

Abstract
Diaphragmatic lesions are usually congenital bronchogenic cysts. A patient with a known diaphragmatic cyst presented with new onset right upper quadrant pain. Repeat imaging showed enlargement of the cyst, the CA19–9 cancer marker was raised at 312iu/ml (normal: <27iu/ml) and positron emission tomography combined with computed tomography showed focally increased uptake in the cystic wall. In view of symptoms and risk of neoplasia, the lesion was excised. Histology showed a benign epidermoid cyst. Features falsely suggesting neoplasia have been reported previously with benign splenic cysts but not with a benign diaphragmatic epidermoid cyst.
Keywords: Epidermoid cyst, CA19–9, Positron emission tomography, Computed tomography
Diaphragmatic lesions are a rare occurrence with the majority being incidental findings on imaging. Approximately 60% represent benign pathology, and are commonly cysts, lipomas and leiomyomas.1 Malignant lesions are predominantly sarcomas but may be mesothelioma and metastases. Diaphragmatic cysts are primarily congenital bronchogenic cysts, which form in an embryo at the stage of lung development and can give the appearance of malignant disease. We present a patient with a retroperitoneal cystic lesion that highlighted some important issues related to investigations and treatment.
Case report
A 56-year-old man presented with severe right hypochondrial pain on inspiration with no other associated symptoms. His past medical history included a transient ischaemic attack and significant ischaemic heart disease, for which he was on regular clopidogrel, aspirin and a statin.
A cyst between segment 7 of the liver and the diaphragm had been an incidental finding on abdominal computed tomography (CT) four years previously. It was unclear whether the cyst was arising from the liver parenchyma or the diaphragm.
Abdominal ultrasonography failed to demonstrate gallstones so the patient proceeded to intravenous contrast CT of the abdomen. The cyst was again demonstrated but had increased from 32mm to 66mm in maximal diameter (Fig 1).
Figure 1.
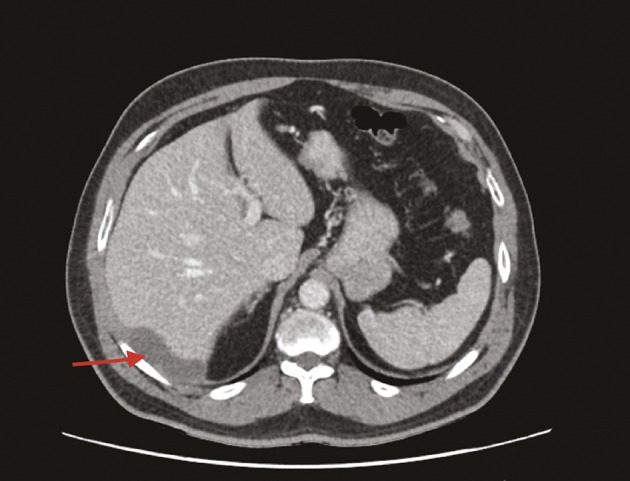
Preoperative computed tomography with arrow showing the cyst between liver and right hemidiaphragm
Liver function tests were normal. CA19–9 was grossly elevated at 312iu/ml (normal: <27iu/ml) while carcinoembryonic antigen (CEA) was 2g/l (normal: <3g/l). CA125 was not measured. All other bloods tests were within normal limits, including inflammatory markers. Positron emission tomography CT (PET-CT) was performed, which demonstrated significant uptake in the wall of the cyst but no disease elsewhere.
The lesion was resected with a 1cm margin of clearance and the defect in the diaphragm was repaired with a Peri-Guard® synthetic mesh (Synovis, St Paul, MN, US). The patient had an uncomplicated postoperative recovery. The resected specimen demonstrated a retroperitoneal epidermoid cyst arising from the diaphragm. There were no features to suggest malignancy. Repeat CA19–9 levels checked two months postoperatively showed that this had returned to within normal limits (5iu/ml).
Discussion
This particular case presented significant preoperative diagnostic difficulty. Preoperative imaging showed a cystic lesion between the liver and the diaphragm. The investigations prior to surgery demonstrated cyst growth and elevated CA19–9 with normal CEA and increased uptake on PET-CT, all of which suggest a malignant process.
Diaphragmatic cysts are a rare occurrence and as such, little is known of their natural history. Of those described in the literature, around 60% are benign.
CA19–9 is a tumour marker that is associated with malignancies of the biliary tract and is raised in approximately 80% of pancreatic malignancies. CA19–9 can be elevated in benign conditions of the biliary tree but not generally to such consistently high levels as we encountered in our patient. A CA19–9 level of over 300iu/ml was found in 63% of patients with a pancreatic malignancy but only in 6% of patients with benign biliary disease.2
There is one case in the literature of an 11-year-old boy with a diaphragmatic cyst but CA19–9 was not measured.3 This cyst was resected laparoscopically.
There have been several reports of epidermoid splenic cysts with associated elevated tumour markers including CA19–9.4,5 Similar to our case, the CA19–9 returns to normal levels following resection of the cyst. A cyst in this location with raised CA19–9 has not been described before.
PET-CT identifies areas of increased metabolism owing to increased uptake of fludeoxyglucose. It is used routinely to investigate possible cancers owing to the increased metabolism and hence increased uptake of malignant tissues. As a result of increased metabolism in inflamed tissues, false positives can arise. There was, however, no indication of inflammation at the cyst and the patient’s inflammatory markers were within normal limits. It therefore remains unclear why the PET-CT was positive.
Conclusions
Although some case series have identified a policy of conservative management for splenic epidermoid cysts with raised CA19–9 and of reserving surgery for large symptomatic cysts, the combination of raised CA19–9 in a cyst in this anatomical location, recent growth of the cyst and positive PET-CT prompted the decision to proceed to open resection. In our patient, despite a significant body of preoperative evidence suggesting a malignant process, the pathology encountered was benign.
References
- 1.Kim MP, Hofstetter WL. Tumors of the diaphragm. Thorac Surg Clin 2009; : 521–529. [DOI] [PubMed] [Google Scholar]
- 2.Haglund C,Roberts PJ, Kuusela P et al. Evaluation of CA 19–9 as a serum tumour marker in pancreatic cancer. Br J Cancer 1986; : 197–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hagr A,Laberge JM,Nguyen LT et al. Laparoscopic excision of subdiaphragmatic epidermoid cyst: a case report. J Pediatr Surg 2001; : E8. [DOI] [PubMed] [Google Scholar]
- 4.Paksoy M,Karabicak I, Kusaslan R et al. Laparoscopic splenic total cystectomy in a patient with elevated CA 19–9. JSLS 2006; : 507–510. [PMC free article] [PubMed] [Google Scholar]
- 5.Inokuma T, Minami S, Suga K et al. Spontaneously ruptured giant splenic cyst with elevated serum levels of CA 19–9, CA 125 and carcinoembryonic antigen. Case Rep Gastroenterol 2010; : 191–197. [DOI] [PMC free article] [PubMed] [Google Scholar]