

Abstract
Health literacy is the capacity to understand basic health information and make appropriate health decisions. Tens of millions of Americans have limited health literacy—a fact that poses major challenges for the delivery of high-quality care. Despite its importance, health literacy has until recently been relegated to the sidelines of health care improvement efforts aimed at increasing access, improving quality, and better managing costs. Recent federal policy initiatives, including the Affordable Care Act of 2010, the Department of Health and Human Services’ National Action Plan to Improve Health Literacy, and the Plain Writing Act of 2010, have brought health literacy to a tipping point—that is, poised to make the transition from the margins to the mainstream. If public and private organizations make it a priority to become health literate, the nation’s health literacy can be advanced to the point at which it will play a major role in improving health care and health for all Americans.
According to the Affordable Care Act of 2010, health literacy is the capacity to obtain, communicate, process, and understand basic health information and services to make appropriate health decisions. An increasing body of research links health literacy with health outcomes. In particular, limited health literacy leads to a cascade of suboptimal outcomes, including reduced ability to interpret labels and health messages, limited ability to take medications appropriately, lower likelihood of receiving preventive care, more hospitalizations, greater use of emergency care, and—among elderly people—worse overall health status and higher mortality rates.1
In years past, clinicians and researchers alike largely viewed these issues and outcomes in terms of individual patient deficits—that is, a patient’s lack of knowledge and skills regarding health issues. We now recognize that health literacy is a dynamic systems issue,2 reflecting the complexity of both the health information being presented and the health care system being navigated.3 As summarized by the Institute of Medicine, addressing the challenge of health literacy requires system-level changes for both health professionals and organizations.4
In this article we review the new opportunities that recent landmark federal policies have created to improve health literacy. Several major health policy developments at the federal level have brought health literacy to a possible tipping point that could move health literacy from the margins to the mainstream of health care practice. Improved health literacy has the potential to help address issues of health care access, quality, and cost.
In particular, three major initiatives in 2010 collectively catalyzed attention to the consequences of, and remedies for, limited health literacy. These are the Affordable Care Act (the health care reform law of 2010); the National Action Plan to Improve Health Literacy (hereafter the Action Plan) of the Department of Health and Human Services (HHS); and the Plain Writing Act of 2010, which requires all new publications, forms, and publicly distributed documents from the federal government to be written in a “clear, concise, well-organized” manner.
In this article we focus on the efforts of HHS, while recognizing the critical contributions of many private-sector and nonprofit organizations and individuals.5–7 All of these entities are stakeholders in making health literacy a vital part of the health care transformation process that will help promote better health and health care for the nation.
Limited Health Literacy And The Cycle Of ‘Crisis Care’
Health systems often function as if all patients have health literacy skills and can be vigilant advocates for themselves.8 In reality, however, a wide chasm often separates what providers intend to convey in written and oral communication and what patients understand.9–11
Moreover, as our population grows more diverse with respect to age, culture, and language, that chasm threatens to widen and exacerbate health disparities.12 The current design of health care systems requires patients to possess and demonstrate multiple skills, including understanding and giving consent, interacting with health professionals, and applying health information to different situations in a variety of life events. For every task, patients must employ the major components of health literacy: print literacy (writing and reading), oral literacy (listening and speaking), and numeracy (using and understanding numbers, such as medication doses).
Unfortunately, many people find these tasks challenging.13 In the only population-level study of health literacy skills conducted to date, the Department of Education’s National Assessment of Adult Literacy documented that only 12 percent of US adults are proficient enough in health literacy to understand and use health information effectively (Exhibit 1).14 Moreover, more than a third of adults are in the “basic” or “below basic” health literacy groups, which means they may fail to understand critically important warnings on the label of an over-the-counter medicine. Adults with “intermediate” health literacy skills find it difficult to define a medical term from a complex document about an unfamiliar topic. Adding to these challenges, twenty-four million Americans (8.7 percent) are not proficient in English.15
EXHIBIT 1. US Adults’ Health Literacy Levels, 2003.
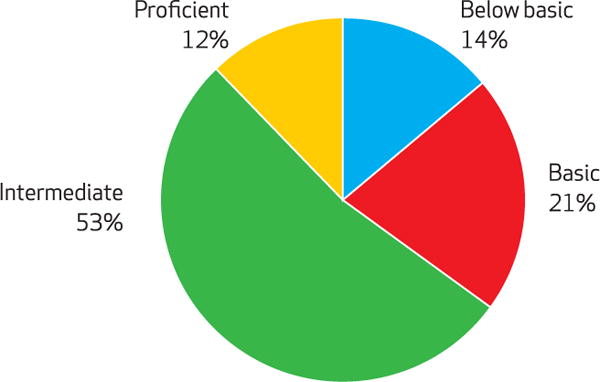
SOURCE Department of Health and Human Services (Note 14 in text).
Navigating the health care system is not just a challenge for those who have limited health literacy. Patients are regularly confronted with complicated, confusing forms and instructions. As a result, too many people are hospitalized after being given ambiguous instructions about medications or failing to recognize the symptoms of a worsening condition. Effective practices have yet to be developed to assess whether patients properly use medications, complete tests, or receive referrals. Using a clinic or hospital setting as an example, Exhibit 2 illustrates how limited health literacy contributes to this cycle of “crisis care.”
EXHIBIT 2. The Cycle Of Crisis Care: A Patient’s Experience.
