

Abstract
Objective
Innate knowledge and developmental stage theory have been used to explain children's understanding of concepts relating to health, illness, and stress. The aim of this study was to investigate the degree to which children demonstrate unconscious cognitive associations between the concepts of stress and illness.
Design
The study employed an experimental design using an age appropriate implicit association task.
Methods
Thirty‐two children (5–11 years of age) completed the Preschool Implicit Association Test (PSIAT), a computer‐based measure of reaction time to consistent (stress and illness) and inconsistent (stress and health) concept pairings.
Results
Whilst age group had a significant effect on reaction times (older children generally displaying faster reaction times than younger children), those as young as 5–6 years of age were able to demonstrate implicit associations between stress and illness using the PSIAT. There was also some indication that this association peaks at around 7–8 years of age.
Conclusions
Findings support a combination of developmental stage theory and the innate theory of children's understanding. Whilst sample size is small, this study is the first to apply the PSIAT to the context of implicit cognitive associations between stress and illness in children. Findings have potential implications for the delivery of interventions to facilitate health promotion and development of positive health behaviours in children and indicate that even children as young as 5–6 years have some ability to relate to the concept that stress may influence illness.
Statement of contribution.
What is already known on this subject?
The way in which children understand health and illness is commensurate with their developmental stage and experience of illness. Children also appear to have a degree of innate understanding of health and illness and their causes. Furthermore, recent work suggests children have some innate understanding and knowledge of the concept of stress.
What does this study add?
This is the first study to use an implicit association task to assess children's understanding of stress and illness.
Implicit stress–illness associations were seen in children as young as 5–6 years of age.
Whilst sample size was small, this proof‐of‐concept study bridges disciplines to further understanding of health.
Keywords: stress, children, health promotion and prevention, developmental perspectives
Background
The understanding of stress as a contributory factor in physical health and well‐being in adults has received increasing recognition in health research and practice. Yet understanding of this link in healthy children has received relatively little attention for over a quarter of a century. The manner in which children conceptualize health and illness was largely advanced by Bibace and Walsh in the 1980s; building on Piaget (1930) four stages of cognitive development and applying it to the concept of illness. They identified six developmental stages: Phenomenism and contagion (3–7 years); contamination and internalization (8–10 years); physiological (11–13 years); and psychophysiological (14 years and older), with an additional level of ‘incomprehension’ for the very youngest 3‐year‐olds (Bibace & Walsh, 1980). As with earlier criticism of Piagetian staging of cognitive development, which pointed to the underestimation of children's abilities (Hughes & Donaldson, 1983), staging theory in relation to illness cognitions has received similar criticisms.
A renewed interest in children's understanding of health and illness is emerging. For example, Koopman, Baars, Chaplin, and Zwinderman (2004) compared illness understanding in a sample of 8‐ to 12‐year‐old children with diabetes and a healthy sample. Findings support the developmental staging process whilst acknowledging the role of illness specific experience. Children with diabetes were found to have a more developed understanding of diabetes compared to healthy controls but this understanding did not transfer to understanding of other illnesses such as the common cold (Koopman et al., 2004). An alternative approach to developmental staging is the theory of innate understanding (Hergenrather & Rabinowitz, 1991) in which children are able to understand more about health and illness than the staging theory would accept and they do so from an earlier age (Bir & Podmore, 1990). This suggests an intuitive knowledge of biological processes that could explain the ability of very young children to give explanations and definitions of illness (Kalish, 1996). Goldman, Whitney‐Saltiel, Granger, and Rodin's (1991) research with 4‐ to 6‐year‐olds also provides support for innate understanding. They used three tasks to determine the level of illness comprehension of 27 children and found that most of the children showed some level of understanding of illness causation, demonstrating a comprehension of health and illness from as young as 4 years.
Whilst the purest test of an innate response or association could be argued to be that closest to birth, thus avoiding experiential input, in referring to innate theory in these studies children of ages four and upwards are frequently the sampled population as such paradigms require a degree of cognitive and verbal ability. We would concur with this view and argue that innate ability can be assessed in young children of school age by comparing across older school‐age children. Furthermore, although termed ‘innate’, the argument is not for ability necessarily demonstrable at birth but one that naturally occurs or is allowed expression following development of necessary communication abilities, in other words that children have a natural ability to make associations between stress and illness and that this is not something that is evident only at the later psychophysiological stages of development but occurs alongside and may influence the earlier stages of development.
Several studies have provided support for both staging theory and an innate understanding of health in children. Normandeau, Kalnins, Jutras, and Hanigan (1998) conducted structured interviews with 1,674 children aged 5–12 years and found age differences across criteria, perception, consequences and threats to health. Yet results also showed that level of understanding in each age group was more multidimensional, suggesting that young children may also have an innate understanding of health and illness. Similar results were found by Myant and Williams (2005) who interviewed 83 children aged 4–12 years about various contagious and non‐contagious illnesses (cold, chicken pox, asthma, toothache) and physical injuries (bruise, broken leg). They found that definitions became more precise with age and that children as young as 4 years could discuss illness to a certain extent, supporting the assertion that even young children have some comprehension of illness.
To date, only one study has focused on children's understanding of stress. Valentine, Buchanan, and Knibb (2010) used semi‐structured interviews to gather qualitative data from 50 children aged 4–11 years about their knowledge of stress, and found that the majority of the participants had some experience of stress, whether personally (direct) or through a friend or relative (indirect). Older children provided more complex definitions of stress than younger children, and the 10‐ to 11‐year‐olds give more multidimensional definitions including emotional and physical/biological factors. Yet an innate understanding was demonstrated by even the youngest children (4 years) having some level of understanding and knowledge of stress, mostly giving definitions including emotional elements.
