

Abstract
Background
A large proportion of European children, adults and older adults do not engage in sufficient physical activity (PA). Understanding individual and contextual factors associated with PA behaviours is essential for the identification and implementation of effective preventative environments, policies, and programmes that can promote an active lifestyle across life course and can potentially improve health. The current paper intends to provide 1) a multi-disciplinary, Pan-European and life course view of key determinants of PA behaviours and 2) a proposal of how these factors may cluster.
Methods
After gathering a list of 183 potential PA behaviours-associated factors and a consensus meeting to unify/consolidate terminology, a concept mapping software was used to collate European experts’ views of 106 identified factors for youth (<19 years), adults (19–64 years), and older adults (≥65 years). The analysis evaluated common trends in the clustering of factors and the ratings of the distinct factors’ expected modifiability and population-level impact on PA behaviours across the life course. Priority for research was also assessed for each cluster.
Results
The concept mapping resulted in six distinct clusters, broadly merged in two themes: 1) the ‘Person’, which included clusters ‘Intra-Personal Context and Wellbeing’ and ‘Family and Social Economic Status’ (42 % of all factors) and 2) the ‘Society’, which included the remaining four clusters ‘Policy and Provision’, ‘Cultural Context and Media’, ‘Social Support and Modelling’, and ‘Supportive Environment’ (58 % of all factors). Overall, 25 factors were rated as the most impactful on PA behaviours across the life course and being the most modifiable. They were mostly situated in the ‘Intra-Personal Context and Wellbeing’ cluster. Furthermore, 16 of them were rated as top priority for research.
Conclusions
The current framework provides a preliminary overview of factors which may account for PA behaviour across the life course and are most relevant to the European community. These insights could potentially be a foundation for future Pan-European research on how these factors might interact with each other, and assist policy makers to identify appropriate interventions to maximize PA behaviours and thus the health of European citizens.
Keywords: Factors, Active lifestyles, Youth, Adults, Older adults, Priority for research
Background
In line with the World Health Organization’s Global Status Report on Noncommunicable Diseases [1], the Council of the European Union [2] has recognised the value of physical activity (PA) for health and has provided recommendations on promoting health-enhancing physical activity (HEPA) across sectors and age groups. The policies of the European Union (EU) also strongly support grassroots and competitive sports [3], which are deeply intertwined with active lifestyles and represent an important opportunity to develop, transfer and/or implement regular PA practices [4], and to foster social inclusion, integration, and gender equality [5–8]. Unfortunately, the majority of European citizens do not engage in sufficient structured (e.g., physical exercise and sports) and/or unstructured (e.g., movements linked with daily life) PA, with a large proportion of children, adults, and older adults adopting inactive lifestyles [9–11]. To counteract the growing social and economic costs of lifestyle-related diseases, the European platform for action on diet, PA, and health aims to increase engagement in PA in the life course of citizens, to foster research for a better understanding of HEPA, and to boost and disseminate effective health policies for the promotion of environments and values supportive of an active lifestyle [5].
Whether or not individuals choose a healthy lifestyle is influenced by a number of inter-dependent and multilevel factors. Several theories and models have been proposed to facilitate the exploration of active lifestyle choice [12]. Recently, ecological perspectives have been proposed as an effective approach in combating current physical inactivity levels [13–17]. Such comprehensive models commonly include individual (e.g., biological, psychological, and behavioural aspects), interpersonal (e.g., relationships with parents, relatives, peers, and socio-cultural networks), environmental (e.g., access/availability of tools/services, and proximal/distal built/natural surroundings), and policy (e.g., organizational and governmental aspects) dimensions. Existing models provide a valuable overview but have not used a systematic methodology (e.g., concept mapping) to engage and analyse multi-disciplinary views, to specify the interrelations between the identified factors that might mediate or moderate PA behaviours, or to indicate how these factors may vary across the life course. To identify key factors that promote or inhibit PA behaviours, an agreed consensus framework, which contains sufficient detail to drive the future research agenda, is necessary. This agenda should focus on how these various factors interact with each other and how individual and population variation in these factors and in their interaction have a causal impact on behaviour and health.
The vehicle for the current research is the Thematic Area 2 of the DEterminants of DIet and Physical ACtivity Knowledge Hub (DEDIPAC-KH). To address the complex social and health phenomenon of healthy lifestyles behaviours in Europe, the European Commission endorsed a Joint Programming Initiative to increase research capacity across Member States to engage in a common research agenda [18]. Twelve Member States adopted this strategy and supported the DEDIPAC-KH to realise joint collaboration and harmonisation among different scientific disciplines, to expand knowledge, to develop new insights and solutions in the stated domains of behaviours, and to prepare the ground for building a coherent approach towards diet and PA behaviours research at European level [19]. Within the DEDIPAC-KH, a cross-disciplinary team coordinated and integrated collaborative research efforts to address the theoretical and practical challenges related to the determinants of PA behaviours and their changes across the life course. The partners recognised the need to identify priorities, to create a unified vision among stakeholders, and to guide future research in Europe. Such harmonisation is essential if meaningful research breakthroughs in the understanding of behaviour and lifestyle choice are to be made. In particular, in the current paper the terms determinants and factors are used interchangeable because they are both referring to the factors associated with PA behaviour. The identification of key factors or distinct clusters of factors, which are known to contribute to behaviour choice, as well as their level of modifiability and priority to research, will facilitate European and national policy makers in planning more effective behaviour enhancing public health policies [20].
According to the literature [21–26], concept mapping is deemed a valuable systematic methodology that involves a system-based approach to integrate ideas across multi-, inter-, trans-disciplinary, and professional knowledge in order to improve theory development as a sound basis for public health policies [20]. The concept mapping procedure requests participants to generate and structure statements and to identify relevant factors related to the question of interest (e.g., determinants of PA behaviours). The subsequent sorting and rating of suggested factors allows the identification of distinct clusters [27], which are represented in a two-dimensional concept map [28]. Clusters located close to each other carry a similar meaning, whereas distant ones are less related [29]. The involvement of a diversity of experts and disciplines is a core strength, which provides a comprehensive theoretical base to inform the concept mapping analysis [30]. This method of rating, clustering and visually mapping concepts by experts and stakeholders has been applied to create logic models to integrate practical knowledge with scientific knowledge for applied decision-making in public health [20, 31–36] and to gain insights into promising active living intervention strategies [37–39].
The primary aim of the current study was to develop, using a concept mapping approach, a EUropean Physical Activity Determinants (EU-PAD) framework to be indicative of the current understanding of PA determinants, which can underpin the future European research agenda and contribute to improving the active lifestyles of European citizens across the life course. The proposed characteristics of the framework were as follows: 1) a European and life-course view of key factors; 2) additional definition regarding the specific nature of the factors when compared to exiting models; and 3) propose how these factors may group into clusters. It is anticipated that the framework will provide significant guidance to future determinant research within Europe and will also provide a structure to increase collaboration and the harmonisation of research methodologies.
Methods
According to the literature on defining and conceptualising complex public health systems with many interacting parts acting at different levels [22–26, 28, 30–35, 37–40], a structured consensus protocol has been developed based on concept mapping. In particular, this method combines qualitative opinions with multivariate statistical analysis to enable a synthesis of experts’ opinions to gather and organise views into a conceptual framework. In line with a parallel DEDIPAC-KH study on systems of sedentary behaviours [41], in the present study data collection, accomplished between December 2013 and December 2015, encompassed multi-method means, including paper forms, face-to-face interactions, and web-based platforms organized in four main phases (Table 1): (I) preparation (terminology, protocol and inclusion criteria of experts), (II) generation of statements, (III) structuring (sorting and rating), (IV) analysis and interpretation. In particular, the development of the EU-PAD framework benefited from the engagement of the members of the DEDIPAC-KH research team and involved also a panel of Pan-European multi-disciplinary experts in areas directly or indirectly related to PA and sport. Data analysis from each phase was necessary before progressing to the following one.
Table 1.
Concept mapping stages, content, time frame and characteristics of participants
| Stage | Content | Time Frame | Participants |
|---|---|---|---|
| Preparation | Terminology, Protocol and Inclusion Criteria of Experts | December 2013-December 2014 | DEDIPAC-KH Research Team |
| Generation of Statements | Maps (brainstorming): 183 Factors | January-June 2015 | |
| Factors Sorting: 106 Factors | |||
| Pilot Sorting and Rating | |||
| Synthesis | |||
| Identification and Recruitment of EU Experts | |||
| Structuring | Sorting and Rating of Factors | July-September 2015 | EU Experts |
| Analysis and Interpretation | Preliminary Analysis and Interpretation (Delphi) | October-December 2015 | DEDIPAC-KH Research Team |
| Final Consensus | EU Experts |
Preparation (terminology, protocol and inclusion criteria of experts)
Considering that PA definitions often lack sufficient detail and present homonymous terms that lead to confusion and difficulty in communication [42, 43], the DEDIPAC-KH research team (consisting of 23 participants from five partner nations) deemed necessary to agree on a DEDIPAC-KH consensus on common nomenclature for PA. In this study, PA encompasses any bodily movement produced by skeletal muscles that results in energy expenditure, which may be unstructured and everyday life activity, exercise that includes prearranged, deliberate and repetitive activity [44–47], and grassroots sports and competitive sports [4].
The DEDIPAC-KH research team developed a protocol to articulate the goal of the present study (i.e., “the development of a framework indicative of the current understanding of PA determinants which can underpin the future European research agenda and contribute to improving the active lifestyles of European citizens across the life course”). Then, standard operating procedures [41] were provided to the members of the DEDIPAC-KH research team to individually establish in an open-ended and non-judgmental fashion an exhaustive list of all potential factors that could influence PA behaviours for youth (<19 years), adult (19–64 years), and older adult (≥65 years) populations, and to organize them into graphic representations to uncover the salient associations among factors and map their importance and modifiability.
To identify and recruit European experts, the DEDIPAC-KH research team conducted a focused search for multi-disciplinary specialists with particular attention to categories of European stakeholders having a relevant role in PA and sport. The following inclusion criteria were used: Experts affiliated with European organizations (President, Secretary, Manager of European institutions/organizations in HEPA, leisure and recreation, and sport; members of national sports departments; partners in relevant European co-funded PA projects), and experts affiliated with academic or research institutions. In particular, a snowball reputation-based sampling procedure was used to ensure an adequate recruitment of European scholars based on their expertise in PA research within the designated categories of the European Research Council Primary Panel Structure (e.g., Life Sciences, Social Sciences and Humanities, and Physical Sciences and Engineering). Thus, 373 European experts were identified.
