

Summary:
Indocyanine green angiography (SPY) was used to guide arterial selection for an anterolateral thigh free flap in the setting of severe peripheral vascular disease. SPY technology serves as a novel and sensitive intraoperative tool to predict decreased tissue perfusion from vessel sacrifice for flap harvest. Change in SPY time parameters measuring superficial blood flow distal to the donor site while temporarily intraoperatively clamping different possible arterial pedicles can optimize free flap design to avoid iatrogenic critical limb ischemia.
The anterolateral thigh (ALT) flap is the most commonly used fasciocutaneous free flap for head and neck reconstruction.1 Flap viability requires adequate tissue perfusion, but vessel sacrifice for the vascular pedicle must not compromise blood flow distal to the donor site. Patients with severe peripheral vascular disease (PVD) bordering on critical limb ischemia (CLI) thus offer unique challenges for the free flap surgeon.
CLI is end-stage PVD, or atherosclerotic disease of the lower limbs, in which inadequate blood flow causes cutaneous hypoxia and acidosis leading to painful ischemic neuritis or skin necrosis.2 The TransAtlantic Inter-Society Consensus defined CLI as chronic ischemic rest pain or presence of ulcers or gangrene with the following evidence of PVD causality: ankle pressure ≤50 to 70 mm Hg, toe pressure ≤30 to 50 mm Hg, or transcutaneous PO2 ≤30 to 50 mm Hg.3
For one challenging patient with values nearing these parameters, we used indocyanine green angiography corroborated by toe pressures to investigate SPY’s utility in free flap harvest. The SPY system (Novadaq Technologies, Inc., Concord, Ontario, Canada) is a laser angiographic fluorescent imaging system providing real-time intraoperative imaging of superficial blood flow. The SPY system uses fluorescence agent indocyanine green, which tightly binds plasma proteins to remain intravascular. Its short plasma half-life of 3 to 5 minutes and rapid tissue clearance allow repeated evaluations during a single surgical procedure.4 Free flap surgeons have previously used the SPY system to identify perforator perfusion zones and to confirm flap perfusion during dissection and after anastomosis.5, 6 Additionally, vascular surgeons have employed this technology to validate successful revascularization and to delineate viable from nonviable tissue.6–10
In limbs with critical ischemia, SPY measurements of perfusion significantly correlate with increased toe-brachial index (TBI) and toe pressures after revascularization procedures.8 Time perfusion parameters are more reliable because intensity parameters vary with distance between the camera and the skin, skin color, and ambient light.9 Igari et al8 demonstrated that time to half-maximum intensity (T1/2) greater than 20 seconds correlates with toe pressure less than 50 mm Hg, thus predicting CLI.
The purpose of this report is to comment on SPY system utility in determining the effect of free flap harvest on distal limb perfusion in a patient with severe PVD.
CASE
We present the case of a 69-year-old male with history of severe PVD and oral cavity carcinoma requiring composite oral cavity resection and free flap reconstruction. His Allen test exceeded 15 seconds bilaterally, precluding forearm tissue harvest. His prior history of a right femoral-popliteal bypass graft eliminated this limb from donor candidacy. Preoperative testing revealed an ankle-brachial index of 0.47 on the left and 0.97 on the right revascularized limb. Left lower extremity duplex ultrasound revealed superficial femoral artery (SFA) occlusion, but a patent profunda femoris artery (PFA) providing monophasic, low-velocity distal flow. Computed tomography angiogram with runoff revealed that the SFA reconstituted distally from genicular collaterals and from collaterals from the distal PFA (Fig. 1). We planned to harvest either an ALT or medial thigh flap based on perforators located intraoperatively. We would determine which flap to harvest based on the distal perfusion changes induced by temporarily clamping the possible pedicles.
Fig. 1.