In this study, we examined children's understanding of the link between stress and illness, assessing both cognitive developmental stage of stress–illness understanding and the level of intuitive understanding of psychosocial influences. The majority of previous studies used self‐report methods such as interviews, yet researchers have highlighted that when investigating stress in children it is better to use a variety of assessments including more objective alternatives to self‐report measures where appropriate (Jessop & Turner‐Cobb, 2008; Turner‐Cobb, Rixon, & Jessop (2008); Turner‐Cobb, Rixon, & Jessop, 2011). The present study builds on the findings by Valentine et al. (2010) and extends these through the use of the Preschool Implicit Association Test (PSIAT) experimental paradigm (Cvencek, Greenwald, & Meltzoff, 2011). The Implicit Association Test (IAT) is an established cognitive assessment tool using reaction times (RTs) to investigate attitudes across a range of topics including stereotyping or attitudes towards age, gender, race, and age and of associations between self‐esteem and self‐concept (Greenwald & Farnham, 2000; Greenwald, McGhee, & Schwarz, 1998). It has only been applied to one area of child health psychology; attitudes towards smoking (Andrews, Hampson, Greenwald, Gordon, & Widdop, 2010) and has not previously been applied in the stress–illness context or to measure the level of understanding of a health concept in children. As such, this is a proof‐of‐concept study that focuses on conceptual design in bridging across disciplines of health and cognitive/developmental psychology. It is acknowledged that the sample size is representative of concept development, it is underpowered to fully test a null hypothesis and as such findings are likely to be suggestive rather than conclusive.
We hypothesized that children of all ages, even the youngest participants, would demonstrate implicit understanding of an association between stress and illness, showing faster RTs and greater accuracy on the PSIAT when consistent stress and illness pairings were presented, compared to inconsistent pairings of stress and health. We reasoned that if the youngest participants were able to significantly distinguish between consistent and inconsistent pairing as effectively as the older participants then this would provide support for the innate theory of understanding. We also hypothesized that there would be a gradual increase in RT (speed) on PSIAT performance, with older children demonstrating significantly faster RTs than the younger children, indicative of a developmental pattern consistent with staging theory. Our expectation was for evidence of developmental staging complemented by an underlying innate understanding. The latter was given greater consideration than afforded in some of the original work in the area.
Method
Participants
Participants (n = 32; 13 girls and 19 boys) were aged 5–11 years and of a similar educational level and socio‐economic background to one another. All were white Caucasian, of standard educational level, attending school in a semi‐rural location of relative affluence. Further sociodemographic data were not collected as parents were not asked to contribute data for the study. Participants were drawn from a local school using an opt‐in procedure. Invitation letters were sent to the parents of all children in the school, to which there was a 32% response rate for their child to opt in for participation in the study.
Materials
Explicit understanding
A test of explicit understanding of the stress–illness link was initially assessed. The explicit measure was a story, based on one used by Valentine et al. (2010) to assess children's understanding of stress. The version in this study was adapted to incorporate health and illness. The story described two characters, one who encountered various stressors and one who did not encounter stressors but carried out health promoting behaviours. After the story, participants were asked about why they thought the character who encountered the stressors in the story became ill. Answers were coded as 0 or 1 as to whether they mentioned stress as a possible cause for the character's illness.
The Preschool Implicit Association Test
The implicit association between stress and illness was measured using a modified version of the PSIAT (Cvencek et al., 2011) adapted from the original adult version of the IAT (Greenwald et al., 1998). The IAT is a computer‐based task that measures RTs to stimulus items. Participants have to sort the stimulus items into one of four categories using two response buttons (where each response button corresponds to two categories). This allows researchers to measure associations between a target concept and an attribute concept by measuring whether people are quicker to respond when consistent/associated or inconsistent/unassociated pairs are paired on the same response button). A faster reaction time indicates a stronger link between concept and attribute. A meta‐analysis by Greenwald, Poehlman, Uhlmann, and Banaji (2009) of the predictive validity of the IAT found it to be a better predictor of attitudes than explicit measures (r = .25 and r = .13, respectively).
The IAT has been adapted very effectively for use with children to include colour‐coded response buttons, auditory presentation of any word stimuli by a neutral female voice rather than written word, and pictures of children's faces rather than adults’ faces (Baron & Banaji, 2006; Dunham, Baron, & Banaji, 2006; Rutland, Cameron, Milne, & McGeorge, 2005; Steffens, Jelenec, & Noack, 2010). Although IATs have been used successfully with children as young as 6 years, it was not until a few years ago that they were adapted by Cvencek et al. (2011) for use in children under 6 years of age. Cvencek et al. (2011) created the PSIAT, an effective tool for measuring 4‐year‐olds’ implicit attitudes towards objects and gender adapted the standard IAT to present both auditory and visual stimuli simultaneously. Reading level was not relied upon and the PSIAT used fewer presentations of stimulus items (trials) than standard adult IATs to ensure concentration throughout the experiment and use of both words and images, image category reminders, and coloured stripes (green and orange) corresponding to response buttons (Cvencek et al., 2011). IATs typically involve 180 trials (Greenwald, Nosek, & Banaji, 2003) but Rutland et al. (2005) suggested a reduction in the number of trials is appropriate for young children to avoid fatigue and boredom effects. Work by Cvencek et al. (2011) reduced the number of trials in young children by 20% to 144. The current study employed 112 trials in total (64 of which were critical trials) with an intertrial interval of 400 ms.