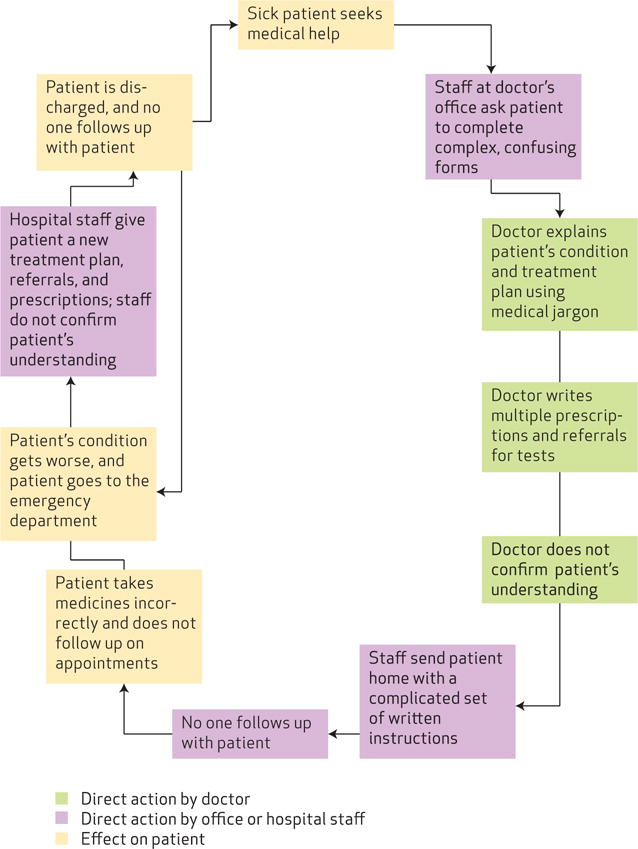
SOURCE Authors’ analysis.
Fortunately, recent research indicates that providers and organizations can adapt their procedures in ways that can make a difference. The following examples of effective actions from randomized trials demonstrate that system changes focused on health literacy issues can support preventive and patient-centered care, thus reducing the length and severity of episodes of crisis care.
SIMPLIFYING AND MAKING WRITTEN MATERIALS EASIER TO UNDERSTAND
Medication counseling using a plain language, pictogram-based intervention resulted in fewer medication-dosage errors (5.4 percent versus 47.8 percent) and greater adherence, compared to standard medication counseling (38 percent versus 9.3 percent).16
IMPROVING PROVIDERS’ COMMUNICATION SKILLS
A study of rates of participation in colon cancer screening compared two groups of providers. One group received feedback on their patients’ health literacy status and underwent subsequent training in communicating with patients who had limited literacy skills; the second group did not. The patients of the first group of providers had higher colon cancer screening rates than the patients of the second group of providers (41.3 percent versus 32.4 percent). Among patients with limited literacy, screening rates for patients of providers in the first group were almost twice as high as those for patients of providers in the second group (55.7 percent versus 30 percent).17
IMPROVING PATIENTS’ SELF-MANAGEMENT SKILLS
A congestive heart failure self-management program—featuring education on self-care, picture-based educational materials, and scheduled telephone follow-up to reinforce adherence to necessary medication regimens and daily weight measurement—reduced hospitalization rates and mortality by 35 percent, compared with patients in the control group.18 Similarly, patients with limited literacy who received a diabetes self-management program that used health literacy strategies were more likely to achieve program goals than people with diabetes who received usual care (42 percent versus 15 percent).19
An Opening For Health Literacy
In 2010 three major federal policy initiatives created an opening to move beyond the cycle of crisis care. The Affordable Care Act directly and indirectly addressed health literacy by incorporating health literacy into professional training (section 5301); and streamlining procedures for enrollment into Medicaid, the Children’s Health Insurance Program, and the state-based insurance exchanges (section 1413).20
One of the efforts to improve health literacy in the Affordable Care Act is the law’s requirement that health plans and insurers provide consumers with clear, consistent, and comparable health information in a standardized summary of benefits and coverage template (section 2715) (see the online Appendix for details).21 In a recent public poll, this new patient-oriented summary was found to be the most popular provision of the act.22 Clear information about benefits will be vital for the estimated thirty-two million Americans, many with limited health literacy skills,14 who are projected to receive coverage through the state-based exchanges and Medicaid expansion in 2014 and beyond.
The Affordable Care Act’s emphasis on patient-centeredness is also a key part of the 2011 National Strategy for Quality Improvement in Health Care23 and the 2011 National Prevention and Health Promotion Strategy.24 Patient-centered care incorporates many health literacy approaches in that it incorporates effective communication techniques, engages the patient and family, and is coordinated. Patient-centeredness is also a key element of the HHS Partnership for Patients, which promotes patient safety in hospitals, as well as new demonstration projects to promote patient-centered medical homes. HHS recently launched its Pioneer Accountable Care Organizations, which emphasize quality and patient satisfaction as outcomes.
The provisions of the Affordable Care Act also align with the National Action Plan to Improve Health Literacy—which, for the first time, presents unified health literacy goals and strategies for the country.25 Developed after considerable public and professional input, the Action Plan is based on the following two principles: that all people have the right to health information that helps them make informed decisions; and that health services should be delivered in ways that are understandable and lead to health, longevity, and good quality of life.