According to the literature on online surveys for academic research [48, 49], a pre-notification email providing information on the development of the EU-PAD framework was prepared for the online recruitment of the identified European experts received. Participation in the task was deemed voluntary and participants could withdraw from the study at any time without providing any reason, and incomplete response would not be considered. Informed consent was assumed with subjects’ reply that they were willing to participate. Furthermore, follow-up contacts have been planned to increase response rates [48, 49], especially important for online surveys including >20 items as they demand long time from the respondent [48]. Considering that the response rate for e-mail surveys tend to be lower than that of traditional mail surveys [49, 50], and when representatives of organizations are involved [51] especially for time consuming responses [48], a response rate between 20 and 30 % was considered fair [52].
Generation of statements
During a workshop, the DEDIPAC-KH research team analysed a list of 183 potential factors associated with PA behaviours by eliminating repetitions, rewording similar statements, and condensing highly specific statements into broader ones. Thus, a synthesis of 106 factors was identified (see numbered items in Table 2). Each factor was individually rated on a Likert-type scale from 1 (lowest value) to 5 (highest value) regarding its level of modifiability (‘To what extent is a factor modifiable at any point across the life course?’) and population-level effect (‘To what extent does a factor have an expected impact on PA behaviours at the youth/adult/older adult population-level?’) for the three life course stages. The internal consistency of factors was ascertained by means of reliability estimates, considering a Cronbach’s alpha coefficient of ≥0.7 acceptable for internal consistency [53]. Based on the outcomes of the above process, the synthesis of the 106 factors was approved for the next phase of the research.
Table 2.
List of identified factors by cluster in ascending order
| Factor # |
Statement by cluster | Priority for Research |
Modifiability | Population Level Effect | p | ||
|---|---|---|---|---|---|---|---|
| Youth | Adult | Old Adult | |||||
| Cluster 1: Intra-Personal Context and Wellbeing | |||||||
| 3 | Actual Body Mass Index | 3.6 ± 0.7 | 3.6 ± 1.1 | 3.4 ± 1.0 | 3.8 ± 0.9 | 3.4 ± 1.0 | 0.032 |
| 4 | Actual PA level | 4.1 ± 0.6 | 4.1 ± 0.8 | 3.9 ± 1.0 | 4.1 ± 0.8 | 4.0 ± 1.0 | n.s. |
| 5 | Addictions (Smoking Gambling Drugs) | 3.0 ± 0.8 | 3.1 ± 1.1 | 2.7 ± 1.2b | 3.2 ± 1.1a | 2.9 ± 1.2 | 0.015 |
| 7 | Age | 2.4 ± 1.0 | 1.8 ± 1.4 | 3.0 ± 1.4c | 3.2 ± 1.4 | 3.7 ± 1.3a | 0.002 |
| 10 | Beliefs/Values | 3.3 ± 0.8 | 3.2 ± 1.0 | 3.3 ± 1.2 | 3.6 ± 1.1 | 3.6 ± 1.1 | n.s. |
| 11 | Capability to Combine Sport and Education/Work Requirements (Dual Career) | 3.1 ± 0.7 | 3.2 ± 1.0 | 3.4 ± 1.3c | 3.8 ± 1.1c | 1.7 ± 1.0ab | <0.001 |
| 14 | Cognitive Function | 3.0 ± 0.9 | 2.7 ± 1.1 | 3.0 ± 1.3c | 3.1 ± 1.2c | 3.9 ± 1.0ab | <0.001 |
| 15 | Conscious Control of Automated Body Movements | 3.0 ± 0.9 | 3.0 ± 1.1 | 2.9 ± 1.1 | 2.8 ± 1.2 | 3.2 ± 1.3 | n.s. |
| 23 | Emotions | 3.3 ± 0.9 | 3.1 ± 1.3 | 3.5 ± 1.0 | 3.4 ± 1.0 | 3.5 ± 1.1 | n.s. |
| 26 | Fear of Injuries/Falling | 3.1 ± 0.6 | 3.0 ± 0.9 | 2.3 ± 1.1bc | 2.9 ± 0.9ac | 4.6 ± 0.6ab | <0.001 |
| 27 | Feeling of Inadequacy (Too Clumsy/Too Old)/Teasing | 3.3 ± 0.7 | 3.1 ± 1.0 | 3.5 ± 1.1 | 3.2 ± 0.8c | 3.6 ± 1.1b | 0.024 |
| 31 | Gender | 2.1 ± 0.8 | 1.5 ± 1.0 | 2.8 ± 1.3 | 2.7 ± 1.2 | 2.7 ± 1.2 | n.s. |
| 33 | Genetics/Talent | 2.0 ± 0.7 | 1.5 ± 0.9 | 2.9 ± 1.2bc | 2.4 ± 1.2a | 2.2 ± 1.3a | <0.001 |
| 38 | Health Status | 3.7 ± 0.7 | 3.3 ± 0.9 | 3.4 ± 1.1bc | 4.0 ± 0.9ac | 4.4 ± 0.8ab | <0.001 |
| 39 | Hormesis (Dose–response)/Training Response | 2.7 ± 0.9 | 2.7 ± 1.2 | 2.6 ± 1.1 | 2.9 ± 1.0 | 2.6 ± 1.0 | n.s. |
| 41 | Intentions/Attitudes | 3.5 ± 0.8 | 3.4 ± 1.0 | 3.5 ± 1.0 | 3.8 ± 1.1 | 3.8 ± 1.1 | n.s. |
| 44 | Job/Occupation-Related Energy Expenditure | 2.8 ± 0.8 | 2.8 ± 1.2 | 2.2 ± 1.1b | 3.7 ± 1.1ac | 2.0 ± 1.1ab | <0.001 |
| 46 | Level of Autonomy/Time Management | 3.4 ± 0.7 | 3.4 ± 1.0 | 2.9 ± 1.0bc | 3.9 ± 1.0ac | 3.4 ± 1.1ab | <0.001 |
| 47 | Life Satisfaction | 3.4 ± 0.8 | 3.3 ± 0.9 | 2.9 ± 1.2bc | 3.7 ± 1.0a | 3.8 ± 1.0a | <0.001 |
| 57 | Overweight/Obesity In Previous Years | 2.6 ± 0.7 | 2.0 ± 1.1 | 3.1 ± 1.1b | 3.5 ± 1.1a | 3.3 ± 1.1 | 0.028 |
| 64 | Past Exercise Behaviour/Experience | 2.7 ± 0.8 | 1.9 ± 1.2 | 3.2 ± 1.2c | 3.5 ± 1.1 | 3.8 ± 1.1a | 0.003 |
| 65 | Perceived Barriers | 3.4 ± 0.7 | 3.2 ± 1.0 | 3.3 ± 1.1c | 3.6 ± 1.0c | 4.1 ± 0.9ab | <0.001 |
| 66 | Perceived Benefits of PA | 3.7 ± 0.7 | 3.7 ± 1.0 | 3.1 ± 1.2bc | 3.9 ± 1.0a | 4.0 ± 0.9a | <0.001 |
| 67 | Perceived Fatigue/Adverse Physiological Response | 3.3 ± 0.8 | 3.2 ± 1.0 | 3.0 ± 1.1c | 3.4 ± 1.0§ | 3.9 ± 1.0ab | <0.001 |
| 68 | Perceived Safe Environment | 3.3 ± 0.7 | 3.1 ± 1.0 | 3.1 ± 1.2§ | 3.3 ± 0.9c | 4.0 ± 0.9ab | <0.001 |
| 70 | Perceived Stress/Life Stressors | 3.1 ± 0.7 | 3.0 ± 1.0 | 2.8 ± 1.2bc | 3.7 ± 0.9ac | 3.3 ± 0.9ab | <0.001 |
| 71 | Personal Goals/Outcome Expectancies/Achievement Orientation/Motivation | 3.8 ± 0.7 | 3.8 ± 1.0 | 3.6 ± 1.2a | 4.1 ± 1.0a | 3.8 ± 1.0 | 0.026 |
| 72 | Personality Traits | 2.8 ± 1.0 | 2.3 ± 1.1 | 3.2 ± 1.2 | 3.4 ± 1.2 | 3.3 ± 1.3 | n.s. |
| 73 | Physical Fitness Levels (Strength, Endurance, Coordination, Agility, Flexibility) | 3.9 ± 0.7 | 3.9 ± 0.9 | 3.7 ± 1.0 | 3.7 ± 1.0c | 4.1 ± 1.0b | 0.022 |
| 76 | Psychological Disorders (Depression, Eating Disorders, Emotional Symptoms) | 3.1 ± 0.8 | 2.8 ± 1.0 | 3.0 ± 1.2c | 3.4 ± 1.2 | 3.6 ± 1.0a | 0.002 |
| 85 | Self PA Monitoring | 3.5 ± 0.7 | 3.6 ± 1.1 | 3.1 ± 1.2b | 3.6 ± 0.8ac | 3.2 ± 0.9b | 0.002 |
| 86 | Self Perceptions (Awareness, Confidence, Efficacy, Body Image, PA level) | 3.6 ± 0.8 | 3.4 ± 1.0 | 3.5 ± 1.0 | 3.8 ± 1.0 | 3.7 ± 1.0 | n.s. |
| 87 | Self-Regulatory Ability | 3.2 ± 0.9 | 3.2 ± 1.2 | 3.0 ± 1.0bc | 3.4 ± 1.1a | 3.5 ± 0.9a | 0.003 |
| 88 | Sensation Seeking | 2.6 ± 0.9 | 2.5 ± 1.8 | 3.0 ± 1.3c | 2.9 ± 1.2c | 2.2 ± 1.0ab | <0.001 |
| 89 | Sleep Quality/Quantity | 3.2 ± 0.9 | 3.2 ± 1.1 | 3.1 ± 1.2c | 3.3 ± 1.1 | 3.6 ± 1.0a | 0.012 |
| 98 | Sub-Pathology/Pathology/Injuries/Pain/Rehabilitation | 3.0 ± 0.8 | 2.6 ± 1.1 | 2.6 ± 1.2bc | 3.2 ± 1.1ac | 4.0 ± 1.1ab | <0.001 |
| 100 | Time Availability | 3.3 ± 0.7 | 3.2 ± 1.0 | 3.3 ± 1.0bc | 4.2 ± 0.8ac | 2.8 ± 1.1ab | <0.001 |
| Cluster 2: Family and Socio-Economic Status | |||||||
| 22 | Educational Level (Parents/Relatives) | 2.6 ± 0.8 | 2.1 ± 1.2 | 3.4 ± 1.1c | 3.2 ± 1.1 | 2.8 ± 1.3a | 0.003 |
| 25 | Ethnicity | 1.9 ± 0.7 | 1.5 ± 1.0 | 2.4 ± 1.1 | 2.2 ± 1.0 | 2.4 ± 1.2 | n.s. |
| 51 | Marital Status (for Children: Marital Status of Parents) | 2.4 ± 0.8 | 2.3 ± 1.2 | 2.1 ± 1.0bc | 2.8 ± 1.1a | 2.7 ± 1.2a | <0.001 |
| 63 | Parents/Relatives/Peers Body Mass Index | 2.5 ± 0.8 | 2.3 ± 1.1 | 3.0 ± 1.1c | 2.8 ± 1.1c | 2.2 ± 1.1ab | <0.001 |
| 69 | Perceived Social Role | 3.0 ± 0.8 | 2.9 ± 1.0 | 3.0 ± 1.3 | 3.1 ± 0.9 | 3.0 ± 1.0 | n.s. |
| 81 | Rewards (Encouragement/Support) | 3.5 ± 0.8 | 3.7 ± 1.0 | 3.7 ± 1.2bc | 3.2 ± 1.0a | 3.1 ± 1.0a | <0.001 |
| 90 | Social Competence/Role | 3.0 ± 0.8 | 3.0 ± 1.0 | 2.9 ± 1.2 | 3.1 ± 1.0 | 3.1 ± 1.0 | n.s. |