The stimuli presented in the PSIAT were a combination of words and images, relating to the four ‘target concept’ categories of ‘health’, ‘illness’, ‘stress’, and ‘no stress’, and were presented in the centre of the laptop screen. Stimulus images were selected from a combination of copyright‐free image websites, the Karolinska Directed Emotional Faces scale, and the International Affective Picture System. Stimulus words were selected from the Affected Norms for English Words (Bradley & Lang, 1999), some used by Cvencek et al. (2011). During material preparation and selection two additional researchers independently coded, rated and verified the choice of pictures and words prior to testing. A total of 36 words and 32 images were collected and rated for how strongly they were associated with the four target concepts. The four images rated as best representative of their target category were selected and used as the category images. These category images remained on the screen throughout the critical blocks of the task (one in each of the four corners of the screen) and can be seen in the bottom pictures in Figure 1. The next highest rated 16 images and 16 words were used as stimulus items (four words and four images per category). For example, the words in the stress category included nervous, scared, worried, and busy, and the pictures showed children looking fearful and upset. Similarly words in the illness category included fever, hospital, medicine and sick and pictures showed medical situations and doctors.
Figure 1.
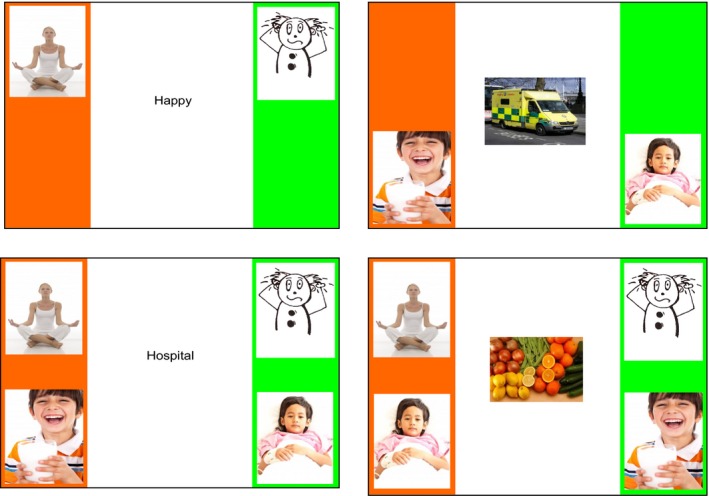
Examples of Preschool Implicit Association Test (PSIAT) blocks presented. The two upper images are examples of two practice blocks; (left) block 1 (no stress and stress) and (right) block 2 (health and illness). The two lower images are examples of two test blocks; (left) block 3 displays associated pairs.
A laptop running ePrime was used to display the stimuli and participants responded using a response button box (only two response keys were needed). Stimulus items were presented in a random order generated by ePrime and each item was presented once. Headphones were used to play the audio files that accompanied the stimulus items (beeps for images, verbalizations for words). The 32 stimulus items in the PSIAT were presented in five blocks: Block 1 contained the 16 stress and no stress words/images, blocks 2 and 4 contained the 16 health and illness words/images, and blocks 3 and 5 included all 32 items. Only two categories were shown in blocks 1, 2, and 4 (see Figure 1 upper images); therefore, each response button corresponded to one category. Conversely, in blocks 3 and 5 four categories were shown, two categories per response button. The purpose of these two blocks is to test implicit understanding of the stress–illness relationship when the two concepts stress and illness are paired together (associated/consistent pairs) or conversely paired (unassociated/inconsistent pairs). In the consistent block the category images for stress and illness were shown on the same side of the screen and shared a response button, and the categories of no stress and health were shown on the other side of the screen and also shared a response button. In the inconsistent block stress and health were paired together and no stress and illness were paired together on the screen and the same response button (see Figure 1 lower images).
During all five blocks the orange and the green stripes with the two/four category images remained on the screen as a reminder to participants as to which button corresponds to which category. The two response buttons each corresponded to a category: The left/orange button to the category on the left and the right/green button to the category on the right. The participants used these response buttons to indicate which category the stimulus word/image belonged to. Counterbalancing ensured that half the participants were randomly allocated the associated pairs first (order A) and half were presented with the unassociated pairs first (order B) as in Cvencek et al. (2011). The health and illness categories alternated between the right and left position on the screen (blocks 2 and 4) whereas the stress and illness categories remained unchanged throughout the task, to cause minimal confusion to participants.
Procedure
Written consent was obtained from parents and verbal assent was provided by child participants in advance of testing. Participant experience of illness was indicated on the consent form by their parents. Children were tested in a quiet room in the school by a female experimenter, who remained present throughout testing (approximately 15 min per participant). A story and question were used to assess participants’ explicit knowledge of the stress–health relationship and to check their comprehension of the words that were to be presented in the implicit task. The researcher wrote down participants’ answers verbatim. Participants then sat in front of the laptop to complete the PSIAT using the response buttons. Participants were given verbal instructions and shown example screens, after which they completed the PSIAT. The researcher gave positive feedback and prompted participants to ‘guess’ which group a word or image belonged to if they were unsure. This ensured that participants responded as quickly as possible to the stimulus. At the end of the experiment participants were debriefed.
