

Abstract
Femoral neck stress fractures have been described in military recruits and athletes. Early recognition and aggressive treatment are important, as femoral neck stress fractures have a high potential for complications and even uncomplicated fractures require an extensive course of rehabilitation. Tension-side (superolateral) stress fractures of the femoral neck are at high risk for complications such as displacement, non-union and avascular necrosis, and need to be treated surgically, while compression-side (inferomedial) fractures can be treated conservatively. We describe a case illustrating a typical presentation of insidious hip pain culminating in sudden onset of severe hip pain in a healthy young man. We perform a literature review of studies showing epidemiology, treatment algorithms and rehabilitation.
Background
Stress fractures resulting from prolonged training among military recruits were first described in the 1800s as ‘march fractures’.1 2 With the advent of running as a leisure-time activity, these fractures were increasingly recognised in the running athlete as well. Prevention, early recognition and expedited treatment are important in preventing the high risk of complications and financial burden of rehabilitation.
Case presentation
The patient is a man aged 27 years who presented with sudden-onset left hip pain that began during a physical training session. The pain was severe, forcing him to be carried out of the session. Approximately 1 month prior to presentation, he had noticed some non-specific pain in the left hip area, which began after a hiatus from physical activity following elective arthroscopic knee surgery. After rehabilitation following the surgery, he had resumed an aggressive running and conditioning programme. The initial low-intensity non-specific hip pain had resolved completely after decreasing his running volume. He denied any associated numbness, tingling, swelling or weakness. He had no prior history of stress fracture. There was no pertinent family or medical history.
Investigations
On physical examination, he was 172 cm and 78 kg with a BMI of 26 and normal vital signs. He was able to weight-bear on his left leg with pain reproduced on walking. Lower extremity strength, sensory and reflex exams were intact and unremarkable. Range of motion of the hip and knee was intact. There was pain with resisted hip flexion, minimal pain with the FADIR (Flexion Adduction Internal Rotation) test and no pain with the FABER (Flexion Abduction External Rotation) test. There was no pain with the log-roll manoeuvre.
Differential diagnosis
Given the sudden onset of severe pain with activity, stress fracture of the hip was the presumed diagnosis. Differential diagnoses included hip labral tear, hip avascular osteonecrosis and less likely hip flexor tendinitis, hip bursitis and lumbar radiculopathy.
X-ray of the left hip in the anterior–posterior and lateral views showed no fractures or dislocations, with slight overhang of the femoral head–neck junction laterally consistent with CAM-type deformity. An acute labral tear was thought unlikely to be the cause of the patient's symptoms, given that pain was reproducible with weight-bearing, there was normal hip range of motion and minimal pain reproduction with FADIR and FABER.
An MRI of the pelvis demonstrated moderate marrow oedema surrounding a linear hypointense area of T1 and T2 signal abnormality on the left, consistent with a non-displaced compression-type posterior femoral neck stress fracture (figure 1).
Figure 1.
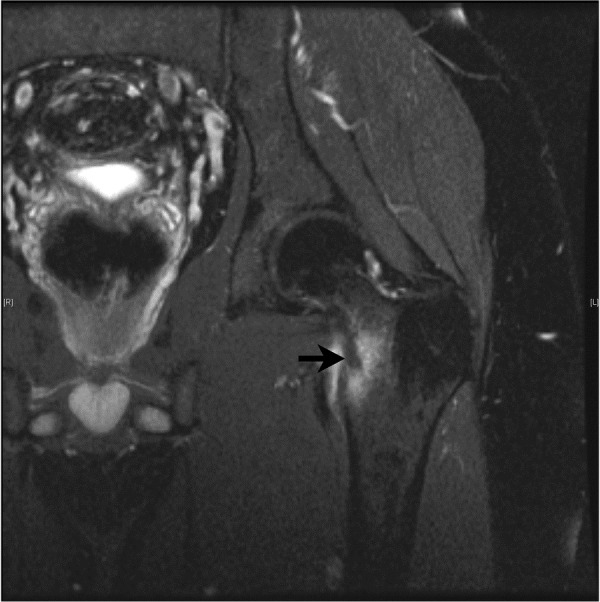
MRI of the left hip demonstrating moderate marrow oedema surrounding a linear hypointense area of T1 and T2 signal abnormality consistent with a non-displaced compression-type posterior femoral neck stress fracture.