| 91 | Social Economic Status/Personal Income (for Children: Parents’ Income)/ Level of Education | 2.9 ± 0.8 | 2.5 ± 1.0 | 3.4 ± 0.9 | 3.5 ± 0.9 | 3.3 ± 1.0 | n.s. |
| Cluster 3: Policy and Provision | |||||||
| 1 | Academic Training Programmes for Health Practitioners | 3.2 ± 0.8 | 3.7 ± 1.1 | 2.7 ± 1.2 | 2.8 ± 1.1 | 2.9 ± 1.2 | n.s. |
| 8 | Architecture and Urbanization (Availability/Access/Proximity of Elevators Escalators Facilities In Public Buildings) |
3.0 ± 0.9 | 2.9 ± 1.2 | 2.8 ± 1.0bc | 3.2 ± 1.1a | 3.5 ± 1.1a | <0.001 |
| 9 | Availability/Access/Proximity of PA Organized Sport Facilities Tools | 3.6 ± 0.7 | 3.4 ± 1.0 | 3.9 ± 0.8 | 3.6 ± 0.9 | 3.7 ± 1.0 | n.s. |
| 12 | City Planning | 3.0 ± 0.9 | 3.0 ± 1.1 | 2.8 ± 1.1 | 3.1 ± 1.1 | 3.1 ± 1.1 | n.s. |
| 13 | City/Nation Density | 2.0 ± 0.8 | 1.8 ± 0.9 | 2.1 ± 1.1 | 2.1 ± 1.0 | 2.2 ± 1.1 | n.s. |
| 16 | Corporate Social Responsibilities | 2.6 ± 0.8 | 2.8 ± 1.0 | 2.1 ± 1.0b | 2.7 ± 1.1a | 2.3 ± 1.1 | 0.004 |
| 17 | Corporate Social Responsibility Interventions | 2.8 ± 0.7 | 3.0 ± 1.0 | 2.3 ± 1.2b | 2.9 ± 1.1ac | 2.3 ± 1.2b | 0.001 |
| 20 | Distance to School/Work/Destination | 3.0 ± 0.7 | 2.7 ± 1.0 | 3.5 ± 0.9c | 3.5 ± 1.1c | 2.8 ± 1.4ab | <0.001 |
| 21 | Education Policies | 2.9 ± 0.9 | 3.2 ± 1.1 | 3.6 ± 1.1bc | 2.3 ± 1.1a | 2.1 ± 1.1a | <0.001 |
| 24 | Environmental Policies | 3.0 ± 0.9 | 3.3 ± 1.1 | 2.6 ± 1.1 | 2.8 ± 1.1 | 2.7 ± 1.0 | n.s. |
| 28 | Financial Measures and Regulation for PA and Sport | 3.0 ± 0.8 | 3.0 ± 1.1 | 2.9 ± 1.0 | 3.0 ± 1.0 | 2.7 ± 1.1 | n.s. |
| 29 | Fiscal Advantages For Sport Clubs/PA Services | 2.9 ± 0.9 | 3.0 ± 1.1 | 2.8 ± 1.1 | 2.9 ± 1.2 | 2.5 ± 1.1 | n.s. |
| 30 | Funding for Sport Federation | 2.7 ± 0.8 | 3.0 ± 1.0 | 2.7 ± 1.0c | 2.5 ± 1.0c | 2.1 ± 1.0ab | <0.001 |
| 37 | Health Education | 3.5 ± 0.7 | 3.7 ± 1.1 | 3.3 ± 1.2 | 3.3 ± 1.0 | 3.3 ± 1.0 | n.s. |
| 40 | Indoor Condition (Air Conditioning) | 2.8 ± 0.8 | 3.1 ± 1.2 | 2.1 ± 0.9c | 2.4 ± 0.8 | 2.8 ± 1.0a | <0.001 |
| 45 | Leisure Activity Subsidy | 3.0 ± 0.8 | 2.9 ± 1.1 | 3.0 ± 1.0 | 3.0 ± 1.0 | 3.0 ± 1.1 | n.s. |
| 48 | Lobbying | 2.4 ± 0.9 | 2.8 ± 1.3 | 1.9 ± 1.0 | 2.3 ± 1.1 | 2.0 ± 1.0 | n.s. |
| 50 | Mandatory PA in Community/Schools | 3.1 ± 0.8 | 3.4 ± 1.1 | 4.0 ± 1.0bc | 2.4 ± 1.1a | 2.3 ± 1.3a | <0.001 |
| 53 | Media and Advertising Regulation by Public Authorities Corporate Social Responsibility Programmes |
3.0 ± 0.8 | 3.2 ± 1.1 | 2.8 ± 1.2 | 2.8 ± 1.1 | 2.5 ± 1.0 | n.s. |
| 54 | Mobility Policy | 2.8 ± 0.9 | 3.0 ± 1.2 | 2.4 ± 1.0c | 2.6 ± 1.1c | 3.1 ± 1.2ab | <0.001 |
| 56 | Outdoor Condition (Pollution and Weather-Season) | 2.6 ± 0.6 | 2.3 ± 1.1 | 2.8 ± 1.0c | 3.0 ± 0.9c | 3.4 ± 1.0ab | <0.001 |
| 58 | PA and Sport Organizations Advocacy | 3.1 ± 0.9 | 3.2 ± 1.1 | 3.1 ± 1.1 | 2.9 ± 1.1 | 2.8 ± 1.2 | n.s. |
| 59 | PA Education (at School/Work)/Knowledge of Effects of PA | 3.4 ± 0.9 | 3.6 ± 1.1 | 3.7 ± 1.1bc | 3.2 ± 1.3a | 2.8 ± 1.1a | <0.001 |
| 60 | PA Programs in School/Office/Community | 3.6 ± 0.8 | 3.6 ± 1.0 | 4.1 ± 1.0bc | 3.4 ± 1.1a | 3.4 ± 1.2a | <0.001 |
| 61 | PA Programs/Plans | 3.6 ± 0.8 | 3.6 ± 1.1 | 3.8 ± 1.0 | 3.5 ± 1.1 | 3.6 ± 1.1 | n.s. |
| 77 | Public Health | 3.0 ± 0.8 | 2.9 ± 1.1 | 2.5 ± 1.1bc | 3.1 ± 1.1a | 3.4 ± 1.1a | <0.001 |
| 78 | Public Organized Sport Events/PA Activities (Field Trips) | 3.4 ± 0.7 | 3.6 ± 1.0 | 3.4 ± 1.0 | 3.0 ± 1.0 | 3.3 ± 1.1 | n.s. |
| 79 | Public Transport Policies | 3.0 ± 0.9 | 3.0 ± 1.1 | 2.7 ± 1.0 | 2.9 ± 1.1 | 3.2 ± 1.0 | n.s. |
| 80 | Public Transport System | 3.1 ± 0.8 | 3.0 ± 1.1 | 3.1 ± 0.9 | 3.0 ± 1.1c | 3.4 ± 1.0b | 0.034 |
| 82 | Rights of Citizenship | 1.9 ± 0.8 | 2.1 ± 1.1 | 1.7 ± 0.9 | 1.9 ± 0.9 | 1.7 ± 0.9 | n.s. |
| 83 | School/Office Hours | 2.7 ± 0.7 | 2.5 ± 1.0 | 3.3 ± 1.1bc | 3.8 ± 0.9ac | 1.7 ± 0.9ab | <0.001 |
| 84 | School/Office Space | 2.7 ± 0.8 | 2.7 ± 1.1 | 3.5 ± 1.1c | 3.2 ± 1.2c | 1.6 ± 0.8ab | <0.001 |
| 96 | Sport Science Research | 3.1 ± 0.9 | 3.5 ± 1.2 | 2.6 ± 1.1 | 2.7 ± 1.1 | 2.5 ± 1.1 | n.s. |
| 97 | Sports Facilities | 3.4 ± 0.7 | 3.3 ± 1.1 | 3.7 ± 0.9c | 3.7 ± 0.8c | 3.2 ± 0.9ab | 0.001 |
| 102 | Traffic | 2.7 ± 0.9 | 2.6 ± 1.1 | 2.7 ± 1.1 | 2.8 ± 1.0 | 2.9 ± 1.2 | n.s. |
| 103 | Traffic Policies | 2.8 ± 0.9 | 2.9 ± 1.2 | 2.5 ± 1.1 | 2.8 ± 1.0 | 2.8 ± 1.2 | n.s. |
| 104 | Transport Policies | 2.9 ± 0.9 | 3.0 ± 1.2 | 2.6 ± 1.1c | 2.8 ± 1.1 | 3.1 ± 1.2a | 0.014 |
| 106 | Urban Planning Policies | 3.0 ± 1.0 | 3.0 ± 1.2 | 2.8 ± 1.1 | 2.9 ± 1.2 | 3.0 ± 1.2 | n.s. |
| Cluster 4: Cultural Context and Media | |||||||
| 6 | Advertisement | 3.1 ± 0.9 | 3.3 ± 1.2 | 3.1 ± 1.1c | 2.8 ± 1.0 | 2.6 ± 1.1a | 0.004 |
| 18 | Cultural Climate | 2.6 ± 0.8 | 2.4 ± 1.0 | 2.8 ± 1.1 | 2.9 ± 1.1 | 2.9 ± 1.2 | n.s. |
| 19 | Cyber Space | 2.7 ± 0.9 | 3.0 ± 1.3 | 3.3 ± 1.4bc | 2.5 ± 1.1ac | 1.8 ± 0.9ab | <0.001 |
| 32 | Gender Equality | 2.6 ± 0.8 | 2.6 ± 1.1 | 2.7 ± 1.3 | 2.8 ± 1.2c | 2.3 ± 1.0b | 0.040 |
| 35 | Group Activity (Outdoor/Indoor) | 3.6 ± 0.7 | 3.5 ± 0.9 | 3.8 ± 0.8b | 3.5 ± 0.8a | 3.8 ± 0.9 | 0.016 |
| 42 | Internet Availability | 3.1 ± 0.9 | 3.4 ± 1.2 | 3.3 ± 1.2bc | 2.7 ± 1.2ac | 2.1 ± 1.0ab | <0.001 |
| 49 | Local/National/Traditions Identity | 2.3 ± 0.9 | 2.0 ± 1.0 | 2.6 ± 1.2 | 2.5 ± 1.1 | 2.6 ± 1.1 | n.s. |
| 52 | Media | 3.2 ± 0.8 | 3.3 ± 1.1 | 3.4 ± 1.1c | 3.0 ± 1.1 | 2.7 ± 1.0a | 0.001 |
| 94 | Social Media | 3.2 ± 0.9 | 3.5 ± 1.2 | 3.7 ± 1.2bc | 3.0 ± 1.0ac | 2.2 ± 0.9ab | <0.001 |
| 95 | Social Trends | 3.0 ± 0.8 | 3.0 ± 1.1 | 3.3 ± 1.2c | 3.2 ± 1.0c | 2.6 ± 0.9ab | <0.001 |
| 105 | Tv Exposure | 3.6 ± 1.0 | 3.7 ± 1.2 | 3.8 ± 1.1bc | 3.3 ± 1.1a | 3.1 ± 1.4a | 0.001 |
| Cluster 5: Social Support and Modelling | |||||||
| 34 | Group (Family Peers Partner) PA Behaviours | 3.5 ± 0.6 | 3.1 ± 1.0 | 4.1 ± 0.9bc | 3.6 ± 1.0a | 3.7 ± 1.0a | 0.010 |
| 36 | Group Health Habits | 3.4 ± 0.8 | 3.2 ± 1.1 | 3.7 ± 1.1 | 3.5 ± 1.0 | 3.8 ± 0.9 | n.s. |
| 62 | Parents/Relatives’ Concern About the Environment | 2.5 ± 0.7 | 2.5 ± 0.9 | 2.9 ± 1.1bc | 2.0 ± 0.9a | 2.4 ± 1.1a | <0.001 |
| 92 | Social Expectation | 2.9 ± 0.8 | 2.8 ± 1.1 | 3.3 ± 1.1c | 3.1 ± 0.9 | 2.8 ± 0.9a | 0.032 |
| 93 | Social Inclusion | 3.1 ± 0.8 | 2.8 ± 1.1 | 3.3 ± 1.1 | 3.1 ± 1.0 | 3.5 ± 1.1 | n.s. |
| 99 | Support of Family/Peers/Partner | 3.7 ± 0.6 | 3.3 ± 0.9 | 4.2 ± 0.9 | 3.8 ± 0.9 | 4.0 ± 0.9 | n.s. |
| Cluster 6: Supportive Environment | |||||||
| 2 | Access to Personal/Family/Peer Transport | 3.2 ± 0.7 | 3.0 ± 0.9 | 3.3 ± 1.0 | 3.1 ± 1.1c | 3.5 ± 1.0b | 0.028 |
| 43 | Involvement in Organized Sport | 3.7 ± 0.8 | 3.7 ± 1.0 | 4.1 ± 0.9bc | 3.6 ± 1.0ac | 3.2 ± 1.2ab | <0.001 |
| 55 | Number of Household Cars/Car Ownership | 2.7 ± 0.8 | 2.6 ± 1.1 | 2.7 ± 0.9 | 2.9 ± 1.0 | 2.6 ± 1.0 | n.s. |
| 74 | Physician Advices | 3.4 ± 0.8 | 3.5 ± 1.3 | 2.6 ± 1.0bc | 3.3 ± 0.9ac | 4.1 ± 0.8ab | <0.001 |
| 75 | Private Environment (Home/Backyard Space) | 3.1 ± 0.9 | 2.9 ± 1.1 | 3.3 ± 1.1 | 3.0 ± 1.0c | 3.5 ± 1.1b | 0.023 |
| 101 | Time Spent Outdoor/Playing Spaces | 3.6 ± 0.8 | 3.7 ± 0.9 | 4.1 ± 0.9bc | 3.1 ± 1.1a | 3.2 ± 1.2a | <0.001 |
Means ± SD of Ratings (Likert scale: 1 = lowest value, 5 = highest value) and Differences (p < 0.05) between Population-Level Effect
a = differences (p < 0.05) with respect to the youth population
b = differences (p < 0.05) with respect to the adult population
c = differences (p < 0.05) with respect to the older adult population
n.s. = not significant