The plan’s seven goals are as follows: Develop and disseminate health and safety information that is accurate, accessible, and actionable; promote changes in the health care system that improve health information, communication, informed decision making, and access to health services; incorporate accurate, standards-based, and developmentally appropriate health and science information and curricula in child care and education through the university level; support and expand local efforts to provide adult education, English language instruction, and culturally and linguistically appropriate health information services in the community; build partnerships, develop guidance, and change policies; increase basic research and the development, implementation, and evaluation of practices and interventions to improve health literacy; and increase the dissemination and use of evidence-based health literacy practices and interventions.
The Plain Writing Act of 2010 aligns with the first goal of the Action Plan: to require federal agencies to write documents clearly so that the public can understand and use them. Plain language helps people better understand and apply for benefits and services for which they are eligible, including health insurance, disability support, and nutrition support.26 The act is not limited to the health sector; it applies to any document that provides information about federal benefits or services, or how to comply with federal requirements. Federal agencies will issue their first reports on the implementation of plain language in spring 2012, thereby providing a view of plain language use across the federal government and a baseline to use in measuring future progress.
In addition to these three major 2010 federal policy initiatives, other notable national developments address health information technology, health disparities and equity, and national health goals that connect health literacy to mainstream policy concerns (see the online Appendix for details).21
For example, the Health Information Technology for Economic and Clinical Health (HITECH) provisions of the American Recovery and Reinvestment Act of 200927 promote the adoption of electronic health records to provide health information that is meaningful and useful to consumers, including after-visit summaries, discharge instructions, patient reminders, and patient-specific education. The 2011 National Stakeholder Strategy for Achieving Health Equity,28 which accompanied the 2011 HHS Strategic Action Plan to Reduce Racial and Ethnic Health Disparities, includes a broad array of actions, such as updating the 2000 National Standards on Culturally and Linguistically Appropriate Services.
Healthy People 202029 includes objectives related to health literacy. Measures of desired system-level changes in these areas include health care providers’ use of what is known as the teach-back method, in which health care providers ask patients to repeat their understanding of directions; the level of shared decision making between patients and providers; and populationwide access to personalized e-health tools.
When fully implemented, the Affordable Care Act, the Action Plan, the Plain Writing Act, and other health improvement initiatives will not only help shift crisis care to patient-centered, prevention-focused care. They have the potential to help improve health care access, quality, and cost management (see Appendix 2).21
Implications Of Improving Access, Quality, And Cost
The cycle of crisis care reflects a cascade of problems in health care access, quality, and cost (Exhibit 2). Health reform and other initiatives described in this article each contribute to breaking this cycle. Incorporating health literacy strategies into health care improvement efforts will help the nation reach the broad goals of the Affordable Care Act and other health care policies. The following are some examples of HHS efforts to bring health literacy into the heart of these efforts.
ACCESS
For consumers and patients, access to clear and actionable health information is integral to being able to obtain health services. Many consumers struggle to understand key health plan concepts, options for health coverage, and specific terms such as cost sharing and managed care.30–33 Also, newly insured individuals, especially those with below basic and basic health literacy skills, need clear, actionable information in order to select and enroll in health plans.34 They also need assistance in completing forms, finding providers after enrolling in an insurance plan, and receiving covered services.
HHS has employed health literacy research and usability principles to meet the health care information needs of the public through two web-based initiatives. Called for by the Affordable Care Act, HealthCare.gov, launched in July 2010, is the first website to provide consumers with both public and private health coverage option tailored specifically to their needs in a single, easy-to-use tool. The site has received more than ten million visits since its inception. A cornerstone of the site is the HealthCare.gov Plan Finder, an interactive feature that enables consumers to compare health insurance options.
A second site, healthfinder.gov, helps the public find reliable and current prevention guidelines and wellness information. This site receives more than 800,000 visits a month. Its interactive consumer tool myhealthfinder provides personalized, prevention-decision support for all clinical preventive services. Under the Affordable Care Act, many insurers are required to cover certain preventive services at no additional cost. In this regard, healthfinder.gov assists Americans in better understanding which preventive services are appropriate, based on personal profile, medical history, and preferences. A number of other guides and tools are also available (see the online Appendix for details).21
QUALITY
Patients with limited health literacy report having lower-quality communication with health professionals. They express confusion regarding medical terminology and say that they have insufficient time to express concerns and fail to receive clear explanations.35–38 Patients with limited health literacy are also less likely than others to use preventive services.39 Furthermore, the Joint Commission finds that “the safety of patients cannot be assured without mitigating the negative effects of low health literacy and ineffective communications on patient care.”40 Although using techniques to address patients’ limited health literacy can improve the quality of health care and health outcomes, clinicians employ them infrequently.41,42
To assist providers, HHS offers an array of free online resources. These include the Health Literacy Universal Precautions Toolkit,43 with tips to encourage patients to bring all their medicines to an office visit, review their use of the medicines, and clarify instructions; a continuing education module, Health Literacy Training for Public Health Professionals;44 and the Unified Health Communications course,45 which addresses health literacy, cultural competence, and limited English proficiency.
