

Abstract
Aim of database
The aim of the National Database of Geriatrics is to monitor the quality of interdisciplinary diagnostics and treatment of patients admitted to a geriatric hospital unit.
Study population
The database population consists of patients who were admitted to a geriatric hospital unit. Geriatric patients cannot be defined by specific diagnoses. A geriatric patient is typically a frail multimorbid elderly patient with decreasing functional ability and social challenges. The database includes 14–15,000 admissions per year, and the database completeness has been stable at 90% during the past 5 years.
Main variables
An important part of the geriatric approach is the interdisciplinary collaboration. Indicators, therefore, reflect the combined efforts directed toward the geriatric patient. The indicators include Barthel index, body mass index, de Morton Mobility Index, Chair Stand, percentage of discharges with a rehabilitation plan, and the part of cases where an interdisciplinary conference has taken place. Data are recorded by doctors, nurses, and therapists in a database and linked to the Danish National Patient Register.
Descriptive data
Descriptive patient-related data include information about home, mobility aid, need of fall and/or cognitive diagnosing, and categorization of cause (general geriatric, orthogeriatric, or neurogeriatric).
Conclusion
The National Database of Geriatrics covers ∼90% of geriatric admissions in Danish hospitals and provides valuable information about a large and increasing patient population in the health care system.
Keywords: quality, research, geriatrics, interdisciplinary, Denmark
Name of database
The name of the database is the National Database of Geriatrics (NDG). Founded in 1998, the database started out as a local development project in the capital area. In 2005, the database became nationwide, although not all geriatric units in Denmark started reporting immediately. In 2015, all geriatric units treating admitted patients, except one, reported data to the database. Figure 1 shows the 23 Danish geriatric hospital units.
Figure 1.
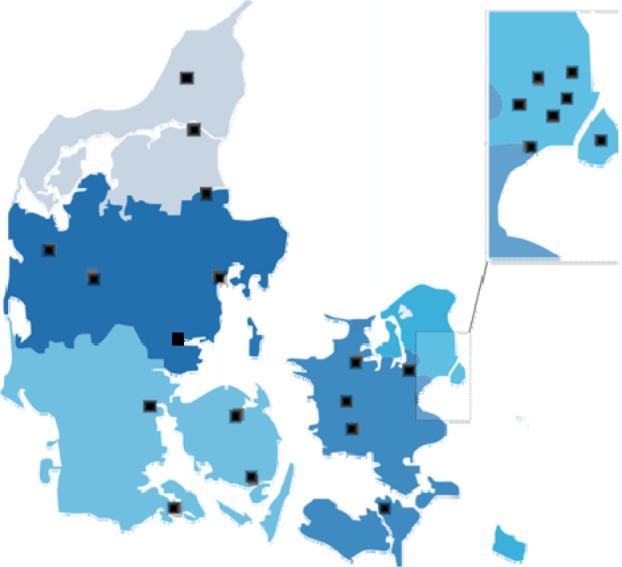
Geriatric units in Denmark (marked with black squares).
The aim of this article is to inform the reader about the Danish effort to monitor the quality of services in the geriatric field.
Aim of database
The aim of the NDG is to monitor the quality of interdisciplinary diagnostics and treatment of patients admitted to a geriatric hospital unit.
In addition to the diagnosing and treatment of elderly patients’ acute and chronic illnesses, the aim of geriatric intervention is to reestablish and advance the patients’ functional abilities. Comprehensive Geriatric Assessment (CGA) is an indispensable tool for doing just that.1 CGA is a systematic evaluation of the patient’s resources and disabilities (both physical and mental in combination with the social situation) and is carried out in every geriatric unit nationwide. The database is dedicated to ensuring that all geriatric patients in Denmark are provided the same access to the health care system and that the quality of the treatment in the geriatric units is characterized by the same high quality.
A secondary aim of the database is to monitor the number and distribution of geriatric units in Demark and the extent of interdisciplinary cooperation in each unit. Interdisciplinary cooperation is a condition of practicing CGA.
Study population
The database population consists of those patients who were admitted to a geriatric hospital unit. In 2014, the population accounted 14,648 admissions.2 Since the beginning of the database, data concerning >103,000 admissions have been reported.2 The outpatient treatment activity is not reported, neither is data concerning the many elderly patients not admitted to a geriatric unit although some may have benefited from that. Geriatric units are found throughout Denmark (Figure 1).