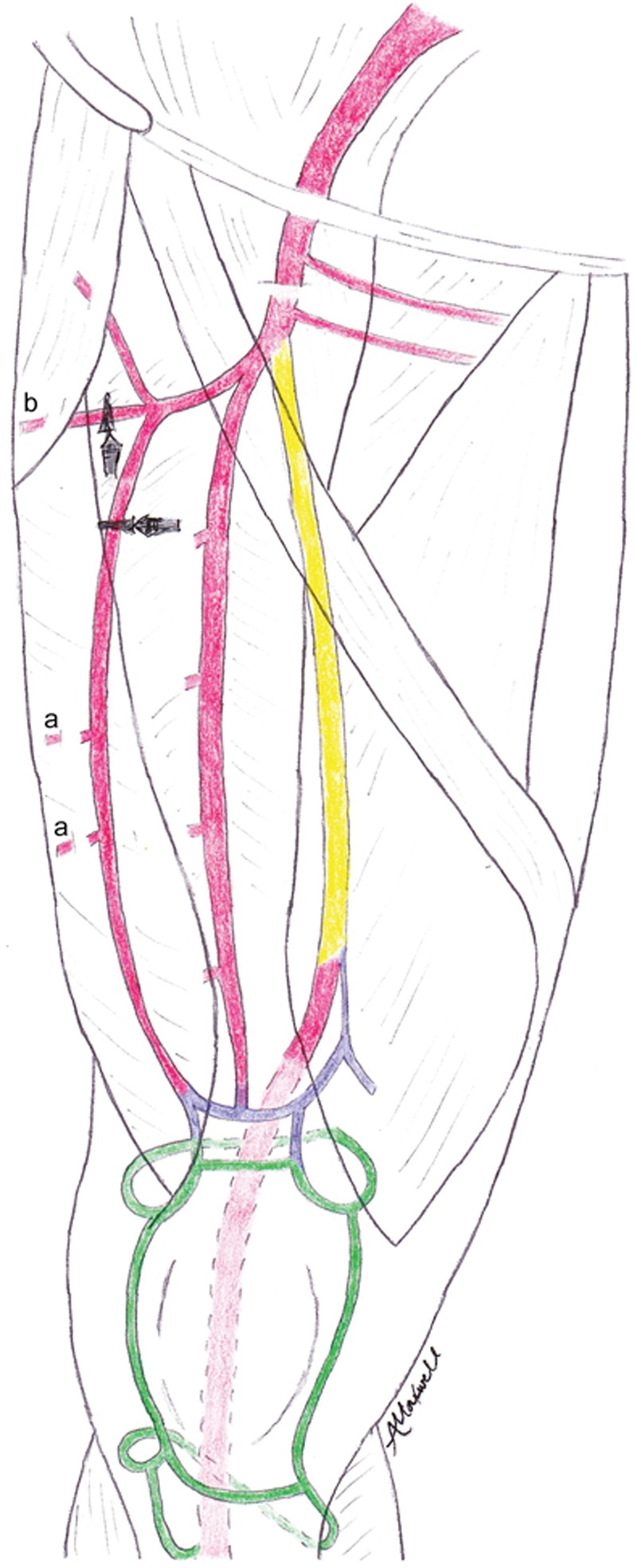
Pedicle options for the ALT flap in the context of SFA occlusion. The distal SFA was reconstituted from genicular collaterals (green) and collaterals from the PFA (purple). Sites of arterial occlusion are in yellow. A, Perforators from the descending branch of the lateral circumflex femoral artery (DCFA). B, Perforator from the transverse branch of the lateral circumflex femoral artery (TCFA). Gray claps on the figure mark sites of arterial branch clamping as described.
The patient was taken to the operative suite for bilateral neck dissections, composite resection of his oral cavity cancer including marginal mandibulectomy, and simultaneous left thigh flap harvest. The lateral thigh was perfused by 2 distinct perforators, one from the transverse branch of the lateral circumflex femoral artery (TCFA) and another from the descending branch of the lateral circumflex femoral artery (DCFA). An indocyanine bolus was administered and the SPY system was used to examine left great toe baseline perfusion. Next, a bulldog clamp was temporarily placed on the DCFA and then the TCFA as perfusion was examined with the SPY system. Toe pressures were measured at the same time.
RESULTS
When the DCFA was clamped intraoperatively, the time to maximum intensity increased from 42 to 100 seconds and T1/2 increased from 18 to 50 seconds, indicating decreased distal perfusion. Full SPY system results are listed in Table 1 and SPY graphs are pictured in Figure 2. The toe pressure dropped to 35 mm Hg with a TBI of 0.38. Upon clamp removal, toe pressure recovered to 40 mm Hg with a TBI of 0.43. We thus determined that DCFA sacrifice could result in an ischemic foot, so this vessel was preserved. With the TCFA clamped, the toe pressures and the T1/2 remained the same. An ALT flap measuring 10 cm in length and 6 cm in width was harvested based on the TCFA (Figs. 3, 4). The patient healed successfully without postoperative concerns for either flap perfusion or donor limb ischemia.
Table 1.
SPY Results
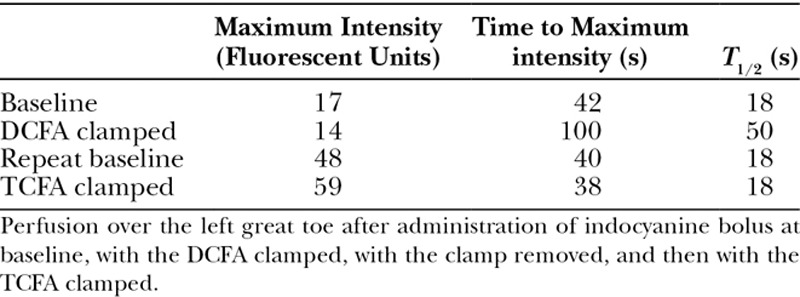
Fig. 2.