These tools are directly relevant to several patient-centered quality themes on the national agenda. First, addressing issues of cultural competence and health literacy can contribute to reducing racial and ethnic health disparities in both the clinical and community setting. Second, adopting strategies to improve health literacy directly contributes to a provider’s becoming a patient-centered medical home that “actively supports patients in learning to manage and organize their own care at the level the patient chooses.”46
The Joint Commission, the National Committee for Quality Assurance, and URAC (formerly the Utilization Review Accreditation Commission, a nonprofit leader in health care quality) have recognized the central role that health literacy plays in their accreditation standards for patient-centered medical homes. An example is the following standard: “The primary care clinician and the interdisciplinary team incorporate the patient’s health literacy needs into the patient’s education.”47
Quality improvement efforts apply not only to health care delivery systems, but also to the broader public health community. Public health quality is defined as “the degree to which policies, programs, services, and research for the population increase desired health outcomes and conditions in which the population can be healthy.”48 Limited health literacy represents a barrier to public health’s quality aims, particularly to successfully promoting health and creating equity among users of public health services.
One example of a public health approach to advancing quality by improving health literacy can be found in the Healthy People 2020 Health Communication and Health Information Technology objectives. Specifically, objective HC/HIT-8.2 focuses on increasing the proportion of high-quality health-related websites. HHS has begun efforts to establish standards, based on heath literacy and usability principles, for what constitutes high-quality health-related websites. Once developed, these standards can be used to survey health websites nationwide and highlight best practices.
COST
Patients’ seeking emergency care and needing repeated inpatient hospitalization, as noted in Exhibit 2, drive up health care costs.49,50 A randomized controlled trial of the “reengineered” discharge, which improves the education patients receive in the hospital and facilitates the transition from hospital to home, reduced rehospitalizations by 30 percent.51 Although the reengineered discharge is in the early stages of replication, it holds promise for meeting the HHS Partnership for Patients’ goal of lowering rehospitalizations, as well as the goal of lower related costs for conditions such as congestive heart failure (associated with rehospitalization costs of more than $10,000 per person with congestive heart failure).52–54
The recent launch of Pioneer Accountable Care Organizations promotes goals of shared savings in Medicare-related expenses by giving providers incentives to work together and meet critical goals in patient satisfaction and quality. Using measures of patients’ experience of care, such as the Consumer Assessment of Healthcare Providers and Services surveys—specifically, the supplemental questions on health literacy, cultural competence, and health information technology—can facilitate the process of accountability for such organizations.
Moving Beyond The Cycle Of Crisis Care
The successful implementation of the types of health literacy system adaptations noted in this article can help break the cycle of crisis care and move health literacy from the margins to the mainstream of health care practices. No longer a cycle of crisis care, the health-literate care scenario features clear communication, simplified forms, offers of assistance, confirmation of understanding through teach-back and other methods, and commitment to patient followup, which has the potential to improve health outcomes (Exhibit 3).
EXHIBIT 3. Health-Literate Care: A Patient’s Experience.
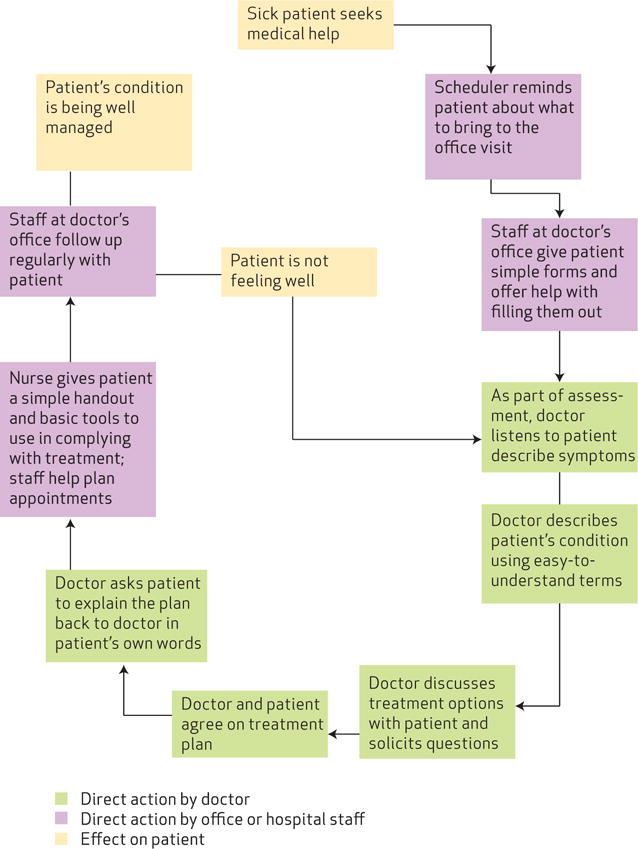
SOURCE Authors’ analysis.
This article has focused on the numerous federal policy advances related to health literacy. However, moving past the tipping point to bring health literacy strategies into routine health care processes will require even further commitments in policy and practice in the public and private sectors. To this end, the Institute of Medicine Roundtable on Health Literacy has started to identify the attributes of a health-literate organization.
According to a commissioned paper by the roundtable’s members,55 health-literate organizations make promoting health literacy an organizational responsibility and prepare their employees to meet it. To become health literate, organizations can begin by conducting organizational self-assessments to identify health literacy–based barriers, training staff in clear communication techniques, securing language assistance for speakers of languages other than English, and providing needed assistance to consumers while being careful not to stigmatize them.
Fortunately, many organizations have already responded to the call to make health literacy a key element of health care improvement. As an example, professional associations such as the American Medical Association, the American Dental Association, the American College of Physicians, and the American Academy of Pediatrics; health plans, including many members of America’s Health Insurance Plans; and some pharmaceutical manufacturers have all undertaken explicit health literacy initiatives. We hope that many more will answer the call.