Structuring (sorting and rating)
The recruitment resulted in seventy-nine experts willing to participate in the concept mapping exercise (response rate to invitation was 21 %). While participants affiliated with academic or research institutions (n = 64) declared expertise in Life Sciences (78 %; e.g., biology, biochemistry, biotechnology, biomechanics, clinical sciences, developmental and ageing sciences, ergonomics, epidemiology, physiology, medicine, nutrition, neurosciences, public health and health promotion, movement and sport sciences), Social Sciences and Humanities (20 %; e.g., anthropology, behavioural sciences, economics and finance, environmental science, history, law, philosophy, psychology, pedagogy, political science, and sociology), and Physical Sciences and Engineering (2 %; e.g., statistics), those affiliated with European organizations relevant to PA promotion (n = 15) declared expertise in Life Sciences (47 %; e.g., movement and sport sciences) and Social Sciences and Humanities (53 %; e.g., economics and finance, law, management, political science, and sociology). The majority of participants (90 %) was from the European Member States (Austria, Belgium, Croatia, Denmark, Finland, Germany, Hungary, Ireland, Italy, Latvia, Poland, Portugal, Slovenia, Spain, Sweden, and United Kingdom), whereas the others (10 %) came from Kosovo, Norway, Russia, Switzerland, and Turkey. Thus, the sample was considered representative of a Pan-European expertise in PA research and promotion.
Respondents were informed about the aim of the investigation and the procedures to access an online analysis platform (i.e., Ariadne; http://www.minds21.biz/). A three-week timeframe was given to complete the clustering and rating of factors. The factors were entered into a project-specific Ariadne software [54], which has been used previously to develop theoretical public health frameworks in Europe [20, 29, 35, 40]. The instructions stated that each factor had to be assigned to one group only, with a maximum number of ten groups permitted. Participants were also required to rate the 106 factors on a Likert-type scale from 1 (lowest value) to 5 (highest value). Ratings were required for factor modifiability across the life course and for the expected population-level effect for youth, adults, and older adults, respectively.
Analysis and interpretation
The concept mapping software (Ariadne) uses a combination of statistical techniques. First, it computes a binary symmetric similarity matrix per respondent. Second, it provides an aggregated (group) matrix by counting the individual matrices, with high values indicating that many of the participants put the named factors together in a group which implies a conceptual similarity between statements. This aggregated similarity matrix is then used as the input for a (non-metric) principal component analysis (PCA), a technique for translating the distances between statements into coordinates in a multidimensional space. A stepwise analysis from the lowest number (e.g. 2) to the highest number (e.g. 18) of clustering of factors and the graphic representation of their origin are provided. In general, the spatial distribution of the clusters on the map (e.g., eastern, western, northern, and southern parts) mirrors different themes [54].
After the collection of the data from the experts, during a second workshop the DEDIPAC-KH research team analysed the findings to facilitate an agreement for a cohesive EU-PAD framework. A stepwise analysis was performed to provide a configuration of the least number of clusters that possessed reasonable and agreed theoretical distinctions. Through further discussion, members of the DEDIPAC-KH research team determined the labels that would best represent the content of the final configuration of clusters based on their included factors. A consensus on face validity was reached. A priority for research score was estimated for each factor by weighting its grading scores of modifiability (50 %) and the sum of population-level effects (50 %). Priority between clusters was established based on the mean values of their weighted grading. Finally, the proposed EU-PAD framework was submitted online to the participating European experts requesting a final consensus regarding the labelling of the clusters and how the included factors represent research priorities within each cluster. An analysis of variance was performed to test differences (p < 0.05) in the level of impact of the 106 factors in the youth, adult, and older adult populations. When significant differences emerged, Bonferroni post-hoc comparisons were used.
According to the literature [21, 33, 37, 39, 55, 56] and to enhance the exploitation of findings for decision making directing future strategic plans, the mean ratings of the modifiability (x-axis) and population-level effect (y-axis) for the youth, adult, and older adult populations were used to plot the position of each factor relative to all other factors. The resulting scatterplots identified four quadrants (e.g., I, II, III, and IV) of “Go-Zones”, reporting factors deemed relevant for their population-level effect but considered to have a low modifiability (Quadrant I), factors that have been attributed low ratings for both modifiability and population-level effect (Quadrant II), factors deemed relevant for their modifiability but considered to have a low population-level effect (Quadrant III), and factors deemed to be most modifiable and having the highest population-level effect (Quadrant IV), respectively. In particular, the Quadrant IV identifıed the factors experts rated as highly important for increasing PA behaviours for each age group.
Results
Clustering and ratings of factors
The preliminary analysis of the concept mapping generated two main areas (Fig. 1), the first comprising 42 % of all factors mainly related to the individual (e.g., ‘Person’), the second comprising 58 % of all factors mainly related to socio-cultural-organizational factors (‘Society). Then, the area ‘Person’ generated two clusters, which were labelled based on the analysis of the included factors as Cluster 1 ‘Intra-Personal Context and Wellbeing’ (i.e., encompassing everything related to the individuals including, but not limited, to their health and wellbeing), and Cluster 2 ‘Family and Social Economic Status’ (i.e., referring to the family environment and social status of the individuals). The area ‘Society’ generated four clusters, which were labelled based on the analysis of the included factors as Cluster 3 ‘Policy and Provision’ (i.e., incorporating political aspects that influence the civic life of individuals/groups at local, national, and international levels); Cluster 4 ‘Cultural Context and Media’ (i.e., referring to the cultural and social environment that individuals/groups live in and interact with); Cluster 5 ‘Social Support and Modelling’ (i.e., incorporating factors related to the habits of family/groups that influence the individual); and Cluster 6 ‘Supportive Environment’ (i.e., referring to the factors that influence the engagement in active lifestyles). Final consensus agreement for the cluster labels obtained through an online survey to all participants ranged from 92.7 % (e.g., ‘Family and Social Economic Status’) to 100.0 % (e.g., ‘Social Support and Modelling’).
Fig. 1.