Statistical analysis
For the explicit task, responses were coded dichotomously as either mentioning/not mentioning stress as a cause of illness (coded 0/1 respectively). In the implicit task, performance was measured by RT to each stimulus item. RTs and accuracy of responses (correct/incorrect) were recorded by ePrime. A higher RT to the associated pairs than to the unassociated pairs would indicate a higher level of understanding of the link between stress and illness (the associated concepts). The RT data were analysed according to the scoring algorithm created by Greenwald et al. (1998). A split‐plot ANOVA was used to compare RT for consistent and inconsistent pair responses across age groups, using a 2 (RT: Consistent, inconsistent) × 4 (Age: 5–6, 7, 8–9, 10–11 years) design. In addition, we have also presented the data using a more recent scoring algorithm which calculates D scores rather than RT scores (Greenwald et al., 2003) and analysed using a univariate ANOVA.
The additional D score analysis, whilst informative, is treated with caution given the small sample size but presented for consistency; therefore, findings are based on the RT scoring as was deemed appropriate for this cohort. The rationale for using RT as opposed to D scores is mostly due to the small sample size. The calculation of D scores is complex and controls for numerous factors such as age and cognitive level. It therefore requires more power and with a small sample such as this one we could not achieve the power necessary for this; a probable explanation for why we found no statistically significant results. As the hypothesis for this study focuses on whether children are faster to respond to consistent or inconsistent concepts, it is appropriate to use the RT data for consistent and inconsistent pairs. Although we have found statically significant results using RT data, they should be treated with caution due to the small sample size.
Results
Age group and concept pairings: Reaction time
Descriptives for the demographic information and dependent variables can be found in Table 1. A paired‐samples t‐test showed that RTs were faster for consistent than inconsistent pairs for all age groups, demonstrating that participants respond more quickly when stress and illness were paired on the same response button, t(31) = −5.32, p < .001, 95% CI (−853.58, −380.20). There was a roughly equal gender split in the sample (59% boys), only 21% of the sample had experience of illness, and the majority of participants (56%) explicitly stated a link between stress and illness.
Table 1.
Number and percentages for the demographic information and means and standard deviations (SD) of the dependent variables by child age (n = 32)
| Child age (years) | ||||
|---|---|---|---|---|
| 5–6 (n = 8) | 7 (n = 7) | 8–9 (n = 10) | 10–11 (n = 7) | |
| Gender, N (%) | ||||
| Male | 2 (25) | 3 (43) | 8 (80) | 6 (86) |
| Female | 6 (75) | 4 (57) | 2 (20) | 1 (14) |
| Experience of illness, N (%) | ||||
| Yes | 2 (25) | 0 (0) | 4 (40) | 1 (14) |
| No | 6 (75) | 7 (100) | 6 (60) | 6 (86) |
| Explicit answer included ‘stress’, N (%) | ||||
| Yes | 2 (25) | 4 (57) | 6 (60) | 6 (86) |
| No | 6 (75) | 3 (43) | 4 (40) | 1 (14) |
| Reaction time (RT) (ms) and D scores, mean (SD) | ||||
| RT for consistent pairs | 2,851 (947) | 2,066 (466) | 1,969 (438) | 1,319 (403) |
| RT for inconsistent pairs | 3,114 (655) | 2,940 (1,091) | 2,723 (812) | 1,889 (476) |
| D scores | 0.24 (0.50) | 0.61 (0.60) | 0.6 (0.30) | 0.53 (0.75) |
A split‐plot ANOVA revealed that age group did exert a significant effect on mean RT, F(1, 28) = 28.37, p < .001, with participants demonstrating faster RTs for consistent concept pairings (M = 2068.59, SD = 787.191) than for inconsistent concept pairings (M = 2685.48, SD = 876.56). Post‐hoc tests showed a significant difference in mean RTs between 5–6 and 10–11 years (p = .01) with 95% CIs (459.77, 2296.65). These results show that older participants (10–11 years) had faster RTs than younger participants (5–6 years). See Figure 2a for a comparison of RT to consistent and inconsistent pairings for each group.
Figure 2.
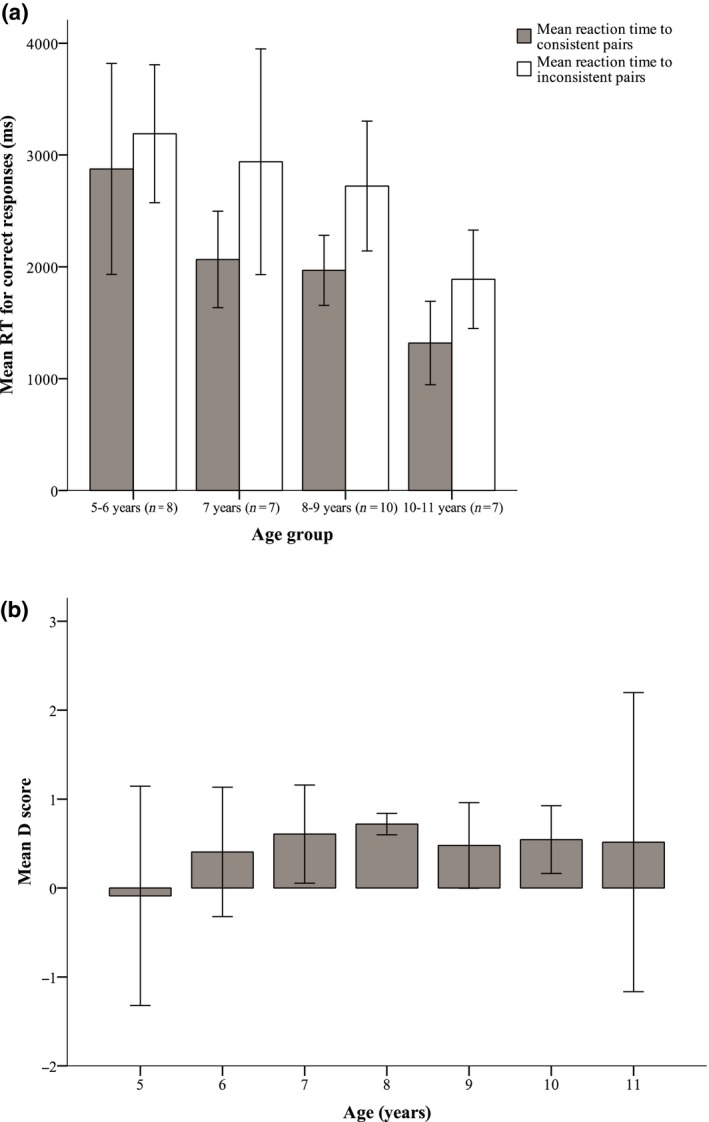
Preschool Implicit Association Test (PSIAT) mean reaction times (RTs) in milliseconds (ms) for consistent and inconsistent concept pairings by age group (a) and mean D scores (positive scores indicate a preference for associated pairs and negative scores suggest a preference for unassociated pairs) (b) across ages 5–11 years. Error bars represent 95% confidence intervals.