Data are collected and registered online in special data forms programmed in the quality measurement system (QMS) by TietoEnator. Further data regarding the registered admissions are extracted from the Danish National Patient Register (NPR).
Data are validated every year when the annual report is produced. All units reporting to the database are required to check their own data in the report and to report back to the steering committee and the competency center if data/results are incorrect.
The NDG is currently working on a development project. In Danish hospitals, a large number of patients with acute symptoms are admitted through the emergency department, which covers all types of acute symptoms, not only injuries. The aim of this project is to define a population of frail multimorbid elderly patients with acute admission to the hospital but not necessarily admitted to the geriatric unit in order to be able to monitor the quality of care in this patient population.
Main variables
Since the beginning of the recording of data, there has been an ongoing adjustment and development of the clinical indicators. Some have been excluded, some enrolled, and others adjusted. This has been a natural consequence of the continuous structural development in the health care system.
A very important part of the geriatric approach is the interdisciplinary collaboration. Indicators, therefore, reflect the combined efforts directed toward the geriatric patient. This effort is provided by both specialists in geriatric medicine; nurses; physical and occupational therapists, who constitute the core of the interdisciplinary effort; as well as other staff groups affiliated with the geriatric units (dieticians, pharmaconomists, social workers, priests, etc). The interdisciplinarity is also reflected in the composition of the steering committee.
Obtaining data from independent geriatric units is not a problem although it requires updated lists of the units’ specific classification code. In some hospitals, the geriatric unit is a part of a large medical unit. Traditionally, it has been problematic to obtain data from these large medical units. During recent years, there has been an increasing focus on this challenge and the steering committee has focused on several factors in an attempt to solve the problem (correct coding, ensuring available interdisciplinary staff delivering the CGA, etc).
The frail multimorbid elderly patient is, when hospitalized, characterized by acute illness in combination with one or more chronic diseases. The situation is often further complicated by decreasing functional ability and social challenges. The indicators listed in Table 1 reflect this multifaceted issue.
Table 1.
A list of quality indicators in the National Database of Geriatrics
| Number | Name of indicator | Data source | Standard |
|---|---|---|---|
| 1a | Proportion of admissions with measurement of Barthel score | Database | >90% |
| 1b | Proportion of admissions ≥7 days with improvement of Barthel score during admission | Database | ND |
| 1b1 | Proportion of general geriatric admissions ≥7 days with improvement of Barthel score during admission | Database | ND |
| 1b2 | Proportion of orthogeriatric admissions ≥77 days with improvement of Barthel score during admission | Database | ND |
| 1b3 | Proportion of neurogeriatric admissions ≥77 days with improvement of Barthel score during admission | Database | ND |
| 2 | Proportion of admissions with measurement of BMI | Database | >90% |
| 3 | Proportion of admissions with measurement of DEMMI | Database | ND |
| 4a | Proportion of admissions with registration of Chair Stand function | Database | >80% |
| 4b | Proportion of admissions ≥77 days with improvement of Chair Stand function during admission | Database | >80% |
| 4b1 | Proportion of general geriatric admissions ≥77 days with improvement of Chair Stand function during admission | Database | ND |
| 4b2 | Proportion of orthogeriatric admissions ≥77 days with improvement of Chair Stand function during admission | Database | ND |
| 4b3 | Proportion of neurogeriatric admissions ≥77 days with improvement of Chair Stand function during admission | Database | ND |
| 5 | Proportion of discharges with a rehabilitation plan for municipal rehabilitation | Database + NPR | ND |
| 5a | Proportion of general geriatric discharges with a rehabilitation plan for municipal rehabilitation | Database + NPR | ND |
| 5b | Proportion of orthogeriatric discharges with a rehabilitation plan for municipal rehabilitation | Database + NPR | ND |
| 5c | Proportion of neurogeriatric discharges with a rehabilitation plan for municipal rehabilitation | Database + NPR | ND |
| 6 | Proportion of discharges with registration of an interdisciplinary conference during admission | Database + NPR | ND |
| 6a | Proportion of general geriatric discharges with registration of an interdisciplinary conference during admission | Database + NPR | ND |
| 6b | Proportion of orthogeriatric discharges with registration of an interdisciplinary conference during admission | Database + NPR | ND |
| 6c | Proportion of neurogeriatric discharges with registration of an interdisciplinary conference during admission | Database + NPR | ND |
Abbreviations: ND, not determined; BMI, body mass index; DEMMI, de Morton Mobility Index; NPR, Danish National Patient Register.