The time is right to accelerate our national commitment to providing the American people with clear, understandable, and actionable science-based health information. The promises of medical research, health information technology, and advances in health care coverage and delivery can be realized only if our nation addresses the challenge of limited health literacy. The federal initiatives of the past few years, combined with a growing commitment to encouraging health-literate organizations and system change, can help the nation tackle health literacy and ultimately help us all lead longer, healthier lives.
Supplementary Material
Acknowledgments
The authors acknowledge the following colleagues for their contributions to this effort: Carter Blakey, Frank Funderburk, Peggy Honoré, Silje Lier, and Jessica Rowden.
Biographies

Howard K. Koh is assistant secretary for health at the Department of Health and Human Services (HHS).
In this month’s Health Affairs, Howard Koh, assistant secretary for health at the Department of Health and Human Services (HHS), and coauthors take up the topic of health literacy—the “capacity to obtain, communicate, process, and understand basic health information and services to make appropriate health decisions.” They describe how the Affordable Care Act of 2010, the HHS National Action Plan to Improve Health Literacy, and the Plain Writing Act of 2010 afford a central role to advancing health literacy in improving the health and health care of all Americans.
At HHS, Koh oversees fourteen public health offices, including the Office of the Surgeon General and the Public Health Service Commissioned Corps; ten regional health offices across the country; and ten presidential and secretarial advisory committees. He manages numerous interdisciplinary programs dedicated to disease prevention, health promotion, reduction of health disparities, women’s and minority health, adolescent health, HIV/AIDS, vaccines, physical fitness and sports, bioethics, population affairs, blood supply, research integrity, and human research protections.
Previously, Koh was professor and associate dean for public health practice and director of the Division of Public Health Practice at the Harvard School of Public Health. From 1997 to 2003 he was commissioner of public health in Massachusetts. Koh received his medical degree from the Yale School of Medicine, and he earned a master of public health degree from Boston University.
Donald M. Berwick is the former administrator of the Centers for Medicare and Medicaid Services.
Donald Berwick is the former administrator of the Centers for Medicare and Medicaid Services (CMS). Previously, he was president and chief executive officer of the Institute for Healthcare Improvement.
Berwick served as chair of the National Advisory Council of the Agency for Healthcare Research and Quality, and he is an elected member of the Institute of Medicine. He was clinical professor of pediatrics and health care policy at Harvard Medical School, professor of health policy and management at Harvard School of Public Health, consultant in pediatrics at Massachusetts General Hospital, and adjunct staff in the Department of Medicine at Children’s Hospital Boston.
Berwick is a pediatrician, and he received his medical degree from Harvard Medical School. He holds a master’s degree in public policy from Harvard’s John F. Kennedy School of Government.

Carolyn M. Clancy is director of the Agency for Healthcare Research and Quality.
Carolyn Clancy is director of the Agency for Healthcare Research and Quality (AHRQ). Previously, she was director of AHRQ’s Center for Outcomes and Effectiveness Research. Her major research interests include improving health care quality and patient safety and reducing disparities in care. As director of AHRQ, she launched the first annual report to Congress on health care disparities and health care quality.
Clancy is a clinical associate professor in the Department of Medicine at the George Washington University School of Medicine and Health Sciences, and she is a member of the Institute of Medicine. In 2009 she was awarded the William B. Graham Prize for Health Services Research. She is a general internist and a graduate of the University of Massachusetts Medical School.

Cynthia Baur is senior adviser for Health Literacy in the CDC Office of the Associate Director for Communication.
Cynthia Baur is senior adviser for health literacy, Office of the Associate Director for Communication, Centers for Disease Control and Prevention (CDC). She is cochair of the Healthy People 2020 Health Communication and Health Information Technology Workgroup and cochair of the HHS Health Literacy Workgroup. Baur holds a doctorate in communication from the University of California, San Diego.

Cindy Brach is a senior health policy researcher at AHRQ.
Cindy Brach is a senior health policy researcher at AHRQ, where she leads health literacy and cultural competence activities, including the development of the Health Literacy Universal Precautions Toolkit and the Consumer Assessment of Healthcare Providers and Systems health literacy measures. Brach received her master’s degree in public policy from the University of California, Berkeley, where she was advanced to candidacy for a doctorate degree.

Linda M. Harris is senior health communication and e-health adviser to the deputy assistant secretary for health, disease prevention, and health promotion at HHS.
Linda Harris is senior health communication and e-health adviser to the deputy assistant secretary for health, disease prevention, and health promotion and the lead of the Health Communication and e-Health Team in the Office of Disease Prevention and Health Promotion at HHS.
Harris oversees the National Health Information Center and manages healthfinder.gov, HealthyPeople.gov, and health.gov. She has a doctorate in communication from the University of Massachusetts. She also undertook postdoctoral work in sociology at the University of New Hampshire and completed a Service Fellowship in the US Public Health Service.

Eileen G. Zerhusen is a health insurance specialist at CMS.
Eileen Zerhusen is a health insurance specialist in the Office of Communications at CMS, where her work includes developing the strategy for implementing the Plain Writing Act of 2010 and writing print and online content for consumers. She is a registered nurse, who specialized in cardiology nursing and patient education before joining CMS. Zerhusen has a bachelor’s degree in nursing from Gwynedd Mercy College.