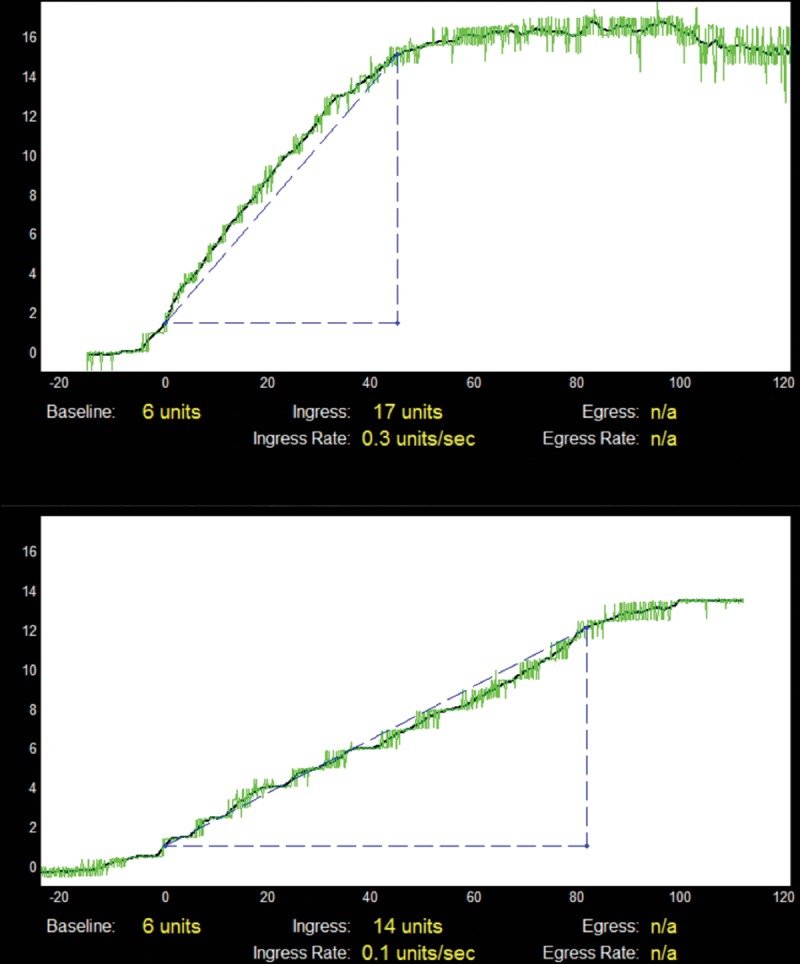
Change in SPY with the DCFA clamped. The y axis represents fluorescent units, and the x axis represents time (seconds). This graph was generated by the SPY software. Measuring left great toe perfusion, the top graph shows baseline intensity and time to maximum intensity (Tmax = 42) with no vessels clamped. With the left DCFA clamped, bottom graph reveals increased time to maximum intensity (Tmax = 100), indicating decreased toe perfusion. Slope of line (in blue) indicates ingress rate, calculated to 90% maximum to better approximate rate. Ingress is defined as the rate at which fluorescence intensity increases in the target area being captured by the infrared camera. A steeper ingress rate clinically implies improved perfusion. Single measurements of the DCFA clamped and not clamped were used.
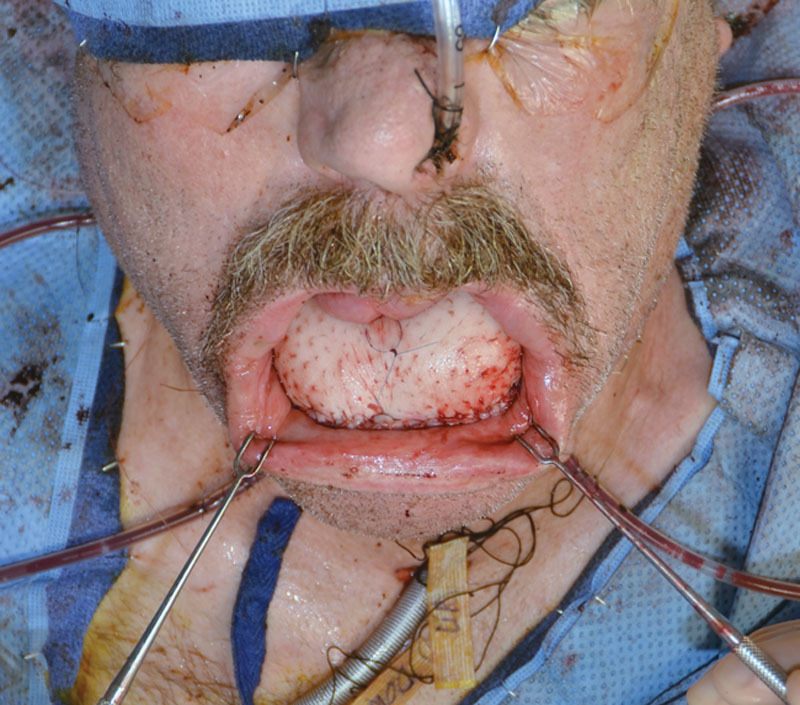
Fig. 3.