Six-cluster map within the two main areas ‘Person’ and ‘’Society’. Legend; Straight lines represent the origin of the clusters from the 3, 4, and 5 cluster arrangements. In particular, the area ‘Person’ originated two clusters (e.g., ‘Intra-Personal Context and Wellbeing’ and ‘Family and Socio-Economic Status’), whilst the area ‘Society’ originated the cluster ‘Policy and Provision’ and a second cluster that, in turn, originated the clusters ‘Cultural Context and Media’, ‘Supportive Environment’, and ‘Social Support and Modelling’
Table 2 presents the 106 factors organized by cluster, including statistics for ratings of priority for research, modifiability, and population-level effects. The number of factors in each cluster ranged from six in the ‘Supportive Environment’ and ‘Social Support and Modelling’ clusters to 38 in the ‘Policy and Provision’ cluster. For the population-level effect age-related differences (p < 0.05) emerged for sixty-seven factors. Post-hoc analysis identified 12 factors that varied across all age groups (e.g., ‘Fear of Injuries/Falling’, ‘Health Status’, ‘Level of Autonomy/Time Management’, ‘Perceived Stress/Life Stressors’, ‘Sub-Pathology/Pathology/Injuries/Pain/Rehabilitation’, and ‘Time Availability’ in the ‘Intra-Personal Context and Wellbeing’ cluster; ‘School/Office Hours’ in the ‘Policy and Provision’ cluster; ‘Cyber Space’, ‘Internet Availability’, and ‘Social Media’ in the ‘Cultural Context and Media’ cluster; ‘Involvement in Organized Sport’ and ‘Physician Advices’ in the ‘Supportive Environment’ cluster). No factors in the other two clusters demonstrated a similar difference across stages of the life course (see Table 2). Post-hoc analysis did not confirm a significant difference only for the factor ‘Actual Body Mass Index’.
Go-zones
The relationships between modifiability and population-level effect for the youth, adult, and older adult populations are presented in Figs. 2, 3 and 4, respectively. Factors receiving high ratings for both modifiability and level effect are presented in Quadrant IV, in which 45 factors were noted for both the youth and older adult populations, and 47 factors for the adult population. Twenty-five of these factors were common between the three age populations (Table 3). The majority of these factors belonged to the ‘Intra-Personal Context and Wellbeing’ and the ‘Policy and Provision’ clusters, representing 52 and 20 % of the total, respectively. The rest belonged to the clusters ‘Social Support and Modelling’, ‘Cultural Context and Media’, ‘Supportive Environment’, and ‘Family and Social Economic Status’, representing 12, 8, 4 and 4 % of the total, respectively.
Fig. 2.
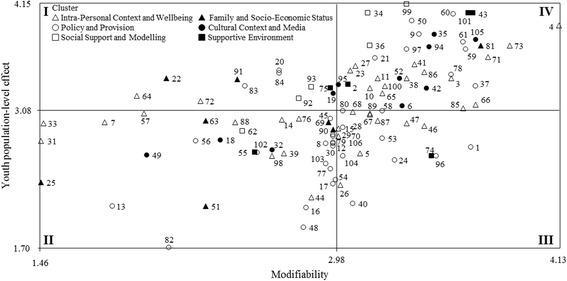
Go-Zone map of modifiability and population-level effect ratings for the youth population
Fig. 3.

Go-Zone map of modifiability and population-level effect ratings for the adult population
Fig. 4.
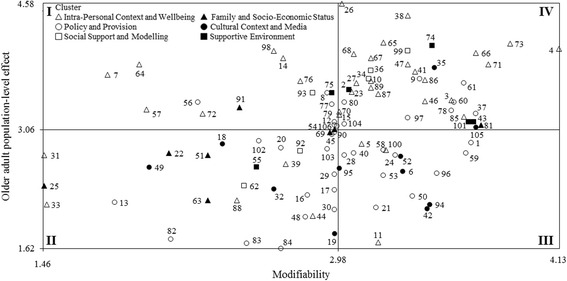
Go-Zone map of modifiability and population-level effect ratings for the older adult population
Table 3.
Factors by clusters included in the quadrant IV of Go-Zones (youth, adults, and older adults)
| Cluster | Factor Number and Statement |
|---|---|
| Intra-Personal Context and Wellbeing | 3 Actual Body Mass Index |
| 4 Actual PA Level | |
| 10 Beliefs/Values | |
| 23 Emotions | |
| 27 Feeling of Inadequacy (Too Clumsy/Too Old)/Teasing | |
| 38 Health Status | |
| 41 Intentions/Attitudes | |
| 65 Perceived Barriers | |
| 66 Perceived Benefits of PA | |
| 71 Personal Goals/Outcome Expectancies/Atchievement Orientation/Motivation | |
| 73 Physical fitness levels (Strength, Endurance, Coordination, Agility, Flexibility) | |
| 85 Self PA Monitoring | |
| 86 Self Perceptions (Awareness, Confidence, Efficacy, Body Image, PA Level) | |
| Family and Socio-Economic Status | 81 Rewards (Encouragement/Support) |
| Policy and Provision | 9 Availability/Access/Proximity of PA Organized Sport Facilities Tools |
| 37 Health Education | |
| 60 PA Programs in School/Office/Community | |
| 61 PA Programs/Plans | |
| 97 Sports Facilities | |
| Cultural Context and Media | 35 Group Activity (Outdoor/Indoor) |
| 105 Tv Exposure | |
| Social Support and Modelling | 34 Group (Family Peers Partner) PA Behaviours |
| 36 Group Health Habits | |
| 99 Support of Family/Peers/Partner | |
| Supportive Environment | 43 Involvement in Organized Sport |
In Quadrant IV, five factors were present only for the youth population (factors ‘Mandatory PA in Community/Schools’ and ‘PA and Sport Organizations Advocacy’ in cluster ‘Policy and Provision’, and factors’Advertisement’,’Cyber Space’, and ‘Internet Availability’ in cluster ‘Cultural Context and Media’) and five factors only for the older adult population (factors ‘Conscious Control of Automated Body Movements’ and ‘Fear of Injuries/Falling’ in cluster Intra-Personal Context and Wellbeing’, and factors’Mobility Policy’, ‘Public Transport Policies’, and ‘Transport Policies’ in cluster ‘Policy and Provision’). Two factors were present only in the adult population (factor ‘Addictions (Smoking Gambling Drugs)’ in cluster ‘Intra-Personal Context and Wellbeing’, and factor ‘Financial Measures and Regulation for PA and Sport’ in cluster ‘Policy and Provision’). Five factors were shared only between the youth and adult populations (factors ‘Capability to Combine Sport and Education/Work Requirements (Dual Career)’ and ‘Time Availability’ in cluster ‘Intra-Personal Context and Wellbeing’, and factors’Media’,’Social Media’, and ‘Social Trends’ in ‘Cultural Context and Media’), whereas six factors were shared only between adult and older adult populations (factors’Level of Autonomy/Time Management’, ‘Life Satisfaction’, and ‘Perceived Stress/Life Stressors’ in cluster ‘Intra-Personal Context and Wellbeing’, factor ‘Social Competence/Role’ in cluster Family and Social Economic Status’, factor ‘City Planning’ in cluster Policy and Provision’, and factor ‘Physician Advices’ in cluster ‘Supportive Environment’).
Priority for research
Table 4 presents the top five factors based on mean rating for the priority for research for each cluster. The overall mean rating ranged from 3.4 ± 0.2 for the cluster ‘Supportive Environment’ to 2.7 ± 0.5 for the cluster ‘Family and Socio-Economic Status’. In particular, the most prioritised factors for research were ‘Actual PA Level’, ‘Physical Fitness Levels (Strength, Endurance, Coordination, Agility, Flexibility)’, and ‘Personal Goals/Outcome Expectancies/Achievement Orientation/Motivation’, all belonging to the cluster ‘Intra-Personal Context and Wellbeing’. Final consensus agreement for the priority of research of factors within each cluster obtained through an online survey to all participants ranged from 83 % (e.g., ‘Intra-Personal Context and Wellbeing’) to 98 % (e.g., ‘Social Support and Modelling’).
Table 4.
Highest-rated factors for priority for research in descending order for each cluster
| Factor # | Statement By Cluster | Priority for Research |
|---|---|---|
| Cluster 1: Intra-Personal Context and Wellbeing | 3.2 ± 0.5 | |
| 4a | Actual PA Level | 4.1 ± 0.6 |
| 73a | Physical Fitness Levels (Strength, Endurance, Coordination, Agility, Flexibility) | 3.9 ± 0.7 |
| 71a | Personal Goals/Outcome Expectancies/Achievement Orientation/Motivation | 3.8 ± 0.7 |
| 66a | Perceived Benefits of PA | 3.7 ± 0.7 |
| 38a | Health Status | 3.7 ± 0.7 |
| Cluster 2: Family and Socio-Economic Status | 2.7 ± 0.5 | |
| 81a | Rewards (Encouragement/Support) | 3.5 ± 0.8 |
| 69 | Perceived Social Role | 3.0 ± 0.8 |
| 90 | Social Competence/Role | 3.0 ± 0.8 |
| 91 | Social Economic Status/Personal Income (for Children: Parents’ Income)/Level of Education | 2.9 ± 0.8 |
| 22 | Educational Level (Parents/Relatives) | 2.6 ± 0.8 |
| Cluster 3: Policy and Provision | 3.0 ± 0.4 | |
| 61a | PA Programs/Plans | 3.6 ± 0.8 |
| 60a | PA Programs in School/Office/Community | 3.6 ± 0.8 |
| 9* | Availability/Access/Proximity of PA Organized Sport Facilities/Tools | 3.6 ± 0.7 |
| 37a | Health Education | 3.5 ± 0.7 |
| 59 | PA Education (at School/Work)/Knowledge of Effects of PA | 3.4 ± 0.9 |
| Cluster 4: Cultural Context and Media | 3.0 ± 0.4 | |
| 35a | Group Activities (Outdoor/Indoor) | 3.6 ± 0.7 |
| 105a | TV Exposure | 3.6 ± 1.0 |
| 94 | Social Media | 3.2 ± 0.9 |
| 52 | Media | 3.2 ± 0.8 |
| 42 | Internet Availability | 3.1 ± 0.9 |
| Cluster 5: Social Support and Modelling | 3.3 ± 0.3 | |
| 99a | Support of Family/Peers/Partner | 3.7 ± 0.6 |
| 34a | Group (Family/Peers/Partner) PA Behaviours | 3.5 ± 0.6 |
| 36a | Group Health Habits | 3.4 ± 0.8 |
| 93 | Social Inclusion | 3.1 ± 0.8 |
| 92 | Social Expectations | 2.9 ± 0.8 |
| Cluster 6: Supportive Environment | 3.4 ± 0.2 | |
| 43a | Involvement in Organized Sport | 3.7 ± 0.8 |
| 101 | Time Spent Outdoor/Playing Spaces | 3.6 ± 0.8 |
| 74 | Physical Advices | 3.4 ± 0.8 |
| 2 | Access to Personal/Family/Peer Transport | 3.2 ± 0.7 |
| 75 | Private Environment (Home/Backyard Space) | 3.1 ± 0.9 |
aIndicates inclusion also in the Quadrant IV of the youth, adult, and older adult populations
Discussion
The current DEDIPAC-KH initiative aimed to develop the EU-PAD framework to provide a Pan-European and life course view of key factors of PA behaviours, and a proposal of how these factors may group into clusters. The combined experience of European scholars and policy makers was capitalized to identify potential factors of PA behaviours and to rate these factors in terms of their importance (level of effect) to the three populations of concern (e.g., youth, adults, and older adults), their modifiability and their priority for research. Not only is the response to these three questions indicative of our current understanding of the determinants of PA behaviours, it could also provide significant guidance to the future research agenda within Europe and a structure to increase collaboration and harmonisation of research methodologies. In fact, the identification of the six clusters fits well into the theoretical perspective of research utilization, which is considered as an important condition for implementing research findings and subsequent translation into policies [20].
