hyposensitivity is causative or secondary to neurological or biomechanical dysfunction and its clinical impact still needs to be defined.21 22 Constipation may also reflect an adverse effect of the drugs that almost universally used in PD, such as anticholinergics and dopaminergic agents.23 The coexistence of symptoms, such as infrequent evacuation, straining at defaecation and a sense of incomplete rectal emptying, suggest that more than one mechanism involved.24
Hence, targeting therapy in patients found to have specific abnormalities might be more successful. In our study, for example, patients with PD with slow transit constipation were treated with osmotic laxatives, lubiprostone or linaclotide, those with dyssynergia were treated with biofeedback and pelvic floor exercises, while many patients were treated with both modalities. Such therapies, however, were not formally assessed as part of our study given its retrospective nature and the lack of standardisation of the end points for each therapy. Prospective trials will be needed in order to examine the impact of such targeted approaches in patients with PD with chronic constipation further characterised by HRAM and WMC, in comparison with those patients who remain undifferentiated and empirically treated. Given the multitude of motor and sensory abnormalities noted in our study, such trials will be challenging, since many patients may require multiple interventions (ie, prucalopride for slow transit constipation, BoTox injection of the anal sphincter for anismus or loperamide for faecal incontinence, among others). Furthermore, proper instruments to accurately assess the therapeutic response (or lack thereof) in the PD population will need to be developed. In general, dietary fibre is not well tolerated by patients with slow transit constipation and is unlikely to be useful in most patients with PD and since rectal sensation is frequently preserved, bulking with fibre—aimed at improving rectal sensation—may not be needed. Osmotic laxatives, linaclotide, lubiprostone, and particularly prucalopride, could be useful in the treatment of slow transit constipation in PD, since they shorten CTT. Patients with PD with absent recto-anal inhibitory reflex (RAIR) may need programmed defaecation. On the other hand, biofeedback therapy should be tried in patients with PD who are so often troubled by defaecatory dyssynergia, but its efficacy and practical utility is unknown. Since many patients with PD with constipation have low anal sphincter pressures, the occurrence of faecal incontinence may be the limiting variable in the overall management.25
There are several strengths and weaknesses in our study. First, since our analysis was conducted in a community-based cohort, its findings could be applicable to the general population with PD and constipation. There have been no previous studies in patients with PD exploring the roles of HRAM, BET and WMC; hence, the data from these analyses could serve as preliminary elements and a launching pad in our further understanding of the relationship between the disease and its gut manifestations. Second, the study carefully excluded selection bias by first clinically assessing an entire PD cohort and then proving that the patients studied were similar to those with constipation who were not. Third, the performance of HRAM and WMC led in many patients not only to a specific diagnosis but also therapy theretofore unavailable (ie, BoTox injection of the anal sphincter). However, the retrospective nature of our study does not allow us to reflect on the impact and true benefit of the treatments applied be it pharmacological, biofeedback or endoscopic. Fourth, inherent limitations of the WMC in assessing CTT (ie, due to unidentifiable pH landmarks) or of the HRAM and BET in assessing dyssynergia (ie, due to non-physiological positioning, or abdominal muscle weakness) could have challenged their validity. Such scenarios were noted in our cohort but their impact is difficult to quantify.8 26 It has also been recently shown that although the various HRAM patterns are reproducible, they may be seen in healthy volunteers, questioning its overall utility in functional constipation.6 Fifth, we did not perform endoanal ultrasound to examine sphincter integrity and such possibility cannot be excluded as a reason for faecal incontinence in some of our patients. Finally, our study design did not allow us to detect any changes in the variables examined over time or in the absence of PD therapies. Given the clinical impact that drug discontinuation would have on the patients' neurological function and mobility, it would have been unethical to even transiently disrupt continuous therapy. Therefore, our data should be considered as reflecting optimised PD control using currently available therapies and additional strategies would need to be implemented if we were to expect a favourable therapeutic impact on the gut manifestations.
In conclusion, chronic constipation in patients with PD may reflect underlying defaecatory dyssynergia, slow transit constipation or both. Clinical symptoms are not discriminatory and functional testing using HRAM, BET and WMC may be beneficial in further characterising such patients.
Footnotes
Contributors: AS and GT were involved in planning and conducting the study; all authors were involved in collecting and interpreting the data, drafting the manuscript and revision.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Ethics approval: Stanford Institutional Review Board (IRB).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: No additional data are available.