Age group and concept pairings: Response accuracy
A mean score for accuracy of responses for consistent and inconsistent pairs was calculated for each participant. Accuracy of responses refers to how many trials participants responded to correctly; the closer the mean score is to 1 the more correct responses there were, the closer it is to 0 the more incorrect responses there were. A paired‐samples t‐test showed that participant responses were more accurate when responding to consistent pairs than to inconsistent pairs, t(31) = 2.88, p = .001, 95% CI (0.02, 0.09) with a medium to large effect size (r = .46). A series of paired‐samples t‐tests demonstrated significant differences in accuracy to consistent and inconsistent pairs for 8–9 years, t(9) = 8.34, p = .001, 95% CI (0.06, 0.10), and 10–11 years, t(6) = 2.83, p = .03, 95% CI (0.01, 0.11), demonstrating the two older age groups responded more accurately to consistent than inconsistent concept pairs, suggesting that they were better able to accurately distinguish between associated and unassociated images and words.
Explicit understanding
An independent t‐test showed that for consistent concept pairs participants who explicitly identified stress as a cause of illness had significantly faster RTs than the participants who did not explicitly link stress and illness, t(29) = −2.12, p = .03, 95% CI (46.65, 1146.46) with a medium effect size (r = .37). No significant difference was found for inconsistent pairs between those who had an explicit understanding of stress and those who did not.
Effect of illness experience
An independent t‐test revealed no significant differences in mean RTs to consistent pairs (p = .76) and inconsistent pairs (p = .78) of participants who had experience of illness and those who did not have experience of illness, nor was there a significant difference between accuracy of responses to consistent pairs (p = .77) and inconsistent pairs (p = .59) for those with experience of illness and those without experience of illness.
Gender differences
An independent t‐test showed there to be a significant effect of gender, with male participants displaying significantly faster RTs to both the consistent, t(30) = −2.28, p = .03, 95% CI (−1138.11, −62.00), and inconsistent concept pairings, t(30) = −2.22, p = .03, 95% CI (−1269.72, −53.49), with a medium effect size (r = .38). However, when gender was added into the ANOVA as a variable there was no significant interaction. An independent t‐test showed no significant difference in accuracy of responses between males and females for consistent (p = .33) or inconsistent concept pairs (p = .37).
IAT assumptions: Order effect, reliability and validity
To ensure that the PSIAT met the assumption that the order in which the blocks were presented to participants had no significant effect on RTs an independent t‐test was administered. This showed no significant effect of order on RTs to consistent (p = .12) or inconsistent concept pairs (p = .65). This study demonstrates the effectiveness of the PSIAT in terms of reliability and validity in research on children's understanding of the relationship between stress and illness. As discussed in the method, the IAT is a reliable tool for measuring implicit beliefs (Nosek, Greenwald, & Banaji, 2007) and has been shown to have high predictive validity (Greenwald et al., 2009). The version of the PSIAT used in the present study also meets the criteria for internal validity as discussed by Nosek et al. (2007) who stated that internal validity can be ensured as long as it is unambiguous which stimulus items belong to each category, the presentation of stimulus items is random, and the consistent and inconsistent concept blocks are counterbalanced. Whilst IATs are commonly used to measure attitudes, implicit beliefs and in some cases concepts, they have rarely been used previously to examine health concepts and this is the first use of the IAT to assess stress–illness associations or understanding. The categories of health, illness, stress and no stress were clear and unambiguous.
Alternative analysis: D scores
As previously discussed, IAT data can be analysed using RT or D scores. IAT performance is measured by response latency (the speed of the response or RT) and response accuracy (whether the responses were correct or incorrect) to each stimulus item. The response latency and accuracy data for each participant were transformed into D scores using the improved IAT scoring algorithm from Greenwald et al. (2003) which has been used effectively in IATs adapted for children including the PSIAT (Cvencek et al., 2011). D scores represent the difference between the RT scores for associated/consistent and unassociated/inconsistent concept pairs. A positive D score suggests a preference for the consistent pairs (equivalent to a faster RT to those pairs) and a negative score indicates a preference for the inconsistent pairs.