Treatment
The patient was treated with strict non-weight-bearing status, ambulating with bilateral crutches for 1 month, followed by graduated return to activity. Since his fracture was non-displaced and located in the inferior–posterior region of the femoral neck (compression-type), surgical fixation was not indicated.
Outcome and follow-up
The patient had good compliance with the non-weight-bearing treatment and no complications during his convalescence. Hip pain had resolved completely in follow-up ∼4 months later. He returned to running up to 10 miles/day, four times per week as well as fully participating in the physical training required by his occupation.
Discussion
Stress fractures of the femoral neck have been described extensively in the runner as well as military recruit population. They occur in ∼10% of all stress fractures.3–6 The pain has been described as presenting typically in the anterior thigh or hip with weight-bearing;2 4 7 however, cases of primarily buttock pain8 as well as asymptomatic cases have also been noted.9 On physical examination, the pain is most often reproduced with internal rotation and passive range of motion at the hip. As with many stress fractures, a positive hop test3 warrants more aggressive workup and treatment, and is positive in at least 70% of radiologically confirmed stress fractures.4
A high degree of suspicion for stress fracture should be maintained after sudden increases or changes in training volume. The onset of fractures after increases in training (such as occurring with military recruit training) has been variably described at 4–5,10 4–711 up to 13–16 weeks,6 and also with even distribution throughout training.1 3 5 11 12 The sudden return to normal training load after hiatus for elective surgery is the presumed aetiological factor in the case of our patient.
At-risk populations include the amenorrhoeic female, patients with prior stress fractures and patients with medical history predisposing to fracture (such as osteopenia, malabsorption, steroid use).13 Risk for development of additional stress fractures is high (10% within 1 year) likely secondary to the underlying risk factors that contributed to initial injury.14
Imaging evaluation of the patient presenting with clinical suspicion of stress fracture should begin with plain radiography of the hip to rule out other underlying bony pathology. X-rays by themselves are insufficient to assess for acute fractures as they are sensitive in only ∼7% of lesions on initial presentation.3 10 Technetium-99m bone scans are sensitive and able to show increased bone turn-over within days of onset. However, the site of increased radionucleotide uptake is non-specific, and cannot differentiate stress reaction or fracture from infection or tumour. Bone scans also pose a radiation dose risk and should be used judiciously, especially in women of childbearing age. Thus, MRI of the hip is the imaging test of choice in a patient with clinical suspicion of stress fracture. MRI imaging approaches 100% sensitivity, and can rule out other differential pathology of the bone, joint and soft tissues, and labrum. On MRI, a stress response or stress reaction is represented by intramedullary low T1 signal and increased T2 signal with marrow enhancement representing marrow oedema; whereas, a stress fracture shows linear low T1 and low T2 signal intensity through the cortex representing a fracture line.10
Early suspicion and treatment with non-weight-bearing status is important in reducing complications and delayed rehabilitation. Our patient exemplifies a typical presentation of delayed diagnosis in which a persistent low-grade pain suddenly becomes severe with findings of a fracture line.
Tension-type fractures (superior–lateral femoral neck) carry a high risk of displacement and non-union; therefore, surgical fixation with percutaneous nail fixation is the treatment of choice.1 Despite surgical intervention, there is still a high risk of non-union and avascular necrosis of the femoral head.11 Compression-type fractures (inferior femoral neck) can be treated conservatively with non-weight-bearing and graduated return to activity.
Femoral neck stress fractures overall are associated with a prolonged rehabilitation course and extended absence from sports and active military duty. An average convalescence has been described as 116 days12 or three times longer than that for other lower extremity stress fractures.15 In a study of 220 stress fractures in military recruits, femoral stress fractures healed the slowest, needing a mean time of 21.1 weeks for rehabilitation.1 Femoral neck stress fractures have been shown to result in medical military discharge in 40% of cases.6 These fractures are also associated with significantly increased medical costs. The US military estimates a cost of $100 000 per case.15
Our case shows that close vigilance and a high degree of suspicion should be maintained in all cases of hip pain, including healthy young men involved in intense physical activity.
Learning points.
Femoral neck stress fractures are fairly common and often occur in athletes without typical risk factors for stress fractures such as the female athlete triad or other known disorders of bone metabolism.