References
- 1.Fasano A, Visanji NP, Liu LW, et al. . Gastrointestinal dysfunction in Parkinson's disease. Lancet Neurol 2015;14:625–39. doi:10.1016/S1474-4422(15)00007-1 [DOI] [PubMed] [Google Scholar]
- 2.Metcalf AM, Phillips SF, Zinsmeister AR, et al. . Simplified assessment of segmental colonic transit. Gastroenterology 1987;92:40–7. doi:10.1016/0016-5085(87)90837-7 [DOI] [PubMed] [Google Scholar]
- 3.Rao SS. Advances in diagnostic assessment of fecal incontinence and dyssynergic defecation. Clin Gastroenterol Hepatol 2010;8:910–19. doi:10.1016/j.cgh.2010.06.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mukherjee A, Biswas A, Das SK. Gut dysfunction in Parkinson's disease. World J Gastroenterol 2016;22:5742–52. doi:10.3748/wjg.v22.i25.5742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rao SS, Camilleri M, Hasler WL, et al. . Evaluation of gastrointestinal transit in clinical practice: position paper of the American and European neurogastroenterology and motility societies. Neurogastroenterol Motil 2011;23:8–23. doi:10.1111/j.1365-2982.2010.01612.x [DOI] [PubMed] [Google Scholar]
- 6.Grossi U, Carrington EV, Bharucha AE, et al. . Diagnostic accuracy study of anorectal manometry for diagnosis of dyssynergic defecation. Gut 2016;65:447–55. doi:10.1136/gutjnl-2014-308835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kuo B, McCallum RW, Koch KL, et al. . Comparison of gastric emptying of a nondigestible capsule to a radio-labelled meal in healthy and gastroparetic subjects. Aliment Pharmacol Ther 2008;27:186–96. doi:10.1111/j.1365-2036.2007.03564.x [DOI] [PubMed] [Google Scholar]
- 8.Rao SS, Kuo B, McCallum RW, et al. . Investigation of colonic and whole-gut transit with wireless motility capsule and radiopaque markers in constipation. Clin Gastroenterol Hepatol 2009;7:537–44. doi:10.1016/j.cgh.2009.01.017 [DOI] [PubMed] [Google Scholar]
- 9.Bharucha AE, Wald A, Enck P, et al. . Functional anorectal disorders. Gastroenterology 2006;130:1510–18. doi:10.1053/j.gastro.2005.11.064 [DOI] [PubMed] [Google Scholar]
- 10.Lacy BE, Mearin F, Chang L, et al. . Bowel disorders. Gastroenterology 2016;150:1393–407. [DOI] [PubMed] [Google Scholar]
- 11.Goetz CG, Poewe W, Rascol O, et al. . Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord 2004;19:1020–8. doi:10.1002/mds.20213 [DOI] [PubMed] [Google Scholar]
- 12.Rosa-E-Silva L, Gerson L, Davila M, et al. . Clinical, radiologic, and manometric characteristics of chronic intestinal dysmotility: the Stanford experience. Clin Gastroenterol Hepatol 2006;4:866–73. doi:10.1016/j.cgh.2006.05.001 [DOI] [PubMed] [Google Scholar]
- 13.Saad RJ. The wireless motility capsule: a one-stop shop for the evaluation of GI motility disorders. Curr Gastroenterol Rep 2016;18:14 doi:10.1007/s11894-016-0489-x [DOI] [PubMed] [Google Scholar]
- 14.Rao SS, Patcharatrakul T. Diagnosis and treatment of dyssynergic defecation. J Neurogastroenterol Motil 2016;22:423–35. doi:10.5056/jnm16060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee HJ, Jung KW, Han S, et al. . Normal values for high-resolution anorectal manometry/topography in a healthy Korean population and the effects of gender and body mass index. Neurogastroenterol Motil 2014;26:529–37. doi:10.1111/nmo.12297 [DOI] [PubMed] [Google Scholar]
- 16.Minguez M, Herreros B, Sanchiz V, et al. . Predictive value of the balloon expulsion test for excluding the diagnosis of pelvic floor dyssynergia in constipation. Gastroenterology 2004;126:57–62. doi:10.1053/j.gastro.2003.10.044 [DOI] [PubMed] [Google Scholar]
- 17.Rao SS. Dyssynergic defecation and biofeedback therapy. Gastroenterol Clin North Am 2008;37:569–86. doi:10.1016/j.gtc.2008.06.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rao SS, Mudipalli RS, Stessman M, et al. . Investigation of the utility of colorectal function tests and Rome II criteria in dyssynergic defecation (anismus). Neurogastroenterol Motil 2004;16:589–96. doi:10.1111/j.1365-2982.2004.00526.x [DOI] [PubMed] [Google Scholar]
- 19.Jost WH, Schrank B. Defecatory disorders in de novo Parkinsonians—colonic transit and electromyogram of the external anal sphincter. Wien Klin Wochenschr 1998;110:535–7. [PubMed] [Google Scholar]
- 20.Bassotti G, Maggio D, Battaglia E, et al. . Manometric investigation of anorectal function in early and late stage Parkinson's disease. J Neurol Neurosurg Psychiatr 2000;68:768–70. doi:10.1136/jnnp.68.6.768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Burgell RE, Scott SM. Rectal hyposensitivity. J Neurogastroenterol Motil 2012;18:373–84. doi:10.5056/jnm.2012.18.4.373 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wang CP, Sung WH, Wang CC, et al. . Early recognition of pelvic floor dyssynergia and colorectal assessment in Parkinson's disease associated with bowel dysfunction. Colorectal Dis 2013;15:e130–7. doi:10.1111/codi.12105 [DOI] [PubMed] [Google Scholar]
- 23.Pagano G, Tan EE, Haider JM, et al. . Constipation is reduced by beta-blockers and increased by dopaminergic medications in Parkinson's disease. Parkinsonism Relat Disord 2015;21:120–5. doi:10.1016/j.parkreldis.2014.11.015 [DOI] [PubMed] [Google Scholar]
- 24.Krogh K, Christensen P. Neurogenic colorectal and pelvic floor dysfunction. Best Pract Res Clin Gastroenterol 2009;23:531–43. doi:10.1016/j.bpg.2009.04.012 [DOI] [PubMed] [Google Scholar]
- 25.Jost WH. Gastrointestinal dysfunction in Parkinson's disease. J Neurol Sci 2010;289:69–73. doi:10.1016/j.jns.2009.08.020 [DOI] [PubMed] [Google Scholar]
- 26.Soh JS, Lee HJ, Jung KW, et al. . The diagnostic value of a digital rectal examination compared with high-resolution anorectal manometry in patients with chronic constipation and fecal incontinence. Am J Gastroenterol 2015;110:1197–204. doi:10.1038/ajg.2015.153 [DOI] [PubMed] [Google Scholar]