The new algorithm differs from the previous algorithm in relation to which extreme values were deleted; in the original algorithm, RT scores were eliminated or recoded if they were outside the range of 300–3,000 ms; however, the new algorithm eliminates scores outside the range of 300–10,000 ms and participants who have more than 10% of trials with a latency of <3,000 ms, making this method more inclusive and the RT method more stringent. Cvencek et al. (2011) excluded participants based on the above criteria and also those who had an error rate or 35% or above. Only one participant in the present study had over this level of errors (50%) and so was excluded from the analysis. The data were screened for outliers, normality, linearity and multicollinearity and no issues arose. D scores were analysed using a univariate ANOVA with D scores entered as the DV, age and gender entered as the IVs and order of blocks, explicit understanding and experience of illness entered as covariates. Order was the only variable that was found to be significant, F(1, 17) = 9.83, p = .006, with a medium effect size (r = .37), whereas age (p = .821), gender (p = .857), explicit understanding (p = .207), and experience of illness (p = .934) were not significant. It appears that people who were presented with order A (M = 0.81, SE = 0.10) which showed the consistent concept pairs first showed a stronger preference for the consistent pairs than those who were presented with order B (M = 0.19, SE = 0.12) and saw the inconsistent pairs first.
Although age and gender were not significant, there is an interesting pattern found when the D scores for each age group are visually assessed. Figure 2b shows that 5‐year‐olds have a preference towards the inconsistent pairs suggesting they lack an understanding of the link between stress and illness. However, all of the other age groups show a preference towards consistent pairs. As D scores represent the difference between RTs to associated and unassociated pairs, a similar pattern was expected with the RT and D score analyses. Reasons for the discrepancy are considered in the discussion.
Discussion
In this sample of 32 children aged 5–11 years, we found that children as young as 6 years of age demonstrated explicit understanding of an association between stress and illness using the PSIAT. There was some indication from D score evaluation that this association peaks at around age 7–8 years of age with no effect found for the very youngest age group of 5‐ to 6‐year‐old children. As expected, older children generally displayed faster RTs than younger children indicative of both cognitive and developmental maturity.
The results of the present study give support for both innate and developmental theories of children's understanding of the relationship between stress and illness. The majority of the younger participants completed the PSIAT with reasonable RTs and these accelerated across age groups, demonstrating a developmental pattern of understanding. Yet evidence for an innate understanding of the link between stress and illness was only partially supported and the relative weight of the findings was in support of a developmental rather than an innate understanding. Children of all ages responded faster to consistent concept pairings (e.g., stress and illness) than inconsistent concept pairings (e.g., stress and health) as expected. This pattern of results suggests that it was easier for the participants to categorize stimuli when associated concepts shared a response button. This could be because the concepts of stress and illness are strongly linked in cognition and are therefore more easily and quickly accessed than when stress and health are paired together. An alternative explanation of these results might suggest that it is children's understanding of the task that develops with age, as opposed to the development of their understanding of the stress–health relationship. However, this cannot explain how even the youngest children were able to complete the task with only a few errors; therefore, the first explanation appears to be substantiated by the findings. Although significant differences were not observed between all of the age groups, a clear age‐related pattern emerged.
Findings of the present study support research by Normandeau et al. (1998) and Myant and Williams (2005) who found evidence of early intuitive understanding, as well as support for children's understanding of illness following a developmental pattern. Valentine et al. (2010) found a similar pattern in children's understanding of stress. The present study demonstrates that even very young children have an understanding of stress although this develops and becomes more comprehensive with age. The present study builds upon qualitative work by Valentine et al. (2010) using an experimental paradigm to address understanding of stress and illness. This link appears to follow the developmental pattern of cognitive abilities in other domains. Yet there is some support for the youngest children having some concept of the stress–illness link which has not been documented previously and which supports the notion of stage theories underestimating young children's intellectual ability (e.g., Siegler, 1998). Innate theories suggest underlying capability for implicit understanding of stress and illness associations which if overlooked may limit the potential for building more sophisticated understanding of the nature of illness and staying healthy. Such understandings could be harnessed and appropriately encouraged in children to promote health and resilience, avoiding over protective or disabling approaches that may generate more harm than good.
Although the results using RT data show clear support for the hypotheses, D score analysis did not reveal significant effects. When analysed using ANOVA, neither age nor gender had an effect on D scores, but in the RT data there were significant age and gender effects. As the RT data and D scores represent the same data, it is unexpected for them to show differing effects. We suggest this discrepancy is due to small sample size causing the D score analysis to be underpowered. Nonetheless, the pattern is conceptually of interest as it suggests that understanding may not follow a linear trajectory. D scores indicate a peak in understanding at ages 7–8 years.
Limitations of the present study
The present study aimed simply to make an initial attempt to apply a well‐established paradigm to a new concept. We acknowledge a major limitation in sample size. A larger sample would be required to improve the overall power of the study and enable more meaningful D score interpretations. This is particularly true for the younger age groups (<7 years old) where a larger sample would enable more in depth breakdown of ages for closer scrutiny of innate understanding. Similarly for the 7‐ to 8‐year‐old age group, who were suggested by the data as being at a potential pivotal age for understanding the stress–illness link but effects were not sufficiently powered to determine significance. As acknowledged in the introduction, the sample size used in this study is representative of concept development and as such suggestive rather than conclusive. Nonetheless, it represents some important ideas and methodological advances which further understanding of health. Issues relating to application of the PSIAT to a stress concept include the lack of uniformity of image stimulus items, being of a variety of colours and styles. A prevalence of male images over female images occurred due to practical issues of image accessibility and may have explained why boys had faster RTs than girls. Furthermore, the categories of ‘no stress’ and ‘health’ were selected as counterparts to ‘stress’ and ‘illness’ although they are not exact opposites, as ‘no stress’ is not a precise description and ‘health’ is not merely the absence of illness. Despite this, the concept descriptors serve their purpose as opposing categories to the main concepts of interest.