Early diagnosis is key to preventing prolonged rehabilitation.
Plain film X-rays are insufficient for early diagnosis and MRI imaging may be required.
Tension-type fractures carry a high risk of displacement and non-union and surgical fixation is treatment of choice.
Compression-type fractures require aggressive non-weight-bearing treatment to prevent poor outcomes.
Footnotes
Contributors: All authors contributed a significant amount to the data collection, write-up and editing of the article. SG, AS and MKP collected initial data including history, examination and imaging. SG and ZP obtained patient consent. ZP wrote the initial document version, which was edited by SG, AS and MKP. Final version was agreed on and vetted by ZP, AS, SG and MKP.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Wood AM, Hales R, Keenan A et al. Incidence and time to return to training for stress fractures during military basic training. J Sports Med 2014;2014:282980 10.1155/2014/282980 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.McCormick F, Nwachukwu BU, Provencher MT. Stress fractures in runners. Clin Sports Med 2012;31:291–306. 10.1016/j.csm.2011.09.012 [DOI] [PubMed] [Google Scholar]
- 3.Matheson GO, Clement DB, McKenzie DC et al. Stress fractures in athletes. A study of 320 cases. Am J Sports Med 1987;15:46–58. 10.1177/036354658701500107 [DOI] [PubMed] [Google Scholar]
- 4.Clement DB, Ammann W, Taunton JE et al. Exercise-induced stress injuries to the femur. Int J Sports Med 1993;14:347–52. 10.1055/s-2007-1021191 [DOI] [PubMed] [Google Scholar]
- 5.Milgrom C, Giladi M, Stein M et al. Stress fractures in military recruits. A prospective study showing an unusually high incidence. J Bone Joint Surg Br 1985;67:732–5. [DOI] [PubMed] [Google Scholar]
- 6.Talbot JC, Cox G, Townend M et al. Femoral neck stress fractures in military personnel—a case series. J R Army Med Corps 2008;154:47–50. 10.1136/jramc-154-01-13 [DOI] [PubMed] [Google Scholar]
- 7.Harrast MA, Colonno D. Stress fractures in runners. Clin Sports Med 2010;29:399–416. 10.1016/j.csm.2010.03.001 [DOI] [PubMed] [Google Scholar]
- 8.Scott MP, Finnoff JT, Davis BA. Femoral neck stress fracture presenting as gluteal pain in a marathon runner: case report. Arch Phys Med Rehabil 1999;80:236–8. 10.1016/S0003-9993(99)90127-2 [DOI] [PubMed] [Google Scholar]
- 9.Finestone AS, Glatstein M, Novack V et al. The completely asymptomatic displaced femoral stress fracture: a case report and review of the literature. Mil Med 2006;171:37–9. 10.7205/MILMED.171.1.37 [DOI] [PubMed] [Google Scholar]
- 10.Wall J, Feller JF. Imaging of stress fractures in runners. Clin Sports Med 2006;25:781–802. 10.1016/j.csm.2006.06.003 [DOI] [PubMed] [Google Scholar]
- 11.Joshi A, Kc BR, Shah BC et al. Femoral neck stress fractures in military personnel. J Nepal Med Assoc 2009;48:99–102. [PubMed] [Google Scholar]
- 12.Sharma J, Greeves JP, Byers M et al. Musculoskeletal injuries in British Army recruits: a prospective study of diagnosis-specific incidence and rehabilitation times. BMC Musculoskelet Disord 2015;16:106 10.1186/s12891-015-0558-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cody JP, Evans KN, Kluk MW et al. Occult femoral neck fracture associated with vitamin D deficiency diagnosed by MRI: case report. Mil Med 2012;177:605–8. 10.7205/MILMED-D-11-00321 [DOI] [PubMed] [Google Scholar]
- 14.Giladi M, Milgrom C, Kashtan H et al. Recurrent stress fractures in military recruits. One-year follow-up of 66 recruits. J Bone Joint Surg Br 1986;68:439–41. [DOI] [PubMed] [Google Scholar]
- 15.Scott SJ, Feltwell DN, Knapik JJ et al. A multiple intervention strategy for reducing femoral neck stress injuries and other serious overuse injuries in U.S. Army Basic Combat Training. Mil Med 2012;177:1081–9. [DOI] [PubMed] [Google Scholar]