The data from the NDG are presented in an annual report, which consists of two parts: the organizational data and the patient-related data. The latter encompasses the following: Barthel index,3,4 body mass index,5 de Morton Mobility Index (DEMMI),6,7 Chair Stand,8 home, mobility aid, need of fall and/or cognitive diagnosing, and categorization of cause (general geriatric, orthogeriatric, or neurogeriatric). The report also includes data on the percentage of discharges with a rehabilitation plan and the part of cases where an interdisciplinary conference has taken place.2
Database completeness is defined as the number of geriatric patients reported to the database/the number of patients discharged from the geriatric units in the same period. Identification of geriatric patients in the NPR is not possible as the patients cannot be identified by specific diagnosis, procedures, or organizational geriatric units. Computation of completeness in the database therefore relies on information from the units treating geriatric patients, regarding the number of geriatric patients discharged during the relevant period. During the last few years, the database completeness has reached 90%, which is the standard requirement for national clinical databases. Owing to technical problems with the procedure of incident reporting in 2014, the database completeness was just below the requirement.2
The length of stay (LOS) in a geriatric unit is decreasing, which is a challenge for a number of the indicators. Showing an improvement in the functional level, eg, in the Barthel index or physical performance (eg, DEMMI), is increasingly difficult in regard to the very short LOS in a majority of the Danish geriatric units. Despite lower LOS, it is still possible to demonstrate an improvement of, eg, Barthel index in 70% of the patients with an LOS of at least 7 days.2
An indicator still in the phase of implementation is the DEMMI test. The process of implementation started with the introduction of the test as a replacement of the Timed Up and Go (TUG) test9 for measurement of physical performance. Replacing the Timed Up and Go test was necessary because the functional status of the admitted geriatric patients has deteriorated over the years making it impossible to test the patients with this test. In 2013, the DEMMI test was optional to use, but in 2014, it became obligatory on a national level. Approximately 46% of the patients are evaluated on admission with the DEMMI test; large regional differences are evident.2 The reporting to the database is functioning as a driver of implementation.
With the municipal reform in 2007, parts of what was earlier included in the in-hospital geriatric intervention are now the responsibility of the municipalities, eg, rehabilitation. In Denmark, the rehabilitation is initiated during hospitalization and continues in the primary sector after discharge. This calls for indicators that reflect that the geriatric intervention is not restricted to the geriatric hospital unit but takes place prior to the admission as well as continues after the discharge (Figure 2).
Figure 2.

The geriatric effort.
Notes: Illustration of the present state and future goals of the National Database of Geriatrics. At present, the register covers the geriatric effort in the geriatric hospital units. The future ambition is to monitor the efforts both before and after an admission in a geriatric unit and to monitor all frail multimorbid elderly patients admitted to the hospital through an emergency department.
Future adjustment of the set of indicators has to take into account that the LOS might decrease even further, and, therefore, has to concentrate around the sector transfers to ensure that the geriatric intervention and quality of it continue beyond the borders of the geriatric unit. Likewise, it is the aim of the steering committee to include indicators that can display the interdisciplinary approach to the geriatric patient in an even clearer light; in the near future, a specific indicator for the intervention of the occupational therapist is expected.
To ease the burden of incident reporting, efforts are being made to make data extracts from the NPR possible. As mentioned earlier, the geriatric patients cannot be identified directly in the NPR. The geriatric population is therefore defined as the geriatric admissions reported in the QMS database. Identification of the correct admission in the NPR corresponding to the admission reported in the QMS database is not straightforward, and data extracts from NPR are therefore not complete compared to the database. In 2014, 97% of the admissions registered in the database could be matched to an admission in the NPR.
Follow-up
Periodic assessments of the quality indicators are made and published on a quarterly basis in the regional information systems. The clinical units can access their own results to ensure both real-time registration and the opportunity to make usage of own results for the further development and quality assurance in the units, respectively. Each unit has access to their own data at any time, but it is also possible to request a specific data extract from the steering committee. Likewise, it is possible to apply for data relevant to a specific study.