Contributor Information
Howard K. Koh, Email: Howard.Koh@HHS.gov, Assistant secretary for health at the Department of Health and Human Services (HHS), in Washington, D.C.
Donald M. Berwick, Former administrator of the Centers for Medicare and Medicaid Services (CMS), in Washington, D.C
Carolyn M. Clancy, Director of the Agency for Healthcare Research and Quality (AHRQ), in Rockville, Maryland
Cynthia Baur, Senior adviser for health literacy, Office of the Associate Director for Communication, Centers for Disease Control and Prevention, in Atlanta, Georgia.
Cindy Brach, Senior health policy researcher at AHRQ.
Linda M. Harris, Senior health communication and e-health adviser to the deputy assistant secretary for health, disease prevention, and health promotion at HHS, in Rockville, Maryland
Eileen G. Zerhusen, Health insurance specialist in the Office of Communications at CMS, in Baltimore, Maryland
NOTES
- 1.Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97–107. doi: 10.7326/0003-4819-155-2-201107190-00005. [DOI] [PubMed] [Google Scholar]
- 2.Rudd R. Improving Americans’ health literacy. N Engl J Med. 2010;363(24):2283–5. doi: 10.1056/NEJMp1008755. [DOI] [PubMed] [Google Scholar]
- 3.Parker R, Ratzan SC. Health literacy: a second decade of distinction for Americans. J Health Commun. 2010;15(Suppl 2):20–33. doi: 10.1080/10810730.2010.501094. [DOI] [PubMed] [Google Scholar]
- 4.Institute of Medicine. Health literacy implications for health care reform: a workshop summary. Washington (DC): National Academies Press; 2011. [Google Scholar]
- 5.Townzen D (Walmart; Bentonville, AR) Attributes of a health literate healthcare organization [Internet]. Presentation to: Institute of Medicine Roundtable on Health Literacy Attributes of a Health Literate Organization Workshop; 2011 Nov 16; Washington, DC. Washington, (DC): IOM; [cited 2012 Jan 10]. Available from: http://www.iom.edu/~/media/Files/Activity%20Files/PublicHealth/HealthLiteracy/2011-NOV-16/Townzen_The%20Other%20Side%20of%20the%20Coin%20%20IOM.pdf. [Google Scholar]
- 6.Johnston L (New York City Health and Hospitals Corporation; New York, NY) Response from a large public hospital system [Internet]. Presentation to: Institute of Medicine Roundtable on Health Literacy Attributes of a Health Literate Organization Workshop; 2011 Nov 16; Washington, DC. Washington, (DC): IOM; [cited 2012 Jan 10]. Available from: http://www.iom.edu/~/media/Files/Activity%20Files/PublicHealth/HealthLiteracy/2011-NOV-16/Johnston_Health%20literacy%20in%20the%20public%20sector%20FINAL.pdf. [Google Scholar]
- 7.America’s Health Insurance Plans. Health literacy and America’s Health Insurance Plans: laying the foundation and beyond [Internet] Washington, (DC): AHIP; 2011. [cited 2012 Jan 10]. Available from: http://www.ahip.org/Issues/Documents/2011/Health-Literacy-and-America%E2%80%99s-Health-Insurance-Plans–Laying-the-Foundation-and-Beyond.aspx. [Google Scholar]
- 8.Paasche-Orlow M, Schillinger D, Greene SM, Wagner EH. How health care systems can begin to address the challenge of limited literacy. J Gen Intern Med. 2006;21(8):884–7. doi: 10.1111/j.1525-1497.2006.00544.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Helitzer D, Hollis C, Cotner J, Oestreicher N. Health literacy demands of written health information materials: an assessment of cervical cancer prevention materials. Cancer Control. 2009;16(1):70–8. doi: 10.1177/107327480901600111. [DOI] [PubMed] [Google Scholar]
- 10.Badarudeen S, Sabharwal S. Readability of patient education materials from the American Academy of Orthopaedic Surgeons and Pediatric Orthopaedic Society of North America web sites. J Bone Joint Surg Am. 2008;90(1):199–204. doi: 10.2106/JBJS.G.00347. [DOI] [PubMed] [Google Scholar]
- 11.Hill-Briggs F, Smith AS. Evaluation of diabetes and cardiovascular disease print patient education materials for use with low-health literate populations. Diabetes Care. 2008;31(4):667–71. doi: 10.2337/dc07-1365. [DOI] [PubMed] [Google Scholar]
- 12.Chao S, Anderson K, Hernandez L. Toward health equity and patient-centeredness: integrating health literacy, disparities reduction, and quality improvement: a workshop summary. Washington (DC): National Academies Press; 2009. [PubMed] [Google Scholar]
- 13.Nielsen-Bohlman L, Panzer AM, Kindig DA. Health literacy: a prescription to end confusion. Washington (DC): National Academies Press; 2004. [PubMed] [Google Scholar]
- 14.Department of Health and Human Services. America’s health literacy: why we need accessible health information [Internet] Washington (DC): HHS; 2008. [cited 2012 Jan 10]. (Issue Brief). Available from: http://www.health.gov/communication/literacy/issuebrief/ [Google Scholar]