Implications for future research
The application of psychosocial concepts of stress and health to an established implicit association paradigm requires further validation, testing with a greater sample size and range of ages. Yet the use of the PSIAT paradigm as a tool for assessing children's understanding of stress and illness has proved extremely valuable. A measure of implicit understanding was used to develop a more complete picture of children's understanding, not always accessible using explicit self‐report measures. The importance of this area of research was highlighted by Burbach and Peterson (1986) who suggested that understanding of children's knowledge can improve the way in which health professionals communicate health messages to children, beneficial for both prevention of illness and treatment interventions. Yet previous research has suggested that in practice, health care professionals do not adapt health messages for children based on patient age, developmental level or experience of illness, instead aiming their information at ‘mid‐school age level’ (Perrin & Perrin, 1983, p. 877). The findings of the current study provide initial support for the inclusion of a child's age or level of understanding of the stress–illness link in health messages given to children. Issues concerned with the prevention of illness are particularly important in relation to the health education given by parents and schools. More broadly, the implicit associations tested could also be explored in adolescent and adult populations to gain a fuller understanding of the differences between child and adult understandings. This work assumes an implicit understanding of stress and illness in adults, but this has not yet been systematically examined using the methods outlined here. This raises important question for future research that could potentially inform health interventions across the lifespan.
In conclusion, the present study is the first to use the experimental PSIAT paradigm to address children's understanding within the health psychology field. It is also the first study to address children's comprehension of associations between stress and illness. Using this novel experimental method, the findings illustrate that children as young as 5–6 years of age demonstrate some knowledge, at the level of implicit understanding, of a relationship between stress and illness, and there is some indication that this unconscious association is strongest in children aged 7–8 years. This study highlights the importance of using psychosocial information from health psychology research informed by cross‐disciplinary work, to appropriately tailor health messages to children of different ages. The findings have potential implications for the delivery of interventions to facilitate health promotion and development of positive health behaviours in children. Whilst such messages requires age appropriate delivery, unconscious understanding or capacity for implicit associations between stress and illness should not be underestimated, even in the youngest of school‐age children.
Conflict of interest
All authors declare no conflict of interest.
Acknowledgements
The authors would like to thank the participants and schools who assisted in this study and Emma Ashwin for providing the audio recordings which accompanied the PSIAT.
The copyright line for this article was changed on 25th February 2016 after original online publication.
References
- Andrews, J. A. , Hampson, S. E. , Greenwald, A. G. , Gordon, J. , & Widdop, C. (2010). Using the Implicit Association Test to assess children's implicit attitudes toward smoking. Journal of Applied Social Psychology, 40, 2387–2406. doi:10.1111/j.1559‐1816.2010.00663.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron, A. S. , & Banaji, M. R. (2006). The development of implicit attitudes: Evidence of race evaluations from ages 6 and 10 and adulthood. Psychological Science, 17, 53–58. doi:10.1111/j.1467‐9280.2005.01664.x [DOI] [PubMed] [Google Scholar]
- Bibace, R. , & Walsh, M. E. (1980). Development of children's concepts of illness. Pediatrics, 66, 912–917. doi:10.1016/S0002‐7138(09)61657‐5 [PubMed] [Google Scholar]
- Bir, J. E. , & Podmore, V. N. (1990). Children's understanding of health and illness. Psychology & Health, 4, 175–185. doi:10.1080/08870449008408151 [Google Scholar]
- Bradley, M. M. , & Lang, P. J. (1999). Affective norms for English words (ANEW): Instruction manual and affective ratings (Technical Report C‐1). Gainsville, FL: The Centre for Research in Psychophysiology, University of Florida. [Google Scholar]
- Burbach, D. J. , & Peterson, L. (1986). Children's concepts of physical illness: A review and critique of the cognitive‐developmental literature. Health Psychology, 5, 307–325. doi:10.1037/0278‐6133.5.3.307 [DOI] [PubMed] [Google Scholar]
- Cvencek, D. , Greenwald, A. G. , & Meltzoff, A. N. (2011). Measuring implicit attitudes of 4‐year‐olds: The Preschool Implicit Association Test. Journal of Experimental Child Psychology, 109, 187–200. doi:10.1016/j.jecp.2010.11.002 [DOI] [PubMed] [Google Scholar]
- Dunham, Y. , Baron, A. S. , & Banaji, M. R. (2006). From American city to Japanese village: A cross‐cultural investigation of implicit race attitudes. Child Development, 77, 1268–1281. doi:10.1111/j.1467‐8624.2006.00933.x [DOI] [PubMed] [Google Scholar]