The steering committee is continually in contact with contact persons for the database in all geriatric units and sends out a newsletter following every meeting. Once a year, the steering committee organizes a meeting just before the report is presented in its final form, where it is possible to discuss the preliminary results or other relevant problems in working with the database. This is part of the communication strategy for the database.
Examples of research
The steering committee has carried out a pilot study regarding the intersectorial effort. In cooperation with a few pilot municipalities, the subject of interest of the pilot study was to examine how many of the rehabilitation plans produced in the geriatric unit were actually carried out in primary health care and when the rehabilitation began. A future hope for the data comprising this database is that they will be used for clinical research. Until now, the studies have been few. At present, a study concerning readmission of geriatric patients is carried out. Furthermore, a study in progress regards the active geriatric patient, a study to ensure patient empowering and strengthening of the interdisciplinary cooperation.
Administrative issues and funding
The database is operated with funds from the Danish Clinical Registries (RKKP), and the organizational conditions are described in the operating agreement of the database.
The organization of the steering committee reflects the interdisciplinary profile of the clinical speciality. Both medical doctors, nurses, physiotherapists, and occupational therapists are represented together with two members representing the competency centers. The doctors represent the five regions in Denmark to mark the national status of the database. The main tasks for the steering committee are to: 1) ensure publication of data on an annual basis, including relevant comments; 2) maintain and develop the indicators; and 3) provide sufficient information to the clinical units reporting to the database.
Conclusion
The NDG is a compulsory nationwide clinical registry, which covers almost all geriatric admissions in Danish hospitals and provides valuable information about this large and increasing patient population in the health care system. With the ongoing development project aiming to include a wider population of frail multimorbid elderly patients, the NDG will provide an even broader perspective on the treatment and care of this patient population.
Acknowledgments
The collection of data in the NDG relies on the interdisciplinary teams of doctors, nurses, and therapists in the geriatric units who enter data in the database on a daily basis. We thank our colleagues throughout Denmark for their thorough and dedicated work.
This paper was funded by the Program for Clinical Research Infrastructure established by the Lundbeck Foundation and the Novo Nordisk Foundation and administered by the Danish Regions.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Rubinstein LZ. An overview of CGA: rationale, history, program models, basic components. In: Rubinstein LZ, Wieland D, Bernabei R, editors. Geriatric Assessment Technology: The State of the Art. New York, NY: Springer; 1995. pp. 1–9. [Google Scholar]
- 2.Den Landsdækkende Database for Geriatri . Coppenhagen, Denmark; Årsrapport 2014. [The National Database of Geriatrics. Annual report 2014] [Google Scholar]
- 3.Mahoney F, Wood O, Barthel D. Rehabilitation of chronically ill patients: the influence of complications on the final goal. South Med J. 1958;51:605–609. doi: 10.1097/00007611-195805000-00011. [DOI] [PubMed] [Google Scholar]
- 4.Mahoney F, Barthel D. Functional evaluation: the Barthel index. Md State Med J. 1965;14(February):61–65. [PubMed] [Google Scholar]
- 5.Beck AM, Ovesen L. At which body mass index and degree of weight loss should hospitalized elderly patients be considered at nutritional risk? Clin Nutr. 1998;17(5):195–198. doi: 10.1016/s0261-5614(98)80058-7. [DOI] [PubMed] [Google Scholar]
- 6.de Morton NA, Davidson M, Keating JL. The de Morton mobility index (DEMMI): an essential health index for an ageing world. Health Qual Life Outcomes. 2008;6:63. doi: 10.1186/1477-7525-6-63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.de Morton NA, Lane K. Validity and reliability of the de Morton mobility index in the subacute hospital setting in a geriatric evaluation and management population. J Rehabil Med. 2010;42(10):956–961. doi: 10.2340/16501977-0626. [DOI] [PubMed] [Google Scholar]
- 8.Jones CJ, Rikli RE, Beam WC. A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport. 1999;70(2):113–119. doi: 10.1080/02701367.1999.10608028. [DOI] [PubMed] [Google Scholar]
- 9.Podsiadlo D, Richardson S. The timed “up and go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi: 10.1111/j.1532-5415.1991.tb01616.x. [DOI] [PubMed] [Google Scholar]