- 15.Shin HB, Kominski RA. Language use in the United States: 2007 [Internet] Washington (DC): Census Bureau; 2010. Apr, [cited 2012 Jan 10]. (American Community Survey Reports, Pub. No. ACS-12). Available from: http://www.census.gov/prod/2010pubs/acs-12.pdf. [Google Scholar]
- 16.Yin HS, Dreyer BP, van Schaick L, Foltin GL, Dinglas C, Mendelsohn AL. Randomized controlled trial of a pictogram-based intervention to reduce liquid medication dosing errors and improve adherence among caregivers of young children. Arch Pediatr Adolesc Med. 2008;162(9):814–22. doi: 10.1001/archpedi.162.9.814. [DOI] [PubMed] [Google Scholar]
- 17.Ferreira MR, Dolan NC, Fitzgibbon ML, Davis TC, Gorby N, Ladewski L, et al. Health care provider–directed intervention to increase colorectal cancer screening among veterans: results of a randomized controlled trial. J Clin Oncol. 2005;23(7):1548–54. doi: 10.1200/JCO.2005.07.049. [DOI] [PubMed] [Google Scholar]
- 18.DeWalt DA, Malone RM, Bryant ME, Kosnar MC, Corr KE, Rothman RL, et al. A heart failure self-management program for patients of all literacy levels: a randomized, controlled trial [ISRCTN11535170] BMC Health Serv Res. 2006;6:30. doi: 10.1186/1472-6963-6-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rothman RL, DeWalt DA, Malone R, Bryant B, Shintani A, Crigler B, et al. Influence of patient literacy on the effectiveness of a primary care–based diabetes disease management program. JAMA. 2004;292(14):1711–6. doi: 10.1001/jama.292.14.1711. [DOI] [PubMed] [Google Scholar]
- 20.Somers SA, Mahadevan R. Institute of Medicine Health literacy implications for health care reform: workshop summary. Washington (DC): National Academies Press; 2011. Health literacy implications of the Affordable Care Act; pp. 69–100. [Google Scholar]
- 21.To access the Appendix, click on the Appendix link in the box to the right of the article online.
- 22.Kaiser Family Foundation. Kaiser health tracking poll—November 2011 [Internet] Menlo Park (CA): KFF; 2011. Nov 30, [cited 2012 Jan 10]. Available from: http://www.kff.org/kaiserpolls/8259.cfm. [Google Scholar]
- 23.Department of Health and Human Services. Report to Congress: national strategy for quality improvement in health care. Washington (DC): HHS; 2011. Mar, [Google Scholar]
- 24.Office of the Surgeon General, National Prevention Council. National prevention strategy. Washington (DC): Department of Health and Human Services; 2011. [Google Scholar]
- 25.Department of Health and Human Services. National action plan to improve health literacy [Internet] Washington (DC): HHS; 2010. [cited 2012 Jan 10]. Available from: http://www.health.gov/communication/hlactionplan/pdf/Health_Literacy_Action_Plan.pdf. [Google Scholar]
- 26.Sunstein CR. Final guidance on implementing the Plain Writing Act of 2010. Washington (DC): Office of Management and Budget; 2011. [Google Scholar]
- 27.Office of the National Coordinator for Health Information Technology. Federal health information technology strategic plan 2011–2015. Washington (DC): Department of Health and Human Services; 2011. [Google Scholar]
- 28.Office of Minority Health, National Partnership for Action to End Health Disparities. National stakeholder strategy for achieving health equity. Washington (DC): Department of Health and Human Services; 2011. Apr, [Google Scholar]
- 29.Office of Disease Prevention and Health Promotion. Healthy people 2020. Washington (DC): Department of Health and Human Services; 2010. [Google Scholar]
- 30.Kleimann Communication Group Consumers Union. Early consumer testing of the coverage facts label: a new way of comparing health insurance. Washington (DC): Consumers Union; 2011. [Google Scholar]
- 31.Hibbard JH, Jewett JJ, Engelmann S, Tusler M. Can Medicare beneficiaries make informed choices? Health Aff (Millwood) 1998;17(6):181–93. doi: 10.1377/hlthaff.17.6.181. [DOI] [PubMed] [Google Scholar]
- 32.Harris-Kojetin LD, McCormack LA, Jael EF, Sangl JA, Garfinkel SA. Creating more effective health plan quality reports for consumers: lessons from a synthesis of qualitative testing. Health Serv Res. 2001;36(3):447–76. [PMC free article] [PubMed] [Google Scholar]
- 33.Uhrig JD, Harris-Kojetin L, Bann C, Kuo TM. Do content and format affect older consumers’ use of comparative information in a Medicare health plan choice? Results from a controlled experiment. Med Care Res Rev. 2006;63(6):701–18. doi: 10.1177/1077558706293636. [DOI] [PubMed] [Google Scholar]
- 34.Martin LT, Parker RM. Insurance expansion and health literacy. JAMA. 2011;306(8):874–5. doi: 10.1001/jama.2011.1212. [DOI] [PubMed] [Google Scholar]
- 35.Makaryus AN, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80(8):991–4. doi: 10.4065/80.8.991. [DOI] [PubMed] [Google Scholar]