Intraoperative photograph after marginal mandibulectomy and composite oral cavity resection before inset of ALT free flap.
Fig. 4.
Intraoperative photograph after ALT free flap.
DISCUSSION
SPY technology provides a useful and novel method to predict decreased distal perfusion after vessel sacrifice for free flap harvest. Fortunately, free flap candidates with PVD so severe that a single vessel perfuses the distal lower limb are rare. In this challenging patient, when the DCFA was clamped intraoperatively, SPY technology predicted critical limb ischemia. SPY technology was thus a sensitive indicator of decreased tissue perfusion guiding perforator selection for his ALT flap.
Use of SPY technology in vascular surgery and more specifically patients with limb ischemia remains in its infancy. To our knowledge, there are currently no studies elucidating its sensitivity in detecting distal perfusion changes. We present the first report of SPY technology utilization to guide free flap arterial selection in a patient bordering on critical limb ischemia. Our successful use of SPY technology could be applied to other patients with CLI. It could also be used to detect decreased perfusion during fibular flap harvest before dividing a peroneal artery in a leg perfused by a single tibial artery or to avoid Steal phenomenon when performing an end-to-side anastomosis in a single-vessel leg receiving a free flap.
CONCLUSIONS
SPY technology was useful in selecting an arterial pedicle for an ALT free flap in a patient with severe PVD. Change in SPY time parameters and measured toe pressures enabled successful free flap design while avoiding iatrogenic critical limb ischemia.
ACKNOWLEDGMENTS
This study conforms to the Declaration of Helsinki.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Chana JS, Wei FC. A review of the advantages of the anterolateral thigh flap in head and neck reconstruction. Br J Plast Surg. 2004;57:603–609. doi: 10.1016/j.bjps.2004.05.032. [DOI] [PubMed] [Google Scholar]
- 2.Novo S, Coppola G, Milio G. Critical limb ischemia: definition and natural history. Curr Drug Targets Cardiovasc Haematol Disord. 2004;4:219–225. doi: 10.2174/1568006043335989. [DOI] [PubMed] [Google Scholar]
- 3.Labs KH, Dormandy JA, Jaeger KA, et al. Basel PAD Clinical Trial Methodology Group. Transatlantic conference on clinical trial guidelines in peripheral arterial disease: clinical trial methodology. Circulation. 1999;100:e75–e81. doi: 10.1161/01.cir.100.17.e75. [DOI] [PubMed] [Google Scholar]
- 4.Gurtner GC, Jones GE, Neligan PC, et al. Intraoperative laser angiography using the SPY system: review of the literature and recommendations for use. Ann Surg Innov Res. 2013;7:1. doi: 10.1186/1750-1164-7-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pestana IA, Coan B, Erdmann D, et al. Early experience with fluorescent angiography in free-tissue transfer reconstruction. Plast Reconstr Surg. 2009;123:1239–1244. doi: 10.1097/PRS.0b013e31819e67c1. [DOI] [PubMed] [Google Scholar]
- 6.Sacks JM, Nguyen AT, Broyles JM, et al. Near-infrared laser-assisted indocyanine green imaging for optimizing the design of the anterolateral thigh flap. Eplasty. 2012;12:e30. [PMC free article] [PubMed] [Google Scholar]
- 7.Perry D, Bharara M, Armstrong DG, et al. Intraoperative fluorescence vascular angiography: during tibial bypass. J Diabetes Sci Technol. 2012;6:204–208. doi: 10.1177/193229681200600125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Igari K, Kudo T, Toyofuku T, et al. Quantitative evaluation of the outcomes of revascularization procedures for peripheral arterial disease using indocyanine green angiography. Eur J Vasc Endovasc Surg. 2013;46:460–465. doi: 10.1016/j.ejvs.2013.07.016. [DOI] [PubMed] [Google Scholar]
- 9.Braun JD, Trinidad-Hernandez M, Perry D, et al. Early quantitative evaluation of indocyanine green angiography in patients with critical limb ischemia. J Vasc Surg. 2013;57:1213–1218. doi: 10.1016/j.jvs.2012.10.113. [DOI] [PubMed] [Google Scholar]
- 10.Brooks D. Perfusion assessment with the SPY system after arterial venous reversal for upper extremity ischemia. Plast Reconstr Surg Glob Open. 2014;2:e185. doi: 10.1097/GOX.0000000000000138. [DOI] [PMC free article] [PubMed] [Google Scholar]