The EU-PAD framework presents a conceptual map to generate recommendations but not conclusions and the findings are relevant to all who have contributed [22]. The uniqueness of the present study lies in the effort in synergising a range of knowledge, capacities, activities, and actions of multiple European experts in an attempt to uncover the multi-level relationships between PA factors applicable to individuals and to society. As expected, experts in the European Research Area of Physical Sciences and Engineering resulted underrepresented compared to those with an expertise in Life Sciences and Social Sciences and Humanities who are more likely to be involved in PA research and European PA organizations. Considering the broad and pervasive nature of PA, the European research agenda should foster research for the promotion of PA also in the disciplines that are typically less associated with PA. The practical relevance of the EU-PAD framework subsumes the resulting theoretical evidence as a sound basis for practical decision-making [20], and urges policy makers and scholars from different disciplines to coordinate their efforts in bridging existing gaps between sciences, practices, and policies in the HEPA area [57]. Thus, the results of this initiative could potentially contribute to the development of a strategic plan for both research and policies at a Pan-European level, and ultimately to more effective European policies and actions in promoting positive PA behaviours [19].
To yield the optimal practical outcomes either at the society level or at the person level, it is critical to consider the importance (level of effect) of each factor to the three populations of interest (i.e., youth, adults, and older adults) and the level of modifiability across the life course. Of the 25 factors identified to be the most modifiable and influential across the life course, 16 of them were rated to be amongst the top 5 of research priority list in each cluster (see Table 4). In all, research focus on these 16 factors might result in a more targeted and fruitful approach for promoting positive PA behaviours across the life course. Despite the high consensus for the priority of research of factors within each cluster (83–98 %), this prioritisation of discrete factors could be less valuable than the identification of discrete or group of factors for specific life stages or contexts [41]. Furthermore, emphasis should be placed on transdisciplinary investigations and interventions, in line with the aim of the European Joint Programming Initiative A Healthy Diet for a Healthy Life to foster a common research agenda for the enhancement of active lifestyles of European citizens [18]. In fact, researchers or policy makers ought not lose sight of the other PA factors because all operate within their respective clusters and interactions between them are complex and ultimately, a holistic view to interpreting the clusters in the framework is needed. Moreover, particular attention should be given to relatively modifiable factors that are unique to a specific age group (e.g., for youth: ‘Cyber Space’; for adults: ‘Financial and Regulation for PA and Sport’; and for older adults: ‘Mobility Policy’) as they might influence PA behaviours for each population in a distinctive way [7, 58, 59].
In extending the examination of the factors in distinct clusters, the analysis noted two core themes from the six clusters within the framework: 1) the ‘Person’ (referring to the proximal relationships between individuals such as family, social relationships, and socioeconomic status), and 2) the ‘Society’ (encompassing environmental, historical, political, social, economic, scientific, cultural, and organization factors), each comprising a cluster with around 35 % of all the factors (e.g., ‘Intra-Personal Context and Wellbeing’ and ‘Policy and Provision’, respectively). Resonating previous research and systematic literature reviews on the determinants of PA, the ‘Person’ theme infers that the individual is central in the adoption of an active lifestyle, including, but not limited to, individual responsibility, personal committment and lifestyle choices for PA behaviours [13, 16, 17, 60–65], whilst the ‘Society’ theme echoes researchers’ plead for attention to the role of policy and the environment in promoting PA in European citizens [13, 16, 17, 66]. Interestingly, out of all the clusters, ‘Supportive Environment’ was considered to be the highest priority for research. This might suggest, and call for, a shift in focus from individual responsibility, personal commitment, and lifestyle choices to influences of supportive environments for overcoming barriers to PA for different age groups at both research and policy levels. Furthermore, the highest ranked factor in this cluster, ‘Involvement in Organized Sports’, is closely related to those positioned at the highest level in clusters within the ‘Person’ theme (e.g., ‘Actual PA Level’,’Rewards (Encouragement/Support)’, and ‘Support of Family/Peers/Partner’). This finding substantiates the complexity and interrelatedness of all the factors in this EU-PAD framework and the personal and social relevance of organized sports for sustainable collaboration programmes to increase active lifestyles. This finding is in line with the recommendations of the European Expert Group on HEPA, which urge Governments to facilitate population level behavioural change by creating supporting and enabling environments for an active lifestyle [4].
According to Trochim and colleagues [34], concept mapping has been considered a cost-effective and successful way of identifying factors determining PA behaviours, despite this inherent value it must be accepted that the process involves very demanding and time-intensive activities, such as brainstorming, the management of a large amount of information, the complex scenery of interrelated ideas to be systematised, and the recruitment of European experts from a diversity of disciplines for reaching a consensus. Some limitations to the present study have been noted. First and foremost, the selection bias of the diverse group of stakeholders engaged in this study cannot be ruled out. Secondly, despite the initial intent to provide a more exhaustive picture of potential factors influencing PA behaviours, experts’ prior knowledge in the field of PA research would almost inevitably influence the list of factors to be included in the current study. When repeating the concept mapping exercise again, it could be advisable to engage additional experts from fields of research that are distinct from the current focus (e.g., urban planning disciplines), to operationalize and measure factors separately within specific areas of competence, and to combine them through a collective effort of inter- and trans-disciplinary expertise to enrich our understanding of PA determinants and their interactions (such as the mediating, moderating and causal role of each determinant to PA behaviours). It is unknown what influence the inclusion of experts from more diverse fields, albeit PA-related, may have on the outcome of the concept mapping exercise.
Conclusions
In conclusion, the cumulated experience and perception of European scholars from different scientific areas and policy makers in the field of sport and HEPA were integrated into a framework of factor clusters which both illuminates and confirms the complexity of PA behaviours phenomenon. In fact, the EU-PAD framework identifies the importance of addressing multiple factors within and between clusters. The factors and clusters present some similarities with respect to those described by previous ecological models for understanding determinants of PA behaviours [13, 16, 17]. Distinctly, by using a concept mapping approach the EU-PAD framework has provided additional and new insights regarding a European and life course view of key factors, additional definition regarding the specific nature of the factors and how these factors group into clusters. In practice, the EU-PAD framework can be used to (i) guide the development of a strategic plan for novel and multi-disciplinary research at Pan-European level addressing the complexity of determinants of PA behaviours across the life course (e.g., evidence production); (ii) identify key aspects for potential strategies to implement multi-sectoral European policies in HEPA (e.g., agenda setting and advocacy); and (iii) develop intervention programmes for individual behavioural change and interventions for impinging on the social and physical (natural and built) environment to improve the involvement of European citizens in healthy active lifestyles (e.g., HEPA guidelines adoption, implementation and delivery). To fully exploit effective actions to increase PA levels, the well-established European platforms (e.g., the Regional Office for Europe of the World Health Organization, the European Sport Forums, the meetings of sports Directors, sport and education Ministers, and Expert Groups, the conferences of the Council Presidency, and of the Enlarged Partial Agreement on Sport of the Council of Europe) provide a valuable infrastructure to enhance communication and cooperation between relevant stakeholders at national and European levels for the development and implementation of an integrated approach to healthy active lifestyle interventions. In fact, future European research and intervention plans are still needed to verify specific mechanisms through which particular influences may interact and implement active lifestyle behaviours of European citizens.
Acknowledgements
Group author members: Lien N, Lakerveld J, Mazzocchi M, O’Gorman D, Monsivais P, Nicolaou M, Renner B, Volkert D.
The authors thank Abelkains I, Al Shayji I, Arrogi A, Bellardini H, Borgogni A, Bosnar K, Bykhovskaya I, Collins C, Dall P, Demirhan G, Dóczi T, Dolan P, Dontje M, Edelson Lisa, Farkas J, Fodor A, Foerster J, Harvey J, Haut JH, Hayes C, Hinze T, Jekauc D, Jurak G, Keldorf O, Klostermann C, Kobel S, Leask C, Määttä S, Mair J, Mattli R, Mellis M, Tanner M, Mussino A, Nunes R, O’Dolan C, Olander E, Ommundsen Y, Perenyi S, Pfister GU, Pisl A, Pohlmann A, Pulsford R, Rama L, Robnik P, Rodriguez AM, Routen A, Samija K, Sherar L, Sjøgaard G, Teixeira A, Tsvhan H, Turner G, Varess R, Zinzen E, and Zysko J for their purposeful contribution in the online concept mapping process, which made possible to finalise this work.
Funding
This project was supported by a grant from:
1 Ministero dell’Istruzione, Università e Ricerca (MIUR), Italy: DEDIPAC F.S. 02.15.02 COD. B84G14000040008.
1, 4, 8, 9, 18 Ministero dell’Istruzione, Università e Ricerca (MIUR), Italy: CDR2.PRIN 2010/11 COD. 2010KL2Y73.
2 Health Research Board, Ireland.
5, 11 The Medical Research Council (MRC), United Kingdom.
7 Italian Ministry of Agricultural, Food, and Forestry Policies, Italy: DEDIPAC-IRILD, D.M. 14474/7303/13.
10 Federal Ministry of Education and Research, Germany 01EA1374.
13 Federal Ministry of Education and Research, Germany 01EA1372E.
16 Institut National de la Recherche Agronomique (INRA), Institut National de Prevention et d’Education pour la Sante (INPES).
17 ZonMw, The Netherlands Organisation for Health Research and Development project, The Netherlands 50-52300-98-003.
19 Federal Ministry of Education and Research, Germany 01EA1372C.
Availability of data and materials
For the present study, we used already existing tests and software for data extraction and analysis which are described in the Methods section with citation of the corresponding sources. Raw data cannot be rendered freely available to other scientists to preserve participants’ anonymity, as required by law in the country where the study has been conducted.
Authors’ contributions
CG, CL, MDC, and LF shared equal responsibilities to led the development of the framework and organised the consensus meeting, analysed results and wrote the manuscript. CS, CL, MDC, and CaG developed the protocol. CG, LF, BA, CS, CaG, CD, CoD, CC, DCM, DBA, GM, HS, IL, IP, JL, LL, ML, MC, MS, PC, PeC, PT, PA, PuA, SA, SW, SH, SC, StA, MDC, and CL developed the focus prompts and the generation of factors and participated in the consensus events. All the co-authors were involved in the review of this manuscript. The responsibility for the content of this manuscript lies with the authors. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Consent for publication was obtained from all participants and informed consent was assumed with subjects’ participation upon provided information regarding the study goals, conditions, and the use of their data in aggregated form for scientific publication, in conformity with national laws, which guarantee that no individual details would be published.