- 36.Kripalani S, Jacobson TA, Mugalla IC, Cawthon CR, Niesner KJ, Vaccarino V. Health literacy and the quality of physician-patient communication during hospitalization. J Hosp Med. 2010;5(5):269–75. doi: 10.1002/jhm.667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Schillinger D, Bindman A, Wang F, Stewart A, Piette J. Functional health literacy and the quality of physician-patient communication among diabetes patients. Patient Educ Couns. 2004;52(3):315–23. doi: 10.1016/S0738-3991(03)00107-1. [DOI] [PubMed] [Google Scholar]
- 38.Kripalani S, Henderson LE, Jacobson TA, Vaccarino V. Medication use among inner-city patients after hospital discharge: patient-reported barriers and solutions. Mayo Clin Proc. 2008;83(5):529–35. doi: 10.4065/83.5.529. [DOI] [PubMed] [Google Scholar]
- 39.Scott TL, Gazmararian JA, Williams MV, Baker DW. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. 2002;40(5):395–404. doi: 10.1097/00005650-200205000-00005. [DOI] [PubMed] [Google Scholar]
- 40.Joint Commission. What did the doctor say? Improving health literacy to protect patient safety. Oakbrook Terrace (IL): Joint Commission; 2007. p. 5. [Google Scholar]
- 41.Schillinger D, Piette J, Grumbach K, Wang F, Wilson C, Daher C, et al. Closing the loop: physician communication with diabetic patients who have low health literacy. Arch Intern Med. 2003;163(1):83–90. doi: 10.1001/archinte.163.1.83. [DOI] [PubMed] [Google Scholar]
- 42.Schwartzberg JG, Cowett A, VanGeest J, Wolf MS. Communication techniques for patients with low health literacy: a survey of physicians, nurses, and pharmacists. Am J Health Behav. 2007;31(Suppl 1):S96–104. doi: 10.5555/ajhb.2007.31.supp.S96. [DOI] [PubMed] [Google Scholar]
- 43.DeWalt DA, Callahan LF, Hawk V, Broucksou KA, Hink A, Rudd R, et al. Health literacy universal precautions toolkit. Rockville (MD): Agency for Healthcare Research and Quality; 2010. [Google Scholar]
- 44.Centers for Disease Control and Prevention. Health literacy for public health professionals [Internet] Atlanta (GA): CDC; [cited 2012 Jan 10 Available from: http://www.cdc.gov/healthliteracy/GetTrainingCE.html. [Google Scholar]
- 45.Health Resources and Services Administration. Unified Health Communication (UHC): addressing health literacy, cultural competency, and limited English proficiency [Internet] Rockville (MD): HHS; [cited 2012 Jan 10]. Available from: http://www.hrsa.gov/publichealth/healthliteracy/index.htmlss. [Google Scholar]
- 46.Agency for Healthcare Research and Quality. What is the PCMH? AHRQ’s definition of the medical home [Internet] Rockville (MD): AHRQ; [last updated 2011 Sep 20 cited 2012 Jan 10]. Available from: http://pcmh.ahrq.gov/portal/server.pt/community/pcmh__home/1483/what_is_pcmh_. [Google Scholar]
- 47.Joint Commission. Joint Commission’s primary care medical home option additional requirements [Internet] Oakbrook Terrace (IL): Joint Commission; 2011. Jun 21, [cited 2012 Jan 17]. Available from: http://www.jointcommission.org/assets/1/18/PCMH_new_stds_by_5_characteristics.pdf. [Google Scholar]
- 48.Honoré PA, Wright D, Berwick DM, Clancy CM, Lee P, Nowinski J, et al. Creating a framework for getting quality into the public health system. Health Aff (Millwood) 2011;30(4):739. doi: 10.1377/hlthaff.2011.0129. [DOI] [PubMed] [Google Scholar]
- 49.Agency for Healthcare Research and Quality. Guide to prevention quality indicators: hospital admission for ambulatory care sensitive conditions [Internet] Rockville (MD): AHRQ; 2001. Oct, [cited 2012 Jan 10]. Available from: http://www.ahrq.gov/downloads/pub/ahrqqi/pqiguide.pdf. [Google Scholar]
- 50.Sanderson C, Dixon J. Conditions for which onset or hospital admission is potentially preventable by timely and effective ambulatory care. J Health Serv Res Policy. 2000;5(4):222–30. doi: 10.1177/135581960000500407. [DOI] [PubMed] [Google Scholar]
- 51.Jack BW, Chetty VK, Anthony D, Greenwald JL, Sanchez GM, Johnson AE, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178–87. doi: 10.7326/0003-4819-150-3-200902030-00007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Calculations based on data from HCUPnet. Welcome to H-CUPnet [home page on the Internet] Rockville (MD): AHRQ; Agency for Healthcare Research and Quality. [cited 2012 Jan 10]. Available from: http://hcupnet.ahrq.gov/ [Google Scholar]
- 53.Voss R, Gardner R, Baier R, Butterfield K, Lehrman S, Gravenstein S. The care transitions intervention: translating from efficacy to effectiveness. Arch Intern Med. 2011;171(14):1232–7. doi: 10.1001/archinternmed.2011.278. [DOI] [PubMed] [Google Scholar]
- 54.Boston University Medical Center. Original Project RED toolkit [Internet] Boston (MA): Boston University Medical Center; [cited 2012 Jan 10]. Available from: http://www.bu.edu/fammed/projectred/toolkit.html. [Google Scholar]
- 55.Schillinger D, Keller D. The other side of the coin: attributes of a “health literate” healthcare organization. Washington (DC): Institute of Medicine; 2011. Nov 16, [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.