- Goldman, S. L. , Whitney‐Saltiel, D. , Granger, J. , & Rodin, J. (1991). Children's representations of “everyday” aspects of health and illness. Journal of Pediatric Psychology, 16, 747–766. doi:10.1093/jpepsy/16.6.747 [DOI] [PubMed] [Google Scholar]
- Greenwald, A. G. , & Farnham, S. D. (2000). Using the Implicit Association Test to measure self‐esteem and self‐concept. Journal of Personality and Social Psychology, 79, 1022–1038. doi:10.1037/0022‐3514.79.6.1022 [DOI] [PubMed] [Google Scholar]
- Greenwald, A. G. , McGhee, D. E. , & Schwarz, J. L. K. (1998). Measuring individual differences in implicit cognition: The Implicit Association Test. Journal of Personality and Social Psychology, 74, 1464–1480. doi:10.1037/0022‐3514.74.6.1464 [DOI] [PubMed] [Google Scholar]
- Greenwald, A. G. , Nosek, B. A. , & Banaji, M. R. (2003). Understanding and using the Implicit Association Test: I. An improved scoring algorithm. Journal of Personality and Social Psychology, 85, 197–216. doi:10.1037/0022‐3514.85.2.197 [DOI] [PubMed] [Google Scholar]
- Greenwald, A. G. , Poehlman, T. A. , Uhlmann, E. L. , & Banaji, M. R. (2009). Understanding and using the Implicit Association Test: III. Meta‐analysis of predictive validity. Journal of Personality and Social Psychology, 97, 17–41. doi:10.1037/a0015575 [DOI] [PubMed] [Google Scholar]
- Hergenrather, J. R. , & Rabinowitz, M. (1991). Age‐related differences in the organization of children's knowledge of illness. Developmental Psychology, 27, 952–959. doi:10.1037/0012‐1649.27.6.952 [Google Scholar]
- Hughes, M. , & Donaldson, M. (1983). The use of hiding games for studying coordination of viewpoints In Donaldson M., Grieve R. & Pratt C. (Eds.), Early childhood development and education (pp. 245–253). Oxford, UK: Basil Blackwell. [Google Scholar]
- Jessop, D. S. , & Turner‐Cobb, J. M. (2008). Measurement and meaning of salivary cortisol: a focus on health and disease in children. Stress, 11, 1–14. doi:10.1080/10253890701365527 [DOI] [PubMed] [Google Scholar]
- Kalish, C. (1996). Causes and symptoms in preschoolers' conceptions of illness. Child Development, 67, 1647–1670. doi:10.2307/1131723 [PubMed] [Google Scholar]
- Koopman, H. M. , Baars, R. M. , Chaplin, J. , & Zwinderman, K. H. (2004). Illness through the eyes of the child: The development of children's understanding of the causes of illness. Patient Education and Counseling, 55, 363–370. doi:10.1016/j.pec.2004.02.020 [DOI] [PubMed] [Google Scholar]
- Myant, K. A. , & Williams, J. M. (2005). Children's concepts of health and illness: Understanding of contagious illnesses, non‐contagious illnesses and injuries. Journal of Health Psychology, 10, 805–819. doi:10.1177/1359105305057315 [DOI] [PubMed] [Google Scholar]
- Normandeau, S. , Kalnins, I. , Jutras, S. , & Hanigan, D. (1998). A description of 5‐ to 12‐year old children's conception of health within the context of their daily life. Psychology & Health, 13, 883–896. doi:10.1080/08870449808407438 [Google Scholar]
- Nosek, B. A. , Greenwald, A. G. , & Banaji, M. R. (2007). The Implicit Association Test at age 7: A methodological and conceptual review In Bargh J. A. (Ed.), Automatic processes in social thinking and behavior (pp. 265–292). New York, NY: Psychology Press. [Google Scholar]
- Perrin, E. C. , & Perrin, J. M. (1983). Clinicians' assessments of children's understanding of illness. American Journal of Diseases of Children, 137, 874–878. doi:10.1001/archpedi.1983.02140350048012 [DOI] [PubMed] [Google Scholar]
- Piaget, J. (1930). The child's conception of physical causality. London: Routledge & Kegan Paul PLC. [Google Scholar]
- Rutland, A. , Cameron, L. , Milne, A. , & McGeorge, P. (2005). Social norms and self‐presentation: Children's implicit and explicit intergroup attitudes. Child Development, 76, 451–466. doi:10.1111/j.1467‐8624.2005.00856.x [DOI] [PubMed] [Google Scholar]
- Siegler, R. S. (1998). Children's thinking (3rd ed.). London: Prentice Hall. [Google Scholar]
- Steffens, M. C. , Jelenec, P. , & Noack, P. (2010). On the leaky math pipeline: Comparing implicit math‐gender stereotypes and math withdrawal in female and male children and adolescents. Journal of Educational Psychology, 102, 947–963. doi:10.1037/a0019920 [Google Scholar]
- Turner‐Cobb, J. M. , Rixon, L. , & Jessop, D. S. (2008). A prospective study of diurnal cortisol responses to the social experience of school transition in four‐year‐old children: Anticipation, exposure, and adaptation. Developmental Psychobiology, 50, 377–389. doi:10.1002/dev.20298 [DOI] [PubMed] [Google Scholar]
- Turner‐Cobb, J. M. , Rixon, L. , & Jessop, D. S. (2011). Hypothalamic‐pituitary‐adrenal axis activity and upper respiratory tract infection in young children transitioning to primary school. Psychopharmacology (Berl), 214, 309–317. doi:10.1007/s00213‐010‐1965‐x [DOI] [PubMed] [Google Scholar]
- Valentine, A. , Buchanan, H. , & Knibb, R. (2010). A preliminary investigation of 4 to 11‐year‐old children's knowledge and understanding of stress. Patient Education and Counseling, 79, 255–257. doi:10.1016/j.pec.2009.08.011 [DOI] [PubMed] [Google Scholar]