Ethics approval and consent to participate
The present work involved experts in virtue of their training or expertise. In fact, experts have information and knowledge in a substantive area beyond that of the average person and who regularly share this information and knowledge through consultation, teaching or public speaking, or publications and written reports. For the Committee of the Protection of Human Subject (CPHS) purposes, experts are not human subjects when asked to provide opinions within their areas of expertise and do not require CPHS approval. Furthermore in the present work, the experts’ opinion were not about the interviewee themselves, but rather about the external topic (e.g., factors deemed relevant for physical activity behaviours), not including demographic queries about age, education, income or other personal information. Finally, the research group simply reported the facts as related by the content experts. In the quest to ensure better knowledge on determinats of physical activity behaviours of youth, adults and older adults, the rights and welfare of research participants have been protected at all times. Participation was voluntary and free of coercion, persuasion, manipulation, deception, undue influence or inducement, and threat or intimidation. The information has been obtained in a private setting (e.g., personal url to access the website) and confidentiality has been ensured and maintained throughout the research. For the above reasons, IRB review was not required.
Participation in the task was voluntary and informed consent was assumed with subjects’ reply that they were willing to participate. Participating experts were free of opting out at any time (i.e., not completing the clustering and rating of factors) without providing any reason and incomplete opinions were not considered.
Abbreviations
- DEDIPAC-KH
DEterminants of DIet and Physical ACtivity Knowledge Hub
- EU
European Union
- EU-PAD
EUropean-Physical Activity Determinants
- HEPA
Health-enhancing physical activity
- PA
Physical activity
- PCA
Principal component analysis
Contributor Information
Giancarlo Condello, Phone: +39 0636733255, Email: giancarlo.condello@gmail.com.
Fiona Chun Man Ling, Email: Fiona.Ling@ul.ie.
Antonino Bianco, Email: antoninobianco@unipa.it.
Sebastien Chastin, Email: Sebastien.Chastin@gcu.ac.uk.
Greet Cardon, Email: greet.cardon@ugent.be.
Donatella Ciarapica, Email: donatella.ciarapica@crea.gov.it.
Daniele Conte, Email: danieleconte25@gmail.com.
Cristina Cortis, Email: c.cortis@unicas.it.
Marieke De Craemer, Email: Marieke.DeCraemer@UGent.be.
Andrea Di Blasio, Email: andiblasio@gmail.com.
Masar Gjaka, Email: masar.gjaka@uni-pr.edu.
Sylvia Hansen, Email: dedipac_ustutt@inspo.uni-stuttgart.de.
Michelle Holdsworth, Email: michelle.holdsworth@sheffield.ac.uk.
Licia Iacoviello, Email: licia.iacoviello@moli-sani.org.
Pascal Izzicupo, Email: pascalizzicupo@gmail.com.
Lina Jaeschke, Email: Lina.Jaeschke@mdc-berlin.de.
Liliana Leone, Email: leone@cevas.it.
Livia Manoni, Email: livia.manoni@romascuola.net.
Cristina Menescardi, Email: ca.menescardi@ucv.es.
Silvia Migliaccio, Email: silvia.migliaccio@uniroma4.it.
Julie-Anne Nazare, Email: julie-anne.nazare@cens-nutrition.com.
Camille Perchoux, Email: camille.perchoux@gmail.com.
Caterina Pesce, Email: caterina.pesce@uniroma4.it.
Frank Pierik, Email: frank.pierik@tno.nl.
Tobias Pischon, Email: tobias.pischon@mdc-berlin.de.
Angela Polito, Email: angela.polito@crea.gov.it.
Anna Puggina, Email: annapuggina@gmail.com.
Alessandra Sannella, Email: alessandra.sannella@unicas.it.
Wolfgang Schlicht, Email: wolfgang.schlicht@sport.uni-stuttgart.de.
Holger Schulz, Email: schulz@helmholtz-muenchen.de.
Chantal Simon, Email: chantal.simon@univ-lyon1.fr.
Astrid Steinbrecher, Email: Astrid.Steinbrecher@mdc-berlin.de.
Ciaran MacDonncha, Email: Ciaran.MacDonncha@ul.ie.
Laura Capranica, Email: laura.capranica@uniroma4.it.
References
- 1.World Health Organization. Global status report on Noncommunicable diseases. http://apps.who.int/iris/bitstream/10665/44579/1/9789240686458_eng.pdf (2010). Accessed 16 Jan 2016.
- 2.Council of the European Union. Council Recommendation of 26 November 2013 on promoting health-enhancing physical activity across sectors. Official Journal of the European Union. 2013/C 354/01.http://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=OJ:C:2013:354:FULL&from=EN (2013). Accessed 18 Jan 2016.
- 3.European Commission. EU Physical Activity Guidelines Recommended Policy Actions in Support of Health-Enhancing Physical Activity. http://ec.europa.eu/sport/library/policy_documents/eu-physical-activity-guidelines-2008_en.pdf (2008). Accessed 16 Jan 2016.
- 4.European Commission. Expert Group on Health-enhancing physical activity: Recommendations to encourage physical education in schools, including motor skills in early childhood, and to create valuable interactions with the sport sector, local authorities and the private sector. http://ec.europa.eu/transparency/regexpert/index.cfm?do=groupDetail.groupDetailDoc&id=19860&no=1 (2015). Accessed 18 Jan 2016.
- 5.European Commission. EU platform on Diet, Physical Activity and Health. http://ec.europa.eu/health/archive/ph_determinants/life_style/nutrition/platform/docs/platform_charter.pdf (2005). Accessed 16 Jan 2016.
- 6.Halleux V. EU sport policy: An overview. Members’ Research Service Directorate-General for Parliamentary Research Services, European Parliament Publ. http://www.europarl.europa.eu/RegData/etudes/IDAN/2015/565908/EPRS_IDA(2015)565908_EN.pdf (2015). Accessed 16 Jan 2016.
- 7.Kokko S, Oja P, Foster C, Koski P, Laalo-Häikiö E, Savola J. Sports Club for Health: Guidelines for health-oriented sports activities in a club setting. 2011. http://kunto-fi-bin.directo.fi/@Bin/3ac08bfa56792096efa51f91ede4fb2d/1456243252/application/pdf/463608/SCforH_Guidelines.pdf. Accessed 16 Jan 2016.
- 8.World Health Organization. Promoting Sport and Enhancing Health in European Union Countries: A Policy Content Analysis to Support Action. http://www.euro.who.int/__data/assets/pdf_file/0006/147237/e95168.pdf (2011). Accessed 18 Jan 2016.
- 9.European Commission. Special Eurobarometer 412 Sport and Physical Activity Report. http://ec.europa.eu/health/nutrition_physical_activity/docs/ebs_412_en.pdf (2014). Accessed 16 Jan 2016.
- 10.European Commission and World Health Organization Europe. Fact sheets on health-enhancing physical activity in the 28 European Union Member States of the WHO European region. http://ec.europa.eu/sport/library/factsheets/eu-wide-overview-methods.pdf (2015). Accessed 18 Jan 2016.
- 11.Hämäläinen RM, Aro AR, van de Goor I, Lau CJ, Jakobsen MW, Chereches RM, Syed AM, REPOPA Consortium Exploring the use of research evidence in health-enhancing physical activity policies. Health Res Policy Syst. 2015;13:43. doi: 10.1186/s12961-015-0047-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Buchan DS, Ollis S, Thomas NE, Baker JS. Physical activity behaviour: an overview of current and emergent theoretical practices. J Obes. 2012;2012:546459. doi: 10.1155/2012/546459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet Physical Activity Series Working Group. Lancet. 2012;380(9838):258–271. doi: 10.1016/S0140-6736(12)60735-1. [DOI] [PubMed] [Google Scholar]
- 14.Glass TA, McAtee MJ. Behavioral science at the crossroads in public health: extending horizons, envisioning the future. Social Sci Med. 2006;62(7):1650–1671. doi: 10.1016/j.socscimed.2005.08.044. [DOI] [PubMed] [Google Scholar]
- 15.Ooms L, Veenhof C, Schipper-Van Veldhoven N, De Bakker DH. Sporting programs for inactive population groups: factors influencing implementation in the organized sports setting. BMC Sports Sci Med Rehabil. 2015;7:12. doi: 10.1186/s13102-015-0007-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sallis JF, Cervero RB, Ascher W, Henderson KA, Kraft MK, Kerr J. An ecological approach to creating more physically active communities. Annu Rev Public Health. 2006;27:297–322. doi: 10.1146/annurev.publhealth.27.021405.102100. [DOI] [PubMed] [Google Scholar]
- 17.Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health behavior and health education: theory, research, and practice. 4. San Francisco: Jossey-Bass; 2008. pp. 465–486. [Google Scholar]
- 18.European Commission. EU Joint Programming Initiative A Healthy Diet for a Healthy Life. http://www.healthydietforhealthylife.eu (2013). Accessed 16 Jan 2016.
- 19.Lakerveld J, van der Ploeg HP, Kroeze W, Ahrens W, Allais O, Andersen LF, et al. DEDIPAC consortium. Towards the integration and development of a cross-European research network and infrastructure: the DEterminants of DIet and Physical ACtivity (DEDIPAC) Knowledge Hub. Int J Behav Nutr Phys Act. 2014;11:143. doi: 10.1186/s12966-014-0143-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.van Bon-Martens MJ, van de Goor LA, Holsappel JC, Kuunders TJ, Jacobs-van der Bruggen MA, te Brake JH, van Oers JA. Concept mapping as a promising method to bring practice into science. Public Health. 2014;128(6):504–514. doi: 10.1016/j.puhe.2014.04.002. [DOI] [PubMed] [Google Scholar]
- 21.Anderson LA, Day KL, Vandenberg AE. Using a concept map as a tool for strategic planning: The Healthy Brain Initiative. Prev Chronic Dis. 2011;8(5):A117. [PMC free article] [PubMed] [Google Scholar]
- 22.Trochim WMK. An introduction to concept-mapping for planning and evaluation. Evaluation and Program Planning. 1989;12(1):1–16. doi: 10.1016/0149-7189(89)90016-5. [DOI] [Google Scholar]
- 23.Trochim, WMK. The reliability of concept-mapping. Annual Conference of the American Evaluation Association; Dallas, TX. 1993.
- 24.Trochim W, Kane M. Concept-mapping: an introduction to structured conceptualization in health care. Int J Qual Health Care. 2005;17(3):187–191. doi: 10.1093/intqhc/mzi038. [DOI] [PubMed] [Google Scholar]
- 25.Trochim W, Cabrera DA, Milstein B, Gallagher RS, Leischow SJ. Practical challenges of systems thinking and modeling in public health. Am J Public Health. 2006;96(3):538–546. doi: 10.2105/AJPH.2005.066001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Trochim WM, Marcus SE, Masse LC, Moser RP, Weld PC. The evaluation of large research initiatives: a participatory integrative mixed-methods approach. Am J Eval. 2008;29(1):8–28. doi: 10.1177/1098214007309280. [DOI] [Google Scholar]
- 27.Schiller C, Winters M, Hanson HM, Ashe MC. A framework for stakeholder identification in concept mapping and health research: a novel process and its application to older adult mobility and the built environment. BMC Public Health. 2013;13:428. doi: 10.1186/1471-2458-13-428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kane M, Trochim WM. Concept mapping for planning and evaluation. Thousand Oaks: Sage Publications; 2007. [Google Scholar]
- 29.Minjman M, Ahaus K, Fabbricotti I, Nabitz U, Huijsman R. A quality management model for integrated care: results of a Delphi and Concept Mapping study. Int J Qual Health Care. 2009;21(1):66–75. doi: 10.1093/intqhc/mzn048. [DOI] [PubMed] [Google Scholar]
- 30.Jackson KM, Trochim WM. Concept mapping as an alternative approach for the analysis of open-ended survey responses. Organ Res Methods. 2002;5(4):307–336. doi: 10.1177/109442802237114. [DOI] [Google Scholar]
- 31.Anderson LA, Gwaltney MK, Sundra DL, Brownson RC, Kane M, Cross AW, Mack R, Jr, Schwartz R, Sims T, Carol WR. Using concept mapping to develop a logic model for the Prevention Research Centers Program. Prev Chronic Dis. 2006;3(1):A06. [PMC free article] [PubMed] [Google Scholar]
- 32.Ewan LA, Mclinden D, Biro F, Dejonckheere M, Vaughn LM. Mapping the views of adolescent health stakeholders. J Adolesc Health. 2016;58(1):24–32. doi: 10.1016/j.jadohealth.2015.09.020. [DOI] [PubMed] [Google Scholar]
- 33.Lebel A, Cantinotti M, Pampalon R, Thériault M, Smith LA, Hamelin AM. Concept mapping of diet and physical activity: uncovering local stakeholders perception in the Quebec City region. Soc Sci Med. 2011;72(3):439–445. doi: 10.1016/j.socscimed.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 34.Trochim W, Milstein B, Wood BJ, Jackson S, Pressler V. Setting objectives for community and systems change: an application of concept mapping for planning a state wide health improvement initiative. Health Promot Pract. 2004;5(1):8–19. doi: 10.1177/1524839903258020. [DOI] [PubMed] [Google Scholar]
- 35.van Bon-Martens MJ, Achterberg PW, van de Goor IA, van Oers HA. Towards quality criteria for regional public health reporting: concept mapping with Dutch experts. Eur J Public Health. 2012;22(3):337–342. doi: 10.1093/eurpub/ckr016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wheeler FC, Anderson LA, Boddie-Willis C, Price PH, Kane M. The role of state public health agencies in addressing less prevalent chronic conditions. Prev Chronic Dis. 2005;2(3):A12. [PMC free article] [PubMed] [Google Scholar]
- 37.Brennan LK, Brownson RC, Kelly C, Ivey MK, Leviton LC. Concept mapping: priority community strategies to create changes to support active living. Am J Prev Med. 2012;435(Suppl 4):S337–S350. doi: 10.1016/j.amepre.2012.07.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Dulin-Keita A, Clay O, Whittaker S, Hannon L, Adams IK, Rogers M, Gans K. The influence of HOPE VI neighborhood revitalization on neighborhood-based physical activity: A mixed-methods approach. Soc Sci Med. 2015;139:90–99. doi: 10.1016/j.socscimed.2015.06.002. [DOI] [PubMed] [Google Scholar]
- 39.Hanson HM, Schiller C, Winters M, Sims-Gould J, Clarke P, Curran E, Donaldson MG, Pitman B, Scott V, McKay HA, Ashe MC. Concept mapping applied to the intersection between older adults’ outdoor walking and the built and social environments. Prev Med. 2013;57(6):785–791. doi: 10.1016/j.ypmed.2013.08.023. [DOI] [PubMed] [Google Scholar]
- 40.Rosenkötter N, Achterberg PW, van Bon-Martens MJ, Michelsen K, van Oers HA, Brand H. Key features of an EU health information system: a concept mapping study. Eur J Public Health. 2016;26(1):65–70. doi: 10.1093/eurpub/ckv075. [DOI] [PubMed] [Google Scholar]
- 41.Chastin SF, De Craemer M, Lien N, Bernaards C, Buck C, Oppert JM, Nazare JA, Lakerveld J, O’Donoghue G, Holdsworth M, Owen N, Brug J, Cardon G, DEDIPAC consortium, expert working group and consensus panel The SOS-framework (Systems of Sedentary behaviours): an international transdisciplinary consensus framework for the study of determinants, research priorities and policy on sedentary behaviour across the life course: a DEDIPAC-study. Int J Behav Nutr Phys Act. 2016;13:83. doi: 10.1186/s12966-016-0409-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Howley ET. Type of activity: resistance, aerobic and leisure versus occupational physical activity. Med Sci Sports Exerc. 2001;33 Suppl 6:S364-9. doi: 10.1097/00005768-200106001-00005. [DOI] [PubMed] [Google Scholar]
- 43.Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U, Lancet Physical Activity Series Working Group Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. 2012;380(9838):247–257. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- 44.Caspersen CJ, Powell KE, Christenson G. Physical activity, exercise and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100(2):126–131. [PMC free article] [PubMed] [Google Scholar]
- 45.Koeneman MA, Verheijden MW, Chinapaw MJ, Hopman-Rock M. Determinants of physical activity and exercise in healthy older adults: a systematic review. Int J Behav Nutr Phys Act. 2011;8:142. doi: 10.1186/1479-5868-8-142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.McNaughton SA, Crawford D, Ball K, Salmon J. Understanding determinants of nutrition, physical activity and quality of life among older adults: the Wellbeing, Eating and Exercise for a Long Life (WELL) study. Health Qual Life Outcomes. 2012;10:109. doi: 10.1186/1477-7525-10-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Van Cauwenberg J, Van Holle V, De Bourdeaudhuij I, Van Dyck D, Deforche B. Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity. Health Place. 2016;37:16–25. doi: 10.1016/j.healthplace.2015.11.003. [DOI] [PubMed] [Google Scholar]
- 48.Deutskens E, De Ruyter K, Wetzels M, Oosterveld P. Response rate and response quality of internet-based surveys: An experimental study. Mark Lett. 2004;15(1):21–36. doi: 10.1023/B:MARK.0000021968.86465.00. [DOI] [Google Scholar]
- 49.Hooley T, Marriott J, Wellens J. What is online research?: Using the internet for social science research. London: Bloomsbury Academic; 2012. [Google Scholar]
- 50.Cook C, Heath F, Thompson RL. A. Meta-Analysis of response rates in web- or internet-based surveys. Educ Psychol Meas. 2000;60:821–836. doi: 10.1177/00131640021970934. [DOI] [Google Scholar]
- 51.Barush Y. Response rate in academic studies: a comparative analysis. Hum Relat. 1999;52(4):421–438. [Google Scholar]
- 52.Denison DR, Mishra AK. Toward a theory of organizational culture and effectiveness. Organ Sci. 1993;6(2):204–223. doi: 10.1287/orsc.6.2.204. [DOI] [Google Scholar]
- 53.O’Donoghue P. Statistics for sport and exercise studies: An introduction. Abingdon: Routledge; 2012. [Google Scholar]
- 54.Severens, P. Handbook for Ariadne Concept Mapping. www.minds21.org (2012). Accessed 16 Jan 2015.
- 55.Iris M, DeBacker NA, Benner R, Hammerman J, Ridings J. Creating a quality of life assessment measure for residents in long term care. J Am Med Dir Assoc. 2012;13(5):438–447. doi: 10.1016/j.jamda.2011.08.011. [DOI] [PubMed] [Google Scholar]
- 56.Waltz TJ, Powell BJ, Matthieu MM, Damschroder LJ, Chinman MJ, Smith JL, Proctor EK, Kirchner JE. Use of concept mapping to characterize relationships among implementation strategies and assess their feasibility and importance: results from the Expert Recommendations for Implementing Change (ERIC) study. Implement Sci. 2015;10:109. doi: 10.1186/s13012-015-0295-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Tubbing L, Harting J, Stronks K. Unravelling the concept of integrated public health policy: Concept mapping with Dutch experts from science, policy, and practice. Health Policy. 2015;119:749–759. doi: 10.1016/j.healthpol.2014.12.020. [DOI] [PubMed] [Google Scholar]
- 58.Livingstone S, d’Haenens L, Hasenbrink U. Childhood in Europe: Context for comparison. In: Livingstone S, Bovill S, editors. Children and their Changing Media Environment: A European Comparative Study. New York: Routledge; 2001. pp. 3–30. [Google Scholar]
- 59.Spirduso WW, Francis KL, MacRae PG. Health-related quality of life. In: Spirduso WW, Francis KL, MacRae PG, editors. Physical Dimensions of Aging. 2. Champaign: Human Kinetics; 2005. pp. 233–257. [Google Scholar]
- 60.Bui L, Mullan B, McCaffery K. Protection motivation theory and physical activity in the general Population: a systematic literature review. Psychol Health Med. 2013;18(5):522–542. doi: 10.1080/13548506.2012.749354. [DOI] [PubMed] [Google Scholar]
- 61.LeBlanc AG, Berry T, Deshpande S, Duggan M, Faulkner G, Latimer-Cheung AE, O’Reilly N, Rhodes RE, Spence JC, Tremblay MS. Knowledge and awareness of Canadian Physical Activity and Sedentary Behaviour Guidelines: a synthesis of existing evidence. Appl Physiol Nutr Metab. 2015;40(7):716–724. doi: 10.1139/apnm-2014-0464. [DOI] [PubMed] [Google Scholar]
- 62.Lipnowski S, Leblanc CM, Canadian Paediatric Society, Healthy Active Living and Sports Medicine Committee Healthy active living: Physical activity guidelines for children and adolescents. Paediatr Child Health. 2012;17(4):209–212. doi: 10.1093/pch/17.4.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Nasuti G, Rhodes RE. Affective judgment and physical activity in youth: review and meta-analyses. Ann Behav Med. 2013;45(3):357–376. doi: 10.1007/s12160-012-9462-6. [DOI] [PubMed] [Google Scholar]
- 64.Rhodes RE, Smith NEI. Personality correlates of physical activity: a review and meta-analysis. Br J Sports Med. 2006;40(12):958–965. doi: 10.1136/bjsm.2006.028860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. 2012;9:78. doi: 10.1186/1479-5868-9-78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Sygit-Kowalkowska E. The health behaviour of people in late adulthood -sociodemographic correlations and differences between social environments. Ann Acad Med Stetin. 2013;59(1):103–113. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
For the present study, we used already existing tests and software for data extraction and analysis which are described in the Methods section with citation of the corresponding sources. Raw data cannot be rendered freely available to other scientists to preserve participants’ anonymity, as required by law in the country where the study has been conducted.